Active Surveillance in Non-Muscle Invasive Bladder Cancer, the Potential Role of Biomarkers: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Objectives
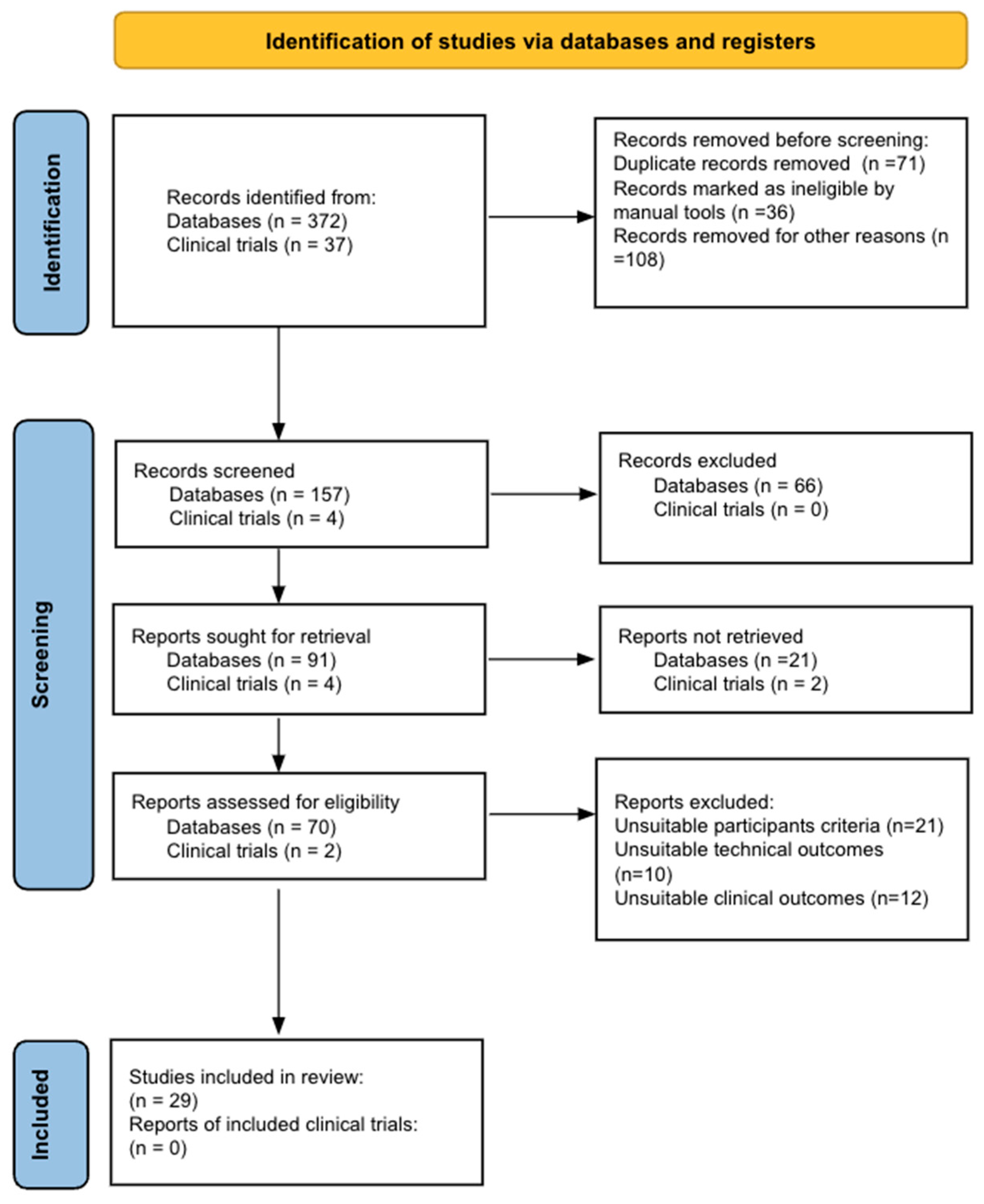
3. Acquisition of Evidence/Methodology
4. Synthesis of Evidence
4.1. Active Surveillance

{kind=link}
| Authors | Stages | N | Study | Inclusion Criteria | Exit Criteria | Follow-Up Period * | Conclusions |
|---|---|---|---|---|---|---|---|
| Soloway et al., 2003 [10] | Ta or T1 G1–G2 | T = 32 Not control group | Retrospective | Small día-meter: 0.5–1.0 cm Papillary tumor Low Grade | Not specify | 10.09 months | Small, recurrent, low-grade appearing bladder tumors are slow growing and pose minimal risk. |
| Gofrit et al., 2005 [25] | Ta tumors (G1–G2) | T = 28 Not control group | Retrospective | No history of previous high grade (G3) tumors, small papillary tumor (<10 mm) negative urinary citology | Additional tumors Excessive tumor growth >10 mm | Small recurrent low-grade Ta papillary tumors possess a low-risk tumor progress, making active surveillance a safe practice. | |
| Pruthi et al., 2008 [26] | Superficial bladder cancer | T = 173 22 patients were included Not control group | Retrospective | Noninvasive low- or high-grade papillary urothelial carcinoma (Ta, T1) or urothelial carcinoma in situ | Urothelial papilloma Papillary urothelial neoplasm low malignancy potential Atypical lesion | 25 months | Conservative treatment of recurrent bladder tumors is an appropriate option in patients with low-grade Ta tumors. |
| Hernandez et al., 2009 [27] | Pta, pT1 | T = 273 64 patients were included 203 were control group | Prospective | Papillary tumors Negative cytological findings Less than 1 cm in size Fewer than 5 tumors | Increase in the number and/or size of lesiones (less than 1 cm, and/or <5 tumors) Gross hematuria Positive urinary cytology | 38.6 months | Small tumors <1 cm and non-muscle invasive tumors can safely be offered the active surveillance protocol. |
| Hernandez et al., 2016 [29] | pTa–pT1 G1–G2 | T = 186 Not control group | Retrospective | Recurrent papillary tumors Less than 1 cm in size Fewer than 5 tumor locations | Increase in the number or size of the lesions Symptoms (mainly hematuria) Positive urine cytology | 53 months | Associated factors with a higher risk of grade progression were multiple lesions, previous stage and grade, age, and time since the initial TURBT, however, they were not related to tumor stage progression. |
| Hurle et al., 2016 [28] | pTa–pT1a | T = 293 55 patients were included not control group | Retrospective | Urinary citology (−) <5 lesions A diameter <10 mm Absence of CIS ª or persistent hematuria | Positive cytology CIS up-grade | 53 months | AS protocol for NMIBC could be a reasonable alternative in patients with recurrent low-grade pTa/pT1a small papillary bladder tumor. |
| Contieri et al., 2022 [3] | pTa (grade 1–2) and pT1a (grade 2) | T = 214 156 patients ≤18 months of AS ° 95 patients >18 months of AS ° | Retrospective | ≤5 suspicious lesions Diameter ≤ 1 cm Absence of gross hematuria Negative urinary cytology | Tumor size increase > 1 cm Number of lesions ≥ 5 Increase in both number and size of lesions Positive cytology Gross hematuria | 36.8 months | Well-selected patients with NMIBC can safely remain on AS for a long period of time. Multiple TURs and multiple lesions at AS enrollment are associated with a higher risk of AS failure. |
4.2. Biomarkers
| Author | Biomarker | Sample | Molecule | Technique | N | Usefulness in Active Surveillance |
|---|---|---|---|---|---|---|
| A Schneider et al., 2000 [46] | iD9S162, IFNA, D16S310, D16S476, D4S243, FGA, ACTBP2, D9S171, D9S747, MJD52, D8S307, THO, D13S802, D17S695, D17S654, D20S48, TP53 | Urine and Blood | Microsatellite DNA | RT-PCR | T = 209 103 BC, 80 other disease and 26 controls | Recurrence SN = 84% |
| Robert S Svatek et al., 2006 [47] | sFAS NMP22 | Urine | RNA | ELISA | T = 229 122 BC and 107 controls | Progression Stage SN = 75% |
| Sheng-Fang Su et al., 2014 [37] | HOXA9, SOX1, NPY, IRAK3, and ZO2,f L1-MET. | Urine | DNA | Pyrosequencing | T = 90 56 BC patients without recurrence and 34 BC patients with recurrence | Recurrence SN = 80% |
| Birkenkamp-Demtröder et al., 2016 [40] | 4–48 personalized genomic variants | Urine and plasma | ucfDNA | RT-PCR | T = 12 6 BC patients with progression and 6 BC patients with recurrence | Progression |
| Roperch J. et al., 2016 [38] | FGFR3 S249C | Urine | DNA | Methylation-specific RT-PCR | T = 263 158 BC and 105 controls | Recurrence SN = 97% SP = 84.8% |
| Ye-Hwan Kim et al., 2016 [48] | Topoisomerase-II alpha (TopoIIA) | Urine supernatant | cfDNA | RT-PCR | T = 198 83 BC, 54 patients with hematuria and 61 controls | Exclusion criteria SN = 73.8% SP = 68.3% |
| Fantony et al., 2017 [49] | NID2 TWIST1 | Urine | DNA | Methylation-specific RT-PCR | T = 172 63 patients with hematuria and 109 NMIBC patients | Recurrence SN = 54% |
| Zhang et al., 2017 [43] | NDRG2 | Urine | RNA | RT-PCR Western blot | T = 221 124 BC and 97 control subjects | Progression Grade Stage SN = 85.5% SP = 81.4% |
| Van der Heijden A. et al., 2018 [50] | CFTR, SALL3, and TWIST1 | Urine | DNA | Pyrosequencing | T = 168 111 BC and 57 controls | Recurrence SN = 96% SP = 40% NPV = 92% |
| Allione A. et al., 2018 [51] | MMP23A MMP23B | Urine | Protein | ELISA Western blot | T = 101 44 BC and 57 controls | Recurrence |
| Lutao Du, et al., 2018 [44] | GAS5 uc004cox.4 | Urine | IncRNA | qRT-PCR Microarray analysis | T = 480 240 BC and 240 controls | Progression Identify high-risk tumors SN = 84.5% SP = 78.2% |
| Thorsten H Ecke et al., 2018 [52] | Cytokeratin 8 Cytokeratin 18 | Urine | Protein (soluble fragments) | ELISA | T = 530 182 NMIBC patients, 60 MIBC, 62 patients with non-evidence of disease and 226 controls | Progression Identify high-grade vs. low-grade tumors SN = 78.8% (Low grade) SN = 75% (High grade) SP = 93.8% |
| Hofbauer S. et al., 2018 [53] | 6 miRs (let-7c, miR-135a, miR-135b, miR-148a, miR-204, miR-345) | Urine | RNA | RT-PCR | T = 245 133 BC and 112 controls | Recurrence SN = 94% SP = 51% |
| Yanjie Xu et al., 2019 [41] | IQGAP3 BMP4 FAM107A | Urine | uctDNA | RT-PCR | 103 BC | Recurrence Progression stage and grade |
| Yujiro Hayashi et al., 2020 [54] | TERT C228T | Urine | ucfDNA | ddPCR RT-PCR | T = 76 40 pre-TURB patients and 36 surveillance group | Recurrence SN = 68.9% SP = 96.2% |
| Xu Chen et al., 2020 [55] | 2 CpG markers (cg21472506 and cg11437784) | Urine | DNA | utMEMA | T = 175 109 BC and 66 controls | Recurrence SN = 90% SP = 83.1% |
| Song Z et al., 2020 [42] | hsa_circ_0137439 | Urine | circRNA | Microarray analysis, RT-PCR | T = 146 116 BC, 30 controls | Progression, predict grade, stage and lymph node status |
| Zhenyu Ou et al., 2020 [56] | Urinary cell-free DNA (ucfDNA) TERT, FGFR3, PIK3CA and KRAS | Urine | cfDNA | Next-generation sequencing | T = 125 92 BC and 33 controls | Recurrence |
| Elsawy et al., 2021 [39] | ANXA10 UPK1B CRH IGF2 | Urine | RNA | Xpert monitor | 181 NMIBC | Recurrence SN = 73.7% SP = 79.6% NPV = 96.3% |
| Leihong Deng et al., 2022 [57] | DMRTA2 | Urine | DNA | Methylation-specific RT-PCR | T = 127 44 BC, 83 controls | Recurrence SN = 82.9% SP = 92.5% |
| Anouk E. Hentschel, 2022 [58] | FAM19A4, GHSR, MAL, miR-129, miR-935, PHACTR3, PRDM14, SST and ZIC1 | Urine | DNA | Methylation-specific RT-PCR | T = 26 14 BC and 12 benign hematuria patients | Recurrence SN = 80% SP = 93% |
| Samah Mamdouh et al., 2022 [45] | miR-200, miR-145 miR-21 | Urine | RNA | RT-PCR | T = 136 11 BC and 25 controls | Recurrence Progression, discriminate high grade v/s low grade SN = 91.7% SP = 46.2% |
| TOTAL | 4013 |
5. Discussion
6. Future Directions
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dyrskjøt, L.; Hansel, D.E.; Efstathiou, J.A.; Knowles, M.A.; Galsky, M.D.; Teoh, J.; Theodorescu, D. Bladder cancer. Nat. Rev. Dis. Primers 2023, 9, 58. [Google Scholar] [CrossRef] [PubMed]
- Fasulo, V.; Paciotti, M.; Lazzeri, M.; Contieri, R.; Casale, P.; Saita, A.; Lughezzani, G.; Diana, P.; Frego, N.; Avolio, P.; et al. Xpert Bladder Cancer Monitor May Avoid Cystoscopies in Patients Under “Active Surveillance” for Recurrent Bladder Cancer (BIAS Project): Longitudinal Cohort Study. Front. Oncol. 2022, 12, 832835. [Google Scholar] [CrossRef] [PubMed]
- Contieri, R.; Paciotti, M.; Lughezzani, G.; Buffi, N.M.; Frego, N.; Diana, P.; Fasulo, V.; Saita, A.; Casale, P.; Lazzeri, M.; et al. Long-term Follow-up and Factors Associated with Active Surveillance Failure for Patients with Non–muscle-invasive Bladder Cancer: The Bladder Cancer Italian Active Surveillance (BIAS) Experience. Eur. Urol. Oncol. 2022, 5, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Zhou, M.; Yang, B.; Zhou, S.; Liu, Z.; Zhang, J. A Systematic Review on the Role of Repeat Transurethral Resection after Initial en Bloc Resection for Non-Muscle Invasive Bladder Cancer. J. Clin. Med. 2022, 11, 5049. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.H.C.; Patel, M.I. Transurethral resection of bladder tumour (TURBT). Transl. Androl. Urol. 2020, 9, 3056–3072. [Google Scholar] [CrossRef] [PubMed]
- Bansal, A.; Sankhwar, S.; Goel, A.; Kumar, M.; Purkait, B.; Aeron, R. Grading of complications of transurethral resection of bladder tumor using Clavien–Dindo classification system. Indian J. Urol. 2016, 32, 232. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, E.; Fujita, K.; Hashimoto, M.; Uemura, H.; Nonomura, N. Urinary markers for bladder cancer diagnosis: A review of current status and future challenges. Int. J. Urol. 2024, 31, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Mossanen, M.; Wang, Y.; Szymaniak, J.; Tan, W.S.; Huynh, M.J.; Preston, M.A.; Trinh, Q.; Sonpavde, G.; Kibel, A.; Chang, S. Evaluating the cost of surveillance for non-muscle-invasive bladder cancer: An analysis based on risk categories. World J. Urol. 2019, 37, 2059–2065. [Google Scholar] [CrossRef]
- Petrelli, F.; Giannatempo, P.; Maccagnano, C.; Contieri, R.; Hurle, R. Active surveillance for non-muscle invasive bladder cancer: A systematic review and pooled-analysis. Cancer Treat Res. Commun. 2021, 27, 100369. [Google Scholar] [CrossRef]
- Soloway, M.S.; Bruck, D.S.; Kim, S.S. Expectant Management of Small, Recurrent, Noninvasive Papillary Bladder Tumors. J. Urol. 2003, 170, 438–441. [Google Scholar] [CrossRef]
- Fan, X.; He, W.; Huang, J. Bladder-sparing approaches for muscle invasive bladder cancer: A narrative review of current evidence and future perspectives. Transl. Androl. Urol. 2023, 12, 802–808. [Google Scholar] [CrossRef]
- Contieri, R.; Lazzeri, M.; Hurle, R. When and How to Perform Active Surveillance for Low-risk Non–muscle-invasive Bladder Cancer. Eur. Urol. Focus. 2023, 9, 564–566. [Google Scholar] [CrossRef] [PubMed]
- von Deimling, M.; Pallauf, M.; Bianchi, A.; Laukhtina, E.; Karakiewicz, P.I.; Rink, M.; Shariat, S.; Pradere, B. Active surveillance for non-muscle-invasive bladder cancer: Fallacy or opportunity? Curr. Opin. Urol. 2022, 32, 567–574. [Google Scholar] [CrossRef]
- Hurle, R.; Maccagnano, C. Active surveillance for recurrent low-grade non-muscle-invasive bladder cancer: Can we take any advantage from the COVID-19 crisis? Arab. J. Urol. 2020, 18, 65–66. [Google Scholar] [CrossRef]
- Lozano, F.; Raventós, C.X.; Carrión, A.; Trilla, E. Optimization biomarkers in the surveillance of non muscle invasive bladder cancer. Arch Esp. Urol. 2022, 75, 133–143. [Google Scholar] [PubMed]
- Sugeeta, S.S.; Sharma, A.; Ng, K.; Nayak, A.; Vasdev, N. Biomarkers in Bladder Cancer Surveillance. Front. Surg. 2021, 8, 735868. [Google Scholar] [CrossRef]
- Harsanyi, S.; Novakova, Z.V.; Bevizova, K.; Danisovic, L.; Ziaran, S. Biomarkers of Bladder Cancer: Cell-Free DNA, Epigenetic Modifications and Non-Coding RNAs. Int. J. Mol. Sci. 2022, 23, 13206. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Holzbeierlein, J.M.; Bixler, B.R.; Buckley, D.I.; Chang, S.S.; Holmes, R.; James, A.C.; Kirkby, E.; McKiernan, J.; Schuckman, A. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline: 2024 Amendment. J. Urol. 2024, 211, 533–538. [Google Scholar] [CrossRef]
- EAU Guidelines. Edition presented at the EAU Annual Congress Milan 2023; EAU Guidelines Office: Arnhem, The Netherlands, 2023; ISBN 978-94-92671-19-6. [Google Scholar]
- Roobol, M.J.; Bangma, C.H.; el Bouazzaoui, S.; Franken-Raab, C.G.; Zwarthoff, E.C. Feasibility study of screening for bladder cancer with urinary molecular markers (the BLU-P project). Urol. Oncol. Semin. Orig. Investig. 2010, 28, 686–690. [Google Scholar] [CrossRef]
- Cowan, B.; Klein, E.; Jansz, K.; Westenfelder, K.; Bradford, T.; Peterson, C.; Scherr, D.; Karsh, L.; Egerdie, B.; Witjes, A.; et al. Longitudinal follow-up and performance validation of an mRNA-based urine test (Xpert Bladder Cancer Monitor) for surveillance in patients with non-muscle-invasive bladder cancer. BJU Int. 2021, 128, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Neuzillet, Y.; Pradère, B.; Xylinas, E.; Allory, Y.; Audenet, F.; Loriot, Y.; Masson-Lecomte, A.; Roumiguié, M.; Seisen, T.; Traxer, O.; et al. French AFU Cancer Committee Guidelines—Update 2022-2024: Non-muscle-invasive bladder cancer (NMIBC). Progrès En Urol. 2022, 32, 1102–1140. [Google Scholar] [CrossRef]
- Babcook, C.J.; Goldstein, R.B.; Barth, R.A.; Damato, N.M.; Callen, P.W.; Filly, R.A. Prevalence of ventriculomegaly in association with myelomeningocele: Correlation with gestational age and severity of posterior fossa deformity. Radiology 1994, 190, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Gofrit, O.N.; Pode, D.; Lazar, A.; Katz, R.; Shapiro, A. Watchful Waiting Policy in Recurrent Ta G1 Bladder Tumors. Eur. Urol. 2006, 49, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Pruthi, R.S.; Baldwin, N.; Bhalani, V.; Wallen, E.M. Conservative Management of Low Risk Superficial Bladder Tumors. J. Urol. 2008, 179, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Hernández, V.; Alvarez, M.; de la Peña, E.; Amaruch, N.; Martín, M.D.; de la Morena, J.M.; Gómez, V.; Llorente, C. Safety of Active Surveillance Program for Recurrent Nonmuscle-invasive Bladder Carcinoma. Urology 2009, 73, 1306–1310. [Google Scholar] [CrossRef] [PubMed]
- Hurle, R.; Pasini, L.; Lazzeri, M.; Colombo, P.; Buffi, N.; Lughezzani, G.; Casale, P.; Morenghi, E.; Peschechera, R.; Zandegiacomo, S.; et al. Active surveillance for low-risk non-muscle-invasive bladder cancer: Mid-term results from the Bladder cancer Active Surveillance project. BJU Int. 2016, 118, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Hernández, V.; Llorente, C.; de la Peña, E.; Pérez-Fernández, E.; Guijarro, A.; Sola, I. Long-term oncological outcomes of an active surveillance program in recurrent low grade Ta bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 165.e19–165.e23. [Google Scholar] [CrossRef] [PubMed]
- Gharibvand, M.; Kazemi, M.; Motamedfar, A.; Sametzadeh, M.; Sahraeizadeh, A. The role of ultrasound in diagnosis and evaluation of bladder tumors. J. Family Med. Prim. Care. 2017, 6, 840. [Google Scholar]
- Stamatiou, K.; Moschouris, H.; Papadaki, M.; Perlepes, G.; Skolarikos, A. Accuracy of modern ultrasonographic techniques in the follow up of patients with superficial bladder carcinoma. Med. Ultrason. 2011, 13, 114–119. [Google Scholar]
- Mukhtar, S.; Perry, M.J.A. Future Prospects for Bladder Cancer Biomarkers. BJU Int. 2011, 108, 1541–1543. [Google Scholar] [CrossRef]
- Chou, R.; Gore, J.L.; Buckley, D.; Fu, R.; Gustafson, K.; Griffin, J.C.; Grusing, S.; Selph, S. Urinary Biomarkers for Diagnosis of Bladder Cancer. Ann. Intern Med. 2015, 163, 922–931. [Google Scholar] [CrossRef]
- Zeng, Y.; Wang, A.; Lv, W.; Wang, Q.; Jiang, S.; Pan, X.; Wang, F.; Yang, H.; Bolund, L.; Lin, C.; et al. Recent development of urinary biomarkers for bladder cancer diagnosis and monitoring. Clin. Transl. Discov. 2023, 3, e183. [Google Scholar] [CrossRef]
- Castaneda, P.R.; Theodorescu, D.; Rosser, C.J.; Ahdoot, M. Identifying novel biomarkers associated with bladder cancer treatment outcomes. Front. Oncol. 2023, 13, 1114203. [Google Scholar] [CrossRef]
- Kim, B.; Jung, M.; Moon, K.C.; Han, D.; Kim, K.; Kim, H.; Yang, S.; Lee, D.; Jun, H.; Lee, K.; et al. Quantitative proteomics identifies TUBB6 as a biomarker of muscle-invasion and poor prognosis in bladder cancer. Int. J. Cancer. 2023, 152, 320–330. [Google Scholar] [CrossRef]
- Su, S.-F.; de Castro Abreu, A.L.; Chihara, Y.; Tsai, Y.; Andreu-Vieyra, C.; Daneshmand, S.; Skinner, E.; Jones, P.; Siegmund, K.; Liang, G. A Panel of Three Markers Hyper- and Hypomethylated in Urine Sediments Accurately Predicts Bladder Cancer Recurrence. Clin. Cancer Res. 2014, 20, 1978–1989. [Google Scholar] [CrossRef]
- Roperch, J.-P.; Grandchamp, B.; Desgrandchamps, F.; Mongiat-Artus, P.; Ravery, V.; Ouzaid, I.; Roupret, M.; Phe, V.; Ciofu, C.; Tubach, F.; et al. Promoter hypermethylation of HS3ST2, SEPTIN9 and SLIT2 combined with FGFR3 mutations as a sensitive/specific urinary assay for diagnosis and surveillance in patients with low or high-risk non-muscle-invasive bladder cancer. BMC Cancer 2016, 16, 704. [Google Scholar] [CrossRef]
- Elsawy, A.A.; Awadalla, A.; Elsayed, A.; Abdullateef, M.; Abol-Enein, H. Prospective Validation of Clinical Usefulness of a Novel mRNA-based Urine Test (Xpert® Bladder Cancer Monitor) for surveillance in Non Muscle Invasive Bladder Cancer. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 77.e9–77.e16. [Google Scholar] [CrossRef]
- Birkenkamp-Demtröder, K.; Nordentoft, I.; Christensen, E.; Høyer, S.; Reinert, T.; Vang, S.; Borre, M.; Agerbæk, M.; Jensen, J.B.; Ørntoft, T.F.; et al. Genomic Alterations in Liquid Biopsies from Patients with Bladder Cancer. Eur. Urol. 2016, 70, 75–82. [Google Scholar] [CrossRef]
- Xu, Y.; Kim, Y.-H.; Jeong, P.; Piao, X.-M.; Byun, Y.J.; Seo, S.P.; Kang, H.; Kim, W.; Lee, J.; Ryu, D.H.; et al. Urinary Cell-Free DNA IQGAP3/BMP4 Ratio as a Prognostic Marker for Non–Muscle-Invasive Bladder Cancer. Clin. Genitourin. Cancer 2019, 17, e704–e711. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Zhang, Q.; Zhu, J.; Yin, G.; Lin, L.; Liang, C. Identification of urinary hsa_circ_0137439 as a potential biomarker and tumor regulator of bladder cancer. Neoplasma 2020, 67, 137–146. [Google Scholar] [CrossRef]
- Zhang, M.; Ren, B.; Li, Z.; Niu, W.; Wang, Y. Expression of N-Myc Downstream-Regulated Gene 2 in Bladder Cancer and Its Potential Utility as a Urinary Diagnostic Biomarker. Med. Sci. Monit. 2017, 23, 4644–4649. [Google Scholar] [CrossRef]
- Du, L.; Duan, W.; Jiang, X.; Zhao, L.; Li, J.; Wang, R.; Yan, S.; Xie, Y.; Yan, K.; Wang, Q.; et al. Cell-free lncRNA expression signatures in urine serve as novel non-invasive biomarkers for diagnosis and recurrence prediction of bladder cancer. J. Cell Mol. Med. 2018, 22, 2838–2845. [Google Scholar] [CrossRef]
- Mamdouh, S.; Sherif, H.; Romeih, M.; Elesaily, K. Urine micro-RNA signature as a potential non-invasive diagnostic biomarker in bladder cancer. Asian Pac. J. Cancer Prev. 2023, 24, 121–131. [Google Scholar]
- Schneider, A.; Borgnat, S.; Lang, H.; Régine, O.; Lindner, V.; Kassem, M.; Saussine, C.; Oudet, P.; Jacqmin, D.; Gaub, M.P. Evaluation of microsatellite analysis in urine sediment for diagnosis of bladder cancer. Cancer Res. 2000, 60, 4617–4622. [Google Scholar]
- Svatek, R.S.; Herman, M.P.; Lotan, Y.; Casella, R.; Hsieh, J.; Sagalowsky, A.I.; Shariat, S.F. Soluble Fas—A promising novel urinary marker for the detection of recurrent superficial bladder cancer. Cancer 2006, 106, 1701–1707. [Google Scholar] [CrossRef]
- Kim, Y.-H.; Yan, C.; Lee, I.-S.; Piao, X.-M.; Byun, Y.J.; Jeong, P.; Kim, W.; Yun, S.; Kim, W. Value of urinary topoisomerase-IIA cell-free DNA for diagnosis of bladder cancer. Investig. Clin. Urol. 2016, 57, 106. [Google Scholar] [CrossRef]
- Fantony, J.J.; Longo, T.A.; Gopalakrishna, A.; Owusu, R.; Lance, R.S.; Foo, W.C.; Inman, B.A.; Abern, M.R. Urinary NID2 and TWIST1 methylation to augment conventional urine cytology for the detection of bladder cancer. Cancer Biomark. 2017, 18, 381–387. [Google Scholar] [CrossRef]
- van der Heijden, A.G.; Mengual, L.; Ingelmo-Torres, M.; Lozano, J.J.; van Rijt-van de Westerlo, C.C.M.; Baixauli, M.; Geavlete, B.; Moldoveanud, C.; Ene, C.; Dinney, C.; et al. Urine cell-based DNA methylation classifier for monitoring bladder cancer. Clin. Epigenet. 2018, 10, 71. [Google Scholar] [CrossRef]
- Allione, A.; Pardini, B.; Viberti, C.; Giribaldi, G.; Turini, S.; Di Gaetano, C.; Guarrera, S.; Cordero, F.; Oderda, M.; Allasia, M.; et al. MMP23B expression and protein levels in blood and urine are associated with bladder cancer. Carcinogenesis 2018, 39, 1254–1263. [Google Scholar] [CrossRef]
- Ecke, T.; Weiß, S.; Stephan, C.; Hallmann, S.; Arndt, C.; Barski, D.; Otto, T.; Gerullis, H. UBC® Rapid Test—A Urinary Point-of-Care (POC) Assay for Diagnosis of Bladder Cancer with a focus on Non-Muscle Invasive High-Grade Tumors: Results of a Multicenter-Study. Int. J. Mol. Sci. 2018, 19, 3841. [Google Scholar] [CrossRef]
- Hofbauer, S.L.; de Martino, M.; Lucca, I.; Haitel, A.; Susani, M.; Shariat, S.F.; Klatte, T. A urinary microRNA (miR) signature for diagnosis of bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 531.e1–531.e8. [Google Scholar] [CrossRef]
- Hayashi, Y.; Fujita, K.; Matsuzaki, K.; Eich, M.-L.; Tomiyama, E.; Matsushita, M.; Koh, Y.; Nakano, K.; Wang, C.; Ishizuya, Y.; et al. Clinical Significance of Hotspot Mutation Analysis of Urinary Cell-Free DNA in Urothelial Bladder Cancer. Front. Oncol. 2020, 10, 755. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, J.; Ruan, W.; Huang, M.; Wang, C.; Wang, H.; Jiang, Z.; Wang, S.; Liu, Z.; Liu, C.; et al. Urine DNA methylation assay enables early detection and recurrence monitoring for bladder cancer. J. Clin. Investig. 2020, 130, 6278–6289. [Google Scholar] [CrossRef]
- Ou, Z.; Li, K.; Yang, T.; Dai, Y.; Chandra, M.; Ning, J.; Wang, Y.; Xu, R.; Gao, T.; Xie, Y.; et al. Detection of bladder cancer using urinary cell-free DNA and cellular DNA. Clin. Transl. Med. 2020, 9, 4. [Google Scholar] [CrossRef]
- Deng, L.; Chao, H.; Deng, H.; Yu, Z.; Zhao, R.; Huang, L.; Gong, Y.; Zhu, Y.; Wang, Q.; Li, F.; et al. A novel and sensitive DNA methylation marker for the urine-based liquid biopsies to detect bladder cancer. BMC Cancer 2022, 22, 510. [Google Scholar] [CrossRef]
- Hentschel, A.E.; Beijert, I.J.; Bosschieter, J.; Kauer, P.C.; Vis, A.N.; Lissenberg-Witte, B.I.; van Moorselaar, J.R.; Steenbergen, R.; Jakko, A.; Nieuwenhuijzen, J. Bladder cancer detection in urine using DNA methylation markers: A technical and prospective preclinical validation. Clin. Epigenet. 2022, 14, 19. [Google Scholar] [CrossRef]
- Scarpato, K.R.; Tyson, M.D.; Clark, P.E. Natural biology and management of nonmuscle invasive bladder cancer. Curr. Opin. Oncol. 2016, 28, 210–215. [Google Scholar] [CrossRef]
- Tilki, D.; Burger, M.; Dalbagni, G.; Grossman, H.B.; Hakenberg, O.W.; Palou, J.; Reich, O.; Rouprêt, M.; Shariat, S.; Zlotta, A. Urine Markers for Detection and Surveillance of Non–Muscle-Invasive Bladder Cancer. Eur. Urol. 2011, 60, 484–492. [Google Scholar] [CrossRef]
- Chakraborty, A.; Dasari, S.; Long, W.; Mohan, C. Urine protein biomarkers for the detection, surveillance, and treatment response prediction of bladder cancer. Am. J. Cancer Res. 2019, 9, 1104–1117. [Google Scholar]
- Lee, H.-H.; Kim, S.H. Review of non-invasive urinary biomarkers in bladder cancer. Transl. Cancer Res. 2020, 9, 6554–6564. [Google Scholar] [CrossRef]
- Vanderbilt University Medical Center. Observation Versus Immediate Surgery of Low Risk Bladder Cancer (NCT02700724). 2016. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT02700724 (accessed on 10 December 2023).
- The University of Texas Health Science Center at San Antonio. Surveillance for Low and Low-Intermediate Risk Non-Muscle Invasive Bladder Cancer: A Pilot Study (NCT02298998). 2014. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT02298998 (accessed on 10 December 2023).
- Reyes, R.M.; Rios, E.; Barney, S.; Hugen, C.M.; Michalek, J.E.; Lotan, Y.; Messing, E.; Svatek, R. A Randomized Feasibility Trial Comparing Surveillance Regimens for Patients with Low and Low-Intermediate Risk Non-Muscle Invasive Bladder Cancer. Bladder Cancer 2021, 7, 285–295. [Google Scholar] [CrossRef]
- Vall Hebron Insitut Recerca. Active Surveillance vs in Office Fulguration for Low Grade Bladder Cancer Tumors (NCT05148728). 2021. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05148728 (accessed on 10 December 2023).
- Bilim, V.; Kuroki, H.; Shirono, Y.; Murata, M.; Hiruma, K.; Tomita, Y. Advanced Bladder Cancer: Changing the Treatment Landscape. J. Pers. Med. 2022, 12, 1745. [Google Scholar] [CrossRef]
- Karimi, A.; Shobeiri, P.; Azadnajafabad, S.; Masinaei, M.; Rezaei, N.; Ghanbari, A.; Rezaei, N.; Rouhifard, M.; Shahin, S.; Rashidi, M.; et al. A global, regional, and national survey on burden and Quality of Care Index (QCI) of bladder cancer: The global burden of disease study 1990–2019. PLoS ONE 2022, 17, e0275574. [Google Scholar] [CrossRef]
- Fujii, T.; Uchiyama, T.; Takeda, M.; Shimada, K. Diagnostic Strategies for Urologic Cancer Using Expression Analysis of Various Oncogenic Surveillance Molecules—From Non-Coding Small RNAs to Cancer-Specific Proteins. Appl. Sci. 2022, 12, 7390. [Google Scholar] [CrossRef]
- Shill, D.K.; Roobol, M.J.; Ehdaie, B.; Vickers, A.J.; Carlsson, S.V. Active surveillance for prostate cancer. Transl. Androl. Urol. 2021, 10, 2809–2819. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parrao, D.; Lizana, N.; Saavedra, C.; Larrañaga, M.; Lindsay, C.B.; San Francisco, I.F.; Bravo, J.C. Active Surveillance in Non-Muscle Invasive Bladder Cancer, the Potential Role of Biomarkers: A Systematic Review. Curr. Oncol. 2024, 31, 2201-2220. https://doi.org/10.3390/curroncol31040163
Parrao D, Lizana N, Saavedra C, Larrañaga M, Lindsay CB, San Francisco IF, Bravo JC. Active Surveillance in Non-Muscle Invasive Bladder Cancer, the Potential Role of Biomarkers: A Systematic Review. Current Oncology. 2024; 31(4):2201-2220. https://doi.org/10.3390/curroncol31040163
Chicago/Turabian StyleParrao, Diego, Nemecio Lizana, Catalina Saavedra, Matías Larrañaga, Carolina B. Lindsay, Ignacio F. San Francisco, and Juan Cristóbal Bravo. 2024. "Active Surveillance in Non-Muscle Invasive Bladder Cancer, the Potential Role of Biomarkers: A Systematic Review" Current Oncology 31, no. 4: 2201-2220. https://doi.org/10.3390/curroncol31040163
APA StyleParrao, D., Lizana, N., Saavedra, C., Larrañaga, M., Lindsay, C. B., San Francisco, I. F., & Bravo, J. C. (2024). Active Surveillance in Non-Muscle Invasive Bladder Cancer, the Potential Role of Biomarkers: A Systematic Review. Current Oncology, 31(4), 2201-2220. https://doi.org/10.3390/curroncol31040163