
The Application of Beta-Tricalcium Phosphate in Implant Dentistry: A Systematic Evaluation of Clinical Studies

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Questions
- Primary question: Is the survival rate of dental implants placed simultaneously with bone regeneration procedures using β-TCP similar to the same procedures using another type of graft material, or similar to dental implants placed without graft material?
- Secondary Question: Are other clinical, radiographic or histologic parameters similar to the same procedures using another type of graft material, or similar to dental implants placed without using graft material?
2.2. PICO Question
2.3. Eligibility Criteria
- Completely or partially edentulous human adults.
- Placement of dental implants simultaneously with the use of β-TCP.
- Controlled and non-controlled studies.
- Randomized clinical trials, controlled clinical trials, clinical trials, clinical studies, comparative studies, observational studies.
- Studies evaluating implant survival rate.
- Case reports and case series.
- Studies in which implants are placed in second stage after bone regeneration.
- β-TCP in combination with platelet concentrates or other biomaterials.
- Immediately loaded dental implants, to avoid the added risk of dental implant failure.
2.4. Search Strategy
2.5. Study Selection
2.6. Data Extraction
2.7. Quality Assessment and Risk of Bias
2.8. Data Synthesis and Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Methods and Characteristics
3.3. Quality Assessment and Risk of Bias
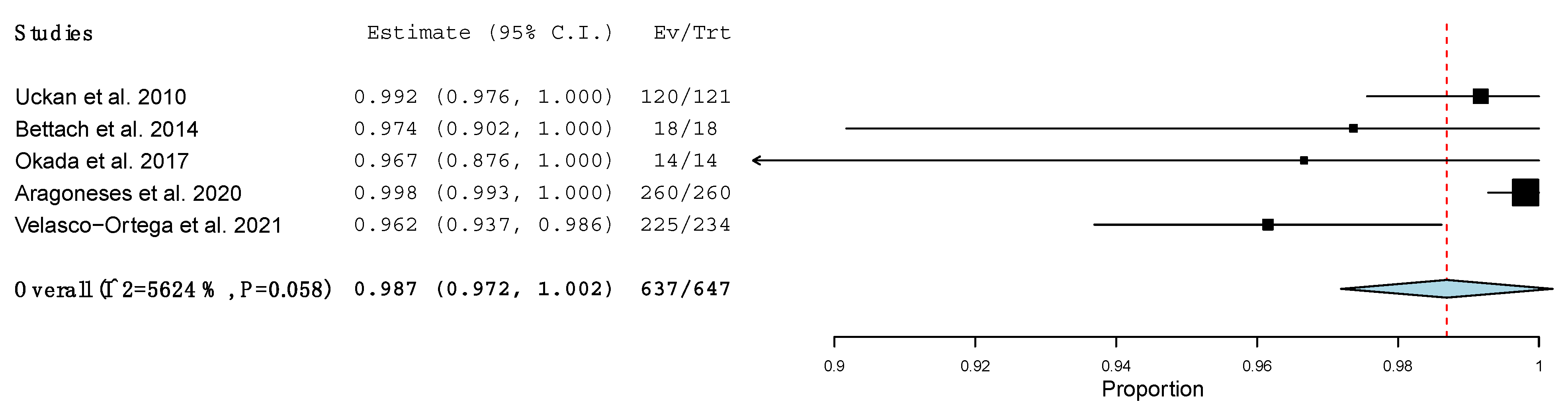
3.4. Implant Survival Rate
Meta-Analysis
3.5. Radiographic Parameters
3.6. Clinical Parameters
3.7. Histological Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Elani, H.W.; Starr, J.R.; Da Silva, J.D.; Gallucci, G.O. Trends in Dental Implant Use in the U.S., 1999–2016, and Projections to 2026. J. Dent Res. 2018, 97, 1424–1430. [Google Scholar] [CrossRef]
- Sekerci, E.; Lambrecht, J.T.; Mukaddam, K.; Kühl, S. Status report on dental implantology in Switzerland. An updated cross-sectional survey. Swiss Dent J. 2020, 130, 486–492. [Google Scholar]
- McAllister, B.S.; Haghighat, K. Bone Augmentation Techniques. J. Periodontol. 2007, 78, 377–3396. [Google Scholar] [CrossRef] [Green Version]
- Yamada, M.; Egusa, H. Current bone substitutes for implant dentistry. J. Prosthodont Res. 2018, 62, 152–161. [Google Scholar] [CrossRef]
- Bohner, M.; Santoni, B.L.G.; Döbelin, N. β-tricalcium phosphate for bone substitution: Synthesis and properties. Acta Biomater. 2020, 113, 23–41. [Google Scholar] [CrossRef]
- Papageorgiou, S.N.; Papageorgiou, P.N.; Deschner, J.; Götz, W. Comparative effectiveness of natural and synthetic bone grafts in oral and maxillofacial surgery prior to insertion of dental implants: Systematic review and network meta-analysis of parallel and cluster randomized controlled trials. J. Dent. 2016, 48, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Rosello-Labres, X.; Rosello-Camps, A.; Jané-Salas, E.; Albuquerque, R.; Velasco-Ortega, E.; López-López, J. Graft Materials in Oral Surgery: Revision. J. Biomim. Biomater. Tissue Eng. 2014, 19, 8. [Google Scholar]
- Sheikh, Z.; Najeeb, S.; Khurshid, Z.; Verma, V.; Rashid, H.; Glogauer, M. Biodegradable Materials for Bone Repair and Tissue Engineering Applications. Materials 2015, 8, 5744–5794. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, R.A.; Mazor, Z.; Foitzik, C.; Prasad, H.; Rohrer, M.; Palti, A. β-tricalcium phosphate as bone substitute material: Properties and clinical applications. J. Osseointegr. 2010, 2, 61–68. [Google Scholar]
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone grafts: Which is the ideal biomaterial? J. Clin. Periodontol. 2019, 46, 92–102. [Google Scholar] [CrossRef]
- Sheikh, Z.; Hamdan, N.; Ikeda, Y.; Grynpas, M.; Ganss, B.; Glogauer, M. Natural graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive applications: A review. Biomater. Res. 2017, 21, 1–20. [Google Scholar] [CrossRef]
- Ebrahimi, M.; Botelho, M.G.; Dorozhkin, S.V. Biphasic calcium phosphates bioceramics (HA/TCP): Concept, physicochemical properties and the impact of standardization of study protocols in biomaterials research. Mater. Sci. Eng. 2017, 71, 1293–1312. [Google Scholar] [CrossRef]
- Owen, G.R.; Dard, M.; Larjava, H. Hydoxyapatite/beta-tricalcium phosphate biphasic ceramics as regenerative material for the repair of complex bone defects. J. Biomed. Mater. Res. 2018, 106, 2493–2512. [Google Scholar] [CrossRef] [PubMed]
- Tavoni, M.; Dapporto, M.; Tampieri, A.; Sprio, S. Bioactive Calcium Phosphate-Based Composites for Bone regeneration. J. Compos. Sci. 2021, 5, 227. [Google Scholar] [CrossRef]
- Chappard, D. Beta-tricalcium phosphate and bone surgery: Editorial. Morphologie 2017, 101, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Zhou, Y.; Ma, Y.; Xiao, L.; Ji, W.; Zhang, Y.; Wang, X. Current Application of Beta-Tricalcium Phosphate in Bone Repair and Its Mechanism to Regulate Osteogenesis. Front. Mater. 2021, 8, 698915. [Google Scholar] [CrossRef]
- Cheah, C.W.; Al-Namnam, N.M.; Lau, M.N.; Lim, G.S.; Raman, R.; Fairbairn, P.; Ngeow, W.C. Synthetic Material for Bone, Periodontal, and Dental Tissue Regeneration: Where Are We Now, and Where Are We Heading Next? Materials 2021, 14, 6123. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; senior clinical research fellow; Cheng, H.-Y.; Corbett, M.S.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Zijderveld, S.A.; Schulten, E.A.J.M.; Aartman, I.H.A.; ten Bruggenkate, C.M. Long-term changes in graft height after maxillary sinus floor elevation with different grafting materials: Radiographic evaluation with a minimum follow-up of 4.5 years. Clin. Oral Implant. Res. 2009, 20, 691–700. [Google Scholar] [CrossRef]
- Bonardi, J.P.; dos Santos Pereira, R.; Lima FB DJ, B.; Faverani, L.P.; Griza, G.L.; Okamoto, R.; Hochuli-Vieira, E. Prospective and Randomized Evaluation of ChronOS and Bio-Oss in Human Maxillary Sinuses: Histomorphometric and Immunohistochemical Assignment for Runx 2, Vascular Endothelial Growth Factor, and Osteocalcin. J. Oral Maxillofac. Surg. 2018, 76, 325–335. [Google Scholar] [CrossRef] [Green Version]
- Ozyuvaci, H.; Bilgiç, B.; Firatli, E. Radiologic and Histomorphometric Evaluation of Maxillary Sinus Grafting with Alloplastic Graft Materials. J. Periodontol. 2003, 74, 909–915. [Google Scholar] [CrossRef]
- Merli, M.; Moscatelli, M.; Mariotti, G.; Pagliaro, U.; Raffaelli, E.; Nieri, M. Comparing membranes and bone substitutes in a one-stage procedure for horizontal bone augmentation. A double-blind randomised controlled trial. Eur. J. Oral Implantol. 2015, 8, 271–281. [Google Scholar]
- Uckan, S.; Deniz, K.; Dayangac, E.; Araz, K.; Özdemir, B.H. Early Implant Survival in Posterior Maxilla With or Without β-Tricalcium Phosphate Sinus Floor Graft. J. Oral Maxillofac. Surg. 2010, 68, 1642–1645. [Google Scholar] [CrossRef]
- Daif, E.T. Effect of a Multiporous Beta–Tricalicum Phosphate on Bone Density Around Dental Implants Inserted Into Fresh Extraction Sockets. J. Oral Implantol. 2013, 39, 339–344. [Google Scholar] [CrossRef]
- Trombelli, L.; Franceschetti, G.; Stacchi, C.; Minenna, L.; Riccardi, O.; Di Raimondo, R.; Rizzi, A.; Farina, R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or β-tricalcium phosphate: A multicenter, double-blind, randomized, controlled clinical trial. J. Clin. Periodontol. 2014, 41, 311–319. [Google Scholar] [CrossRef]
- Marković, A.; Mišić, T.; Calvo-Guirado, J.L.; Delgado-Ruíz, R.A.; Janjić, B.; Abboud, M. Two-Center Prospective, Randomized, Clinical, and Radiographic Study Comparing Osteotome Sinus Floor Elevation with or without Bone Graft and Simultaneous Implant Placement: Osteotome Sinus Floor Elevation with versus without Bone Graft. Clin. Implant. Dent. Relat. Res. 2016, 18, 873–882. [Google Scholar] [CrossRef]
- Steigmann, M.; Garg, A.K. A Comparative Study of Bilateral Sinus Lifts Performed with Platelet-Rich Plasma Alone Versus Alloplastic Graft Material Reconstituted with Blood. Implant Dent. 2005, 14, 261–266. [Google Scholar] [CrossRef] [Green Version]
- Merli, M.; Moscatelli, M.; Mariotti, G.; Pagliaro, U.; Raffaelli, E.; Nieri, M. Comparing membranes and bone substitutes in a one-stage procedure for horizontal bone augmentation. Three-year post-loading results of a double-blind randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 441–452. [Google Scholar]
- Bettach, R.; Guillaume, B.; Taschieri, S.; Del Fabbro, M. Clinical Performance of a Highly Porous Beta-TCP as the Grafting Material for Maxillary Sinus Augmentation. Implant Dent. 2014, 23, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Okada, T.; Kanai, T.; Tachikawa, N.; Munakata, M.; Kasugai, S. Histological and Histomorphometrical Determination of the Biogradation of β-Tricalcium Phosphate Granules in Maxillary Sinus Floor Augmentation: A Prospective Observational Study. Implant Dent. 2017, 26, 275–283. [Google Scholar] [CrossRef]
- Aragoneses Lamas, J.M.; Gómez Sánchez, M.; Cuadrado González, L.; Suárez García, A.; Aragoneses Sánchez, J. Vertical Bone Gain after Sinus Lift Procedures with Beta-Tricalcium Phosphate and Simultaneous Implant Placement—A Cross-Sectional Study. Medicina 2020, 56, 609. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Ortega, E.; Sierra-Baztan, A.; Jiménez-Guerra, A.; España-López, A.; Ortiz-Garcia, I.; Núñez-Márquez, E.; Moreno-Muñoz, J.; Rondón-Romero, J.L.; López-López, J.; Monsalve-Guil, L. Long-Term Clinical Study of Implants Placed in Maxillary Sinus Floor Augmentation Using Beta-Tricalcium Phosphate. Int. J. Environ. Res. Public Health 2021, 18, 9975. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Moscatelli, M.; Mariotti, G.; Pagliaro, U.; Breschi, L.; Mazzoni, A.; Nieri, M. Membranes and Bone Substitutes in a One-Stage Procedure for Horizontal Bone Augmentation: A Histologic Double-Blind Parallel Randomized Controlled Trial. Int. J. Periodontics Restor. Dent. 2015, 35, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suba, Z.; Takács, D.; Matusovits, D.; Barabás, J.; Fazekas, A.; Szabó, G. Maxillary sinus floor grafting with β-tricalcium phosphate in humans: Density and microarchitecture of the newly formed bone. Clin. Oral Implant. Res. 2006, 17, 102–108. [Google Scholar] [CrossRef]
- Szabó, G.; Huys, L.; Coulthard, P.; Malorana, C.; Garagiola, U.; Barabás, J.; Németh, Z.; Hrabák, K.; Suba, Z. A prospective multicenter randomized clinical trial of autogenous bone versus β-tricalcium phosphate graft alone for bilateral sinus elevation: Histologic and histomorphometric evaluation. Int. J. Oral Maxillofac. Implant. 2005, 20, 371–381. [Google Scholar] [CrossRef]
- Jasser, R.A.; AlSubaie, A.; AlShehri, F. Effectiveness of beta-tricalcium phosphate in comparison with other materials in treating periodontal infra-bony defects around natural teeth: A systematic review and meta-analysis. BMC Oral Health 2021, 21, 1–14. [Google Scholar] [CrossRef]
- Guillaume, B. Filling bone defects with β-TCP in maxillofacial surgery: A review. Morphologie 2017, 101, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Ormianer, Z.; Palti, A.; Shifman, A. Survival of immediately loaded dental implants in deficient alveolar bone sites augmented with beta-tricalcium phosphate. Implant Dent. 2006, 15, 395–403. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Type of Study | N Control | N Test | Control Material | Test Material | Procedure | Follow-up (months) | Survival Rate (Implant Failures) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patients | Implants | Patients | Implants | ||||||||
| Steigmann et al., 2005 [29] | USA | Split mouth RCT | 20 | Not specified | 20 | Not Specified | PRP | β-TCP | LMSA or TSL | 6 | 100% (0) |
| Uckan et al., 2010 [25] | Turkey | CT | 65 | 136 | 62 | 121 | Alveolar ridge | β-TCP | LMSA | CG 32.3; TG 29.8 | CG 99.26% (1); TG 99.17% (1) |
| Daif et al., 2013 [26] | Egypt | RCT | 14 | 14 | 14 | 14 | Blood clot | β-TCP | Immediate implants | 6 after loading | 100% (0) |
| Trombelli et al., 2014 [27] | Italy | RCT | 19 | 19 | 19 | 19 | DBB | β-TCP | TSL | 6 | 100% (0) |
| Markovic et al., 2016 [28] | Serbia | RCT | 45 | 45 | 45 | 135 (45 every test group) | Blood clot | T1 β-TCP; T2 DBB; T3 β-TCP+DBB | TSL | 24 after loading | 100% (0) |
| Merli et al., 2018 [30] | Italy | RCT | 18 | 23 | 14 | 16 | DBB | β-TCP | HBA | 36 after loading | 100% (0) |
| Author | Country | Type of Study | N | Procedure | Follow-up (months) | Survival Rate (Implant Failures) | |
|---|---|---|---|---|---|---|---|
| Patients | Implants | ||||||
| Bettach et al., 2014 [31] | France | Retrospective study | 4 | 18 | LMSA | 22–52 | 100% (0) |
| Okada et al., 2017 [32] | Japan | Prospective study | 7 | 14 | LMSA | 37–46 | 100% (0) |
| Aragoneses et al., 2020 [33] | Dominican Republic | Cross-sectional study | 119 | 260 | LMSA | 6 | 100% (0) |
| Velasco-Ortega et al., 2021 [34] | Spain | Prospective study | 101 | 234 | LMSA | 104–146 | 96.2% (9) |
| Product | Company |
|---|---|
| Adbone® TCP | Medbone Biomaterials, Lisboa, Portugal |
| Bonegraft® | Bonegraft biomaterials, Turkey |
| Cerasorb-Curasan® | Ancladen, Barcelona, Spain |
| Iceberg™ TCP | Global Medical Implants, Madrid, Spain |
| IngeniOs® | Zimmer Biomet, Indiana, USA |
| KeraOs® | Keramat, Coruña, Spain |
| MimetikOss® (20% β-TCP and 80% CDHA) | Mimetis Biomaterials, Barcelona, Spain |
| OSTEOwelt® | Biolot Medical, Turkey |
| Osteoblast® | Galimplant, Sarria, Spain |
| Powerbone® | Medical Expo Bonegraft Biomaterials, Madrid, Spain |
| R.T.R. Fosfato tricálcico Septodent® | Broquer dental , Barcelona, Spain // Contidental, Barcelona, Spain |
| Straumann® BoneCeramic™ | Manohay Dental SA, Alcobendas, Spain |
| Suprabone TCP® | BMT Group, Madrid, Spain-Turkey |
| SynMax® (40% β-TCP and 60% (hydroxyapatite) | BioHorizons, Madrid, Spain |
| Trioss® | Dilesa, Paterna, Spain |
| 4MATRIX+® (40% β-TCP, 60% HA and hydrogel) | MIS Implants Technologies Ltd, Israel |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roca-Millan, E.; Jané-Salas, E.; Marí-Roig, A.; Jiménez-Guerra, Á.; Ortiz-García, I.; Velasco-Ortega, E.; López-López, J.; Monsalve-Guil, L. The Application of Beta-Tricalcium Phosphate in Implant Dentistry: A Systematic Evaluation of Clinical Studies. Materials 2022, 15, 655. https://doi.org/10.3390/ma15020655
Roca-Millan E, Jané-Salas E, Marí-Roig A, Jiménez-Guerra Á, Ortiz-García I, Velasco-Ortega E, López-López J, Monsalve-Guil L. The Application of Beta-Tricalcium Phosphate in Implant Dentistry: A Systematic Evaluation of Clinical Studies. Materials. 2022; 15(2):655. https://doi.org/10.3390/ma15020655
Chicago/Turabian StyleRoca-Millan, Elisabet, Enric Jané-Salas, Antonio Marí-Roig, Álvaro Jiménez-Guerra, Iván Ortiz-García, Eugenio Velasco-Ortega, José López-López, and Loreto Monsalve-Guil. 2022. "The Application of Beta-Tricalcium Phosphate in Implant Dentistry: A Systematic Evaluation of Clinical Studies" Materials 15, no. 2: 655. https://doi.org/10.3390/ma15020655
APA StyleRoca-Millan, E., Jané-Salas, E., Marí-Roig, A., Jiménez-Guerra, Á., Ortiz-García, I., Velasco-Ortega, E., López-López, J., & Monsalve-Guil, L. (2022). The Application of Beta-Tricalcium Phosphate in Implant Dentistry: A Systematic Evaluation of Clinical Studies. Materials, 15(2), 655. https://doi.org/10.3390/ma15020655