
New Therapeutic Maneuver for Horizontal Semicircular Canal Cupulolithiasis: A Prospective Randomized Trial


Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Diagnosis of HSCC Cupulolithiasis and Lateralization
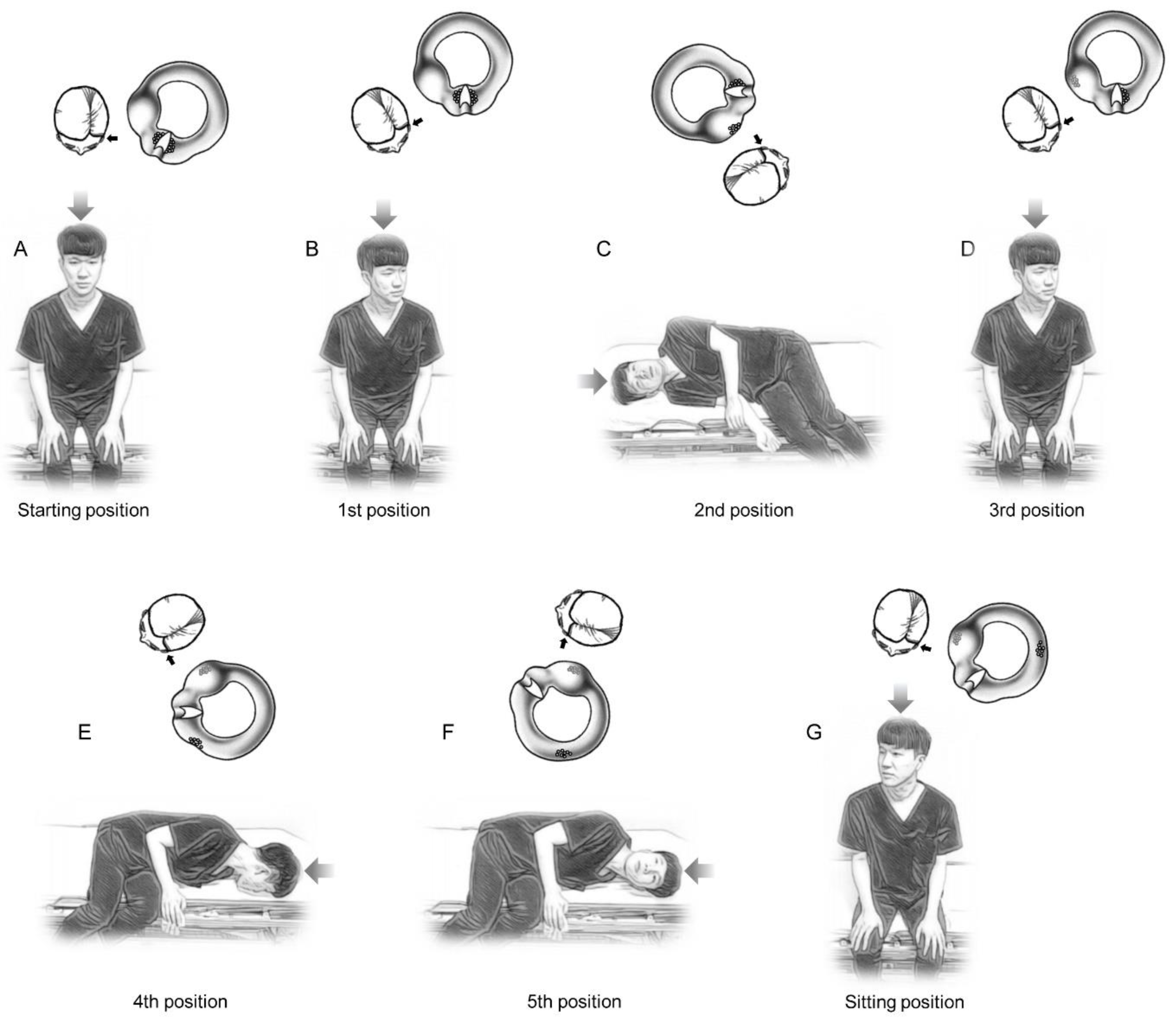
2.3. Treatment Procedures and Treatment Effects Evaluation
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
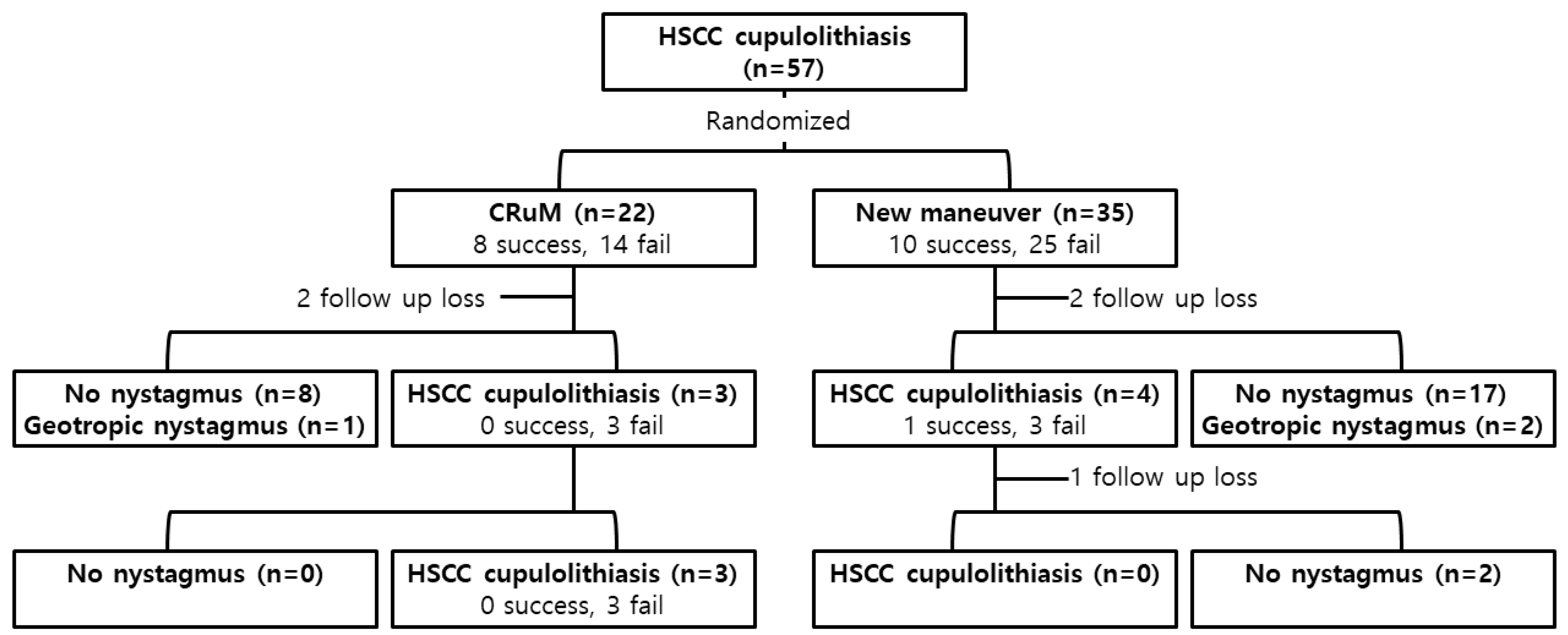
3.2. Immediate and Short-Term Treatment Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhattacharyya, N.; Gubbels, S.P.; Schwartz, S.R.; Edlow, J.A.; El-Kashlan, H.; Fife, T.; Holmberg, J.M.; Mahoney, K.; Hollingsworth, D.B.; Roberts, R.; et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol.—Head Neck Surg. 2017, 156 (Suppl. 3), S1–S47. [Google Scholar] [CrossRef]
- Yetiser, S.; Ince, D. Demographic analysis of benign paroxysmal positional vertigo as a common public health problem. Ann. Med. Health Sci. Res. 2015, 5, 50–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahm, H.; Han, K.; Shin, J.E.; Kim, C.H. Benign Paroxysmal Positional Vertigo in the Elderly: A Single-center Experience. Otol. Neurotol. 2019, 40, 1359–1362. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.Y.; Kim, J.S.; Jeong, S.H.; Oh, Y.-M.; Choi, K.-D.; Kim, B.-K.; Lee, S.-H.; Lee, H.-S.; Moon, I.-S.; Lee, J.-J. Treatment of apogeotropic benign positional vertigo: Comparison of therapeutic head-shaking and modified Semont maneuver. J. Neurol. 2009, 256, 1330–1336. [Google Scholar] [CrossRef]
- Bisdorff, A.R.; Debatisse, D. Localizing signs in positional vertigo due to lateral canal cupulolithiasis. Neurology 2001, 57, 1085–1088. [Google Scholar] [CrossRef] [PubMed]
- Ramos, B.F.; Cal, R.; Brock, C.M.; Mangabeira Albernaz, P.L.; Zuma e Maia, F. Apogeotropic variant of horizontal semicircular canal benign paroxysmal positional vertigo: Where are the particles? Audiol. Res. 2019, 9, 228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.H.; Kim, Y.G.; Shin, J.E.; Yang, Y.S.; Im, D. Lateralization of horizontal semicircular canal canalolithiasis and cupulopathy using bow and lean test and head-roll test. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3003–3009. [Google Scholar] [CrossRef]
- Koo, J.W.; Moon, I.J.; Shim, W.S.; Moon, S.Y.; Kim, J.S. Value of lying-down nystagmus in the lateralization of horizontal semicircular canal benign paroxysmal positional vertigo. Otol. Neurotol. 2006, 27, 367–371. [Google Scholar] [CrossRef]
- Kim, S.H.; Jo, S.W.; Chung, W.K.; Byeon, H.K.; Lee, W.S. A cupulolith repositioning maneuver in the treatment of horizontal canal cupulolithiasis. Auris Nasus Larynx 2012, 39, 163–168. [Google Scholar] [CrossRef]
- Yamanaka, T.; Sawai, Y.; Murai, T.; Okamoto, H.; Fujita, N.; Hosoi, H. New treatment strategy for cupulolithiasis associated with benign paroxysmal positional vertigo of the lateral canal: The head-tilt hopping exercise. Eur. Arch. Oto-Rhino-Laryngol. 2014, 271, 3155–3160. [Google Scholar] [CrossRef]
- Zuma e Maia, F. New Treatment Strategy for Apogeotropic Horizontal Canal Benign Paroxysmal Positional Vertigo. Audiol. Res. 2016, 6, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otsuka, K.; Negishi, M.; Suzuki, M.; Inagaki, T.; Yatomi, M.; Konomi, U.; Kondo, T.; Ogawa, Y. Experimental study on the aetiology of benign paroxysmal positional vertigo due to canalolithiasis: Comparison between normal and vestibular dysfunction models. J. Laryngol. Otol. 2014, 128, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Liston, D.B.; Adelstein, B.D.; Stone, L.S. Onset of positional vertigo during exposure to combined G loading and chest-to-spine vibration. Aviat. Space Environ. Med. 2014, 85, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.J.; Lee, J.W.; Kim, S.J.; Lee, C.W.; Park, H.J. Development of a murine model of traumatic benign paroxysmal positional vertigo: A preliminary study. Acta Oto-Laryngol. 2017, 137, 29–34. [Google Scholar] [CrossRef]
- Amir, I.; Young, E.; Belloso, A. Self-limiting benign paroxysmal positional vertigo following use of whole-body vibration training plate. J. Laryngol. Otol. 2010, 124, 796–798. [Google Scholar] [CrossRef]
- Lee, J.; Lee, D.H.; Noh, H.; Shin, J.E.; Kim, C.H. Immediate and short-term effects of Gufoni and Appiani liberatory maneuver for treatment of ageotropic horizontal canal benign paroxysmal positional vertigo: A prospective randomized trial. Laryngoscope Investig. Otolaryngol. 2021, 6, 832–838. [Google Scholar] [CrossRef]
- Lee, S.H.; Choi, K.D.; Jeong, S.H.; Oh, Y.M.; Koo, J.W.; Kim, J.S. Nystagmus during neck flexion in the pitch plane in benign paroxysmal positional vertigo involving the horizontal canal. J. Neurol. Sci. 2007, 256, 75–80. [Google Scholar] [CrossRef]
- Nuti, D.; Vannucchi, P.; Pagnini, P. Benign paroxysmal positional vertigo of the horizontal canal: A form of canalolithiasis with variable clinical features. J. Vestib. Res. Equilib. Orientat. 1996, 6, 173–184. [Google Scholar] [CrossRef]
- Han, B.I.; Oh, H.J.; Kim, J.S. Nystagmus while recumbent in horizontal canal benign paroxysmal positional vertigo. Neurology 2006, 66, 706–710. [Google Scholar] [CrossRef]
- Li, J.C. Mastoid oscillation: A critical factor for success in canalith repositioning procedure. Otolaryngol.—Head Neck Surg. 1995, 112, 670–675. [Google Scholar] [CrossRef]
- Ruckenstein, M.J.; Shepard, N.T. The canalith repositioning procedure with and without mastoid oscillation for the treatment of benign paroxysmal positional vertigo. ORL J. Oto-Rhino-Laryngol. Relat. Spec. 2007, 69, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Motamed, M.; Osinubi, O.; Cook, J.A. Effect of mastoid oscillation on the outcome of the canalith repositioning procedure. Laryngoscope 2004, 114, 1296–1298. [Google Scholar] [CrossRef] [PubMed]
- Macias, J.D.; Ellensohn, A.; Massingale, S.; Gerkin, R. Vibration with the canalith repositioning maneuver: A prospective randomized study to determine efficacy. Laryngoscope 2004, 114, 1011–1014. [Google Scholar] [CrossRef] [PubMed]
- Hain, T.C.; Helminski, J.O.; Reis, I.L.; Uddin, M.K. Vibration does not improve results of the canalith repositioning procedure. Arch. Otolaryngol.—Head Neck Surg. 2000, 126, 617–622. [Google Scholar] [CrossRef] [Green Version]
- Andaz, C.; Whittet, H.B.; Ludman, H. An unusual cause of benign paroxysmal positional vertigo. J. Laryngol. Otol. 1993, 107, 1153–1154. [Google Scholar] [CrossRef]
- Persichetti, P.; Di Lella, F.; Simone, P.; Marangi, G.F.; Cagli, B.; Tenna, S.; Trivelli, M. Benign paroxysmal positional vertigo: An unusual complication of rhinoplasty. Plast. Reconstr. Surg. 2004, 114, 277–278. [Google Scholar] [CrossRef]
- Chiarella, G.; Leopardi, G.; De Fazio, L.; Chiarella, R.; Cassandro, E. Benign paroxysmal positional vertigo after dental surgery. Eur. Arch. Oto-Rhino-Laryngol. 2008, 265, 119–122. [Google Scholar] [CrossRef]
- Vannucchi, P.; Libonati, G.A.; Gufoni, M. The Physical Treatment of Lateral Semicircular Canal Canalolithiasis. Audiol. Med. 2005, 3, 52–56. [Google Scholar] [CrossRef]
- Riga, M.; Korres, S.; Korres, G.; Danielides, V. Apogeotropic variant of lateral semicircular canal benign paroxysmal positional vertigo: Is there a correlation between clinical findings, underlying pathophysiologic mechanisms and the effectiveness of repositioning maneuvers? Otol. Neurotol. 2013, 34, 1155–1164. [Google Scholar] [CrossRef]
- Appiani, G.C.; Catania, G.; Gagliardi, M.; Cuiuli, G. Repositioning maneuver for the treatment of the apogeotropic variant of horizontal canal benign paroxysmal positional vertigo. Otol. Neurotol. 2005, 26, 257–260. [Google Scholar] [CrossRef]
- Califano, L.; Melillo, M.G.; Mazzone, S.; Vassallo, A. “Secondary signs of lateralization” in apogeotropic lateral canalolithiasis. Acta Otorhinolaryngol. Ital. 2010, 30, 78–86. [Google Scholar] [PubMed]
- Vannucchi, P.; Giannoni, B.; Pagnini, P. Treatment of horizontal semicircular canal benign paroxysmal positional vertigo. J. Vestib. Res. Equilib. Orientat. 1997, 7, 1–6. [Google Scholar] [CrossRef]
- Shim, D.B.; Ko, K.M.; Lee, J.H.; Park, H.J.; Song, M.H. Natural history of horizontal canal benign paroxysmal positional vertigo is truly short. J. Neurol. 2015, 262, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Imai, T.; Takeda, N.; Ito, M.; Inohara, H. Natural course of positional vertigo in patients with apogeotropic variant of horizontal canal benign paroxysmal positional vertigo. Auris Nasus Larynx 2011, 38, 2–5. [Google Scholar] [CrossRef]
- Hwang, M.; Kim, S.H.; Kang, K.W.; Lee, D.; Lee, S.Y.; Kim, M.K.; Lee, S.H. Canalith repositioning in apogeotropic horizontal canal benign paroxysmal positional vertigo: Do we need faster maneuvering? J. Neurol. Sci. 2015, 358, 183–187. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CuRM (n = 22) | New Maneuver (n = 35) | p-Value | |
|---|---|---|---|
| Age, mean ± SD | 50.8 ± 14.6 | 50.7 ± 11.9 | 0.700 † |
| Sex, male:female | 5:17 | 8:27 | 0.991 ‡ |
| Affected side, right:left | 11:11 | 12:23 | 0.239 ‡ |
| Duration of vertigo, days | 2.43 ± 6.73 | 2.86 ± 6.74 | 1.000 † |
| CuRM (n = 22) | New Maneuver (n = 35) | p Value | |
|---|---|---|---|
| Initial visit (immediate response) | |||
| Success | 8 (of 22, 36.4%) | 10 (of 35, 28.6%) | 0.538 † |
| Apogeotropic nystagmus | 14 (of 22, 63.6%) | 25 (of 35, 71.4%) | |
| First follow-up | |||
| Follow-up loss | 2 | 2 | |
| Spontaneous resolution | 9 (of 12, 75.0%) | 19 (of 23, 82.6%) | 0.670 ‡ |
| Success | 0 (of 3, 0%) | 1 (of 4, 25.0%) | |
| Apogeotropic nystagmus | 3 (of 3, 100%) | 3 (of 4, 75.0%) | |
| Second follow-up | |||
| Follow-up loss | 0 | 1 | |
| Spontaneous resolution | 0 (of 3, 0%) | 2 (of 2, 100%) | |
| Success | 0 (of 3, 0%) | N/A | |
| Apogeotropic nystagmus | 3 (of 3, 100%) | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.-H.; Park, J.Y.; Kim, T.H.; Shin, J.E.; Kim, C.-H. New Therapeutic Maneuver for Horizontal Semicircular Canal Cupulolithiasis: A Prospective Randomized Trial. J. Clin. Med. 2022, 11, 4136. https://doi.org/10.3390/jcm11144136
Lee D-H, Park JY, Kim TH, Shin JE, Kim C-H. New Therapeutic Maneuver for Horizontal Semicircular Canal Cupulolithiasis: A Prospective Randomized Trial. Journal of Clinical Medicine. 2022; 11(14):4136. https://doi.org/10.3390/jcm11144136
Chicago/Turabian StyleLee, Dong-Han, Joon Yong Park, Tae Hee Kim, Jung Eun Shin, and Chang-Hee Kim. 2022. "New Therapeutic Maneuver for Horizontal Semicircular Canal Cupulolithiasis: A Prospective Randomized Trial" Journal of Clinical Medicine 11, no. 14: 4136. https://doi.org/10.3390/jcm11144136
APA StyleLee, D.-H., Park, J. Y., Kim, T. H., Shin, J. E., & Kim, C.-H. (2022). New Therapeutic Maneuver for Horizontal Semicircular Canal Cupulolithiasis: A Prospective Randomized Trial. Journal of Clinical Medicine, 11(14), 4136. https://doi.org/10.3390/jcm11144136