

Safety and Efficacy of Buprenorphine-Naloxone in Pregnancy: A Systematic Review of the Literature


Abstract
:1. Introduction
2. Materials and Methods
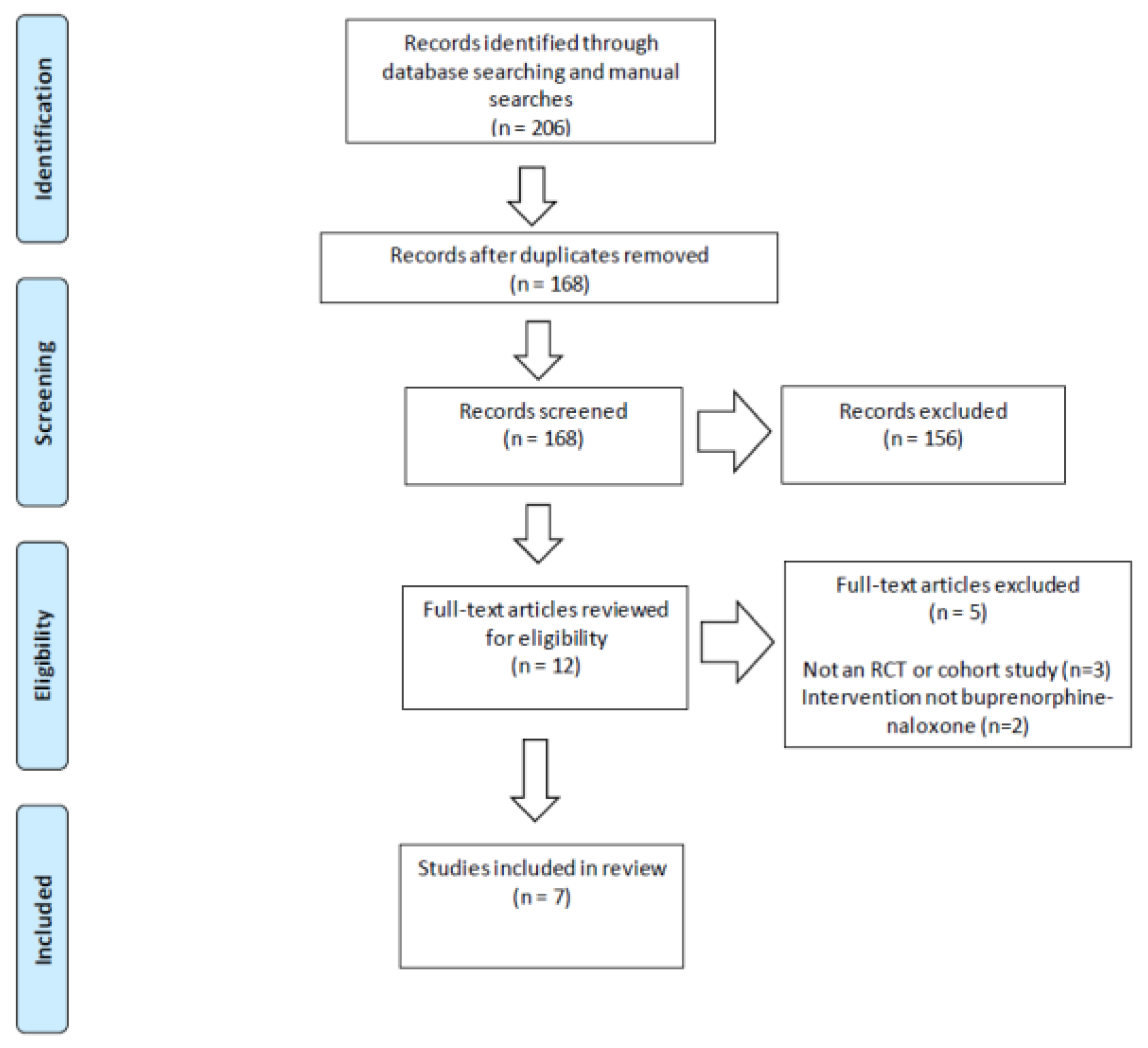
2.1. Data Sources and Study Selection
2.2. Data Extraction and Analysis
2.3. Reporting of Study Risk of Bias Assessment
3. Results
3.1. Study Characteristics
3.2. Neonatal Outcomes
3.2.1. Birth Parameters
3.2.2. Congenital Anomalies
3.2.3. Neonatal Abstinence Syndrome
3.3. Maternal Outcomes
3.4. Risk of Bias in Included Studies
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ordean, A.; Wong, S.; Graves, L. SOGC clinical practice guideline no. 349—Substance use in pregnancy. J. Obstet. Gynaecol. Can. 2017, 39, 922–937. [Google Scholar] [CrossRef] [PubMed]
- British Columbia Centre on Substance Use, B.C. Ministry of Health, B.C. Ministry of Mental Health and Addictions, & Perinatal Services BC. A Guideline for the Clinical Management of Opioid Use Disorder—Pregnancy Supplement. 2018. Available online: https://www.bccsu.ca/wp-content/uploads/2018/06/OUD-Pregnancy.pdf (accessed on 29 March 2022).
- Substance Abuse and Mental Health Services Administration. 2020 National Survey on Drug Use and Health: Detailed Tables. Table 6.20B—Types of Illicit Drug, Tobacco Product, and Alcohol Use in Past Month: Among Females Aged 15 to 44; by Pregnancy Status, Percentages, 2019 and 2020. Available online: https://www.samhsa.gov/data/report/2020-nsduh-detailed-tables (accessed on 29 March 2022).
- Hirai, A.H.; Ko, J.Y.; Owens, P.L.; Stocks, C.; Patrick, S.W. Neonatal abstinence syndrome and maternal opioid-related diagnoses in the US, 2010–2017. JAMA 2021, 325, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.E.; Kaltenbach, K.; Heil, S.H.; Stine, S.M.; Coyle, M.G.; Arria, A.M.; O’Grady, K.E.; Selby, P.; Martin, P.R.; Fischer, G. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N. Engl. J. Med. 2010, 363, 2320–2331. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.E.; Heil, S.H.; Baewert, A.; Arria, A.M.; Kaltenbach, K.; Martin, P.R.; Coyle, M.G.; Selby, P.; Stine, S.M.; Fischer, G. Buprenorphine treatment of opioid-dependent pregnant women: A comprehensive review. Addiction 2012, 107, 5–27. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Opioid use and opioid use disorder in pregnancy—Committee opinion no. 711. Obstet. Gynecol. 2017, 130, e81–e94. [Google Scholar] [CrossRef] [PubMed]
- British Columbia Centre on Substance Use and B.C. Ministry of Health. 286 A Guideline for the Clinical Management of Opioid Use Disorder. 2017. Available online: https://bccsu.ca/wp-content/uploads/2018/06/OUD-Pregnancy.pdf (accessed on 29 March 2022).
- Kampman, K.; Jarvis, M. American Society of Addiction Medicine (ASAM) national practice guideline for the use of medications in the treatment of addiction involving opioid use. J. Addict. Med. 2015, 9, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. Clinical Guidance for Treating Pregnant and Parenting Women with Opioid Use Disorder and their Infants. HHS Publication No. (SMA) 18-5054. Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2018. Available online: https://store.samhsa.gov/product/Clinical-Guidance-for-Treating-Pregnant-and-Parenting-Women-With-Opioid-Use-Disorder-and-Their-Infants/SMA18-5054 (accessed on 29 March 2022).
- World Health Organization. Guidelines for the Identification and Management of Substance Use and Substance Use Disorders in Pregnancy. World Health Organization: Geneva, Switzerland, 2014. Available online: https://www.who.int/publications/i/item/9789241548731 (accessed on 29 March 2022).
- Debelak, K.; Morrone, W.R.; O’Grady, K.E.; Jones, H.E. Buprenorphine + naloxone in the treatment of opioid dependence during pregnancy-initial patient care and outcome data. Am. J. Addict. 2013, 22, 252–254. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.; Lander, L.R.; O’Grady, K.E.; Marshalek, P.J.; Schmidt, A.; Kelly, A.K.; Jones, H.E. Treating women with opioid use disorder during pregnancy in Appalachia: Initial neonatal outcomes following buprenorphine + naloxone exposure. Am. J. Addict. 2018, 27, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Mullins, N.; Galvin, S.; Ramage, M.; Gannon, M.; Lorenz, K.; Sager, B.; Coulson, C.C. Buprenorphine and naloxone versus buprenorphine for opioid use disorder in pregnancy: A cohort study. J. Addict. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Gawronski, K.M.; Prasad, M.R.; Backes, C.R.; Lehman, K.J.; Gardner, D.K.; Cordero, L. Neonatal outcomes following in utero exposure to buprenorphine/naloxone or methadone. SAGE Open Med. 2014, 2, 2050312114530282. [Google Scholar] [CrossRef] [Green Version]
- Wiegand, S.L.; Stringer, E.M.; Stuebe, A.M.; Jones, H.; Seashore, C.; Thorp, J. Buprenorphine and naloxone compared with methadone treatment in pregnancy. Obstet. Gynecol. 2015, 125, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Dooley, J.; Gerber-Finn, L.; Antone, I.; Guilfoyle, J.; Blakelock, B.; Balfour-Boehm, J.; Hopman, W.M.; Jumah, N.; Kelly, L. Buprenorphine-naloxone use in pregnancy for treatment of opioid dependence: Retrospective cohort study of 30 patients. Can. Fam. Physician 2016, 62, e194–e200. [Google Scholar]
- Jumah, N.A.; Edwards, C.; Balfour-Boehm, J.; Loewen, K.; Dooley, J.; Gerber Finn, L.; Kelly, L. Observational study of the safety of buprenorphine+naloxone in pregnancy in a rural and remote population. BMJ Open 2016, 6, e011774. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. Congenital Anomalies in Canada 2013: A Perinatal Health Surveillance Report. Ottawa. 2013. Available online: https://publications.gc.ca/site/eng/443924/publication.html (accessed on 29 March 2022).
- Data & Statistics on Birth Defects. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/ncbddd/birthdefects/data.html (accessed on 29 March 2022).
- MacMillan, K.D.L.; Rendon, C.P.; Verma, K.; Riblet, N.; Washer, D.B.; Holmes, A.V. Association of rooming-in with outcomes for neonatal abstinence syndrome: A systematic review and meta-analysis. JAMA Pediatr. 2018, 172, 345–351. [Google Scholar] [CrossRef]
- Maremmani, I.; Gerra, G. Buprenorphine-based regimens and methadone for the medical management of opioid dependence: Selecting the appropriate drug for treatment. Am. J. Addict. 2010, 19, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Link, H.M.; Jones, H.; Miller, L.; Kaltenbach, K.; Seligman, N. Buprenorphine-naloxone use in pregnancy: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. MFM 2020, 2, 100179. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year | Setting | Number of Participants | Demographics |
|---|---|---|---|
| Debelak et al., 2013 [12] | Outpatient substance abuse and mental health facility Michigan, USA | Bup-nlx group: n = 10 8 initiated pre-pregnancy 2 initiated during first trimester No comparison group | Mean age: 26 years White: 90% High school: 60% Single: 90% |
| Dooley et al., 2016 [17] | Outpatient multidisciplinary obstetric program Ontario, Canada | Bup-nlx group: n = 30 30 initiated pre-pregnancy 5 continued for entire pregnancy Comparison groups: Other opioids n = 134 No opioids n = 476 | Mean age: 26 years Mean gravidity: 4 Mean parity: 2 Higher gravidity and parity in bup-nlx group compared to non- exposed group * |
| Gawronski et al., 2014 [15] | Academic medical center Ohio, USA | Bup-nlx group: n = 58 Comparison group: Methadone n = 92 | Mean age: 27 years White: 95% High school: 31% No significant differences between groups |
| Jumah et al., 2016 [18] | Community-based outpatient Treatment program Ontario, Canada | Bup-nlx group: n = 62 51 initiated pre-pregnancy 11 initiated during pregnancy 48 switched to monoproduct Comparison groups: Illicit opioids n = 159 No opioids n = 618 | Mean age: 26 years Mean gravidity: 4 Indigenous: 85% High school: 16% Higher gravidity in bup-nlx group compared to non-exposed group * |
| Mullins et al., 2020 [14] | Community-based perinatal substance use disorders program North Carolina, USA | Bup-nlx group: n = 85 Comparison group: Bup-monoproduct: n = 108 | Mean age: 28 years White: 89% Primiparous: 26% No significant differences between groups |
| Nguyen et al., 2018 [13] | Outpatient treatment program For pregnant women with opioid use disorder West Virginia, USA | Bup-nlx group: n = 26 No comparison group | Mean age: 28 years White: 89% Single: 60% Mean parity: 2 |
| Wiegand et al., 2015 [16] | Residential and outpatient women’s substance use disorder treatment program North Carolina, USA | Bup-nlx group: n = 31 Comparison group: Methadone n = 31 | Mean age: 27 years White: 81% Single: 87% Mean high school educated Primiparous: 26% No significant differences between groups |
| Study | Birth Parameters | Neonatal Abstinence Syndrome (NAS) Outcomes | Significant Differences |
|---|---|---|---|
| Debelak [12] | Mean GA: 38 weeks Mean HC: 33 cm Mean length: 46 cm Mean BW: 2816 g | NAS requiring pharmacotherapy: 40% Mean duration of NAS treatment: 7 days Mean hospital LOS: 10 days | No comparison group |
| Dooley [17] | Mean GA: 39 weeks Mean BW: 3569 g | NAS requiring pharmacotherapy: 0% | Higher BW in bup-nlx group compared to other opioids group * |
| Gawronski [15] | Mean GA: 38 weeks Mean HC: 33 cm Mean length: 49 cm Mean BW: 2905 g | NAS requiring pharmacotherapy: 64% Mean duration of NAS treatment: 32 days Mean hospital LOS: 9 days | Lower rate of NAS requiring pharmacotherapy in bup-nlx group than in methadone group * |
| Jumah [18] | Mean GA: 39 weeks Mean BW: 3541 g | NAS requiring pharmacotherapy: 2% | Higher BW in bup-nlx group compared to illicit opioids group * |
| Mullins [14] | Mean GA: 39 weeks Mean HC: 36 cm Mean length: 45 cm Mean BW: 2700 g | NAS requiring pharmacotherapy: 35% Median duration of NAS treatment: 9 days Median hospital LOS: 6 days | No significant differences |
| Nguyen [13] | Mean GA: 37 weeks Mean HC: 35 cm Mean length: 45 cm Mean BW: 2700 g | NAS requiring pharmacotherapy: 19% Mean hospital LOS: 16 days | No comparison group |
| Wiegand [16] | Mean GA: 40 weeks Mean HC: 34 cm Mean length: 50 cm Mean BW: 3175 g | NAS requiring pharmacotherapy: 25% Mean duration of NAS treatment: 11 days Mean hospital LOS: 6 days | Higher GA at delivery, lower rates of NAS requiring pharmacotherapy and shorter LOS in bup-nlx group compared to methadone group |
| Study | Buprenorphine-Naloxone Group Outcomes | Significant Differences |
|---|---|---|
| Debelak [12] | Bup-nlx dose 1: 8–16 mg UDS pos for illicit drugs 2: 0% | No comparison group |
| Dooley [17] | Quit illicit opioid use: 80% Reduced illicit opioid use: 10% | Higher rate of illicit opioid cessation in bup-nlx group compared to illicit opioid group * |
| Gawronski [15] | Mean bup-nlx dose: 20 mg UDS pos for illicit drugs: 47% | Higher rate of pos UDS in bup-nlx group compared to methadone group * |
| Jumah [18] | Mean bup-nlx dose: 8 mg Prenatal opioid use: 18% | Lower rate of daily prenatal opioid use in bup-nlx group compared to illicit opioid group * |
| Mullins [14] | Median bup-nlx dose: 12 mg UDS pos for illicit drugs: 55% | Lower median dose in bup-nlx group compared to bup-monoproduct group * |
| Nguyen [13] | UDS pos for illicit drugs: 35% | No comparison group |
| Wiegand [16] | Mean bup-nlx dose: 14 mg UDS pos for illicit drugs: 20% | No significant differences |
| Study | Confound-ing | Selection Bias | Classification of Interventions | Deviations from Intended Interventions | Missing Data | Measure-ment of Outcomes | Selection of Reported Results |
|---|---|---|---|---|---|---|---|
| Debelak et al. [12] | Low | Low | Low | Low | Low | Low | Low |
| Dooley et al. [17] | Moderate | Low | Moderate | Low | Low | Low | Low |
| Gawronski et al. [15] | Moderate | Low | Moderate | Low | Low | Low | Low |
| Jumah et al. [18] | Moderate | Low | Moderate | Low | Low | Low | Low |
| Mullins et al. [14] | Low | Moderate | Low | Low | Low | Low | Low |
| Nguyen et al. [13] | Low | Low | Low | Low | Low | Low | Low |
| Wiegand et al. [16] | Low | Low | Low | Low | Low | Low | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ordean, A.; Tubman-Broeren, M. Safety and Efficacy of Buprenorphine-Naloxone in Pregnancy: A Systematic Review of the Literature. Pathophysiology 2023, 30, 27-36. https://doi.org/10.3390/pathophysiology30010004
Ordean A, Tubman-Broeren M. Safety and Efficacy of Buprenorphine-Naloxone in Pregnancy: A Systematic Review of the Literature. Pathophysiology. 2023; 30(1):27-36. https://doi.org/10.3390/pathophysiology30010004
Chicago/Turabian StyleOrdean, Alice, and Meara Tubman-Broeren. 2023. "Safety and Efficacy of Buprenorphine-Naloxone in Pregnancy: A Systematic Review of the Literature" Pathophysiology 30, no. 1: 27-36. https://doi.org/10.3390/pathophysiology30010004
APA StyleOrdean, A., & Tubman-Broeren, M. (2023). Safety and Efficacy of Buprenorphine-Naloxone in Pregnancy: A Systematic Review of the Literature. Pathophysiology, 30(1), 27-36. https://doi.org/10.3390/pathophysiology30010004