
Narrow Diameter Dental Implants as an Alternative Treatment for Atrophic Alveolar Ridges. Systematic Review and Meta-Analysis


 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reporting Format
2.2. PICO (Population, Intervention, Comparison, Outcomes) Question
2.3. Eligibility Criteria
2.4. Search Strategy and Study Selection
2.5. Data Collection
2.6. Quality Assessment and Risk of Bias
2.7. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Methods and Characteristics
3.3. Quality Assessment and Risk of Bias
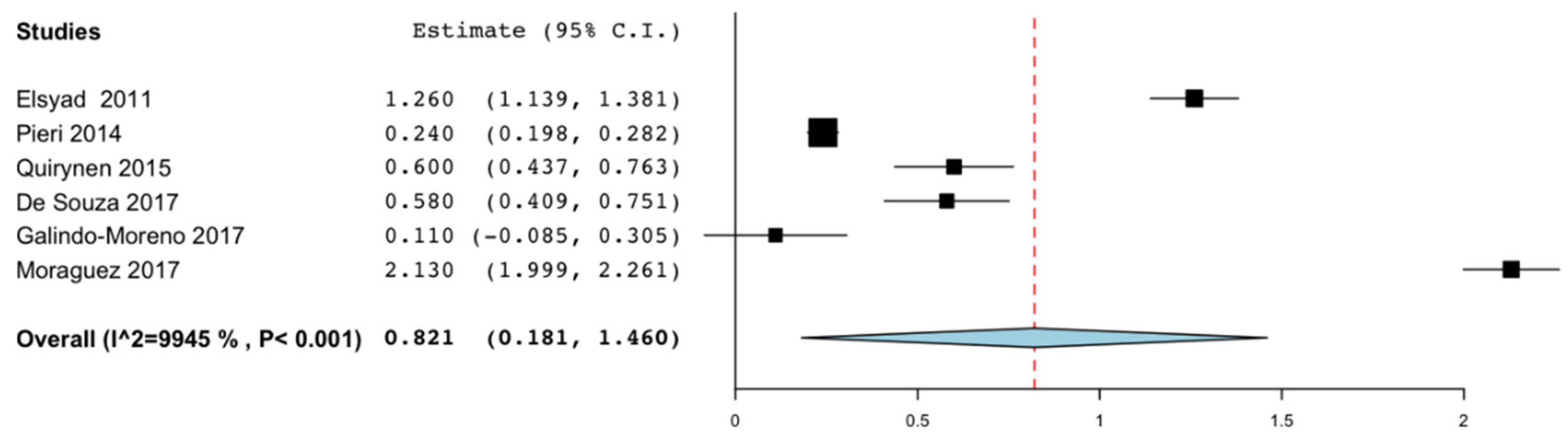
3.4. Marginal Bone Loss
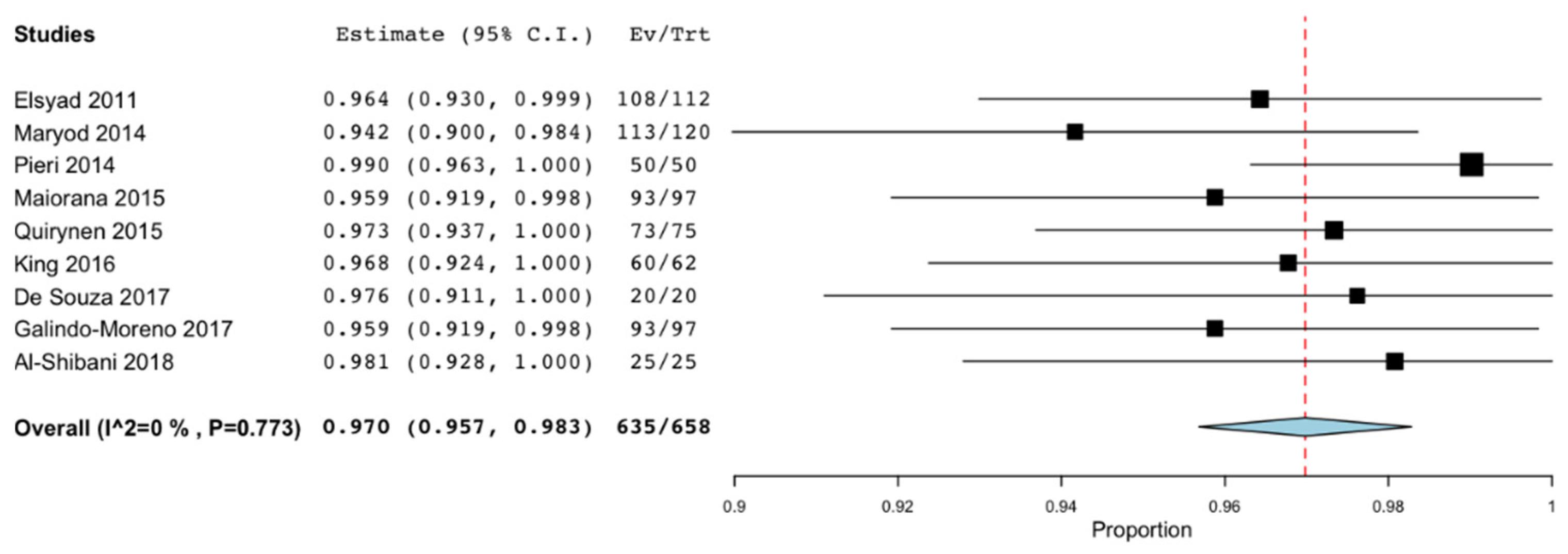
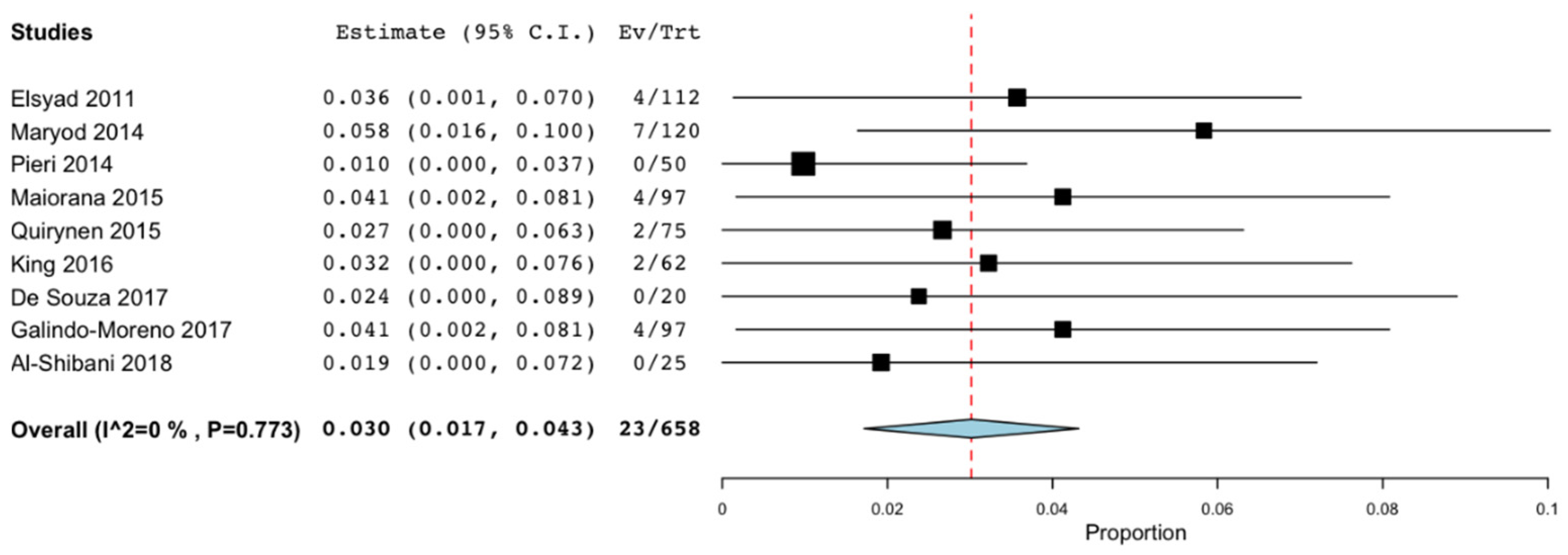
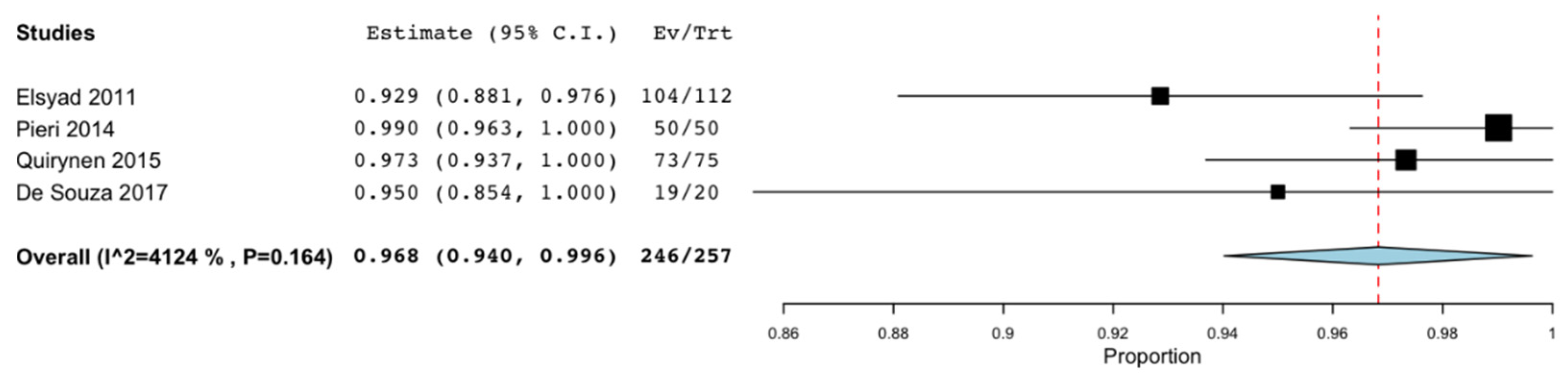
3.5. Failure, Success, and Survival Rates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heydecke, G.; Locker, D.; Awad, M.A.; Lund, J.P.; Feine, J.S. Oral and general health-related quality of life with conventional and implant dentures. Community Dent. Oral Epidemiol. 2003, 31, 161–168. [Google Scholar] [CrossRef]
- Schiegnitz, E.; Kammerer, P.W.; Sagheb, K.; Wendt, A.J.; Pabst, A.; Al-Nawas, B.; Klein, M.O. Impact of maxillary sinus augmentation on oral health-related quality of life. Int. J. Implant. Dent. 2017, 3, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.; Jung, U.W.; Cho, K.S.; Lee, J.S. Retrospective radiographic observational study of 1692 Straumann tissue-level dental implants over 10 years: I. Implant survival and loss pattern. Clin. Implant. Dent. Relat. 2018, 20, 860–866. [Google Scholar] [CrossRef]
- Moraschini, V.; Poubel, L.A.; Ferreira, V.F.; Barboza Edos, S. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Schiegnitz, E.; Al-Nawas, B.; Tegner, A.; Sagheb, K.; Berres, M.; Kammerer, P.W.; Wagner, W. Clinical and radiological long-term outcome of a tapered implant system with special emphasis on the influence of augmentation procedures. Clin. Implant. Dent. Relat. Res. 2015, 18, 810–820. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Mericske-Stern, R.; Bernard, J.P.; Behneke, A.; Behneke, N.; Hirt, H.P.; Belser, U.C.; Lang, N.P. Long-term evaluation of non-submerged ITI implants. Part 1: 8-yearlife table analysis of a prospective multi-center study with 2359 implants. Clin. Oral Implant. 1997, 8, 161–172. [Google Scholar] [CrossRef]
- Klein, M.O.; Schiegnitz, E.; Al-Nawas, B. Systematic review on success of narrow diameter dental implants. Int. J. Oral Maxillofac. Implant. 2014, 29, 43–54. [Google Scholar] [CrossRef] [Green Version]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Marcello-Machado, R.M.; Faot, F.; Schuster, A.J.; Nascimento, G.G.; Del Bel Cury, A.A. Miniimplants and narrow diameter implants as mandibular overdenture retainers: A systematic review and meta-analysis of clinical and radiographic outcomes. J. Oral Rehabil. 2018, 45, 161–183. [Google Scholar] [CrossRef]
- Al-Nawas, B.; Schiegnitz, E. Augmentation procedures using bone substitute materials or autogenous bone-a systematic review and meta-analysis. Eur. J. oral Implant. 2014, 7, 219–234. [Google Scholar]
- Schiegnitz, E.; Al-Nawas, B.; Kammerer, P.W.; Grotz, K.A. Oral rehabilitation with dental implants in irradiated patients: A meta-analysis on implant survival. Clin. Oral Investig. 2014, 18, 687–698. [Google Scholar] [CrossRef]
- Walter, C.; Al-Nawas, B.; Wolff, T.; Schiegnitz, E.; Grotz, K.A. Dental implants in patients treated with antiresorptive medication-a systematic literature review. Int. J. Implant. Dent. 2016, 2, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Lambert, F.; Botilde, G.; Lecloux, G.; Rompen, E. Effectiveness of temporary implants in teenage patients: A prospective clinical trial. Clin. Oral Implant. Res. 2017, 28, 1152–1157. [Google Scholar] [CrossRef]
- Maryod, W.H.; Ali, S.M.; Shawky, A.F. Immediate versus early loading of mini-implants supporting mandibular overdentures: A preliminary 3-year clinical outcome report. Int. J. Prosthodont. 2014, 27, 553–560. [Google Scholar] [CrossRef] [Green Version]
- Elsyad, M.A.; Gebreel, A.A.; Fouad, M.M.; Elshoukouki, A.H. The clinical and radiographic outcome of immediately loaded mini implants supporting a mandibular overdenture. A 3-year prospective study. J. Oral Rehabil. 2011, 38, 827–834. [Google Scholar] [CrossRef]
- King, P.; Maiorana, C.; Luthardt, R.G.; Sondell, K.; Øland, J.; Galindo-Moreno, P.; Nilsson, P. Clinical and Radiographic Evaluation of a Small-Diameter Dental Implant Used for the Restoration of Patients with Permanent Tooth Agenesis (Hypodontia) in the Maxillary Lateral Incisor and Mandibular Incisor Regions: A 36-Month Follow-Up. Int. J. Prosthodont. 2016, 29, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Maiorana, C.; King, P.; Quaas, S.; Sondell, K.; Worsaae, N.; Galindo-Moreno, P. Clinical and radiographic evaluation of early loaded narrow-diameter implants: 3 years follow-up. Clin. Oral Implant. 2015, 26, 77–82. [Google Scholar] [CrossRef]
- Pieri, F.; Siroli, L.; Forlivesi, C.; Corinaldesi, G. Clinical, esthetic, and radiographic evaluation of small-diameter (3.0-mm) implants supporting single crowns in the anterior region: A 3-year prospective study. Int. J. Periodontics Restor. Dent. 2014, 34, 825–832. [Google Scholar] [CrossRef]
- Moráguez, O.; Vailati, F.; Grütter, L.; Sailer, I.; Belser, U.C. Four-unit fixed dental prostheses replacing the maxillary incisors supported by two narrow-diameter implants—A five-year case series. Clin. Oral Implant. 2017, 28, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Al-Nawas, B.; Meijer, H.J.; Razavi, A.; Reichert, T.E.; Schimmel, M.; Storelli, S.; Romeo, E.; Roxolid Study Group. Small-diameter titanium Grade IV and titanium-zirconium implants in edentulous mandibles: Three-year results from a double-blind, randomized controlled trial. Clin. Oral Implant. 2015, 26, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Arisan, V.; Bölükbaşi, N.; Ersanli, S.; Ozdemir, T. Evaluation of 316 narrow diameter implants followed for 5–10 years: A clinical and radiographic retrospective study. Clin. Oral Implant. 2010, 21, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Al-Aali, K.A.; ArRejaie, A.S.; Alrahlah, A.; AlFawaz, Y.F.; Abduljabbar, T.; Vohra, F. Clinical and radiographic peri-implant health status around narrow diameter implant-supported single and splinted crowns. Clin. Implant. Dent. Relat. 2019, 21, 386–390. [Google Scholar] [CrossRef]
- Al-Shibani, N.; Al-Aali, K.A.; Al-Hamdan, R.S.; Alrabiah, M.; Basunbul, G.; Abduljabbar, T. Comparison of clinical peri-implant indices and crestal bone levels around narrow and regular diameter implants placed in diabetic and non-diabetic patients: A 3-year follow-up study. Clin. Implant. Dent. Relat. 2019, 21, 247–252. [Google Scholar] [CrossRef]
- de Souza, A.B.; Sukekava, F.; Tolentino, L.; César-Neto, J.B.; Garcez-Filho, J.; Araújo, M.G. Narrow and regular-diameter implants in the posterior region of the jaws to support single crowns: A 3-year split-mouth randomized clinical trial. Clin. Oral Implant. 2018, 29, 100–107. [Google Scholar] [CrossRef]
- Shi, J.Y.; Xu, F.Y.; Zhuang, L.F.; Gu, Y.X.; Qiao, S.C.; Lai, H.C. Long-term outcomes of narrow diameter implants in posterior jaws: A retrospective study with at least 8-year follow-up. Clin. Oral Implant. 2018, 29, 76–81. [Google Scholar] [CrossRef]
- Froum, S.J.; Shi, Y.; Fisselier, F.; Cho, S.C. Long-Term Retrospective Evaluation of Success of Narrow-Diameter Implants in Esthetic Areas: A Consecutive Case Series with 3 to 14 Years Follow-up. Int. J. Periodontics Restor. Dent. 2017, 37, 629–637. [Google Scholar] [CrossRef] [Green Version]
- Galindo-Moreno, P.; Nilsson, P.; King, P.; Worsaae, N.; Schramm, A.; Padial-Molina, M.; Maiorana, C. Clinical and radiographic evaluation of early loaded narrow-diameter implants: 5-year follow-up of a multicenter prospective clinical study. Clin. Oral Implant. 2017, 28, 1584–1591. [Google Scholar] [CrossRef] [PubMed]
- Pommer, B.; Mailath-Pokorny, G.; Haas, R.; Busenlechner, D.; Fürhauser, R.; Watzek, G. Patients’ preferences towards minimally invasive treatment alternatives for implant rehabilitation of edentulous jaws. Eur. J. Oral. Implantol. 2014, 7, 91–109. [Google Scholar]
- Safii, S.H.; Palmer, R.M.; Wilson, R.F. Risk of implant failure and marginal bone loss in subjects with a history of periodontitis: A systematic review and meta-analysis. Clin. Implant. Dent. Relat. 2010, 12, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.A.; Bassetti, R.G.; Bosshardt, D.D. The alveolar ridge splitting/expansion technique: A systematic review. Clin. Oral Implant. 2016, 27, 310–324. [Google Scholar] [CrossRef] [PubMed]
- Waechter, J.; Leite, F.R.; Nascimento, G.G.; Carmo Filho, L.C.; Faot, F. The split crest technique and dental implants: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. Res. 2017, 46, 116–128. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implant. 1986, 1, 11–25. [Google Scholar]
- Buser, D.; Weber, H.P.; Lang, N.P. Tissue integration of non-submerged implants: 1-year results of a prospective study with 100 ITI hollow-cylinder and hollow-screw implants. Clin. Oral Implant. 1990, 1, 33–40. [Google Scholar] [CrossRef]
- Schiegnitz, E.; Al-Nawas, B. Narrow-diameter implants: A systematic review and meta-analysis. Clin. Oral Implant. 2018, 29, 21–40. [Google Scholar] [CrossRef] [Green Version]
- Lemos, C.A.; Ferro-Alves, M.L.; Okamoto, R.; Mendonça, M.R.; Pellizzer, E.P. Short dental implants versus standard dental implants placed in the posterior jaws: A systematic review and meta-analysis. J. Dent. 2016, 47, 8–17. [Google Scholar] [CrossRef] [Green Version]
- Assaf, A.; Saad, M.; Daas, M.; Abdallah, J.; Abdallah, R. Use of narrow-diameter implants in the posterior jaw: A systematic review. Implant. Dent. 2015, 24, 294–306. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, C.J.; Singh, M.; Weber, H.P.; Gallucci, G.O. Success criteria in implant dentistry: A systematic review. J. Dent. Res. 2012, 91, 242–248. [Google Scholar] [CrossRef]
- Roos, J.; Sennerby, L.; Lekholm, U.; Jemt, T.; Gröndahl, K.; Albrektsson, T. A qualitative and quantitative method for evaluating implant success: A 5-year retrospective analysis of the Brånemark implant. Int. J. Oral Maxillofac. Implant. 1997, 12, 504–514. [Google Scholar]
- Di Girolamo, M.; Calcaterra, R.; DI Gianfilippo, R.; Arcuri, C.; Baggi, L. Bone level changes around platform switching and platform matching implants: A systematic review with meta-analysis. Oral Implantol. 2016, 13, 1–10. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Type of Study | Number of Patients | Age (Range) | Diameter (mm) Length (mm) | Number of Implants | Location (Maxilla/ Mandible) | Type of Restoration | Follow-up | Failure; Survival Rate; Succes Rate, Implant | Mean Marginal Bone Loss (mm) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| M | F | ||||||||||
| Lambert et al. 2017 (17) | CT | 6 | 14 | 15.6 (13–19) | 2 × 10; 13 | 30 | MAX/MAND | Single crowns in anterior sector | 42 | 1; 96.6%; ND | −1.09 ± 1.74 |
| 2.5 × 10; 13 | |||||||||||
| Maryod et al. 2014 (18) | RCT | 20 | 16 | 64.1 | 1.8 × 15 | 120 | MAND | Overdenture | 36 | 7; 94.2%; ND | ND |
| Elsyad, et al. 2011 (19) | CT | 16 | 12 | 62.9 (49–75) | 1.8 × 12; 18 | 112 | MAND | Overdenture | 36 | 4; 96.4%; 92.90% | −1.26 ± 0.64 |
| King et al. 2016 (20) | CT | 18 | 20 | 24 | 3.0 × 11; 15 | 62 | MAX/MAND | Single crowns in anterior sector | 36 | 2; 96.8%; ND | −0.23 |
| Maiorana et al. 2015 (21) | CT | 36 | 33 | 32 | 3.0 × 11; 15 | 97 | MAX/MAND | Single crowns in anterior sector | 36 | 4; 95.9%; ND | −0.09 |
| Pieri et al. 2014 (22) | CT | 18 | 32 | 41.58 (19–64) | 3.0 × 11; 15 | 50 | MAX/MAND | Single crowns in anterior sector | 36 | 0; 100%; 100% | −0.24 ± 0.15 |
| Moraguez et al. 2017 (23) | CS | 4 | 6 | 49.4 (32–68) | 3.3 × 10; 12 | 20 | MAX | Single crowns in anterior sector | 60 | 0;100%; ND | −2.17 ± 0.38 |
| Quirynen et al. 2015 (24) | RTC | 40 | 49 | 65.8 | 3.3 × 8; 14 | 75 (titanium implants) | MAND | Overdenture | 36 | 2; 97.3%; 97.3% | −0.6 ± 0.71 |
| Arisan et al. 2010 (25) | Cohort | 66 | 73 | 55.3 (21–80) | 3.3 × 8; 14, 9.5; 15 | 316 | ND | Overdenture; Single crowns in anterior sector | 124 | 14; 95.6%; 91.40% | −1.32 ± 0.13 maxilla |
| 3.4 × 8; 14, 9.5; 15 | −1.28 ± 0.14 mandible | ||||||||||
| Al-Aali et al. 2018 (26) | Cohort | 43 | 35 | ≥25 | 3.3 × 10; 12 | 102 | MAND | Crowns posterior sector | 42 | ND | −1.17 ± 0.06 |
| Al-Shibani et al. 2018 (27) | CT | 44 | 41.6 (30–50) | 3.3 × 10 | 25 | MAND | Crowns posterior sector | 36 | 0; 100%; ND | 0.15 (0.1–0.4) | |
| De Souza et al. 2017 (28) | RTC | 10 | 12 | 59.2 | 3.3 × 6; 12 | 22 | MAX/MAND | Crowns posterior sector | 36 | 0; 100%; 95% | −0.58 ± 0.39 |
| Yu-Shi et al. 2017 (29) | Cohort | 38 | 29 | 35.6 (21–56) | 3.3 × 10; 12 | 98 | MAX/MAND | Crowns posterior sector | 121 | 3; 96.9%; ND | −1.19 ± 1.07 |
| Froum et al. 2017 (30) | CS | 6 | 8 | 48.6 (23–87) | 1.8 × 7; 10; 14 | 19 | MAX/MAND | Single crowns in anterior sector | 137 | 0; 100%; 84% | −0.16 |
| 2.2 × 7; 10; 14 | |||||||||||
| 2.4 × 7; 10; 14 | |||||||||||
| Galindo-Moreno et al. 2017 (31) | CT | 36 | 33 | 32.5 (18–72) | 3 × 11; 13; 15 | 97 | MAX/MAND | Single crowns in anterior sector | 60 | 4; 92.8%; ND | −0.15 |
| Author | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Researchers | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Outcome Reporting | Other Sources of Bias |
|---|---|---|---|---|---|---|---|
| Maryod et al. 2014 (18) |  | |  |  | | | |
| Quirynen et al. 2015 (24) | | | | | | | |
| De Souza et al. 2017 (28) | | | | | | | |
| Author | A Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Collection of Data | Endpoints Appropriate to the Aim of the Study | Unbiased Assessment of the Study Endpoint | Follow-up Period Appropriate to the Aim of the Study | Loss to Follow up Less than 5% | Prospective Calculation of the Study Size | An Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analyses |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lambert et al. 2017 (17) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 0 | NE | NE | NE | NE |
| Elsyad, et al. 2011 (19) | 2 | 2 | 2 | 2 | 0 | 2 | 1 | 2 | NE | NE | NE | NE |
| King et al. 2016 (20) | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | NE | NE | NE | NE |
| Maiorana et al. 2015 (21) | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | NE | NE | NE | NE |
| Pieri et al. 2014 (22) | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | NE | NE | NE | NE |
| Arisan et al. 2010 (25) | 2 | 2 | 2 | 1 | 0 | 2 | 2 | 0 | NE | NE | NE | NE |
| Al-Aali et al. 2018 (26) | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | NE | NE | NE | NE |
| Al-Shibani et al. 2018 (27) | 2 | 2 | 2 | 2 | 0 | 2 | 1 | 0 | 0 | 2 | 2 | 0 |
| Yu-Shi et al. 2017 (29) | 2 | 2 | 2 | 2 | 0 | 2 | 1 | 0 | NE | NE | NE | NE |
| Galindo-Moreno et al. 2017 (31) | 2 | 2 | 2 | 2 | 0 | 2 | 0 | 0 | NE | NE | NE | NE |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Valls, G.; Roca-Millan, E.; Céspedes-Sánchez, J.M.; González-Navarro, B.; Torrejon-Moya, A.; López-López, J. Narrow Diameter Dental Implants as an Alternative Treatment for Atrophic Alveolar Ridges. Systematic Review and Meta-Analysis. Materials 2021, 14, 3234. https://doi.org/10.3390/ma14123234
González-Valls G, Roca-Millan E, Céspedes-Sánchez JM, González-Navarro B, Torrejon-Moya A, López-López J. Narrow Diameter Dental Implants as an Alternative Treatment for Atrophic Alveolar Ridges. Systematic Review and Meta-Analysis. Materials. 2021; 14(12):3234. https://doi.org/10.3390/ma14123234
Chicago/Turabian StyleGonzález-Valls, Georgina, Elisabet Roca-Millan, Juan Manuel Céspedes-Sánchez, Beatriz González-Navarro, Aina Torrejon-Moya, and José López-López. 2021. "Narrow Diameter Dental Implants as an Alternative Treatment for Atrophic Alveolar Ridges. Systematic Review and Meta-Analysis" Materials 14, no. 12: 3234. https://doi.org/10.3390/ma14123234
APA StyleGonzález-Valls, G., Roca-Millan, E., Céspedes-Sánchez, J. M., González-Navarro, B., Torrejon-Moya, A., & López-López, J. (2021). Narrow Diameter Dental Implants as an Alternative Treatment for Atrophic Alveolar Ridges. Systematic Review and Meta-Analysis. Materials, 14(12), 3234. https://doi.org/10.3390/ma14123234