A Clinical Trial to Evaluate the Efficacy and Safety of 3D Printed Bioceramic Implants for the Reconstruction of Zygomatic Bone Defects


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
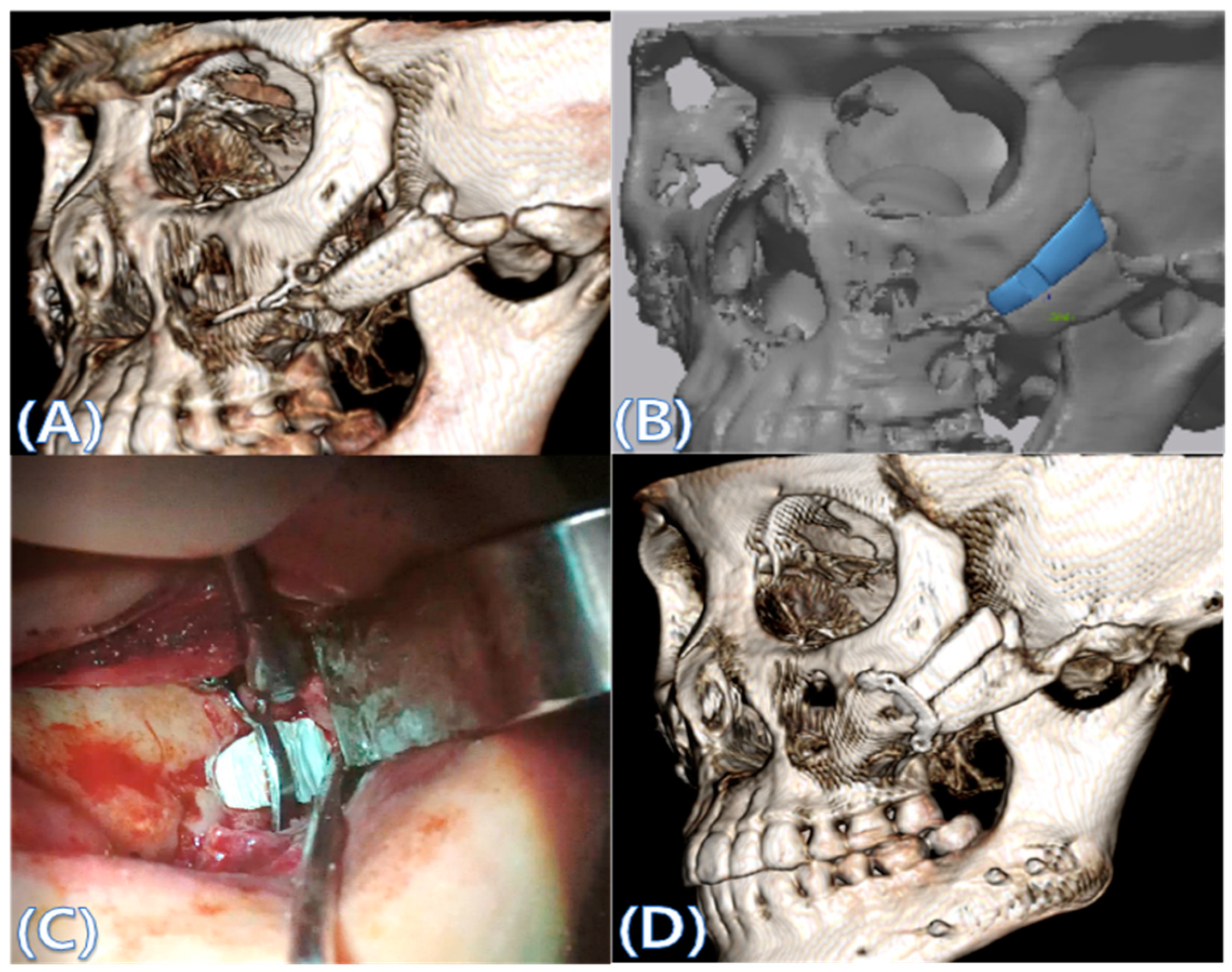
2.2. Computer-Aided Virtual Surgery, Design, and Fabrication of Patient-Specific Devices
2.3. Surgical Procedure
2.4. Evaluation
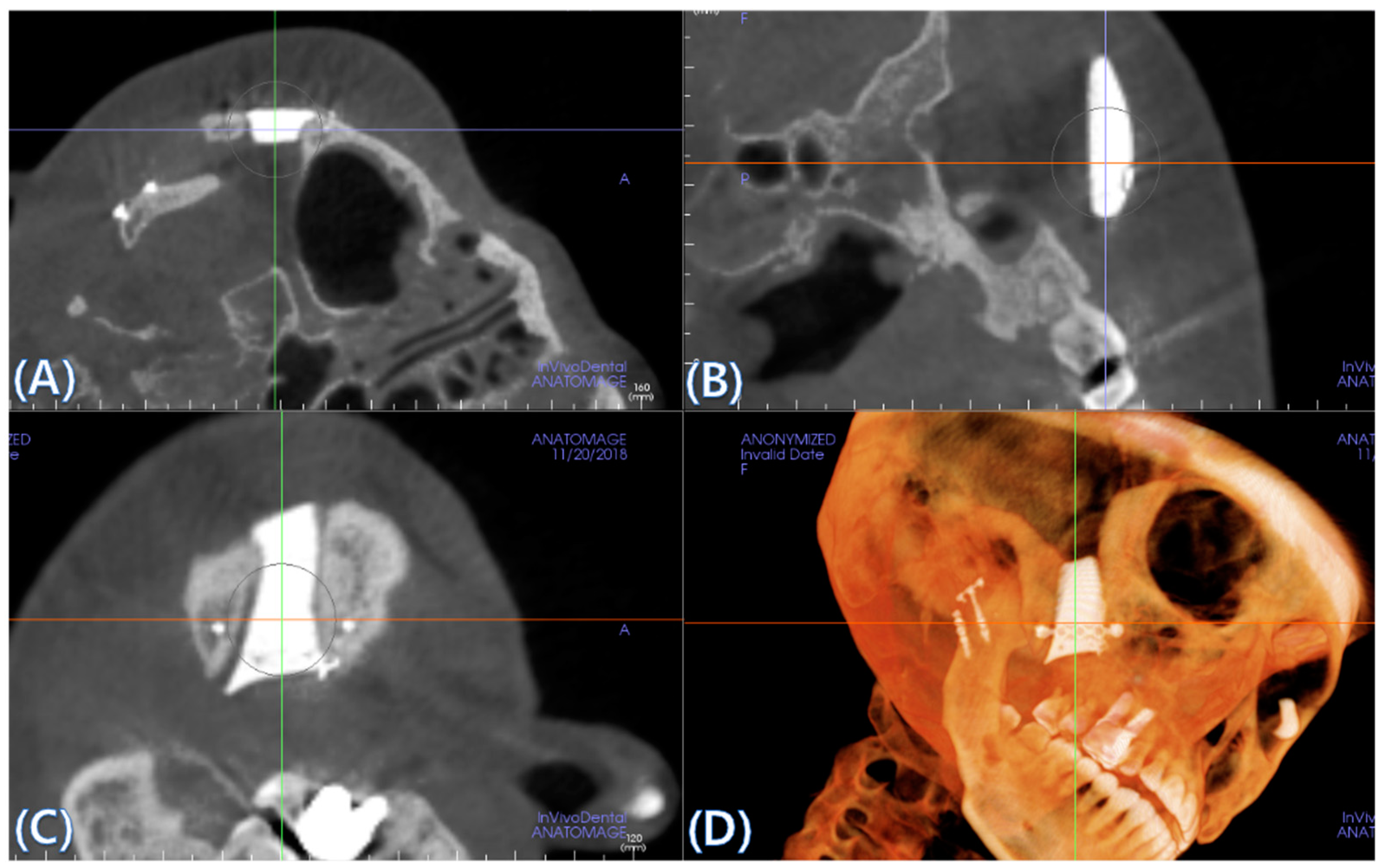
2.5. Cone Beam CT and 3D Comparison
2.6. Sample Size Determination
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
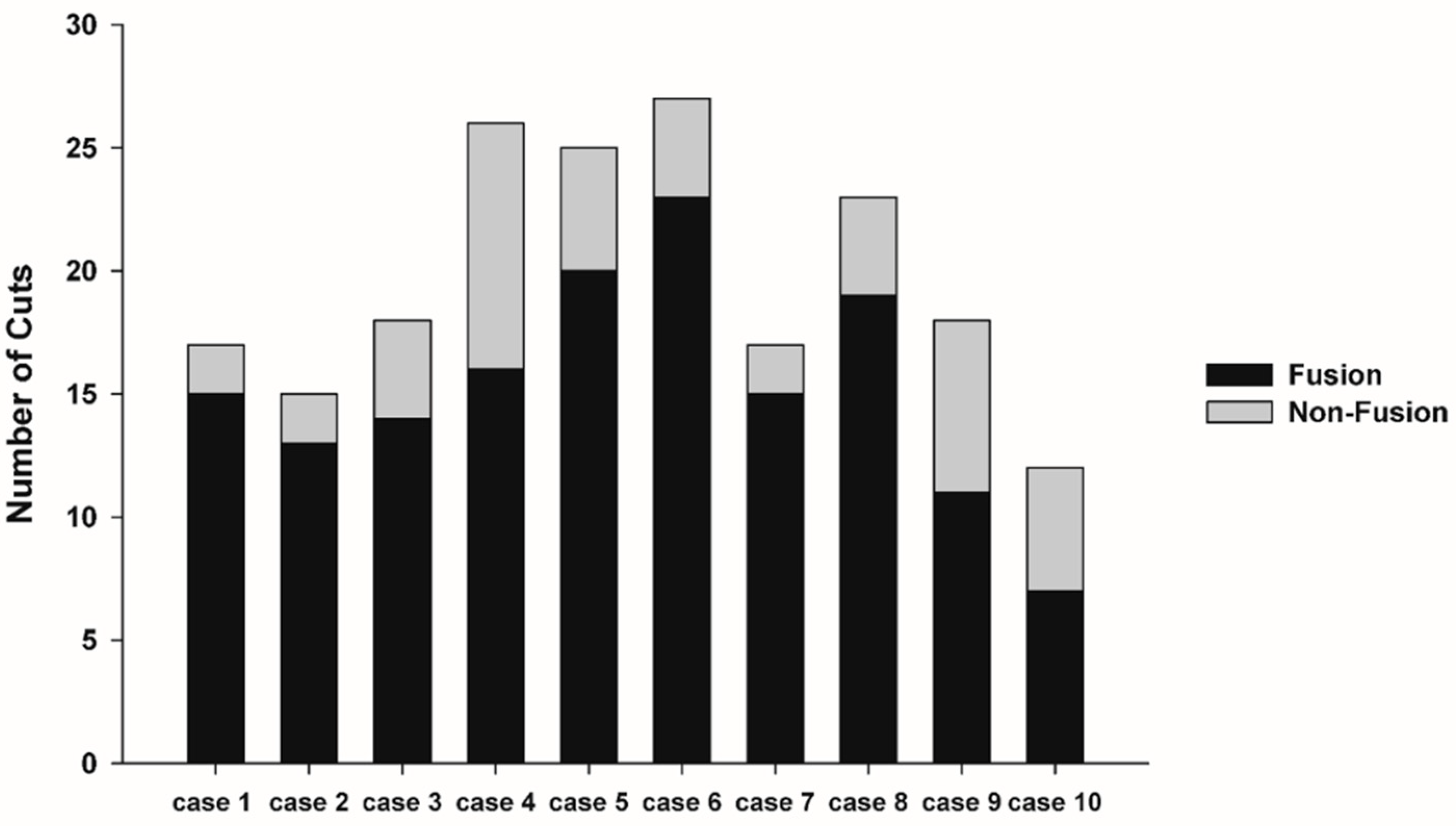
3.2. Fusion Rate Analysis Using 3D CT
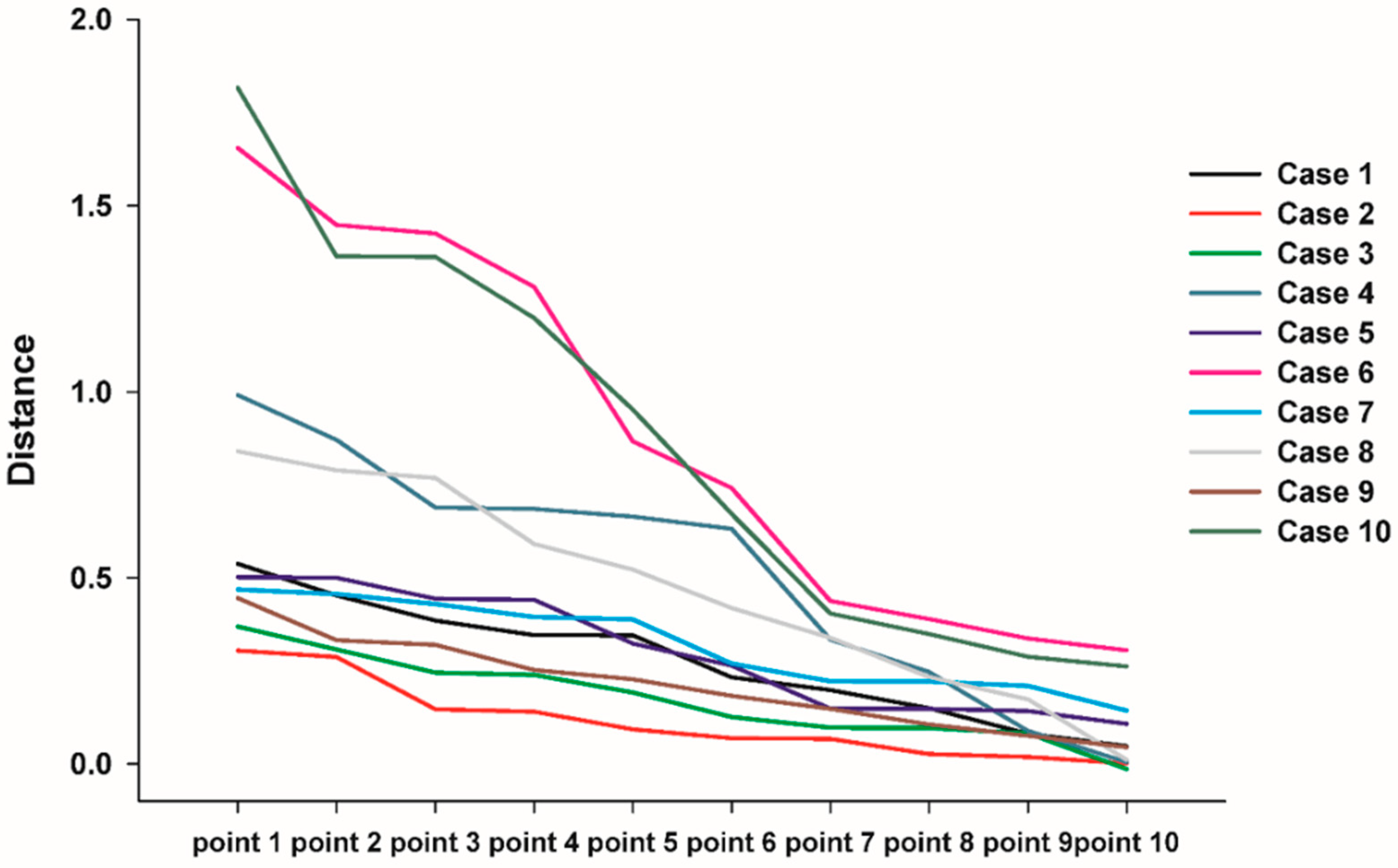
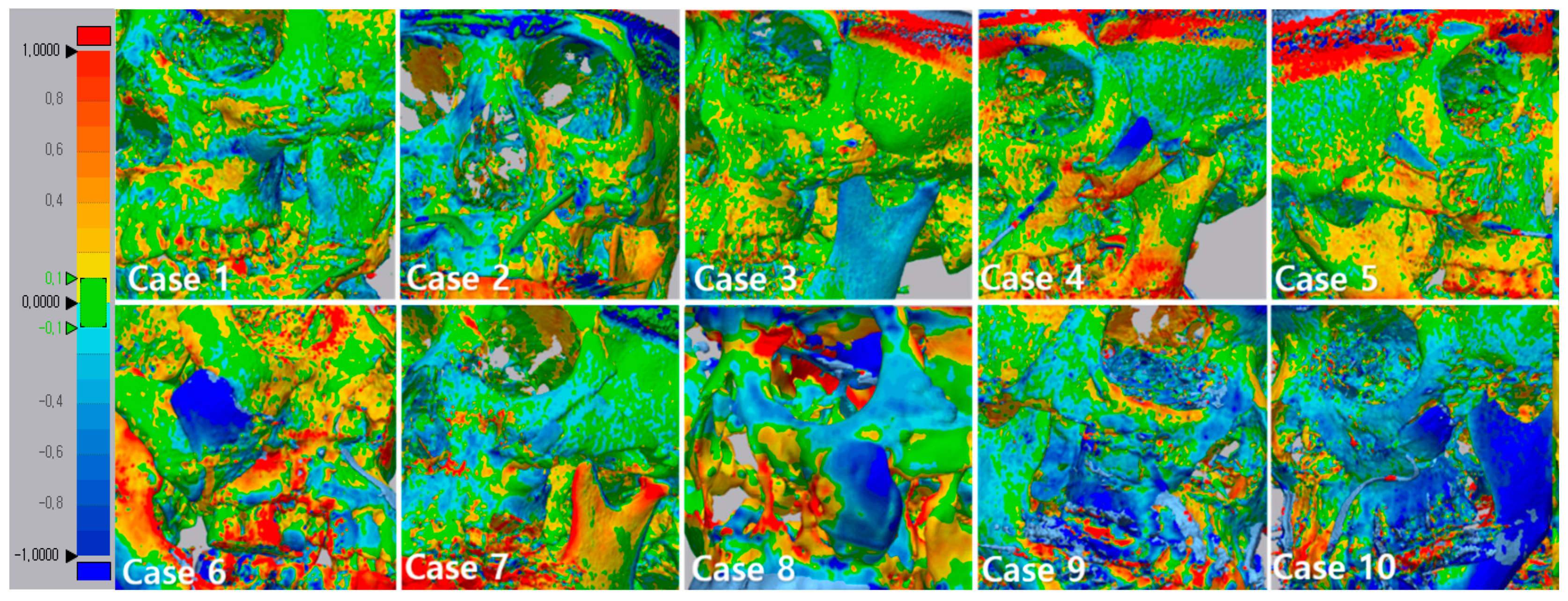
3.3. 3D Comparison between Immediate Post Operative and 6 Months Post Operative
3.4. Results of Satisfactory Scale and Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lee, U.-L.; Kwon, J.-S.; Woo, S.-H.; Choi, Y.-J. Simultaneous Bimaxillary Surgery and Mandibular Reconstruction With a 3-Dimensional Printed Titanium Implant Fabricated by Electron Beam Melting: A Preliminary Mechanical Testing of the Printed Mandible. J. Oral Maxillofac. Surg. 2016, 74, 1501.e1–1501.e15. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Covani, U. Maxillary Alveolar Ridge Reconstruction With Nonvascularized Autogenous Block Bone: Clinical Results. J. Oral Maxillofac. Surg. 2007, 65, 2039–2046. [Google Scholar] [CrossRef] [PubMed]
- Grassi, F.R.; Grassi, R.; Vivarelli, L.; Dallari, D.; Govoni, M.; Nardi, G.M.; Kalemaj, Z.; Ballini, A. Design Techniques to Optimize the Scaffold Performance: Freeze-dried Bone Custom-made Allografts for Maxillary Alveolar Horizontal Ridge Augmentation. Materials 2020, 13, 1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ettl, T.; Driemel, O.; Dresp, B.V.; Reichert, T.E.; Reuther, J.; Pistner, H. Feasibility of alloplastic mandibular reconstruction in patients following removal of oral squamous cell carcinoma. J. Cranio-Maxillofac. Surg. 2010, 38, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Shan, X.-F.; Chen, H.-M.; Liang, J.; Huang, J.-W.; Cai, Z.-G. Surgical Reconstruction of Maxillary and Mandibular Defects Using a Printed Titanium Mesh. J. Oral Maxillofac. Surg. 2015, 73, 1437.e1–1437.e9. [Google Scholar] [CrossRef] [PubMed]
- Bertollo, N.; Da Assunção, R.; Hancock, N.J.; Lau, A.; Walsh, W.R. Influence of Electron Beam Melting Manufactured Implants on Ingrowth and Shear Strength in an Ovine Model. J. Arthroplast. 2012, 27, 1429–1436. [Google Scholar] [CrossRef]
- Hrabe, N.W.; Heinl, P.; Flinn, B.; Körner, C.; Bordia, R.K. Compression-compression fatigue of selective electron beam melted cellular titanium (Ti-6Al-4V). J. Biomed. Mater. Res. Part B Appl. Biomater. 2011, 99, 313–320. [Google Scholar] [CrossRef]
- Joshi, G.V.; Duan, Y.; Neidigh, J.; Koike, M.; Chahine, G.; Kovacevic, R.; Okabe, T.; Griggs, J.A. Fatigue testing of electron beam-melted Ti-6Al-4V ELI alloy for dental implants. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 101, 124–130. [Google Scholar] [CrossRef]
- Wilde, F.; Hanken, H.; Probst, F.; Schramm, A.; Heiland, M.; Cornelius, C.-P. Multicenter study on the use of patient-specific CAD/CAM reconstruction plates for mandibular reconstruction. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 2035–2051. [Google Scholar] [CrossRef]
- Watson, J.; Hatamleh, M.; Alwahadni, A.; Srinivasan, D. Correction of Facial and Mandibular Asymmetry Using a Computer Aided Design/Computer Aided Manufacturing Prefabricated Titanium Implant. J. Craniofacial Surg. 2014, 25, 1099–1101. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, S.K.; Kang, S.S.; Han, S.J.; Lee, C.-K.; Chang, B.-S. A Long-Term Follow-up, Multicenter, Comparative Study of the Radiologic, and Clinical Results Between a CaO-SiO2-P2O5-B2O3 Bioactive Glass Ceramics (BGS-7) Intervertebral Spacer and Titanium Cage in 1-Level Posterior Lumbar Interbody Fusion. Clin. Spine Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kokubo, T.; Ito, S.; Huang, Z.T.; Hayashi, T.; Sakka, S.; Kitsugi, T.; Yamamuro, T. Ca, P-rich layer formed on high-strength bioactive glass-ceramic A-W. J. Biomed. Mater. Res. 1990, 24, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Ohtsuki, C.; Kamitakahara, M.; Miyazaki, T. Bioactive ceramic-based materials with designed reactivity for bone tissue regeneration. J. R. Soc. Interface 2009, 6, S349–S360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Nam, H.; Chang, B.-S.; Lee, C.-K.; Ryu, H.-S.; Seo, J.-H. Bioactive ceramic coating of cancellous screws improves the osseointegration in the cancellous bone. J. Orthop. Sci. 2011, 16, 291–297. [Google Scholar] [CrossRef]
- Lee, J.H.; Hong, K.S.; Baek, H.-R.; Seo, J.-H.; Lee, K.M.; Ryu, H.-S.; Lee, H.-K. In Vivo Evaluation of CaO-SiO2-P2O5-B2O3 Glass-Ceramics Coating on Steinman Pins. Artif. Organs 2013, 37, 656–662. [Google Scholar] [CrossRef]
- Lee, J.H.; Seo, J.-H.; Lee, K.M.; Ryu, H.-S.; Baek, H.-R. Fabrication and Evaluation of Osteoblastic Differentiation of Human Mesenchymal Stem Cells on Novel CaO-SiO2-P2O5-B2O3 Glass-Ceramics. Artif. Organs 2013, 37, 637–647. [Google Scholar] [CrossRef]
- Lee, J.H.; Ryu, H.-S.; Seo, J.-H.; Chang, B.-S.; Lee, C.-K. A 90-day intravenous administration toxicity study of CaO-SiO2-P2O5-B2O3 glass-ceramics (BGS-7) in rat. Drug Chem. Toxicol. 2009, 33, 38–47. [Google Scholar] [CrossRef]
- World Medical Association General Assembly World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects Revised October 7, 2000. HIV Clin. Trials 2001, 2, 92–95. [CrossRef]
- Cho, J.; Kwon, J.-S.; Lee, U.-L. Occlusion-Fit Three-Dimensional–Printed Zygoma Repositioner. J. Craniofacial Surg. 2018, 29, 731–732. [Google Scholar] [CrossRef]
- Baek, R.-M.; Kim, J.; Lee, S.W. Revision reduction malarplasty with coronal approach. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, 2018–2024. [Google Scholar] [CrossRef]
- Lee, J.H.; Ryu, H.-S.; Seo, J.-H.; Lee, D.-Y.; Chang, B.-S.; Lee, C.-K. Negative Effect of Rapidly Resorbing Properties of Bioactive Glass-Ceramics as Bone Graft Substitute in a Rabbit Lumbar Fusion Model. Clin. Orthop. Surg. 2014, 6, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Ryu, H.-S.; Lee, D.-S.; Hong, K.S.; Chang, B.-S.; Lee, C.-K. Biomechanical and histomorphometric study on the bone–screw interface of bioactive ceramic-coated titanium screws. Biomaterials 2005, 26, 3249–3257. [Google Scholar] [CrossRef] [PubMed]
- LeGeros, R. Calcium Phosphate Materials in Restorative Dentistry: A Review. Adv. Dent. Res. 1988, 2, 164–180. [Google Scholar] [CrossRef] [PubMed]
- Jarcho, M. Retrospective analysis of hydroxyapatite development for oral implant applications. Dent. Clin. North Am. 1992, 36, 19–26. [Google Scholar] [PubMed]
- Piattelli, A.; Cordioli, G.P.; Trisi, P.; Passi, P.; A Favero, G.; Meffert, R.M. Light and confocal laser scanning microscopic evaluation of hydroxyapatite resorption patterns in medullary and cortical bone. Int. J. Oral Maxillofac. Implant. 1993, 8, 309–315. [Google Scholar]
- Ozawa, S. Evaluation of implant materials (hydroxyapatite, glass-ceramics, titanium) in rat bone marrow stromal cell culture. Biomaterials 1996, 17, 23–29. [Google Scholar] [CrossRef]
- Zablotsky, M. The surgical management of osseous defects associated with endosteal hydroxyapatite-coated and titanium dental implants. Dent. Clin. North Am. 1992, 36, 117. [Google Scholar]
- De Lange, G.; Donath, K. Interface between bone tissue and implants of solid hydroxyapatite or hydroxyapatite-coated titanium implants. Biomaterials 1989, 10, 121–125. [Google Scholar] [CrossRef]
- Rocca, M.; Fini, M.; Giavaresi, G.; Aldini, N.N.; Giardino, R. Osteointegration of hydroxyapatite-coated and uncoated titanium screws in long-term ovariectomized sheep. Biomaterials 2002, 23, 1017–1023. [Google Scholar] [CrossRef]
- Cook, S.D.; Kay, J.F.; A Thomas, K.; Jarcho, M. Interface mechanics and histology of titanium and hydroxylapatite-coated titanium for dental implant applications. Int. J. Oral Maxillofac. Implant. 1987, 2, 15–22. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1. Adults aged 19 to under 75 who have completed craniofacial growth 2. Those with obvious zygoma defects, who need and want reconstruction 3. In the case of women of childbearing potential, those who consent to contraceptive use during the clinical trial participation period (more than 6 months after surgery) 4. Those who voluntarily agreed to participate in clinical trials and were willing to comply with the study protocol. | 1. People with uncontrolled metabolic diseases (e.g., diabetes, osteomalacia, thyroid disease) 2. People who are taking or are planning to take drugs that can affect bone metabolism (Bisphosphonate, Recombinant human parathyroid hormone, Denosumab, etc.) 3.Those with uncontrolled gingivitis, periodontitis, and dental caries 4. People with severe heart disease or severe liver dysfunction 5. Persons with infectious diseases with a risk of recurrence 6. People with blood diseases (leukemia, hemophilia, sepsis, etc.) 7. People who cannot stop taking steroids, anti-thrombotics, or anticoagulants before surgery 8. People who cannot stop systemic corticosteroids or anabolic steroids for 3 months after surgery 9. People with osteomalacia and Paget’s disease 10. People who have experienced radiation therapy at the surgical site 11. People who are allergic to implant materials 12. Patients with syphilis and severe epilepsy 13. Drug abuse or alcoholics 14. Smokers 15. People who are pregnant or have a pregnancy plan during the clinical trial period 16. In case the investigator judges that participation in the clinical trial is inappropriate because other ethical or clinical trial results may be affected. |
| Screening Number | Gender/Age | Cause of Defect | Defect | Defect Area (mm) | Virtual Planning | Fixation Method |
|---|---|---|---|---|---|---|
| 1S-01 | F/29 | Zygoma plasty |  | X = 16.4 Y = 9.8 Z = 3.8 |  | Plate |
| 1S-02 | F/24 | Zygoma plasty |  | X = 32.4 Y = 12 Z = 4.8 |  | Plate |
| 1S-03 | M/25 | Zygoma plasty |  | X = 17.3 Y = 13.3 Z = 5 | 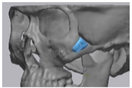 | Plate |
| 1S-04 | F/28 | Zygoma plasty |  | X = 28.4 Y = 10.9 Z = 5 | 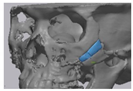 | Plate |
| 1S-05 | F/28 | Zygoma plasty |  | X = 26 Y = 8.2 Z = 4.4 |  | Plate |
| 1S-06 | F/41 | Zygoma plasty |  | X = 29 Y = 19.2 Z = 5 |  | Plate and wire |
| 1S-07 | F/26 | Zygoma plasty |  | X = 18.1 Y = 7 Z = 4.1 | 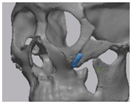 | Plate |
| 1S-08 | F/53 | Zygoma plasty |  | X = 37 Y = 21.5 Z = 5 | 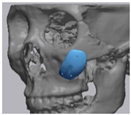 | Plate and wire |
| 1S-09 | F/53 | Zygoma plasty |  | X = 21.8 Y = 13.3 Z = 5 | 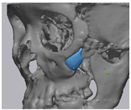 | Wire |
| 1S-10 | F/53 | Zygoma plasty | 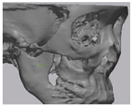 | X = 16.8 Y = 13 Z = 4 |  | Wire |
| Point 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Aver. | SD | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 0.3853 | 0.3461 | 0.5375 | 0.3455 | 0.4526 | 0.233 | 0.1499 | 0.1982 | 0.0476 | 0.0812 | 0.2776 | 0.1616 |
| 2 | 0.1469 | 0.3044 | 0.0014 | 0.2874 | 0.0191 | 0.1403 | 0.0927 | 0.0263 | 0.0695 | 0.0675 | 0.1155 | 0.1064 |
| 3 | 0.0979 | 0.0137 | 0.1259 | 0.0966 | 0.0821 | 0.1918 | 0.2396 | 0.3076 | 0.2452 | 0.3689 | 0.1741 | 0.1170 |
| 4 | 0.3342 | 0.0045 | 0.0888 | 0.2472 | 0.6319 | 0.6853 | 0.6889 | 0.6646 | 0.871 | 0.9915 | 0.5207 | 0.3327 |
| 5 | 0.1479 | 0.3236 | 0.1486 | 0.1077 | 0.4406 | 0.1422 | 0.5004 | 0.4437 | 0.5019 | 0.2645 | 0.3021 | 0.1602 |
| 6 | 0.4378 | 0.3892 | 0.337 | 0.3052 | 0.8668 | 0.7413 | 1.2819 | 1.4485 | 1.4251 | 1.6551 | 0.8887 | 0.5231 |
| 7 | 0.4298 | 0.2216 | 0.3879 | 0.2224 | 0.2695 | 0.2097 | 0.4689 | 0.3944 | 0.1436 | 0.456 | 0.3203 | 0.1192 |
| 8 | 0.4187 | 0.3392 | 0.5911 | 0.8404 | 0.5219 | 0.7681 | 0.7887 | 0.2335 | 0.1735 | 0.011 | 0.4686 | 0.2826 |
| 9 | 0.3199 | 0.1057 | 0.2524 | 0.1483 | 0.2272 | 0.3322 | 0.1833 | 0.4457 | 0.0755 | 0.045 | 0.2135 | 0.1270 |
| 10 | 0.3489 | 0.2618 | 0.9525 | 0.4041 | 0.288 | 1.3645 | 1.1981 | 0.6722 | 1.8174 | 1.3628 | 0.8670 | 0.5513 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, U.-L.; Lim, J.-Y.; Park, S.-N.; Choi, B.-H.; Kang, H.; Choi, W.-C. A Clinical Trial to Evaluate the Efficacy and Safety of 3D Printed Bioceramic Implants for the Reconstruction of Zygomatic Bone Defects. Materials 2020, 13, 4515. https://doi.org/10.3390/ma13204515
Lee U-L, Lim J-Y, Park S-N, Choi B-H, Kang H, Choi W-C. A Clinical Trial to Evaluate the Efficacy and Safety of 3D Printed Bioceramic Implants for the Reconstruction of Zygomatic Bone Defects. Materials. 2020; 13(20):4515. https://doi.org/10.3390/ma13204515
Chicago/Turabian StyleLee, Ui-Lyong, Jun-Young Lim, Sung-Nam Park, Byoung-Hun Choi, Hyun Kang, and Won-Cheul Choi. 2020. "A Clinical Trial to Evaluate the Efficacy and Safety of 3D Printed Bioceramic Implants for the Reconstruction of Zygomatic Bone Defects" Materials 13, no. 20: 4515. https://doi.org/10.3390/ma13204515