
The Biomechanical Impact of Loss of an Implant in the Treatment with Mandibular Overdentures on Four Nonsplinted Mini Dental Implants: A Finite Element Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
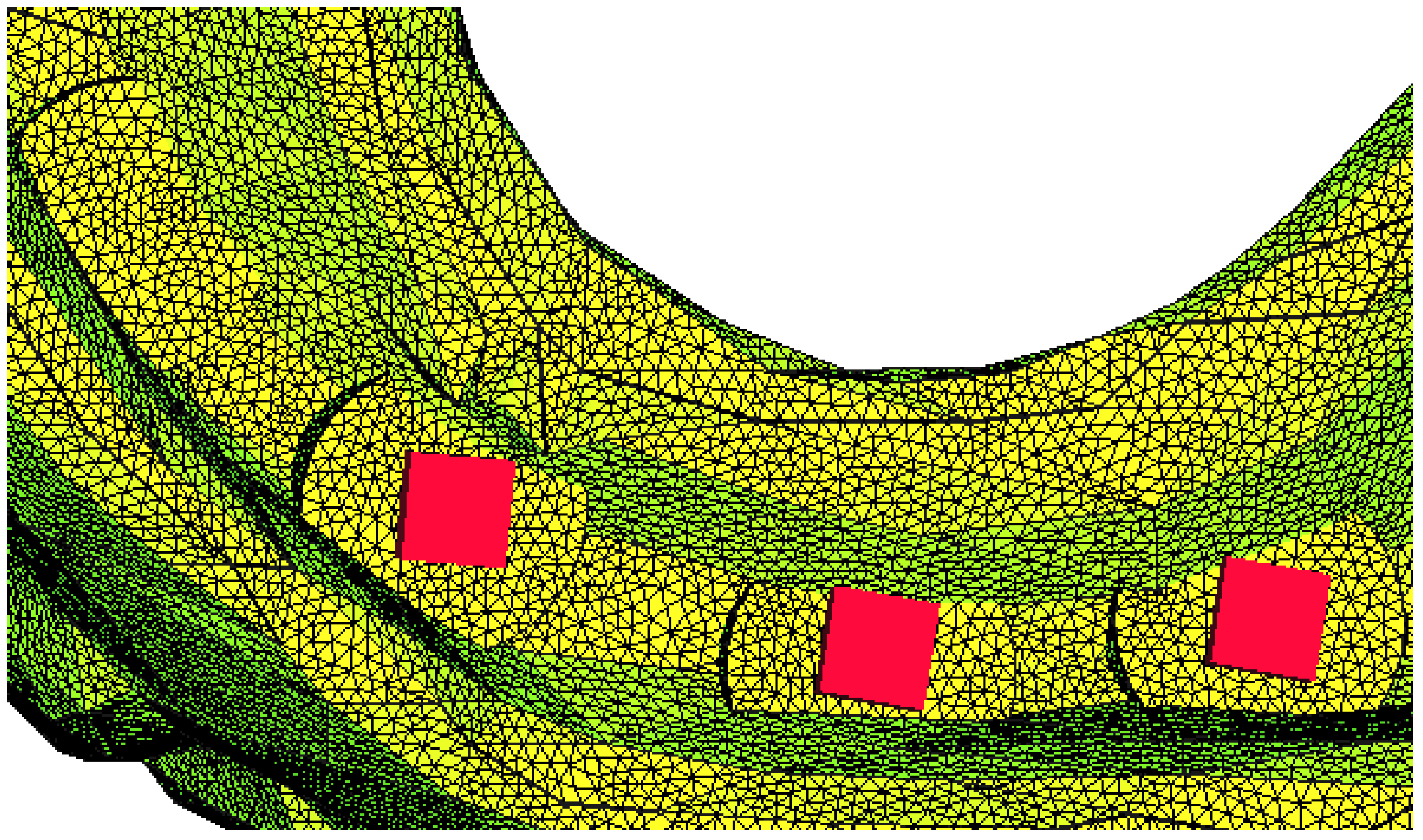
2.1. Finite Element Modeling of the Mandibular Overdenture
2.2. Boundary Conditions
3. Results
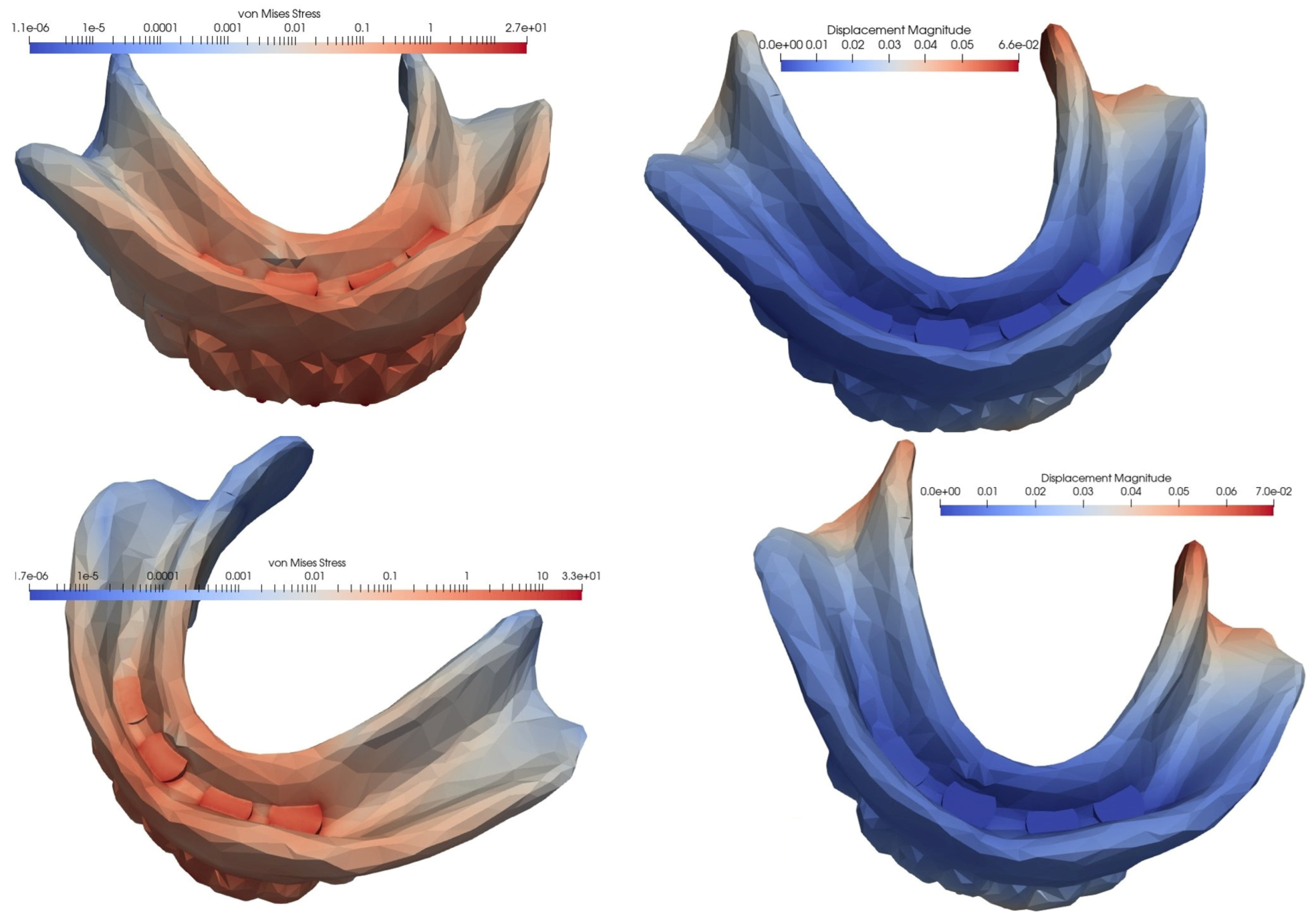
3.1. Loading of an Overdenture on four MDIs Inserted in the Interforaminal Area
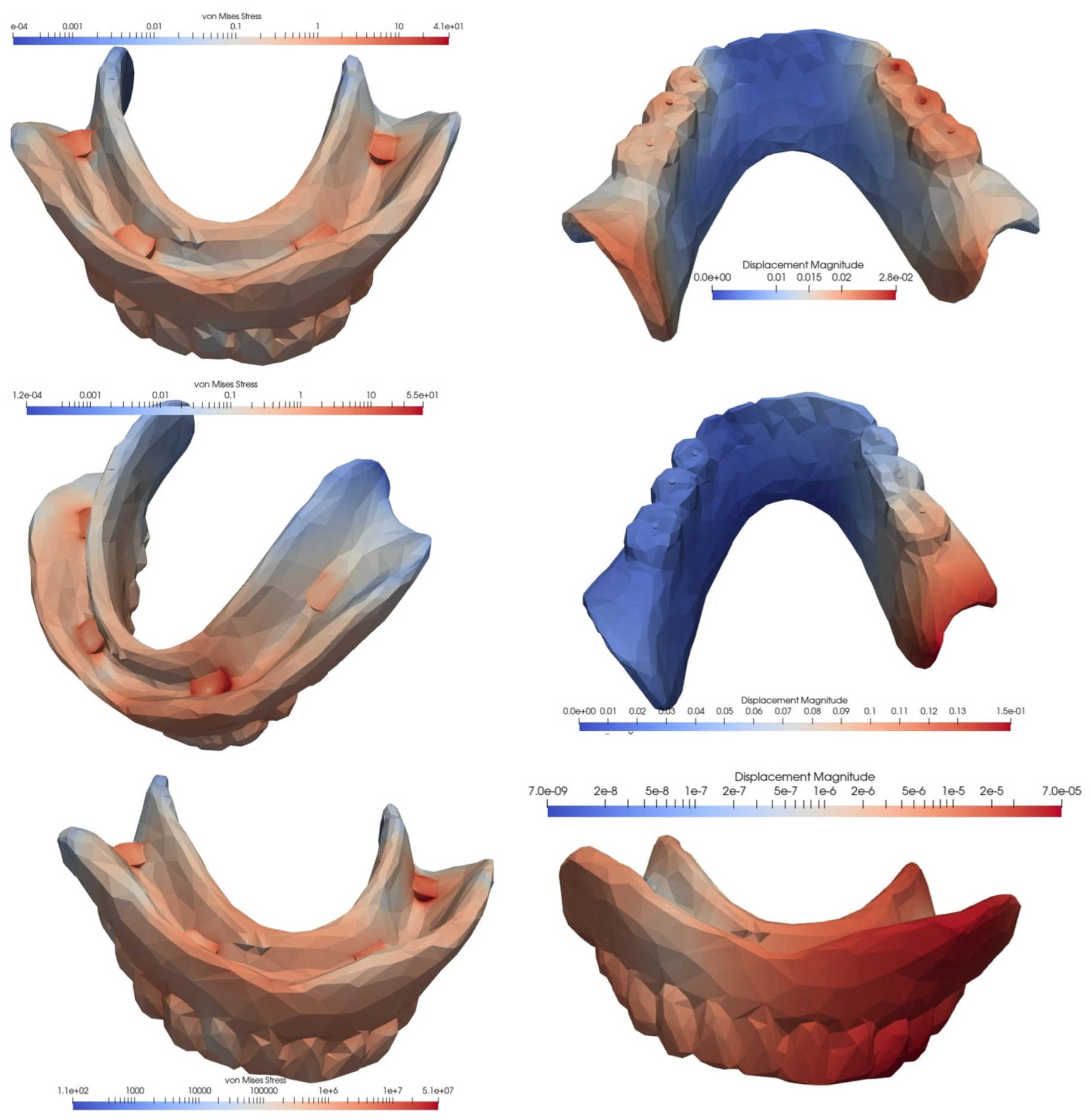
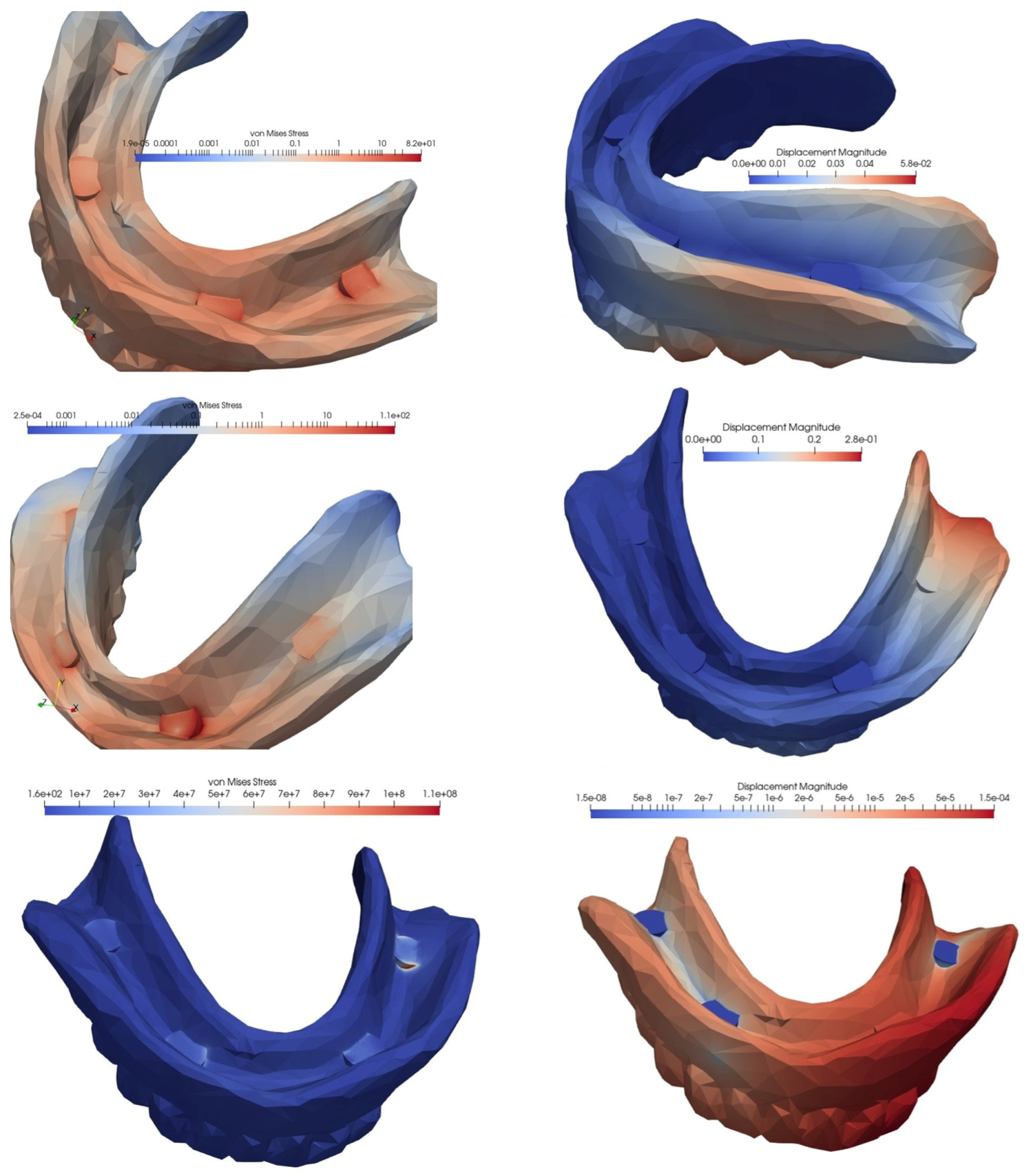
3.2. Loading of an Overdenture on Four MDIs Inserted in the Canine and Molar Areas
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- United Nations Department of Economic and Social Affairs, Population Division. World Population Prospects 2022: Summary of Results; UN DESA/POP/2022/TR/NO. 3; UN: New York, NY, USA, 2022. [Google Scholar]
- Polzer, I.; Schimmel, M.; Müller, F.; Biffar, R. Edentulism as Part of the General Health Problems of Elderly Adults. Int. Dent. J. 2010, 60, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Preoteasa, E.; Păuna, M. Aspecte Practice În Protezarea Edentației Totale; Cermaprint S.R.L.: Bucharest, Romania, 2002; pp. 229–231. [Google Scholar]
- Alvarez-Arenal, A.; Gonzalez-Gonzalez, I.; DeLlanos-Lanchares, H.; Brizuela-Velasco, A.; Martin-Fernandez, E.; Ellacuria-Echebarria, J. Influence of Implant Positions and Occlusal Forces on Peri-Implant Bone Stress in Mandibular Two-Implant Overdentures: A 3-Dimensional Finite Element Analysis. J. Oral Implantol. 2017, 43, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Preoteasa, E.; Imre, M.M.; Preoteasa, C.T. A 3-Year Follow-up Study of Overdentures Retained by Mini-Dental Implants. Int. J. Oral Maxillofac. Implant. 2014, 29, 1170–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melescanu Imre, M.; Marin, M.; Preoteasa, E.; Tancu, A.M.; Preoteasa, C.T. Two Implant Overdenture-the First Alternative Treatment for Patients with Complete Edentulous Mandible. J. Med. Life 2011, 4, 207–209. [Google Scholar]
- Preoteasa, E.; Imre, M.; Lerner, H.; Tancu, A.M.; Preoteasa, C.T. Narrow Diameter and Mini Dental Implant Overdentures. In Emerging Trends in Oral Health Sciences and Dentistry; Virdi, M.S., Ed.; IntechOpen: Rijeka, Croatia, 2015. [Google Scholar] [CrossRef] [Green Version]
- Iosif, L.; Preoteasa, C.T.; Preoteasa, E.; Ispas, A.; Ilinca, R.; Murariu-Mǎgureanu, C.; Amza, O.E. Oral Health Related Quality of Life and Prosthetic Status among Institutionalized Elderly from the Bucharest Area: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 6663. [Google Scholar] [CrossRef]
- Batisse, C.; Bonnet, G.; Veyrune, J.L.; Nicolas, E.; Bessadet, M. Predictive Parameters of Oral Health Quality of Life in Complete Mandibular Denture Wearers Stabilized by Mini-Implants: A Two-Year Follow-up Study. Materials 2017, 10, 1197. [Google Scholar] [CrossRef] [Green Version]
- Borges, G.A.; Codello, D.J.; Del Rio Silva, L.; Dini, C.; Barão, V.A.R.; Mesquita, M.F. Factors and Clinical Outcomes for Standard and Mini-Implants Retaining Mandibular Overdentures: A Systematic Review and Meta-Analysis. J. Prosthet. Dent. 2022, 1–13. [Google Scholar] [CrossRef]
- Bidra, A.S.; Almas, K. Mini Implants for Definitive Prosthodontic Treatment: A Systematic Review. J. Prosthet. Dent. 2013, 109, 156–164. [Google Scholar] [CrossRef]
- Preoteasa, E.; Meleşcanu-Imre, M.; Preoteasa, C.T.; Marin, M.; Lerner, H. Aspects of Oral Morphology as Decision Factors in Mini-Implant Supported Overdenture. Rom. J. Morphol. Embryol. 2010, 51, 309–314. [Google Scholar]
- Chatzopoulos, G.S.; Wolff, L.F. Dental Implant Failure and Factors Associated with Treatment Outcome: A Retrospective Study. J. Stomatol. Oral Maxillofac. Surg. 2022, in press. [Google Scholar] [CrossRef]
- Radi, I.A.W.; Ibrahim, W.; Iskandar, S.M.S.; AbdelNabi, N. Prognosis of Dental Implants in Patients with Low Bone Density: A Systematic Review and Meta-Analysis. J. Prosthet. Dent. 2018, 120, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Karasan, D.; Todorovic, A.; Ligoutsikou, M.; Pjetursson, B.E. Prosthetic Failures in Dental Implant Therapy. Periodontol. 2000 2022, 88, 130–144. [Google Scholar] [CrossRef] [PubMed]
- El Askary, A.S.; Meffert, R.M.; Griffin, T. Why Do Dental Implants Fail? Part II. Implant Dent. 1999, 8, 265–277. [Google Scholar] [CrossRef]
- Lemos, C.A.A.; Verri, F.R.; de Souza Batista, V.E.; Júnior, J.F.S.; Mello, C.C.; Pellizzer, E.P. Complete Overdentures Retained by Mini Implants: A Systematic Review. J. Dent. 2017, 57, 4–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cernescu, A.; Faur, N.; Bortun, C.; Hluscu, M. A Methodology for Fracture Strength Evaluation of Complete Denture. Eng. Fail. Anal. 2011, 18, 1253–1261. [Google Scholar] [CrossRef]
- Sheng, T.J.; Shafee, M.F.; Ariffin, Z.; Jaafar, M. Review on Poly-Methyl Methacrylate as Denture Base Materials. Malays. J. Microsc. 2018, 14, 1–16. [Google Scholar]
- Cheng, Y.Y.; Cheung, W.L.; Chow, T.W. Strain Analysis of Maxillary Complete Denture with Three-Dimensional Finite Element Method. J. Prosthet. Dent. 2010, 103, 309–318. [Google Scholar] [CrossRef]
- Velasco-Ortega, E.; del Rocío Jiménez-Martin, I.; Moreno-Muñoz, J.; Núñez-Márquez, E.; Rondón-Romero, J.L.; Cabanillas-Balsera, D.; Jiménez-Guerra, Á.; Ortiz-García, I.; López-López, J.; Monsalve-Guil, L. Long-Term Treatment Outcomes of Implant Prostheses in Partially and Totally Edentulous Patients. Materials 2022, 15, 4910. [Google Scholar] [CrossRef]
- Gavrila-Ardelean, L.; Gavrila-Ardelean, M. The Flexural Strength of Traditional and Modern Acrylic Prosthetic Bases. Mater. Plast. 2020, 57, 111–116. [Google Scholar] [CrossRef]
- Preoteasa, E.; Găvan, M.; Preoteasa, C.T.; Murariu Măgureanu, C. Ranforsarea Bazelor Acrilice Cu Agenți Fibrilari Și Cu Pulberi; Cermaprint S.R.L.: Bucharest, Romania, 2008; pp. 70, 360. [Google Scholar]
- Mocanu, R.G.; Preoteasa, C.; Meghea, D.; Preoteasa, E.; Florica, L.; Mocanu, S. The Influence of Cantilever Length and Implant Angulation in Completely Edentulous Patients Using the Finite Element Analysis and the All-on-Four/Fast & Fixed Treatment Concept—A Review of the Literature. Rom. J. Stomatol. 2020, 66, 162–166. [Google Scholar] [CrossRef]
- Ogawa, T.; Sato, Y.; Kitagawa, N.; Nakatsu, M. Relationship between Retention Forces and Stress at the Distal Border in Maxillary Complete Dentures: Measurement of Retention Forces and Finite-Element Analysis in Individual Participants. J. Prosthet. Dent. 2017, 117, 524–531. [Google Scholar] [CrossRef] [Green Version]
- Darbar, U.R.; Huggett, R.; Harrison, A. Stress Analysis Techniques in Complete Dentures. J. Dent. 1994, 22, 259–264. [Google Scholar] [CrossRef]
- Bonnet, A.S.; Postaire, M.; Lipinski, P. Biomechanical Study of Mandible Bone Supporting a Four-Implant Retained Bridge. Finite Element Analysis of the Influence of Bone Anisotropy and Foodstuff Position. Med. Eng. Phys. 2009, 31, 806–815. [Google Scholar] [CrossRef]
- Barão, V.A.R.; Delben, J.A.; Lima, J.; Cabral, T.; Assunção, W.G. Comparison of Different Designs of Implant-Retained Overdentures and Fixed Full-Arch Implant-Supported Prosthesis on Stress Distribution in Edentulous Mandible—A Computed Tomography-Based Three-Dimensional Finite Element Analysis. J. Biomech. 2013, 46, 1312–1320. [Google Scholar] [CrossRef] [Green Version]
- Pisani, M.X.; Presotto, A.G.C.; Mesquita, M.F.; Barão, V.A.R.; Kemmoku, D.T.; Del Bel Cury, A.A. Biomechanical Behavior of 2-Implant– and Single-Implant–Retained Mandibular Overdentures with Conventional or Mini Implants. J. Prosthet. Dent. 2018, 120, 421–430. [Google Scholar] [CrossRef]
- Andreiotelli, M.; Att, W.; Strub, J.-R. Prosthodontic Complications with Implant Overdentures: A Systematic Literature Review. Int. J. Prosthodont. 2010, 23, 195–203. [Google Scholar]
- Assaf, A.; Daas, M.; Boittin, A.; Eid, N.; Postaire, M. Prosthetic Maintenance of Different Mandibular Implant Overdentures: A Systematic Review. J. Prosthet. Dent. 2017, 118, 144–152.e5. [Google Scholar] [CrossRef]
- Preoteasa, E.; Oncescu Moraru, A.M.; Meghea, D.; Murariu Magureanu, C.; Preoteasa, C.T. Food Bolus Properties in Relation to Dentate and Prosthetic Status. Healthcare 2022, 10, 1596. [Google Scholar] [CrossRef]
- Topkaya, T.; Solmaz, M.Y. The Effect of Implant Number and Position on the Stress Behavior of Mandibular Implant Retained Overdentures: A Three-Dimensional Finite Element Analysis. J. Biomech. 2015, 48, 2102–2109. [Google Scholar] [CrossRef]
- Alshenaiber, R.; Barclay, C.; Silikas, N. The Effect of Number and Distribution of Mini Dental Implants on Overdenture Stability: An In Vitro Study. Materials 2022, 15, 2988. [Google Scholar] [CrossRef]
- Hong, H.R.; Pae, A.; Kim, Y.; Paek, J.; Kim, H.-S.; Kwon, K.-R. Effect of Implant Position, Angulation, and Attachment Height on Peri-Implant Bone Stress Associated with Mandibular Two-Implant Overdentures: A Finite Element Analysis. Int. J. Oral Maxillofac. Implant. 2020, 27, e69–e76. [Google Scholar]
- Preoteasa, C.T.; Nabil, S.A.; Popa, L.; Ghica, M.V.; Ionescu, E.; Ţâncu, A.M.C.; Preoteasa, E. Studies Regarding the Wettability of Acrylic and Silicone Dental Materials. Farmacia 2011, 59, 871–878. [Google Scholar]
- Teodorescu, C.; Preoteasa, E.; Preoteasa, C.T.; Murariu-Măgureanu, C.; Teodorescu, I.M. Perception and Attitudes of Dentists Regarding the Complications of Conventional Acrylic Dentures and Overdentures Supported by Teeth or Implants. J. Med. Life 2022, 15, 1031–1037. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Four MDIs | Three MDIs, after the Loss of a Distal Implant | |||
|---|---|---|---|---|
| Occlusal Loading | von Mises Stress (MPa) | Displacement (mm) | von Mises Stress (MPa) | Displacement (mm) |
| On the frontal teeth (using the frontal area in mastication) | 26.96 | 0.065 | 32.91 | 0.069 |
| On three lateral teeth on both sides (maximum intercuspation and bilateral mastication) | 70.41 | 0.15 | 103.56 | 0.48 |
| On three lateral teeth on one side (unilateral mastication) | 91.5 | 0.27 | 155.72 | 1.14 |
| Four MDIs | Three MDIs, after the Loss of an Implant in the Molar Area | Three MDIs, after the Loss of an Implant in the Canine Area | ||||
|---|---|---|---|---|---|---|
| Occlusal Loading | von Mises Stress (MPa) | Displacement (mm) | von Mises stress (MPa) | Displacement (mm) | von Mises Stress (MPa) | Displacement (mm) |
| On the frontal teeth (using the frontal area in mastication) | 35.8 | 0.061 | 91.67 | 0.088 | 166.1 | 0.11 |
| On three lateral teeth on both sides (maximum intercuspation and bilateral mastication) | 40.87 | 0.028 | 55.13 | 0.15 | 50.92 | 0.07 |
| On three lateral teeth on one side (unilateral mastication) | 82 | 0.057 | 110.66 | 0.28 | 113.08 | 0.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teodorescu, C.; Preoteasa, E.; Preoteasa, C.T.; Murariu-Măgureanu, C.; Teodorescu, I.M. The Biomechanical Impact of Loss of an Implant in the Treatment with Mandibular Overdentures on Four Nonsplinted Mini Dental Implants: A Finite Element Analysis. Materials 2022, 15, 8662. https://doi.org/10.3390/ma15238662
Teodorescu C, Preoteasa E, Preoteasa CT, Murariu-Măgureanu C, Teodorescu IM. The Biomechanical Impact of Loss of an Implant in the Treatment with Mandibular Overdentures on Four Nonsplinted Mini Dental Implants: A Finite Element Analysis. Materials. 2022; 15(23):8662. https://doi.org/10.3390/ma15238662
Chicago/Turabian StyleTeodorescu, Cristian, Elena Preoteasa, Cristina Teodora Preoteasa, Cătălina Murariu-Măgureanu, and Ioana Monica Teodorescu. 2022. "The Biomechanical Impact of Loss of an Implant in the Treatment with Mandibular Overdentures on Four Nonsplinted Mini Dental Implants: A Finite Element Analysis" Materials 15, no. 23: 8662. https://doi.org/10.3390/ma15238662