Challenges and Opportunities in Developing an Oncology Clinical Trial Network in the United States Veterans Affairs Health Care System: The VA STARPORT Experience

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
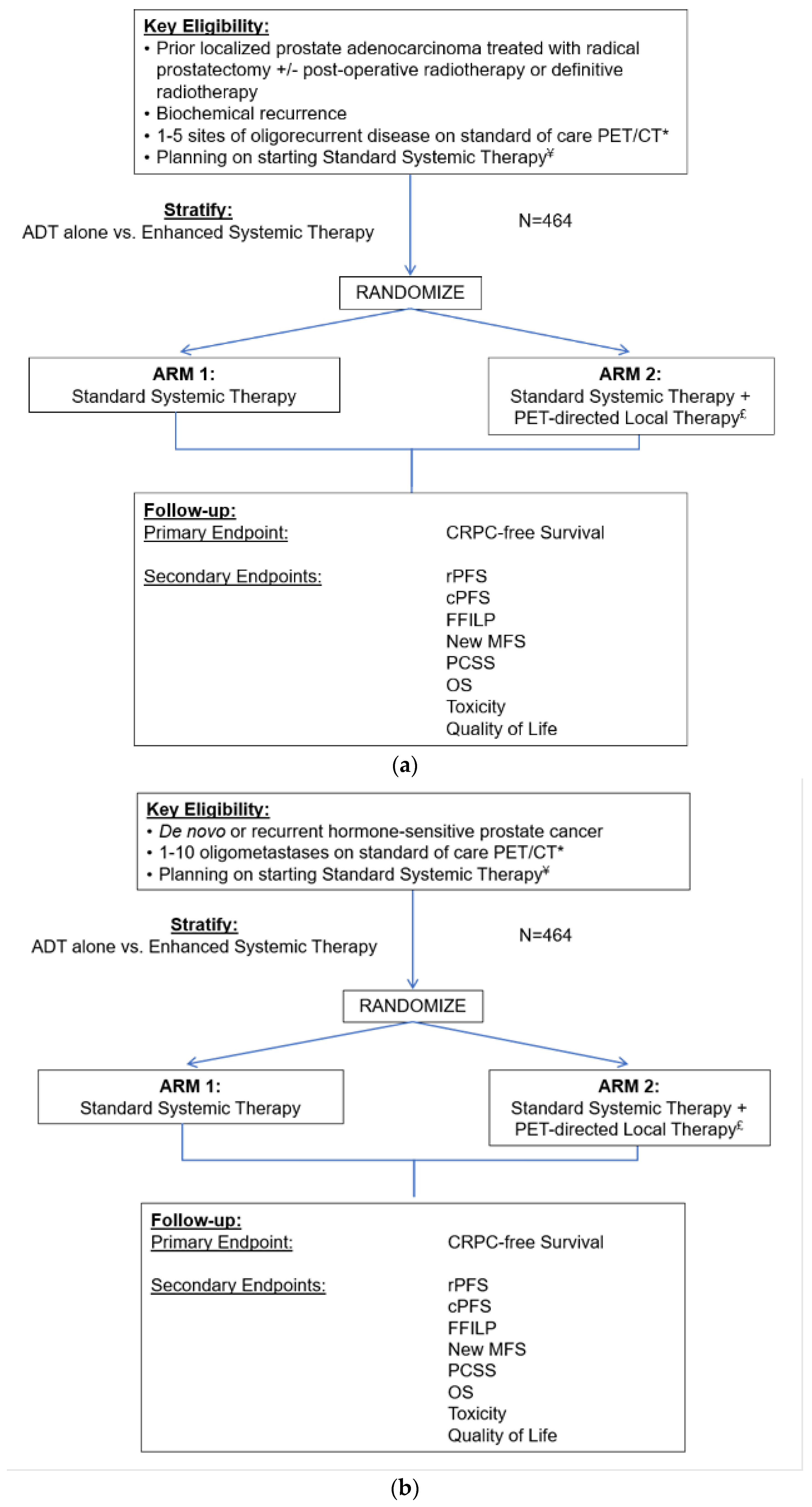
2.1. Study Design
2.2. Site Selection
2.3. Protocol Development
3. Results
3.1. Challenge #1: Developing a Clinical Trial Network
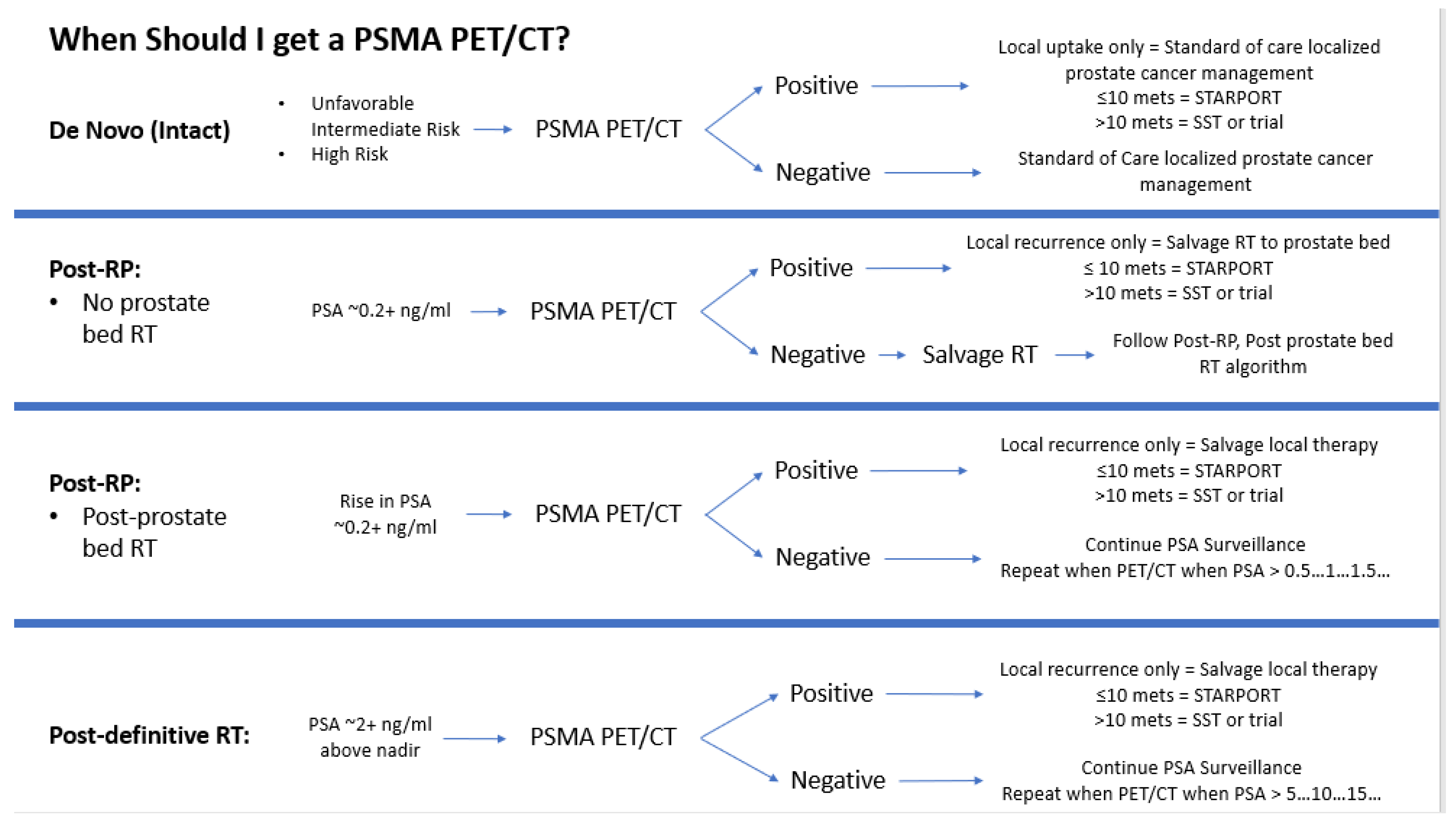
3.2. Challenge #2: Adapting to the Shifting Sands of Clinical Practice in Metastatic Prostate Cancer
3.3. Challenge #3: Maintaining Local Study Team Engagement over the Course of the Study
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolf, G.T.; Fisher, S.G.; Hong, W.K.; Hillman, R.; Spaulding, M.; Laramore, G.E.; Endicott, J.W.; McClatchey, K.; Henderson, W.G. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. N. Engl. J. Med. 1991, 324, 1685–1690. [Google Scholar] [CrossRef] [PubMed]
- Wilt, T.J.; Vo, T.N.; Langsetmo, L.; Dahm, P.; Wheeler, T.; Aronson, W.J.; Cooperberg, M.R.; Taylor, B.C.; Brawer, M.K. Radical Prostatectomy or Observation for Clinically Localized Prostate Cancer: Extended Follow-up of the Prostate Cancer Intervention Versus Observation Trial (PIVOT). Eur. Urol. 2020, 77, 713–724. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) Prostate Cancer Version 1.2024. Available online: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 15 May 2024).
- VA Oncology Prostate Cancer Clinical Pathway V2.2024. Available online: https://www.cancer.va.gov/CANCER/assets/pdf/clinical-pathways/21/ProstateCancer.pdf (accessed on 15 May 2024).
- Hillyer, G.C.; Park, Y.A.; Rosenberg, T.H.; Mundi, P.; Patel, I.; Bates, S.E. Positive attitudes toward clinical trials among military veterans leaves unanswered questions about poor trial accrual. Semin. Oncol. 2021, 48, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Zullig, L.L.; Sims, K.J.; McNeil, R.; Williams, C.D.; Jackson, G.L.; Provenzale, D.; Kelley, M.J. Cancer Incidence Among Patients of the U.S. Veterans Affairs Health Care System: 2010 Update. Mil. Med. 2017, 182, e1883–e1891. [Google Scholar] [CrossRef] [PubMed]
- Hellman, S.; Weichselbaum, R.R. Oligometastases. J. Clin. Oncol. 1995, 13, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Ost, P.; Reynders, D.; Decaestecker, K.; Fonteyne, V.; Lumen, N.; De Bruycker, A.; Lambert, B.; Delrue, L.; Bultijnck, R.; Goetghebeur, E.; et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence (STOMP): Five-year results of a randomized phase II trial. J. Clin. Oncol. 2020, 38 (Suppl. S6), 10. [Google Scholar]
- Phillips, R.; Shi, W.Y.; Deek, M.; Radwan, N.; Lim, S.J.; Antonarakis, E.S.; Rowe, S.P.; Ross, A.E.; Gorin, M.A.; Deville, C.; et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Harrow, S.; Palma, D.A.; Olson, R.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Radiation for the Comprehensive Treatment of Oligometastases (SABR-COMET)-Extended Long-Term Outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 611–616. [Google Scholar] [CrossRef]
- Tang, C.; Sherry, A.D.; Haymaker, C.; Bathala, T.; Liu, S.; Fellman, B.; Cohen, L.; Aparicio, A.; Zurita, A.J.; Reuben, A.; et al. Addition of Metastasis-Directed Therapy to Intermittent Hormone Therapy for Oligometastatic Prostate Cancer: The EXTEND Phase 2 Randomized Clinical Trial. JAMA Oncol. 2023, 9, 825–834. [Google Scholar] [CrossRef]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Pienta, K.J.; Gorin, M.A.; Rowe, S.P.; Carroll, P.R.; Pouliot, F.; Probst, S.; Saperstein, L.; Preston, M.A.; Alva, A.S.; Patnaik, A.; et al. A Phase 2/3 Prospective Multicenter Study of the Diagnostic Accuracy of Prostate Specific Membrane Antigen PET/CT with 18F-DCFPyL in Prostate Cancer Patients (OSPREY). J. Urol. 2021, 206, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.J.; Rowe, S.P.; Gorin, M.A.; Saperstein, L.; Pouliot, F.; Josephson, D.; Wong, J.Y.C.; Pantel, A.R.; Cho, S.Y.; Gage, K.L.; et al. Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study. Clin. Cancer Res. 2021, 27, 3674–3682. [Google Scholar] [CrossRef] [PubMed]
- Batra, A.; Glick, D.; Valdes, M. Contemporary Systemic Therapy Intensification for Prostate Cancer: A Review for General Practitioners in Oncology. Curr. Oncol. 2024, 31, 1047–1062. [Google Scholar] [CrossRef]
- O’Leary, T.J.; Dominitz, J.A.; Chang, K.M. Veterans Affairs Office of Research and Development: Research Programs and Emerging Opportunities in Digestive Diseases Research. Gastroenterology 2015, 149, 1652–1661. [Google Scholar] [CrossRef] [PubMed]
- Concato, J.; Peduzzi, P.; Huang, G.D.; O’Leary, T.J.; Kupersmith, J. Comparative effectiveness research: What kind of studies do we need? J. Investig. Med. 2010, 58, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Ritter, T.A.; Chao, H.H.; Chang, M.G.; Katsoulakis, E.; Padilla, L.; Xiao, Y.; Kang, H.; Al-Hallaq, H.A.; Moghanaki, D.; Palta, J.R.; et al. Enhancing Radiation Therapy Plan Quality in a Multi-Site Randomized Clinical Trial with a Benchmark Credentialing Exercise: The VA STARPORT Experience. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, S95–S96. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Correa, R.J.M.; Schneiders, F.; Haasbeek, C.J.A.; Rodrigues, G.B.; Lock, M.; Yaremko, B.P.; Bauman, G.S.; et al. Stereotactic ablative radiotherapy for the comprehensive treatment of 4-10 oligometastatic tumors (SABR-COMET-10): Study protocol for a randomized phase III trial. BMC Cancer 2019, 19, 816. [Google Scholar] [CrossRef]
- Guckenberger, M.; Lievens, Y.; Bouma, A.B.; Collette, L.; Dekker, A.; deSouza, N.M.; Dingemans, A.C.; Fournier, B.; Hurkmans, C.; Lecouvet, F.E.; et al. Characterisation and classification of oligometastatic disease: A European Society for Radiotherapy and Oncology and European Organisation for Research and Treatment of Cancer consensus recommendation. Lancet Oncol. 2020, 21, e18–e28. [Google Scholar] [CrossRef]
- Schroen, A.T.; Petroni, G.R.; Wang, H.; Gray, R.; Wang, X.F.; Cronin, W.; Sargent, D.J.; Benedetti, J.; Wickerham, D.L.; Djulbegovic, B.; et al. Preliminary evaluation of factors associated with premature trial closure and feasibility of accrual benchmarks in phase III oncology trials. Clin. Trials 2010, 7, 312–321. [Google Scholar] [CrossRef]
- Liu, F.F.; Okunieff, P.; Bernhard, E.J.; Stone, H.B.; Yoo, S.; Coleman, C.N.; Vikram, B.; Brown, M.; Buatti, J.; Guha, C. Lessons learned from radiation oncology clinical trials. Clin. Cancer Res. 2013, 19, 6089–6100. [Google Scholar] [CrossRef]
- O’Dwyer, P.J.; Gray, R.J.; Flaherty, K.T.; Chen, A.P.; Li, S.; Wang, V.; McShane, L.M.; Patton, D.R.; Tricoli, J.V.; Williams, P.M.; et al. The NCI-MATCH trial: Lessons for precision oncology. Nat. Med. 2023, 29, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Huddart, R.A.; Hall, E.; Lewis, R.; Birtle, A. Life and death of spare (selective bladder preservation against radical excision): Reflections on why the spare trial closed. BJU Int. 2010, 106, 753–755. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| VA STARPORT: Summary of Main Challenges and Strategies to Address Them | |
|---|---|
| Challenges | Strategies |
Developing a clinical trial network
| Facilitating local success through central support
|
Shifts in clinical practice for prostate cancer treatment
| Adapting the study protocol to evolving research
|
| Maintaining local study team engagement
| Maximize local site participation in study procedure development and provide value to local clinical programs through participation in the study
|
| Time (Months) | |||||
|---|---|---|---|---|---|
| Site Selection to Site Coordinator Hire | Site Selection to Local R&D Approval | Site Selection to Enrollment Start | Site Selection to First Consent | Enrollment Start to First Consent | |
| Median | 9.7 | 8.8 | 11 | 13.6 | 2.6 |
| 25th percentile | 7.7 | 6.7 | 10.6 | 11.5 | 0.8 |
| 75th percentile | 10.9 | 10.3 | 12.2 | 16.1 | 4.7 |
| Average | 10.1 | 8.7 | 10.8 | 14.1 | 3.3 |
| Std Deviation | 5.2 | 2.6 | 2.3 | 3.9 | 2.9 |
| Minimum | 1.3 | 4.3 | 5.1 | 7.8 | 0.2 |
| Maximum | 23.7 | 12.6 | 14.5 | 22.4 | 9.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solanki, A.A.; Zheng, K.; Skipworth, A.N.; Robin, L.M.; Leparski, R.F.; Henry, E.; Rettig, M.; Salama, J.K.; Ritter, T.; Jones, J.; et al. Challenges and Opportunities in Developing an Oncology Clinical Trial Network in the United States Veterans Affairs Health Care System: The VA STARPORT Experience. Curr. Oncol. 2024, 31, 4781-4794. https://doi.org/10.3390/curroncol31080358
Solanki AA, Zheng K, Skipworth AN, Robin LM, Leparski RF, Henry E, Rettig M, Salama JK, Ritter T, Jones J, et al. Challenges and Opportunities in Developing an Oncology Clinical Trial Network in the United States Veterans Affairs Health Care System: The VA STARPORT Experience. Current Oncology. 2024; 31(8):4781-4794. https://doi.org/10.3390/curroncol31080358
Chicago/Turabian StyleSolanki, Abhishek A., Kevin Zheng, Alicia N. Skipworth, Lisa M. Robin, Ryan F. Leparski, Elizabeth Henry, Matthew Rettig, Joseph K. Salama, Timothy Ritter, Jeffrey Jones, and et al. 2024. "Challenges and Opportunities in Developing an Oncology Clinical Trial Network in the United States Veterans Affairs Health Care System: The VA STARPORT Experience" Current Oncology 31, no. 8: 4781-4794. https://doi.org/10.3390/curroncol31080358
APA StyleSolanki, A. A., Zheng, K., Skipworth, A. N., Robin, L. M., Leparski, R. F., Henry, E., Rettig, M., Salama, J. K., Ritter, T., Jones, J., Quek, M., Chang, M., Block, A. M., Welsh, J. S., Kumar, A., Chao, H.-H., Chen, A. C., Shapiro, R., Bitting, R. L., ... Carlson, K., on behalf of the VA STARPORT Investigators Group. (2024). Challenges and Opportunities in Developing an Oncology Clinical Trial Network in the United States Veterans Affairs Health Care System: The VA STARPORT Experience. Current Oncology, 31(8), 4781-4794. https://doi.org/10.3390/curroncol31080358