1. Introduction
The Kyoto Protocol [
1] established a long-term strategy to reduce energy consumption and CO
2 emissions in buildings by 20% when compared to 1990, among others. The complexity of some of the objectives stated led to the development of a common European framework to promote energy efficiency and meet the 2020 Horizon Agenda established through European Directive 2012/27/EU [
2], and subsequent legislation [
3]. Moreover, in order to combat and mitigate the effects of global warning, the European Commission has presented a strategy to reduce heating and cooling energy in the residential and service sectors [
4], with the long-term objective of decarbonising the building stock by 2050 [
5]. To date, the necessary reduction of energy consumption in the building sector has focused particularly on retrofitting housing buildings. However, priority should also be given to hospital buildings, which account for 7% of the building area in EU27 countries, together with Norway and Switzerland, as well as for the consumption of 10% of final energy use in non- residential buildings in Europe [
6]. According to Papadopoulos [
7], the energy demand of hospital buildings is among the highest for non-residential buildings. In Spanish hospitals, the average annual energy consumption is around 20% of the total consumption in the tertiary sector [
8].
The indoor environments of hospital buildings are highly demanding, with ambient parameters that are highly dependent on use patterns, activities and specific sanitary purposes. As a result, guaranteeing adequate comfort conditions becomes a more important and pressing issue than energy consumption [
9] since it is one of the crucial factors for healing environments [
10]. Healthcare built environments can have a significant impact on health outcomes: improving patients’ moods [
11]; reducing errors and infections [
12] and enhancing control [
13]. Lighting plays a major part, in addition to the noise, colour and temperature conditions of these built environments.
Patients’ rooms usually have high window-to-wall ratios that enhance daylighting parameters and result in visual comfort and energy savings. However, in climates such as that of the Mediterranean area, the benefits of daylight provided by large windows can be substantially penalized due to high solar radiation levels, which can lead to thermal and visual discomfort. In these conditions overheating problems [
14] can also occur, leading to high cooling energy consumption as well as high daylight levels and glare [
15]. Blinds and shutters are normally used to resolve this, with users regulating and controlling solar radiation conditions, reducing indoor natural illuminance levels and increasing use of artificial lighting systems.
Moreover, inadequate use of rolling shutters may darken the room to the detriment of health and wellbeing. Choi et al. [
16] identified a significant relationship between indoor daylight environments and a patient’s average length of stay in a hospital room. The authors found that, in addition to the seasonal weather factor, indoor illuminance and luminance ratio can potentially influence the design of healing environments in hospitals. Benedetti et al. [
17] highlight the antidepressant effect of daylighting on occupants and conclude that direct exposure to natural sunlight has therapeutic effects on patients, reducing the average hospital stay. Meanwhile, Raanaas et al. [
18] report the beneficial aspects of having views through the windows as opposed to partially or totally blocked views, since this helps to alleviate stress and shorten patients’ stays.
In contrast to other improvements generally used for energy saving in buildings, such as innovative technologies or renewable sources [
19], the use of simple energy saving techniques reduces the primary energy consumed in a hospital building [
20]. However, as pointed out by Durmisevic and Ciftcioglu [
21], the complexity of hospital buildings makes it difficult to adopt a holistic approach to the different environmental features. For this reason, daylighting conditions, indoor illuminance levels and visibility from the room to the outside should be key considerations for work on the energy retrofitting of hospitals.
The first action strategy should focus on window aperture, given that it is the weakest element of the energy envelope and highly conditions indoor illuminance levels. Authors such as Fernández et al. [
22] implement a computational optimization method to establish optimal openings based on the hourly sky conditions of a whole year. Given the complexity of reducing the configuration of the windows in existing buildings, one of the most common solutions is the addition of external shading devices [
23] to improve indoor ambient conditions [
24]. However, these devices can affect the external appearance of the building and also obstruct views depending on the building typology.
In this context, several studies have proposed advanced solar control solutions [
25]. The implementation of effective energy and low-cost solutions in retrofitting should not condition the use of the building. One of the possible solutions to be applied to existing glazing surfaces is the application of solar control films, reflective materials that reduce solar heat gains, as stated by Lampert [
26].
Depending on their composition, solar control films modify the thermal and optical properties of glazing surfaces, decreasing both the solar factor and light transmittance [
27]. Their physical properties have been determined using theoretical models, such as that proposed by ASHRAE [
28], through testing [
29] or with mathematical models [
30]. Mostly, these elements are presented with thermal insulation functions [
31], and are evaluated with building energy simulation tools.
This use of solar control films leads to a reduction in solar radiation, as already concluded through on-site measurements in an air-conditioned office building by Li et al. [
32]. This reduction in solar radiation is reflected in lower cooling energy consumption, as well as in daylight, and is affected by reduced visible transmittance. Yin et al. [
33] used simulation tools to analyse this in two commercial buildings in Shanghai, while Xamán et al. [
34] present a thermal analysis of natural convection of a double glazing unit in a warm climate. It was established that the optimal separation distance between the glass sheets was ≥6.0 cm, and the use of solar control film was highly recommended, as energy gains were reduced by 55%.
The study by Moretti and Belloni [
35] is one of the few analysing daylight performance in existing glazed offices, with and without solar control films. Using a full-scale experimental set-up and numerical analysis, they established that the use of a solar control film reduces incoming solar radiation by 60%, cooling energy demand by around 29% and daily illuminance levels by 59%.
The beneficial reduction in cooling loads and consumption due to the use of solar control films is clear. In addition, the financial costs of retrofitting processes are significantly low. However, their use does result in some uncertainty regarding the penalization of daylight illuminance, and electric consumption of the artificial lighting system.
The main aim of this paper is to evaluate a solar control film installed on windows, analysing its influence on the natural illuminance conditions and artificial lighting consumption in a hospital room in a Mediterranean climate. In order to do so, a room was monitored for a whole year, with and without solar control film, considering real operation and use conditions. Indoor illuminance levels (lux) and lighting consumption (kWh) have been analysed and found to be greatly influenced by the percentage of user-controlled rolling shutter aperture.
The structure of the results of this paper is as follows:
Section 2 refers to the methodology used, describing the case study (
Section 2.1), the monitoring system (
Section 2.2), the characteristics of the window and solar control film considered (
Section 2.3) and the monitoring periods analysed (
Section 2.4). Given that the monitoring system does not record data on energy demand, this analysis has been complemented with an energy simulation model to evaluate cooling and heating demand (kWh), both with and without solar film. The energy modelling phase is explained in
Section 2.5. The results obtained in this study are incorporated into
Section 3 through several analyses: general illuminance levels (
Section 3.1), natural illuminance considering the distance from the window (
Section 3.2), electric light consumption (
Section 3.3) and cooling/heating energy demand (
Section 3.4). The strengths and limitations of this research have also been stated (
Section 3.5). Finally, the conclusions are reported in
Section 4.
2. Methodology
The methodology followed consists of on-site monitoring, measuring several ambient variables in a hospital room in southern Spain, considering real use conditions. Given functional restrictions imposed by the hospital personnel, it was not possible to conduct a simultaneous analysis of two hospital rooms in order to evaluate the real influence of the solar film installed. Hence, only one room was analysed and monitored for more than 12 months, structuring the study into two temporal phases. In the first stage, from July 2016 to May 2017, the room was monitored with no additional solar protection other than the rolling shutters installed in the original construction. In the second phase, from June 2017 to June 2018, the same room was monitored, this time considering a solar protection film on the external glazing surface, complementing the existing rolling shutters.
This paper focuses mainly on the analysis of the lighting results obtained in both phases: with and without solar protection film. A descriptive statistical analysis was carried out on natural illuminance levels and the electric consumption of the artificial lighting system using the Statistic Toolbox of Matlab (R2017a) [
36]. Monitored data were subsequently processed and filtered using Excel 2016 ® [
37]. In addition, in order to assess cooling and heating energy demand in the room with and without solar protection film, an energy simulation model was constructed, using Design Builder (v. 4.7.0.027), recognized by the US DOE [
38], as an interface to EnergyPlus [
39].
2.1. Description of Case Study
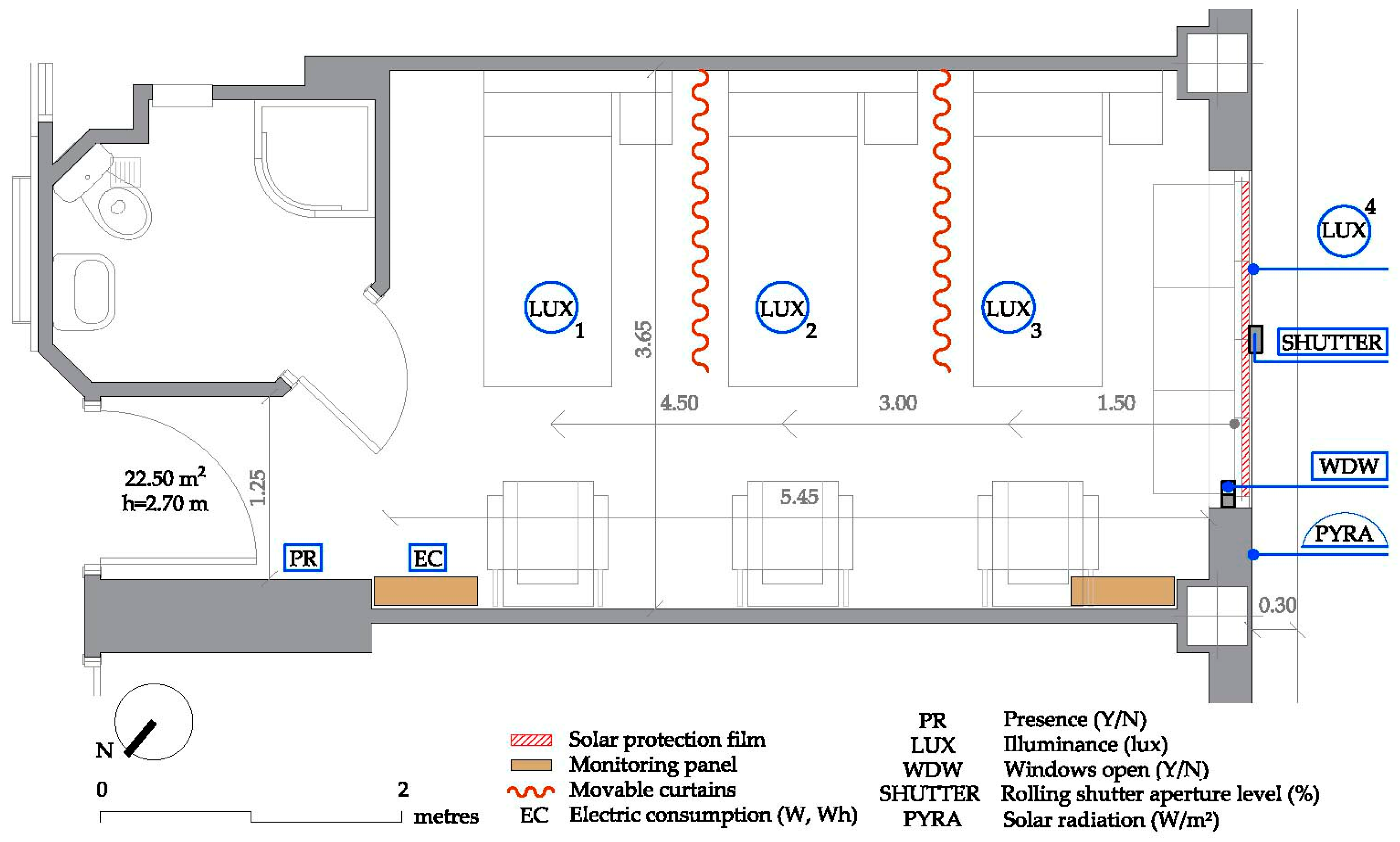
The room monitored is located in the public Virgen Macarena University Hospital, built in 1974 in the city of Seville, in southern Spain, with a Mediterranean climate: latitude 37.25° N and longitude −5.60° W. The 3.65 m wide and 5.45 m deep room is on the fifth floor of the southeast wing of the building. With a total useful area of 22.50 m
2 and a clearance height of 2.70 m, it has three patients’ beds with individual floor-to-ceiling curtains between them to ensure privacy and three armchairs for possible companions (
Figure 1).
As regards the artificial lighting system, the room has three linear luminaires with 18 W fluorescent lamps, one above each headboard. In addition, there is a downlight in the entrance area to the room, with two 18 W low energy consumption bulbs. Each of these luminaires can be controlled individually by users, their companions or hospital personnel.
2.2. Monitoring System
The monitoring system (
Figure 2), installed following EN ISO 7726:2001 [
40], records data at 10-min intervals using several data loggers placed inside two monitoring panels in the room.
These data loggers store information every 30 min, uploading it to a file transfer protocol (FTP) server through a static IP using a mobile card. The first data logger saves information on the electric consumption of the lighting system, storing data on voltage (V), power consumption (W) and electric current (A). The second data logger is connected to a detection sensor and four sensors that control the window opening (Y or open/N or closed). The third incorporates an outdoor pyranometer (placed vertically and parallel to the facade line), one sensor that measures the rolling shutter aperture level and four luxmeters (three indoors and one outdoors). The three indoor luxmeters are at distances of 1.5 m, 3.0 m and 4.5 m from the window whereas the outdoor luxmeter is placed on the external facade line.
Data recorded by the monitoring system is complemented with information from a weather station in Test Cells 3.5 km from the hospital, managed by the research team [
41]. The outdoor ambient conditions measured by this station are used in this paper for the outdoor air temperatures.
Table 1 shows the main technical characteristics of the sensors used in the hospital room and weather station. Further information about the monitoring system is available in previous research conducted in the building analysed [
42], which evaluates the influence of a shading system (an egg-crate device) installed on the window exterior.
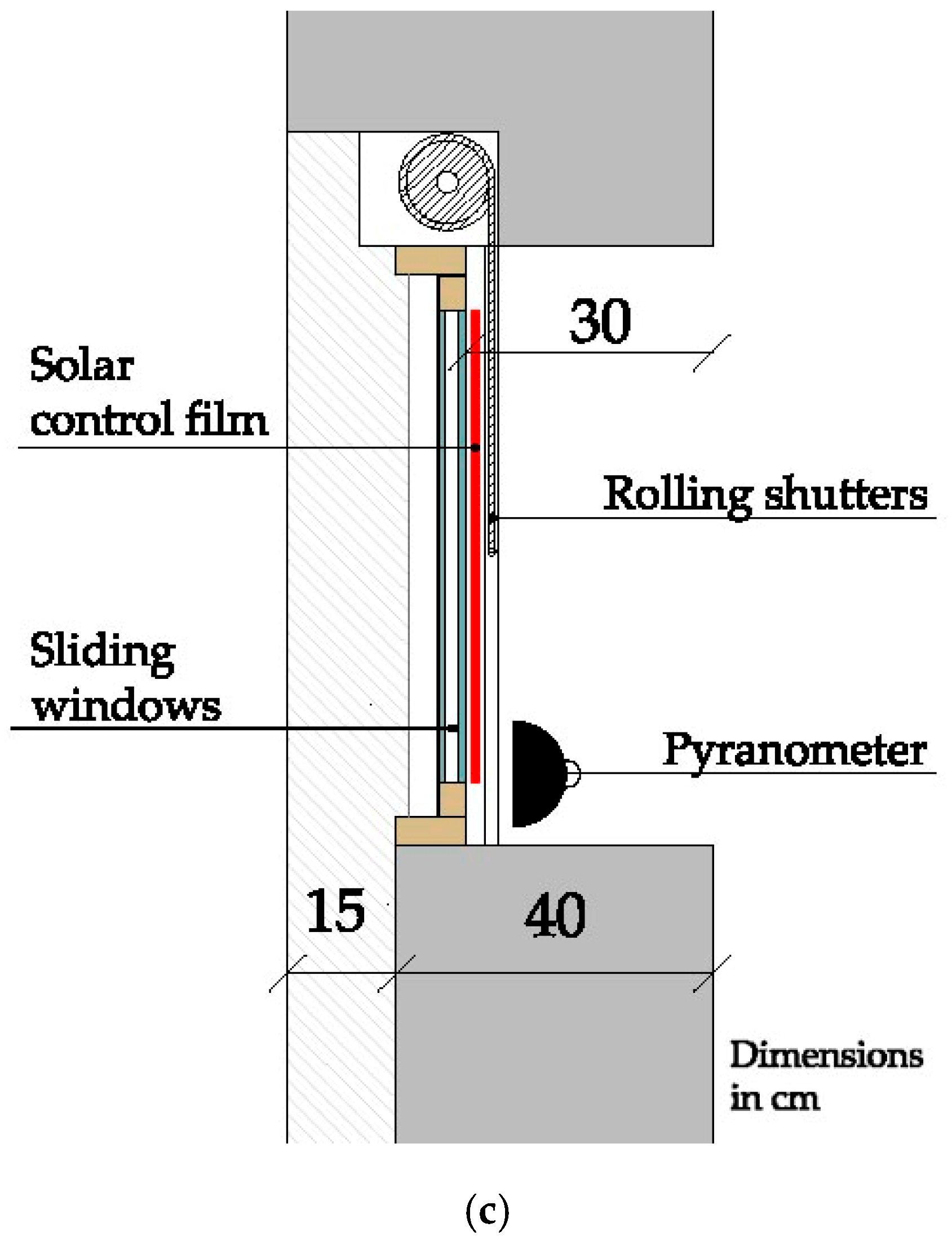
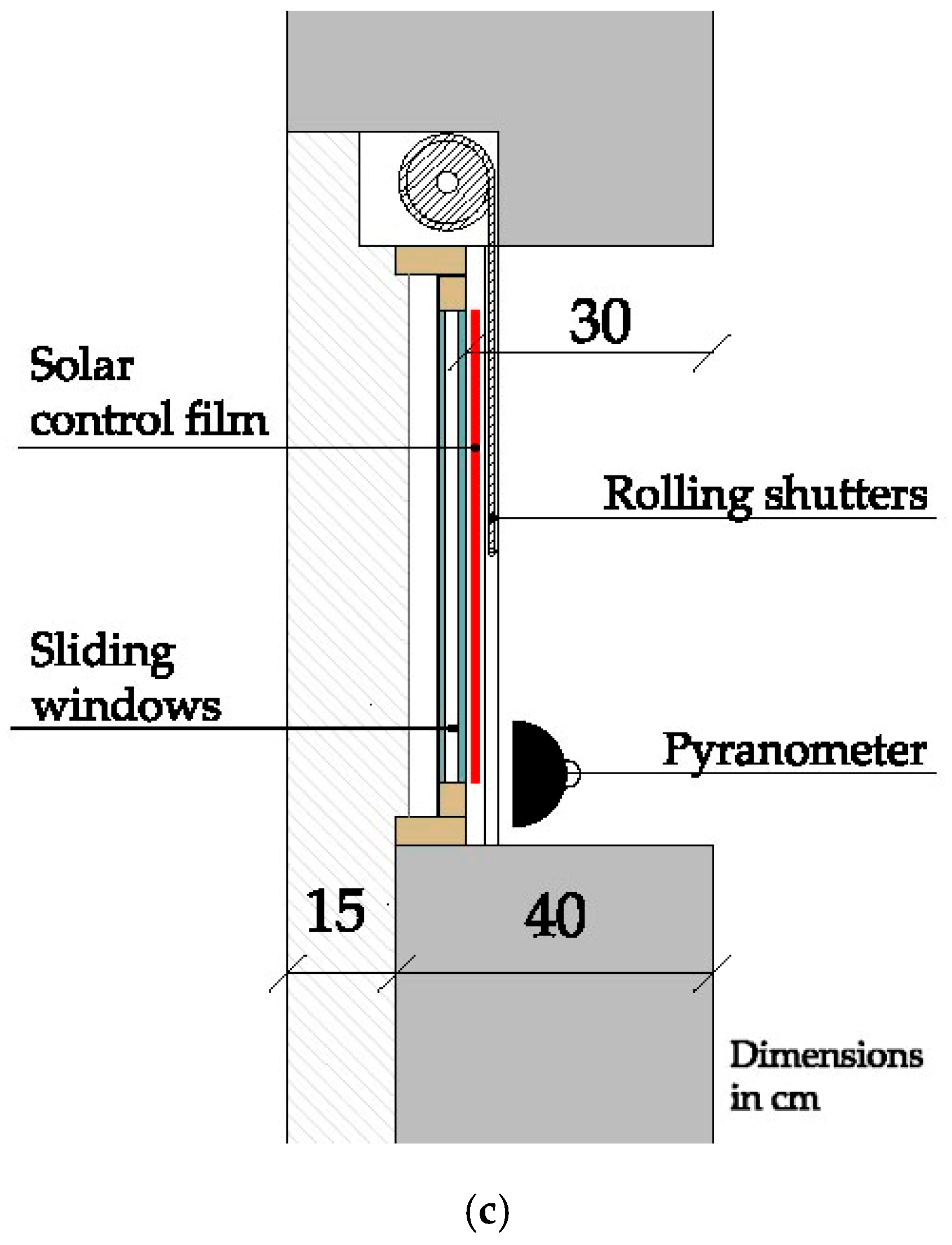
2.3. Window and Solar Protection Film Description
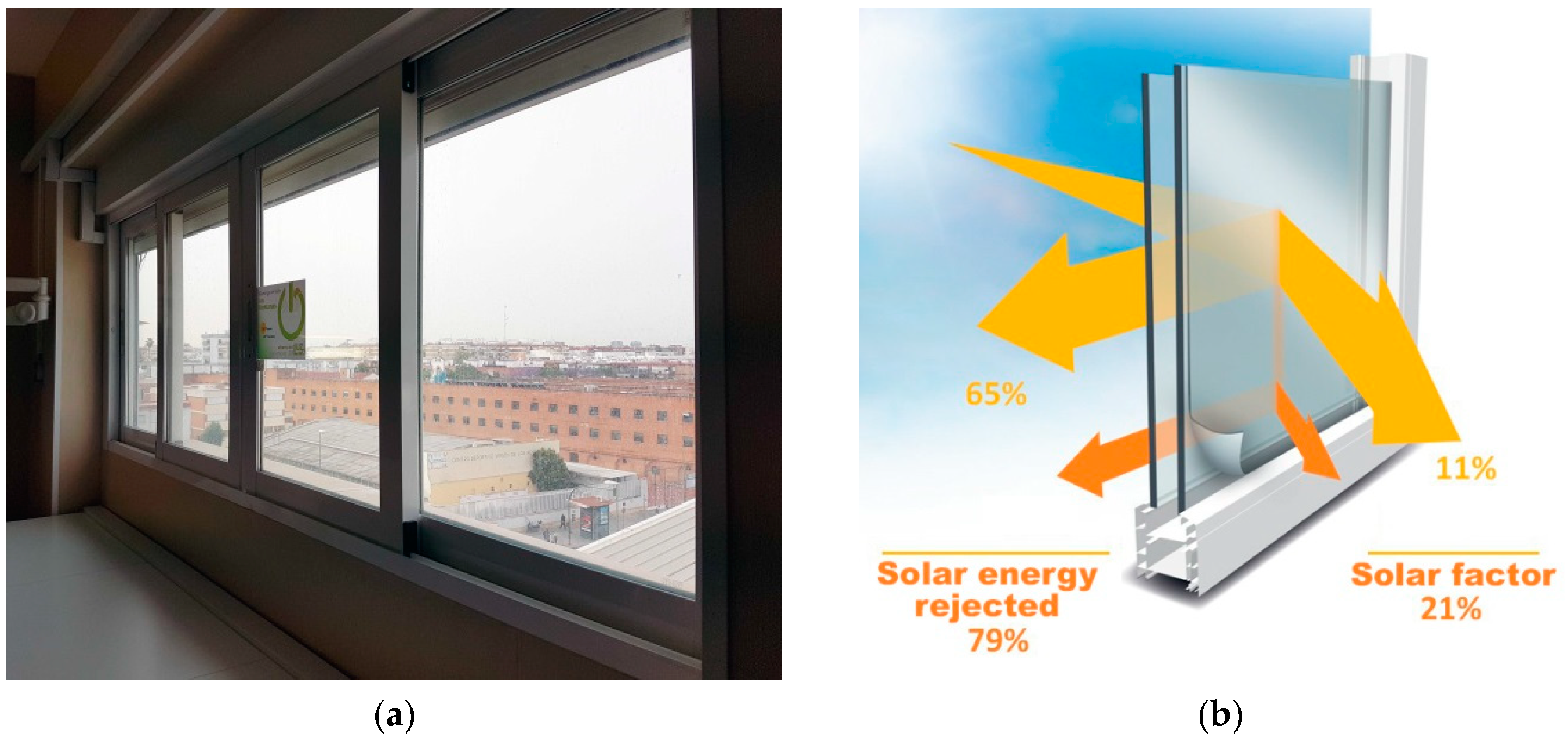
The analysed room includes a 0.85 m × 2.30 m south-oriented sliding window with an aluminium frame, facing the room entrance (
Figure 3a). This window represents around 20% of the facade surface in the room and is set back 0.30 m from the external facade line, creating a continuous cantilevered lintel.
In the second phase of the analysis, a solar protection film was installed on the external surface of the window (
Figure 3b). The thermal and solar characteristics of the window and glazing surface, provided by the manufacturer [
43], are shown in
Table 2.
The original room also has an external shading system of polyvinyl chloride (PVC) slatted rolling shutters with horizontal slats (
Figure 3c). These rolling shutters have no shading control to gradually darken the room. They consist of an ON-OFF element made of horizontal slats (with no gaps in between) that darken the room by sliding them down.
2.4. Monitoring Phases
Given that a simultaneous analysis of two hospital rooms for the evaluation of the real influence of the solar film was not possible, the following aspects were considered in the analysis of the results obtained in this research:
It is important to highlight that, according to the information provided by hospital personnel, the room was occupied throughout the entire monitoring period. This has been confirmed by the data monitored by the presence detector.
2.5. Energy Simulation Model
For the construction of an energy simulation model to assess energy demand in the room, data shown in
Table 4 was used, as with
Table 2 above. Simulations for both cases were carried out with an occupancy rate of 0.5 people/m
2 and a schedule of 50% use, except from 16:00 to 19:00 (visiting hours), where 100% use was considered. Since no real data was provided by the hospital personnel, for the lighting system, internal gains of 4.80 W/m
2 during 12 h per day were assumed, according to the Spanish Technical Building Code [
44]. Calculations considered a metabolic rate of 1.0 met and a thermal resistance of 0.5 clo in summer and 1.0 clo in winter.
The composition of the facade is: 0.015 m exterior mortar rendering, 0.115 m perforated brick wall, 0.015 m interior mortar rendering, 0.07 m non-ventilated air chamber, 0.06 m partition brick wall and 0.015 m gypsum plaster (U = 1.32 W/m2·K). That of the partition wall is: 0.015 m gypsum plaster, 0.07 m partition brick wall and 0.015 m gypsum plaster (U = 1.92 W/ m2·K). Finally, the composition of the intermediate floor/ceiling is: 0.02 m artificial stone floor, 0.025 m mortar rendering, 0.30 m ceramic beam filling pieces and 0.015 m gypsum plaster (U = 1.29 W/ m2·K).
Moreover, the fact that the mechanical ventilation system of the hospital building is always ON has been taken into consideration. In addition, running operative temperatures of the HVAC system are set at 24 °C (for heating) and 25 °C (for cooling) by the hospital personnel.
Energy simulation was also used to evaluate the real influence of the 0.30 m existing cantilever on the facade on the energy demand of both cases (with and without solar protection film).
3. Analysis of Results
The lighting results obtained in the comparison of the room without solar film and with protection film are presented below. For the sake of clarity, this section has been subdivided into three sections. The first is a statistical analysis of the illuminance levels registered in each seasonal period. The second section provides a more precise analysis of the natural illuminance levels, considering the distance between measurement points and window. Finally, the third section presents the results of the electric consumption of the artificial lighting system.
3.1. Statistical Analysis of Illuminance Levels.
A descriptive statistical analysis of the use of the artificial lighting system was conducted to compare the cases of the room with solar film and the room without protection film (
Table 5).
The percentages of hours (%) in which the artificial lighting system is turned ON was studied, along with the rolling shutter aperture levels (%) recorded in those moments. Similarly, rolling shutter aperture levels were also analysed when natural illuminance was considered. It should be noted that the rolling shutter aperture level refers to % open, so a rolling shutter aperture level of 100% means that rolling shutters are fully open.
This analysis is completed with the percentage of hours (%) with natural illuminance levels (when there was no electric lighting consumption), which have been classified according to different illuminance ranges (lux). In this last case, only illuminance levels recorded by the luxmeter closest to the window were studied in order to reduce uncertainties derived from the use of the individual curtains. This minimized the influence relating to the occupancy of the room. In addition, only outdoor illuminance levels equal to and above 10 klux were analysed in all cases. Therefore, daily hours with ambient conditions similar to clear sky have been considered.
As the table shows, the artificial lighting system is activated during all the seasonal periods analysed and around 50% of the total hours (with a higher percentage of hours in the room without solar film). The sole exception is summer: the percentage of hours with artificial lighting is only 12.3% in the room with no solar film. In contrast, this increases to 63.2% of hours with artificial lighting in the room with solar protection film.
Rolling shutter aperture levels do not present a clear pattern when compared to other variables, since users turn ON the artificial lighting when there are low or high rolling shutter aperture levels. In other words, there is no clear performance pattern, with a 95% confidence level, between rolling shutter aperture levels and the activation of the artificial lighting system. The same conclusion is reported when the seasonal period is considered.
With regard to indoor illuminance, the values recorded for a large fraction of the hours are above 300 lux, with higher levels in the room without solar film, especially in winter. It should be stressed that there is a higher percentage of hours with illuminance levels between 100 and 300 lux in the room with solar film in all periods analysed.
Figure 4,
Figure 5 and
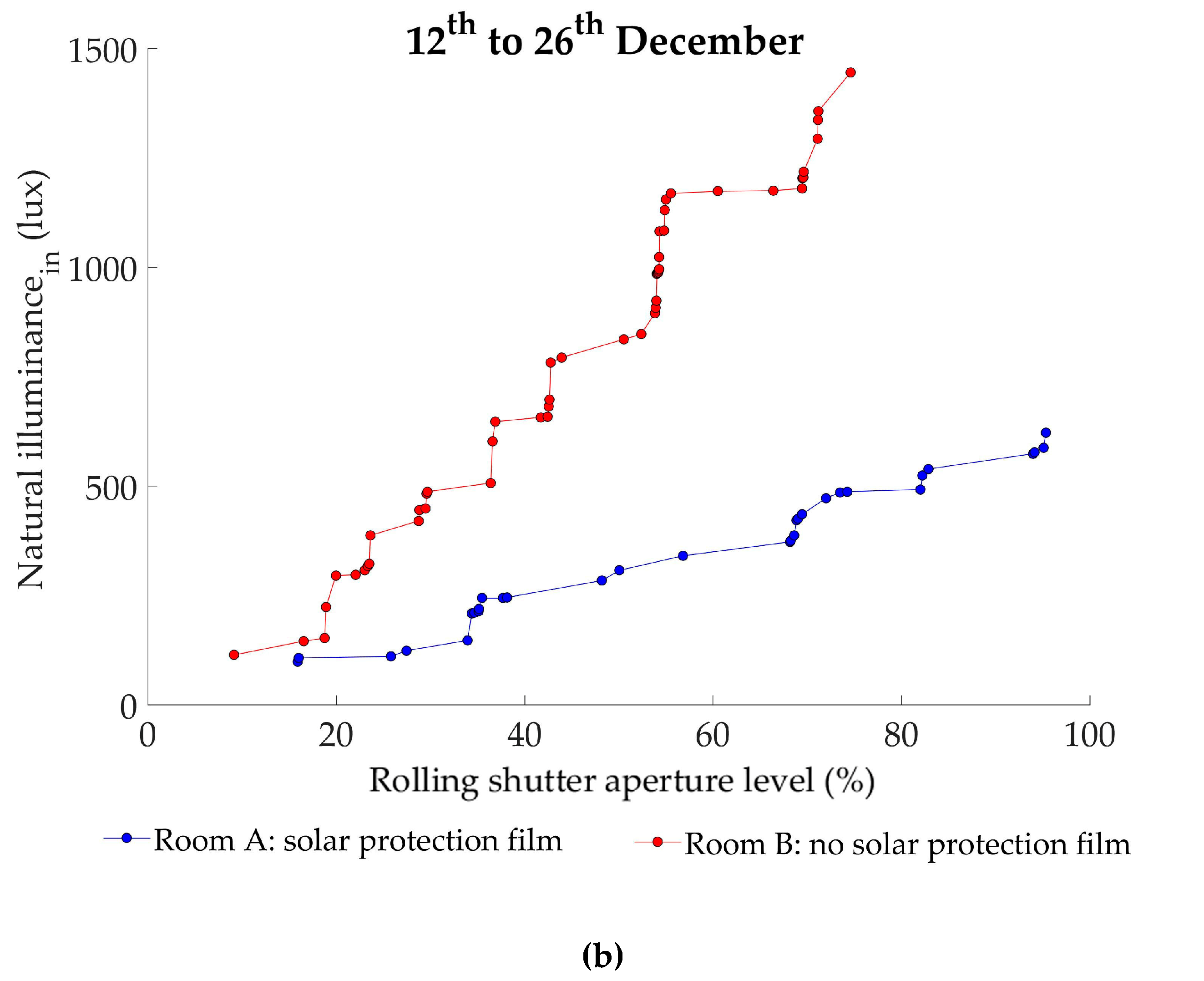
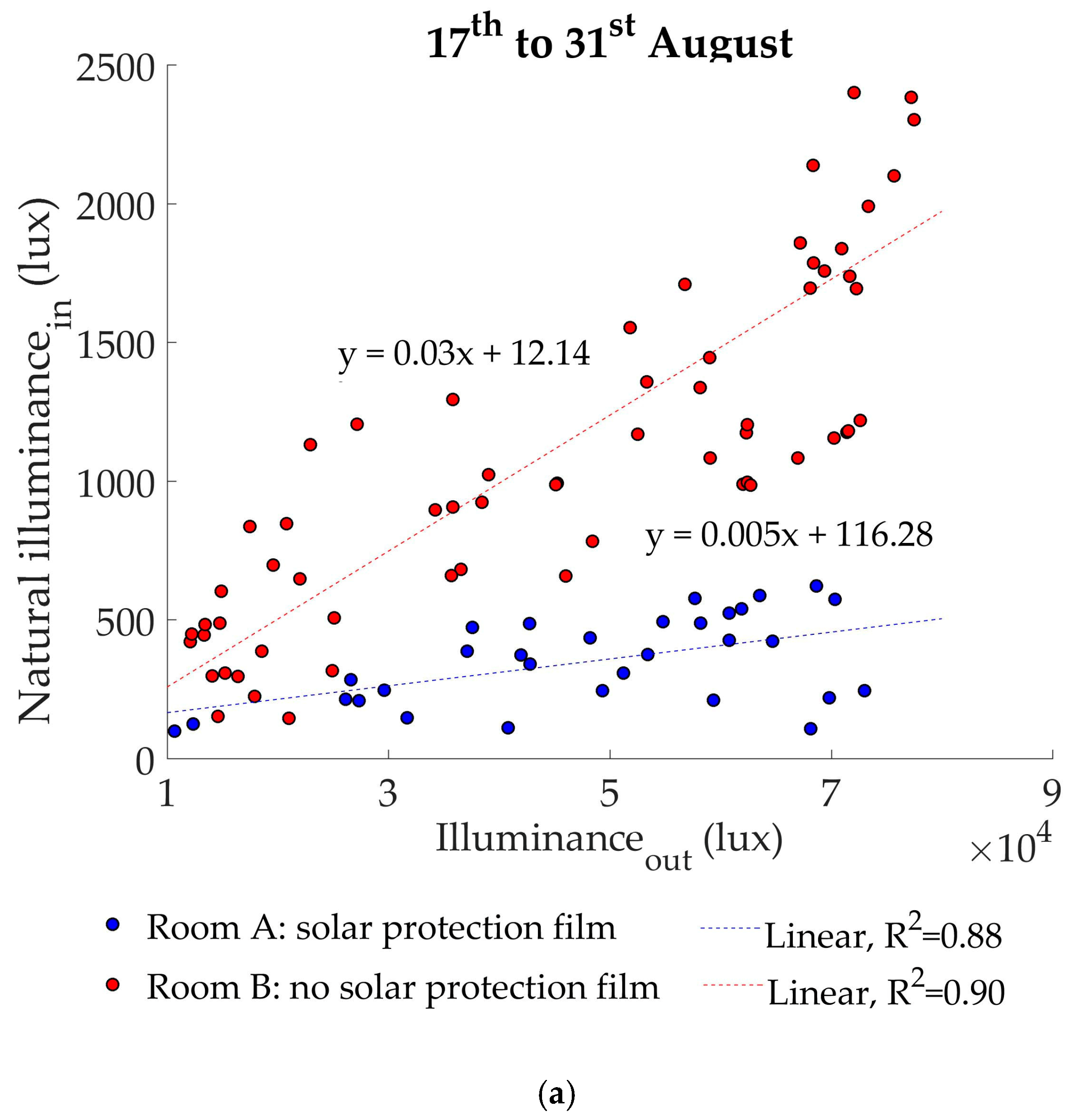
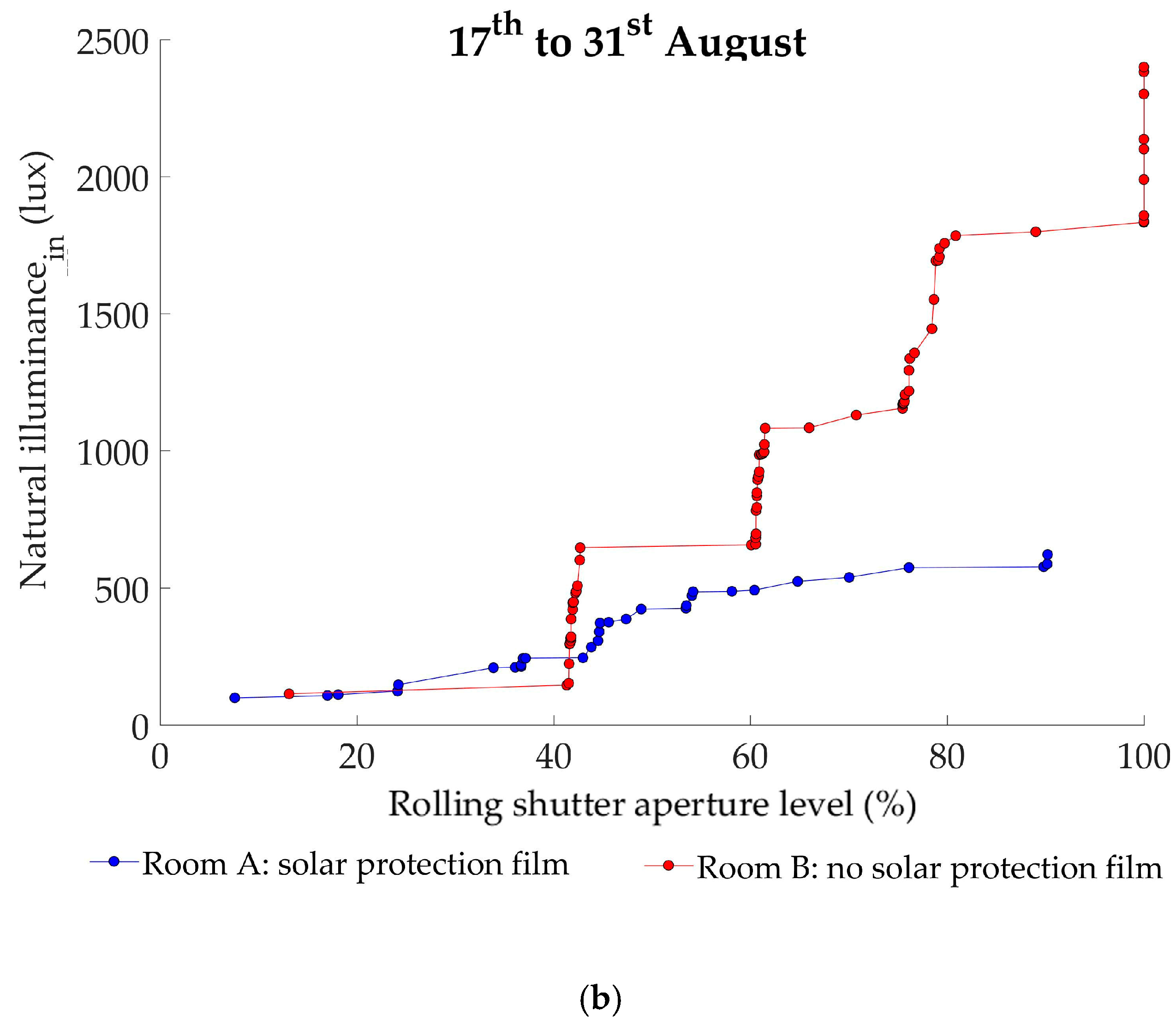
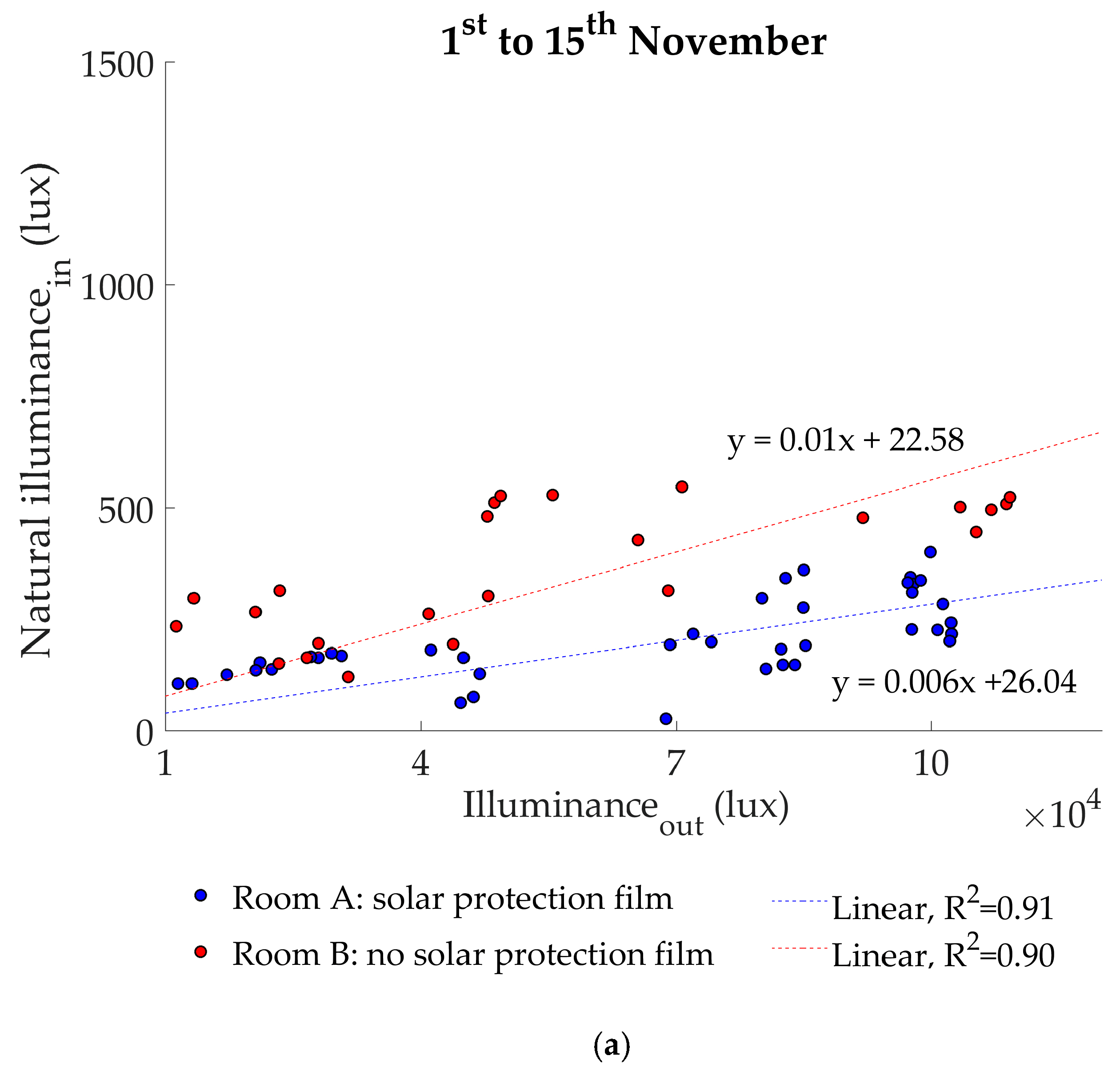
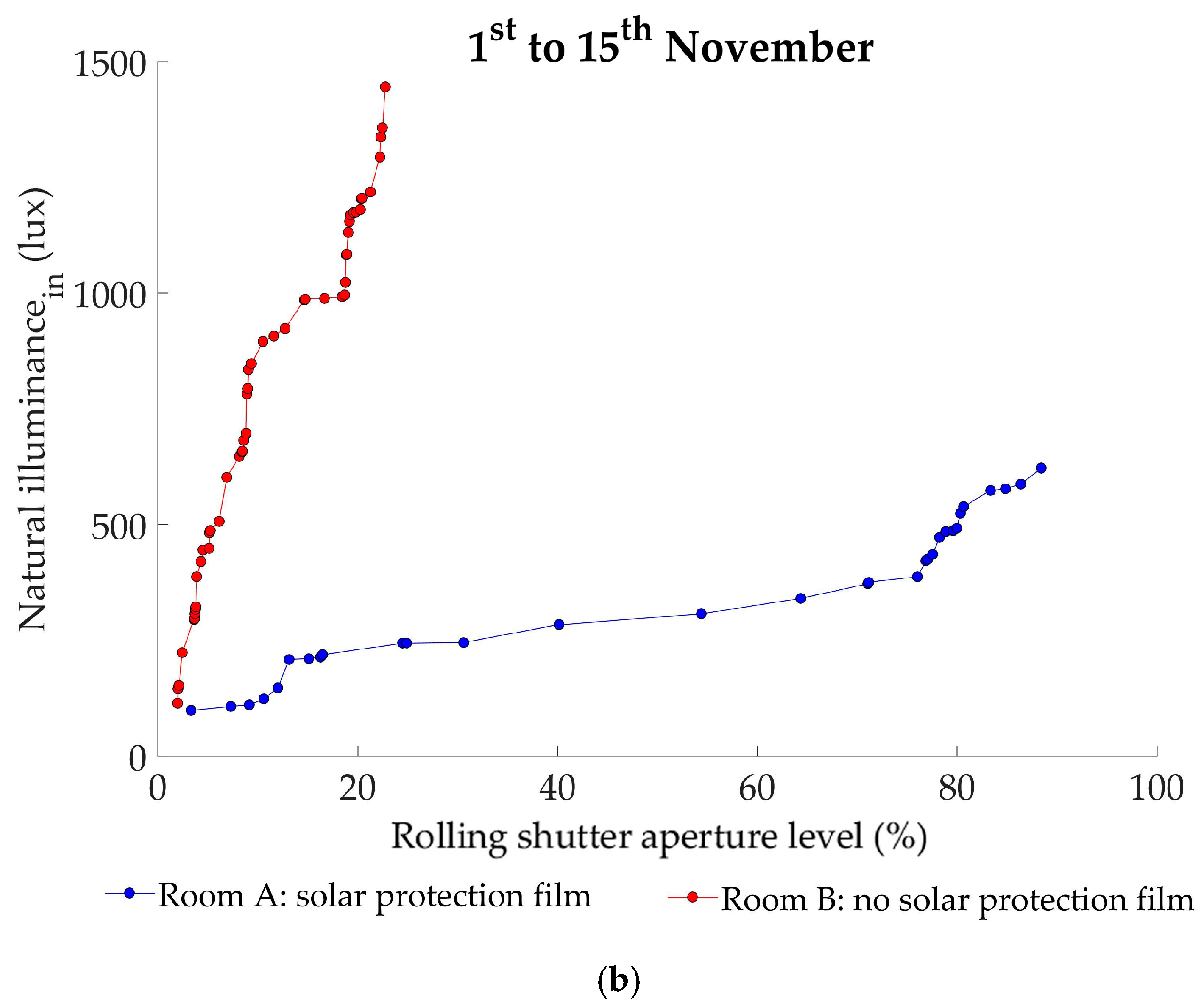
Figure 6 show comparisons of indoor natural illuminance and outdoor illuminance levels, recorded in winter, summer and mid-season. Cumulative distributions of rolling shutter aperture levels and indoor illuminance for each period are also included, in order to give a rough idea of the trend for the use of rolling shutters and thus, user behaviour.
Values referring to both the room without solar film (red points) and the room with solar protection film (blue points) are shown. Each of these points corresponds to the average hourly value, determined with measurements at 10-minute intervals. Previous analysis had verified that hourly values properly represent the 10-minute performances. This analysis considers daily hours with minimum outdoor illuminance levels of 10 klux, which are similar to clear sky conditions, not including night hours and those when there is electric lighting consumption in the analysis.
Furthermore, adjustment techniques have been used in the graphs to analyse the regression models of the samples. The linear equations obtained for each room provide a mathematical regression model, explaining the correlation between outdoor and indoor illuminance. The determination coefficient (R2) has been considered to determine the quality of these models. This coefficient is a statistical measure of how close the sample values are to the regression line and can adopt values between 0 and 1, with a value close to 1 implying the model has a good adjustment.
In all three figures, it can be seen that the higher the outdoor illuminance levels, the higher the indoor illuminance values. The adjustment of the regression models used is quite accurate in all the periods, as the R2 coefficients obtained are close to 1.
The trend of natural illuminance in the room with no solar film is clearly higher than in the room with solar protection film, for all periods.
Indoor illuminance is 48% higher in the room without solar film in winter (
Figure 4a) while rolling shutter aperture levels are quite similar in both cases with an average aperture level of 57.3% open in the room with solar control films and 57.2% with no solar films (
Figure 4b).
In summer, this aspect is more remarkable, with an average difference between indoor illuminance values close to 65% (
Figure 5a), higher with no solar film. Rolling shutter aperture levels are quite different, with an average value of 48.0% open in the room with solar protection film and 71.1% in the other. While the opening of the rolling shutters in the room with solar film tends to be more gradual, in the other room rolling shutter aperture is normally more staggered (
Figure 5b).
The difference in indoor illuminance is less significant in mid-season: natural illuminance levels in the room with solar film are 26% lower (
Figure 6a). This is mainly due to the noticeable difference between the rolling shutter aperture of both cases: an average value of 51.8% open in the room with solar film and 21% in the room with no solar protection. This is clearly seen in
Figure 6b, where the rolling shutter aperture levels of the room with no solar film are usually around 25% open.
Considering all periods, the average illuminance reduction of the solar control film is around 46.3%. Thus, average illuminance reflected is 53.7%, which is close to the 60% visible light reflection provided by the manufacturer. This could be explained by the impact of user behaviour on the lighting performance, as users control rolling shutter aperture levels.
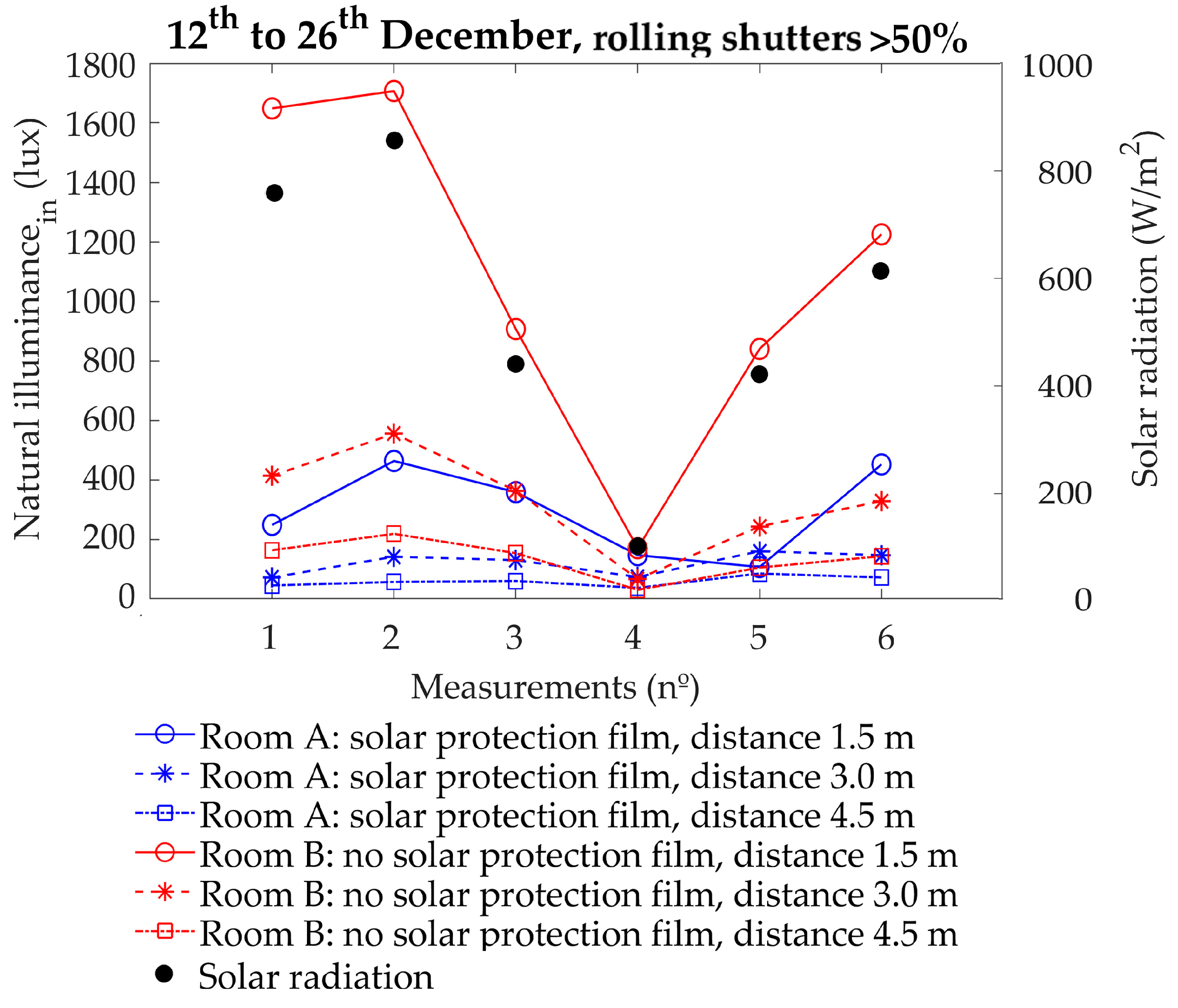
3.2. Natural Illuminance Level Analysis Regarding Distance to the Window
This section is dedicated to the analysis of the natural illuminance levels recorded in the room without (red points) and with solar film (blue points), when the distance between the luxmeters and the sliding window is considered. Data on incident solar radiation on the external facade were also used (vertical surface). Three luxmeters—1.5 m, 3.0 m and 4.5 m from the window—were used to measure illuminance. Natural illuminance values were obtained considering that there was no electric lighting consumption.
In this analysis, it was crucial to filter the data as follows: (1) restricting analysis to the hours in which no artificial lighting consumption is registered; (2) considering the hours with outdoor illuminance levels equal to or above 10 klux; (3) setting rolling shutter aperture levels at a minimum of 50% open. After considering all these conditions, the hours to be analysed are reduced to 6 in winter and 10 in summer. None of the hours monitored in mid-season met those requirements.
In winter (
Figure 7), the highest natural illuminance levels are recorded by the luxmeter closest to the window in the room with no solar film: up to 1200 lux above the illuminance in the room with solar film. Early in the morning (measurements 4 and 6), the luxmeter located 3.0 m from the window records illuminance levels slightly higher in the room with solar film than in that without. This situation is reversed mid-morning (measurements 1 and 3). The points with the lowest illuminance levels are those farthest from the window, especially in the room with solar film. These points are also influenced by the use of the individual curtains between beds. When outdoor illuminance is low, slightly over 10,000 lux (measurement 4), indoor natural illuminance levels are also low and significant differences are barely recorded: around 20 lux in the point closest to the window and 6 lux in the remaining points. The differences are greater in measurement 2, with an outdoor illuminance of approximately 100 klux: about 1200 lux in the luxmeter closest to the window, 400 lux in the middle and 160 lux in the point farthest from the window.
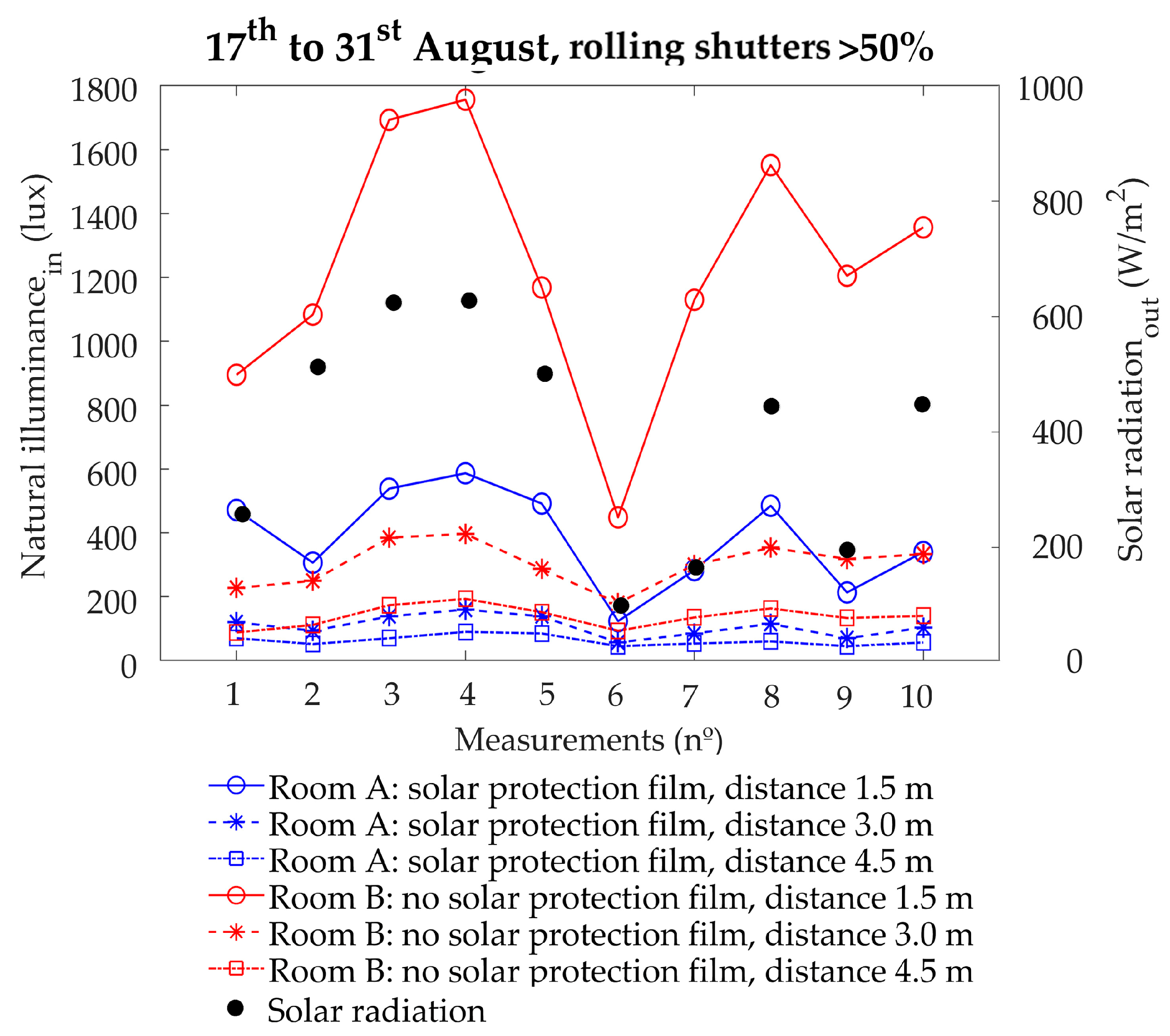
In summer (
Figure 8), a performance pattern similar to the winter period can be observed. Natural illuminance levels are slightly lower in the room with solar film when compared to the room with no solar film. The maximum difference is up to 1000 lux, recorded at 12:00, with lower values in the room with solar protection film.
Both in winter and summer, indoor illuminance levels are in keeping with the incident solar radiation measured. The higher the solar radiation, the higher the indoor natural illuminance. In addition, when solar radiation is reduced, the difference in indoor natural illuminance between the rooms with and without solar film also decreases dramatically.
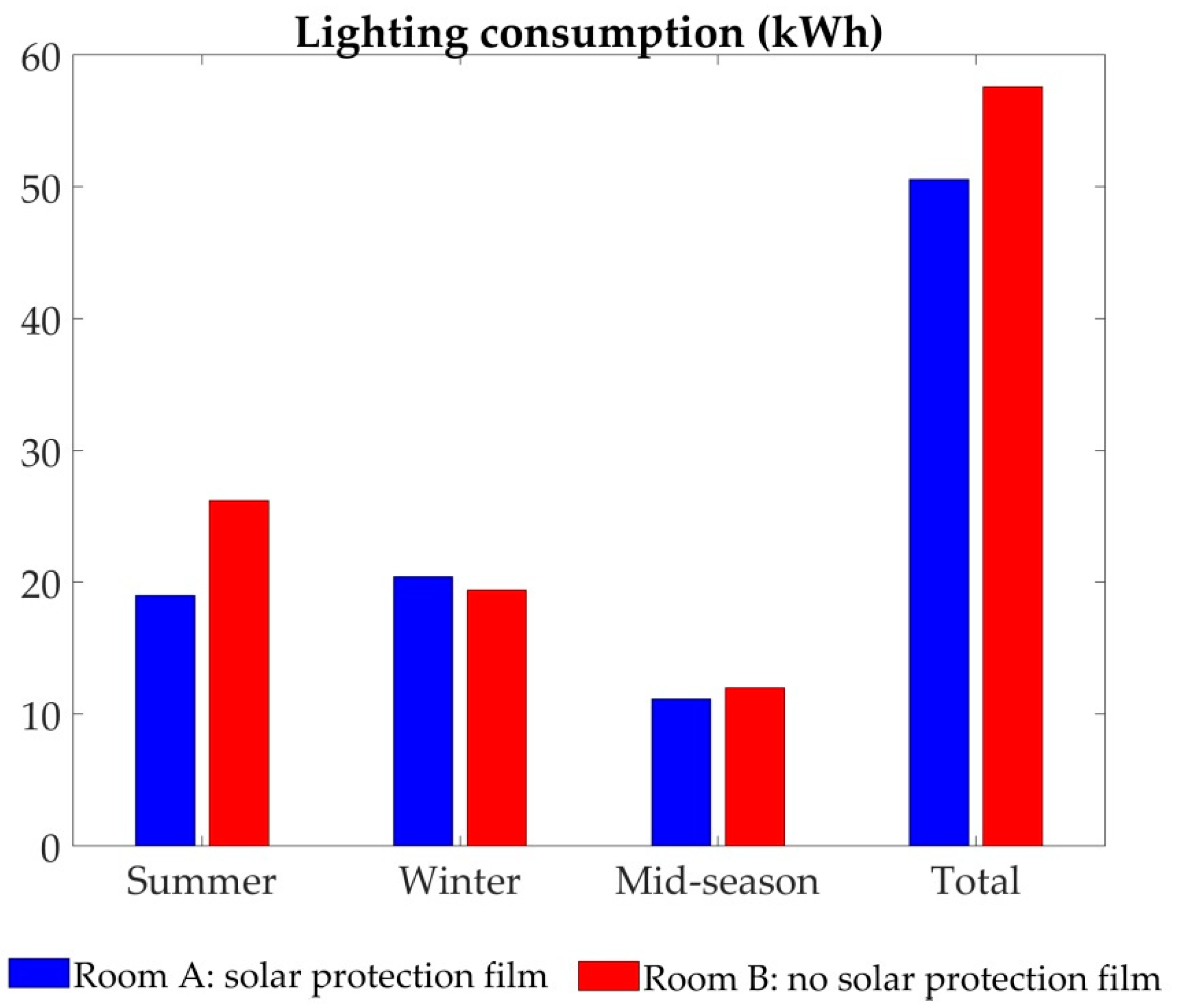
3.3. Electric Consumption Analysis of the Artificial Lighting System.
This section presents the results for the electric consumption (kWh) of the artificial lighting system for each period analysed, together with the final global value (
Figure 9).
In this case, results obtained by the monitoring system have been used directly, with no previous data filtering. Installing solar protection film on the room window results in a 27% reduction in electric lighting consumption in summer and 7% in mid-season. In contrast, electric consumption in winter increases by around 5% in comparison with the room without solar protection film. In other words, the use of solar protection film leads to a total consumption saving of 12.2% during the 75 days analysed, when compared to a room with no solar film.
3.4. Cooling and Heating Energy Demand Analysis
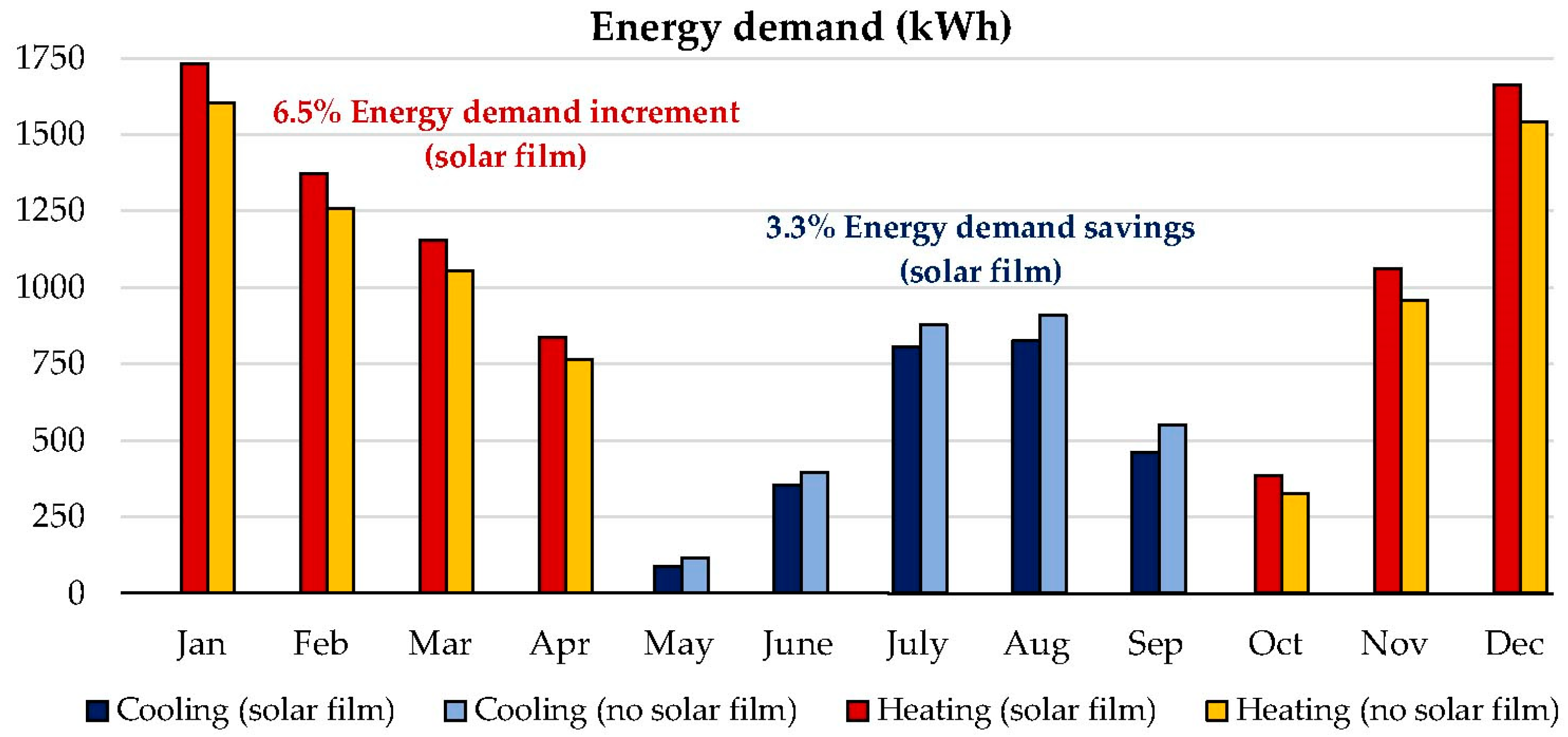
Figure 10 shows the results of the energy demand simulation conducted for the room both with and without solar protection film. The room with solar film registers energy cooling demand savings of around 3.3%. In contrast, energy demand in relation to heating increases by 6.5% compared with the room with no solar protection film, given the reduction of incident solar radiation. In the global balance (
Table 6), energy demand of the room with solar film is 3.2% (approximately 345 kWh) higher than that of the other room. These results are obtained considering the influence of the 0.30 m cantilever of the facade.
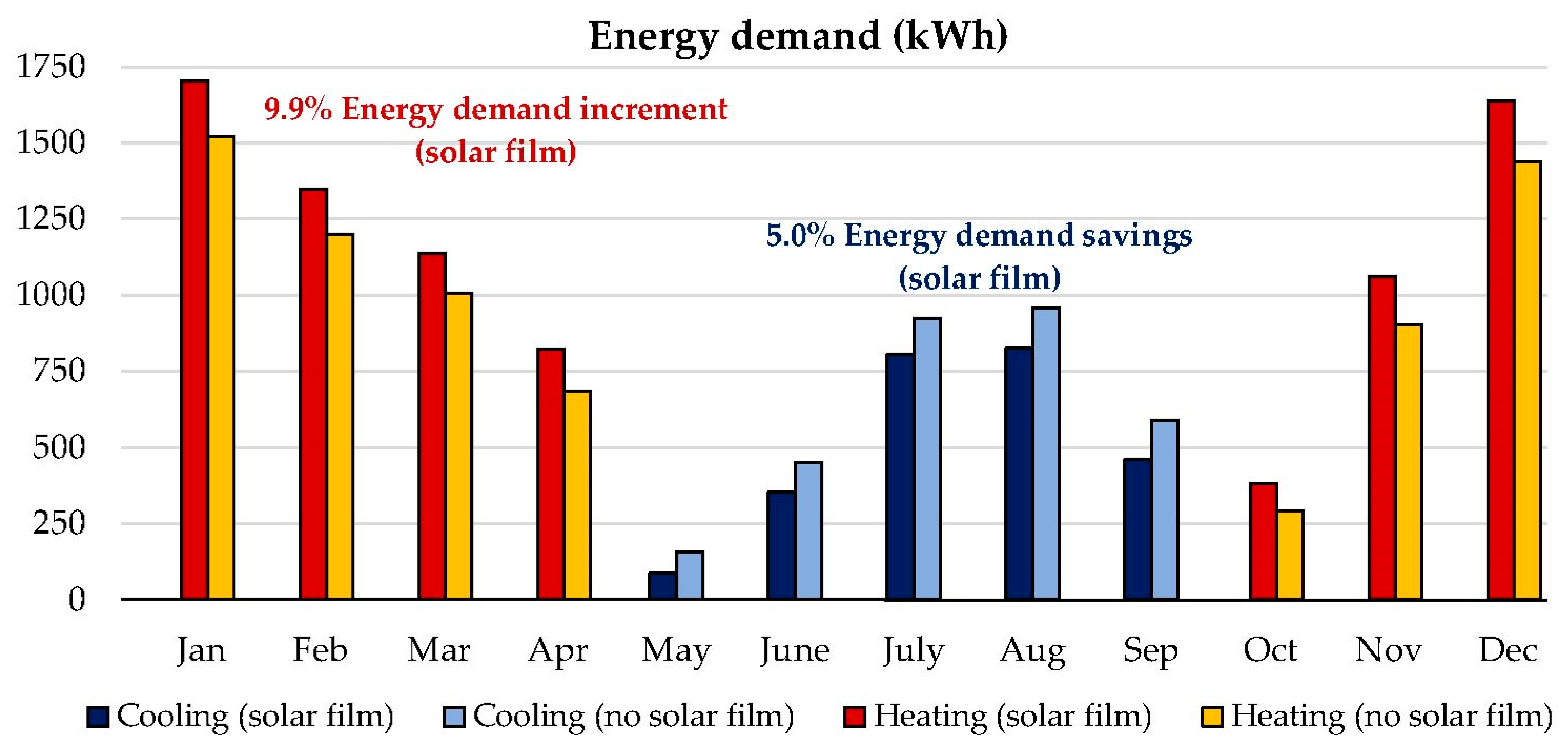
Energy demand differences between both cases are not highly significant given the considerable influence of the cantilever, which also noticeably reduces the incident solar radiation. For this reason, the energy demand of both cases has also been evaluated considering no cantilever (
Figure 11).
In this case, energy demand savings associated with the cooling system are around 5% when the solar protection film is installed. However, energy heating demand increases by 9.9% in the room with solar film, when compared to that without. Quantitatively (
Table 6), the total energy demand of the room with solar protection film is 4.8% (about 510 kWh) higher.
3.5. Strengths and Limitations
In this analysis, the energy and ambient variables of natural and artificial lighting are evaluated in a hospital room, considering real use and occupancy conditions. Monitoring and analysis are extremely complex due to the major influence of users. For instance, users may modify rolling shutter aperture levels in order to adjust indoor lighting conditions to suit their own demands. In comparison with simulation approaches, in which solar control films are directly correlated with a reduction in indoor illuminance levels, on-site results show that this reduction mainly affects high illuminance levels. This means that the indoor daylight environment improves substantially thanks to solar control films. Moreover, given their low cost and quick installation, these devices can be easily included in the retrofitting process of hospital buildings in the Mediterranean climate. Various limitations should also be noted in the analysis conducted:
- -
The use of solar protection films on the glazing surfaces results in a reduction in indoor solar radiation levels. However, this reduction could not be evaluated in the monitored room as hospital personnel did not allow sensors of any sort to be installed on the internal sliding window surface. For this reason, the monitoring system only reports information on the incident solar radiation on the facade.
- -
Similarly, the reduction in indoor solar radiation should have an impact on the indoor temperatures in the room. However, the hospital building has a centralized HVAC system, controlled by hospital personnel, which uses outdoor air to guarantee indoor air quality. This system runs continuously (always turned ON), ensuring indoor temperatures are always maintained at 23–25°C. Given the limitations imposed by hospital personnel, it was not possible to monitor HVAC energy consumption. An energy simulation model was therefore constructed in order to assess cooling and heating energy demand of the room with and without solar protection film.
- -
It should also be emphasised that the presence of individual curtains between patients’ beds gives rise to other uncertainties relating to the lighting analysis. As these curtains are not controlled by the monitoring system, their real influence on natural illuminance levels could not be assessed adequately. In this respect, more in-depth research should be conducted in future to properly analyse the influence of curtains on indoor natural illuminance, also taking into consideration the distance from the window.
- -
Finally, it should be noted that the monitoring system does not measure electric consumption for individual luminaires in the room, and instead provides an overall value of the system. Hence, there is no information about which individual luminaires are turned OFF and ON at different times.
4. Conclusions
This paper assesses the influence of a solar protection film installed on the outer surface of a window of a hospital building in southern Spain (Mediterranean climate). A room was monitored during three distinct seasonal periods (winter, summer and mid-season) under real use conditions. This analysis was divided into two phases: (1) the room was monitored with no solar film on the glazed surface and (2) the room was monitored after a solar protection film was added.
More specifically, this paper reports results relating to indoor illuminance levels (lux) and lighting consumption (kWh). Even though monitoring periods were reduced to approximately two weeks per season for the purposes of the analysis, the following conclusions can be highlighted:
The use of a solar control film on the exterior of the window, when combined with shading shutters, brings about a noticeable reduction in the electric consumption of the artificial lighting system: 12.2% in comparison with a room without solar film. This is due to the fact that, considering all the hours monitored, users tend to activate the lighting system less often because rolling shutter levels usually remain at higher aperture levels. In other words, the implementation of a solar control film helps to create a more comfortable indoor environment in terms of daylight, which contributes to users maintaining rolling shutters open at higher levels more often. Hence illuminance values are higher in these circumstances in the room with solar control films, with less artificial lighting consumption. Electric savings are especially significant in summer, when the electric consumption of the room with solar film is reduced by almost one third (27%). In mid-season, the room without solar film barely exceeds the electric consumption of the room with solar film by 7%. In contrast, the solar protection film presents a 5% penalization of electric consumption in winter. These results prove that users highly influence the activation of the lighting system and the use of shading shutters, which clearly have an impact on electric consumption.
Furthermore, the use of shading protection based on solar film involves a considerable reduction in natural illuminance levels when the lighting system is simultaneously turned OFF in both the room with and without solar control film. In summer, the average reduction in natural illuminance is 65%. This value represents 48% and 26% in winter and mid-season, respectively. However, solar protection generally allows natural illuminance levels above 300 lux to be reduced. Meanwhile, the room with solar protection film records a higher percentage of hours with natural illuminance levels between 100 and 300 lux, when compared to the room with no solar film.
In this paper, no clear correlation was found between rolling shutter aperture levels and the activation of lighting for any of the periods monitored, considering a confidence level of 95%. It should be stressed that the energy demand of the HVAC system could not be monitored because of the limitations imposed by the hospital personnel. However, energy simulation models showed that the room with solar protection film presents cooling demand savings of 3.3%, while heating demand increases by 6.5%. This leads to an energy demand deficit of 3.2% when the solar protection film is installed in the hospital room. However, energy demand differences between both cases are not significant given the small dimensions of the windows and the presence of a continuous 0.30 m cantilever which reduces incident solar radiation.
The use of solar control films in retrofitting hospital buildings in the Mediterranean climate not only brings about a reduction in cooling loads, as established by previous studies in the field, but this research also describes the benefits on the indoor daylight environment when combined with user operation of the rolling shutters. This in turn contributes to improving the health outcomes of patients and to reducing electric lighting consumption when compared to a room with no solar control film, but with rolling shutters.
In terms of policy implications, besides the health benefits of having clear views through the windows, the low-cost and easy implementation of solar control films for retrofitting hospital rooms should be emphasised, especially regarding the minimal disruption to users and health procedures. However, given the significant influence of users on the results, further research should be carried out to determine the real impact of the variables freely controlled by users: the rolling shutters and particularly the individual curtains between beds.



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}