
In Vitro Study of Preload Loss in Different Implant Abutment Connection Designs


 , ,
, ,  , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. KL 0.7® Implant
2.2. SK2® Implant
2.3. Essential® Implant Cone 0.7 and 1.5
2.4. VEGA® Implant
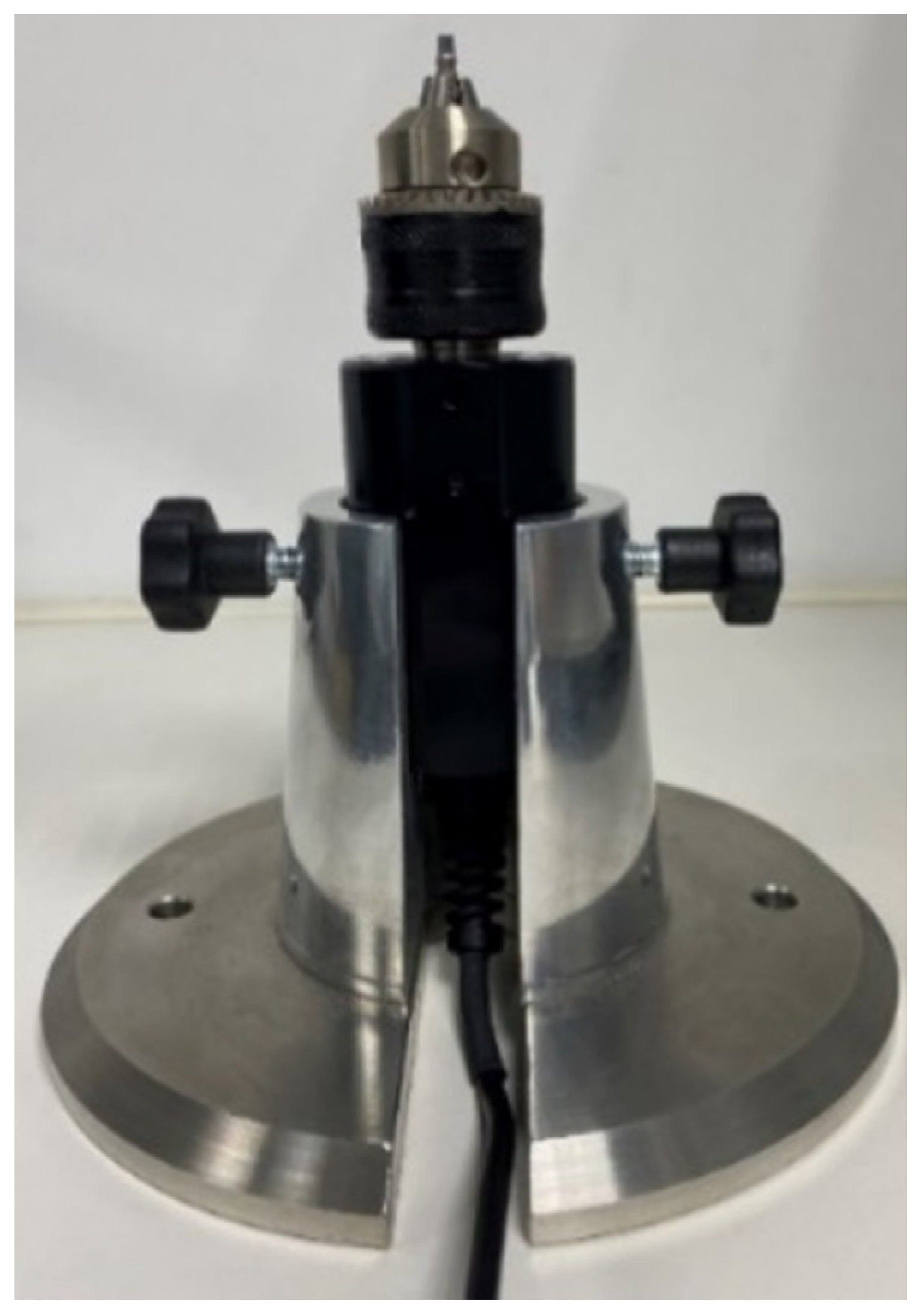
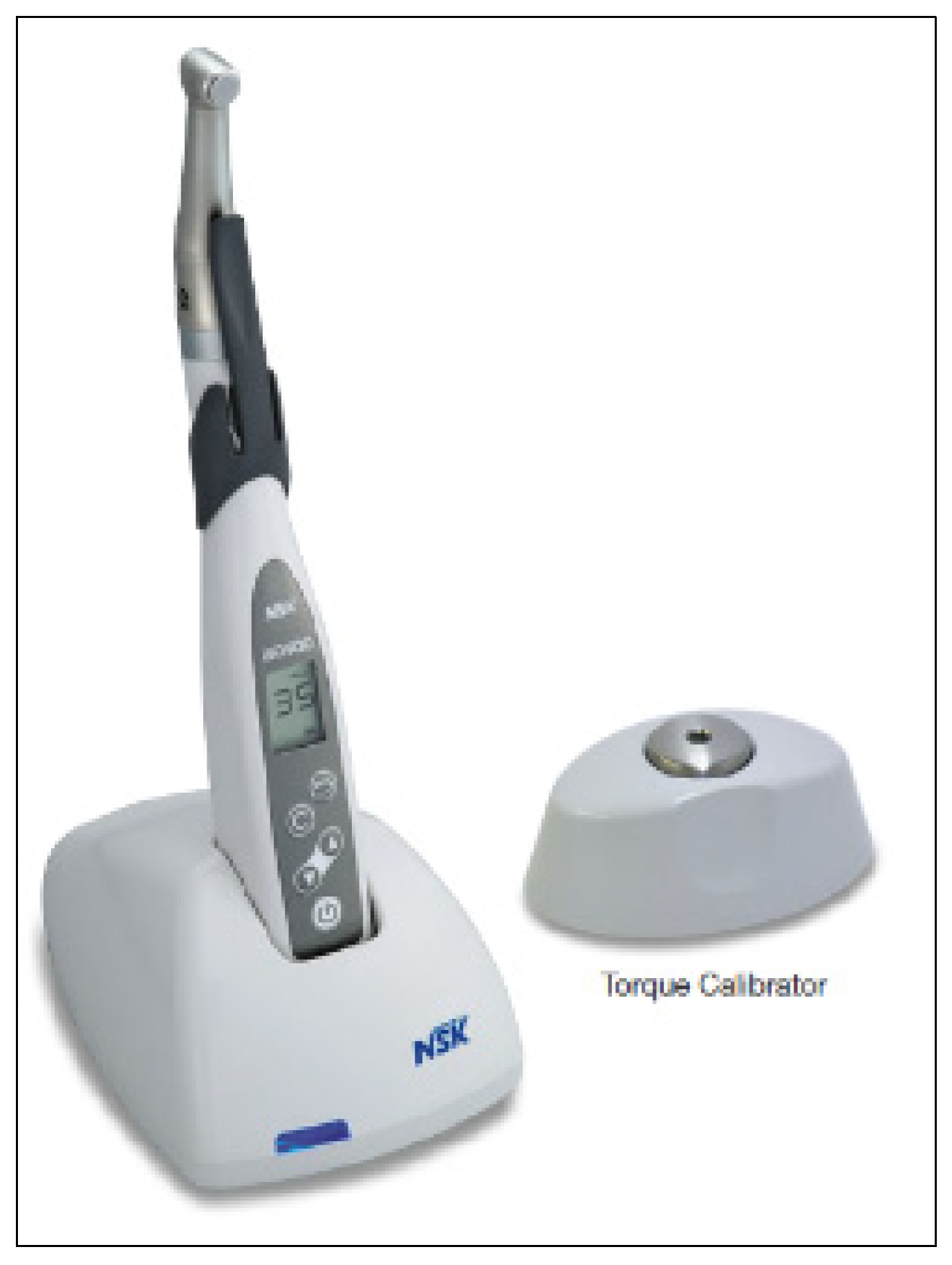
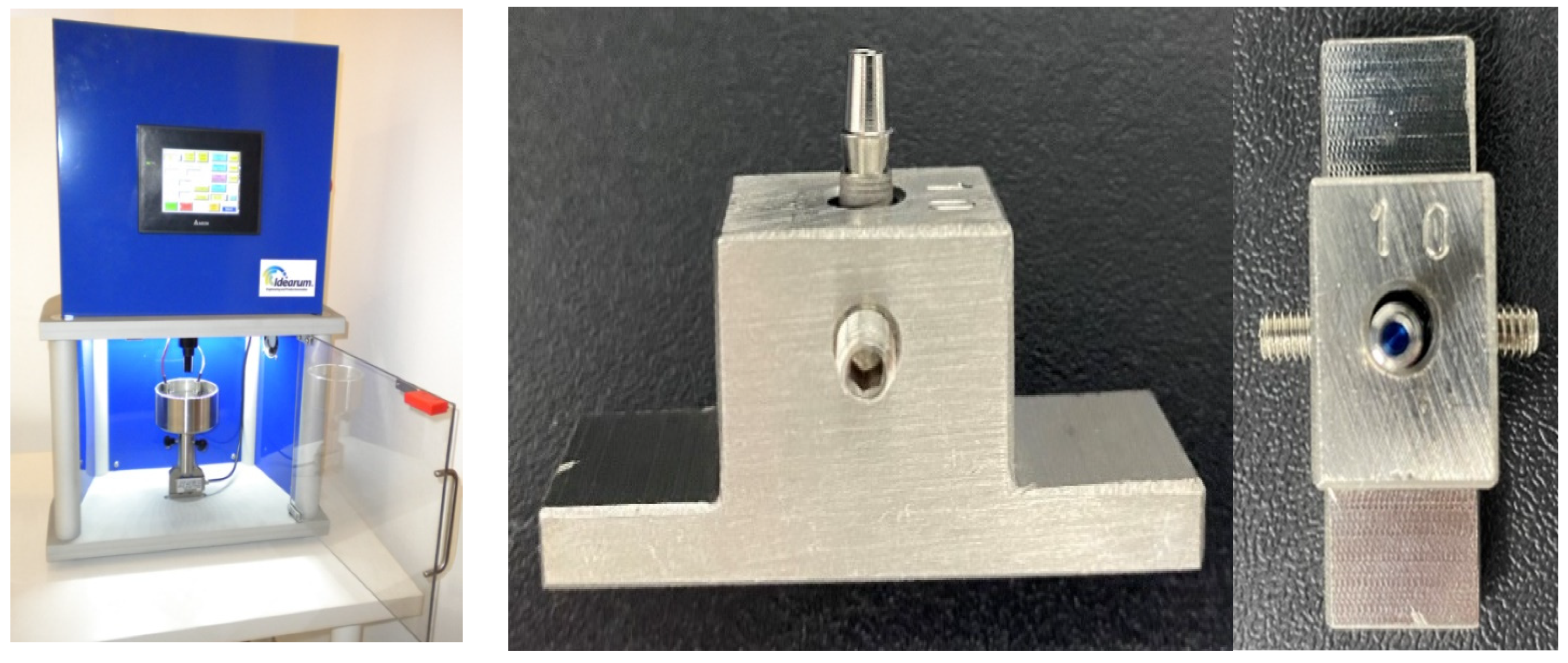
2.5. Equipment Used
2.6. Statistical Analysis
- in the descriptive study of the data—qualitative and quantitative variables (bar charts, circulars, frequency tables, wire box charts).
- evaluation of data distribution—Shapiro-Wilks’s test (SW) to test the normality adjustment of the data (for continuous variables) and/or graphical methods (P-P plot).
- in the comparative study—t-student comparison tests (for two independent samples) or if the normality assumption is not met by its non-parametric equivalent, if the conditions of the Central Limit Theorem (large samples) are not applicable. For more than two normal independent samples, the ANOVA methodology or its non-parametric equivalent, Kruskal-Walli’s test, was used.
- in the comparative study of pairs—t-student test for 2 paired samples (when comparing two torque measurements) for the pairs of measurements evaluated. When the normal conditions were not met, the Wilcoxon test (W) was used.
- in the comparative study over time—ANOVA tests with repeated measurements with k evaluation levels (k = 10 different times).
- In the comparative study of two factors (binding and phase)—ANOVA two way to evaluate the differences in tightening and untightening torque.
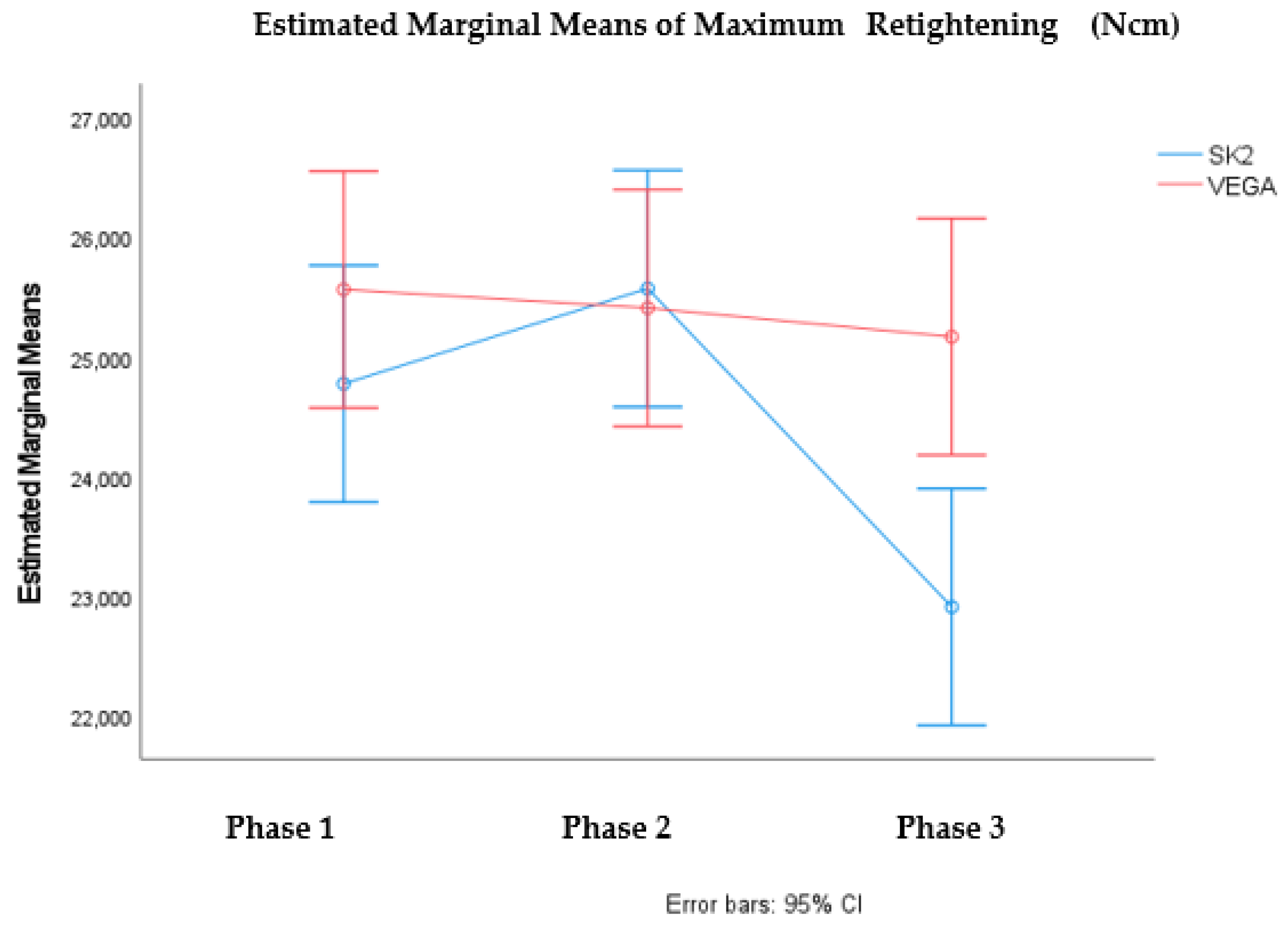
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mangano, C.; Mangano, F.; Piattelli, A.; Iezzi, G.; Mangano, A.; La Colla, L. Prospective clinical evaluation of 1920 Morse taper connection implants: Results after 4 years of functional loading. Clin. Oral Implant. Res. 2009, 20, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T. A multicenter report on osseointegrated oral implants. J. Prosthet. Dent. 1988, 60, 75–84. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, C.J.; Chuang, S.K.; Weber, H.P.; Gallucci, G.O. A systematic review of biologic and technical complications with fixed implant rehabilitations for edentulous patients. Int. J. Oral Maxillofac. Implant. 2012, 27, 102–110. [Google Scholar]
- Kazemi, M.; Rohanian, A.; Monzavi, A.; Nazari, M.S. Evaluation of the Accuracy and Related Factors of the Mechanical Torque-Limiting Device for Dental Implants. J. Dent. Tehran Univ. Med. Sci. 2013, 10, 112–118. [Google Scholar]
- Siamos, G.; Winkler, S.; Boberick, K.G. The Relationship Between Implant Preload and Screw Loosening on Implant-supported Prostheses. J. Oral Implant. 2002, 28, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Winkler, S.; Ring, K.; Ring, J.D.; Boberick, K.G. Implant Screw Mechanics and the Settling Effect: An Overview. J. Oral Implant. 2003, 29, 242–245. [Google Scholar] [CrossRef]
- Piermatti, J.; Yousef, H.; Luke, A.; Mahevich, R.; Weiner, S. An In Vitro Analysis of Implant Screw Torque Loss With External Hex and Internal Connection Implant Systems. Implant Dent. 2006, 15, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Jaarda, M.J.; Razzoog, M.E.; Gratton, D.G. Geometric comparison of five interchangeable implant prosthetic retaining screws. J. Prosthet. Dent. 1995, 74, 373–379. [Google Scholar] [CrossRef]
- Bulaqi, H.A.; Mousavi Mashhadi, M.; Safari, H.; Samandari, M.M.; Geramipanah, F. Dynamic nature of abutment screw retightening: Finite element study of the effect of retightening on the settling effect. J. Prosthet. Dent. 2015, 113, 412–419. [Google Scholar] [CrossRef]
- McGlumphy, E.A.; Mendel, D.A.; Holloway, J.A. Implant screw mechanics. Dent. Clin. N. Am. 1998, 42, 71–89. [Google Scholar]
- Freitas, A.C., Jr.; Bonfante, E.A.; Martins, L.M.; Silva, N.R.; Marotta, L.; Coelho, P.G. Reliability and failure modes of anterior single-unit implant-supported restorations. Clin. Oral Implant. Res. 2012, 23, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.M.; Nogueira-Filho, G.; Tenenbaum, H.C.; Lai, J.Y.; Brito, C.; Doering, H.; Nonhoff, J. Performance of conical abutment (Morse Taper) connection implants: A systematic review. J. Biomed. Mater. Res. A 2014, 102, 552–574. [Google Scholar] [CrossRef] [PubMed]
- Sinjari, B.; D’Addazio, G.; De Tullio, I.; Traini, T.; Caputi, S. Peri-Implant Bone Resorption during Healing Abutment Placement: The Effect of a 0.20% Chlorhexidine Gel vs. Placebo—A Randomized Double Blind Controlled Human Study. BioMed Res. Int. 2018, 2018, 5326340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callan, D.P.; O’Mahony, A.; Cobb, C.M. Loss of crestal bone around dental implants: A retrospective study. Implant Dent. 1998, 7, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Dellow, A.G.; Driessen, C.H.; Nel, H.J.C. Scanning electron microscopy evaluation of the interfacial fit of interchanged components of four dental implant systems. Int. J. Prosthodont. 1997, 10, 216–221. [Google Scholar]
- Ricomini Filho, A.P.; Fernandes, F.S.; Straioto, F.G.; da Silva, W.J.; Del Bel Cury, A.A. Preload loss and bacterial penetration on different implant-abutment connection systems. Braz. Dent. J. 2010, 21, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Goiato, M.C.; Pellizzer, E.P.; Silva, E.; Bonatto, L.D.R.; Dos Santos, D.M. Is the internal connection more efficient than external connection in mechanical, biological, and esthetical point of views? A systematic review. Oral Maxillofac. Surg. 2015, 19, 229–242. [Google Scholar] [CrossRef]
- Aroso, C.; Silva, A.S.; Mendes, J.M.; Ustrell, R.; Manzanares, M.C.; Escuin, T. Projection and construction of universal testing machine to simulate fatigue cycles during the insertion/detachment of implant attachments. In Biodental Engineering II, Proceedings of the 2nd International Conference on Biodental Engineering, Porto, Portugal, 7–8 December 2012; CRC Press: Boca Raton, FL, USA; pp. 101–106.
- Aroso, C.; Silva, A.S.; Ustrell, R.; Mendes, J.M.; Braga, A.C.; Berastegui, E.; Escuin, T. Effect of abutment angulation in the retention and durability of three overdenture attachment systems: An in vitro study. J. Adv. Prosthodont. 2016, 8, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Silva, A.S.; Aroso, C.; Ustrell, R.; Braga, A.C.; Mendes, J.M.; Escuin, T. The influence of saliva pH value on the retention and durability of bar-clip attachments. J. Adv. Prosthodont. 2015, 7, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Al-Otaibi, H.N.; Al-Fouzan, A.F.; Al-Mufleh, T.S.; Labban, N. Effect of different maintenance time of torque application on detorque values of abutment screws in full-arch implant-supported fixed prostheses. Clin. Implant Dent. Relat. Res. 2018, 20, 848–851. [Google Scholar] [CrossRef]
- Jorge, J.R.P.; Barao, V.A.R.; Delben, J.A.; Assuncao, W.G. The role of implant/abutment system on torque maintenance of retention screws and vertical misfit of implant-supported crowns before and after mechanical cycling. Int. J. Oral Maxillofac. Implant. 2013, 28, 415–422. [Google Scholar] [CrossRef] [Green Version]
- Mishra, S.K.; Chowdhary, R.; Kumari, S. Microleakage at the Different Implant Abutment Interface: A Systematic Review. J. Clin. Diagn. Res. 2017, 11, ZE10–ZE15. [Google Scholar] [CrossRef]
- Breeding, L.C.; Dixon, D.L.; Nelson, E.W.; Tietge, J.D. Torque required to loosen single-tooth implant abutment screws before and after simulated function. Int. J. Prosthodont. 1993, 6, 435–439. [Google Scholar] [PubMed]
- Byrne, D.; Jacobs, S.; O’Connell, B.; Houston, F.; Claffey, N. Preloads Generated with Repeated Tightening in Three Types of Screws Used in Dental Implant Assemblies. J. Prosthodont. 2006, 15, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Saboury, A.; Asli, H.N.; Vaziri, S. The Effect of Repeated Torque in Small Diameter Implants with Machined and Premachined Abutments. Clin. Implant Dent. Relat. Res. 2012, 14, e224–e230. [Google Scholar] [CrossRef] [PubMed]
- Al-Otaibi, H.N.; Almutairi, A.; Alfarraj, J.; Algesadi, W. The Effect of Torque Application Technique on Screw Preload of Implant-Supported Prostheses. Int. J. Oral Maxillofac. Implant. 2017, 32, 259–263. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.S.; Lim, Y.J. Axial Displacements and Removal Torque Changes of Five Different Implant-Abutment Connections under Static Vertical Loading. Materials 2020, 13, 699. [Google Scholar] [CrossRef] [Green Version]
- Burguete, R.L.; Johns, R.B.; King, T.; Patterson, E.A. Tightening characteristics for screwed joints in osseointegrated dental implants. J. Prosthet. Dent. 1994, 71, 592–599. [Google Scholar] [CrossRef]
- Jeong, C.-G.; Kim, S.-K.; Lee, J.-H.; Kim, J.-W.; Yeo, I.-S.L. Clinically available preload prediction based on a mechanical analysis. Arch. Appl. Mech. 2017, 87, 2003–2009. [Google Scholar] [CrossRef]
- Haack, J.E.; Sakaguchi, R.L.; Sun, T.; Coffey, J.P. Elongation and preload stress in dental implant abutment screws. Int. J. Oral Maxillofac. Implant. 1995, 10, 529–536. [Google Scholar]
- Farina, A.P.; Spazzin, A.O.; Consani, R.L.; Mesquita, M.F. Screw joint stability after the application of retorque in implant-supported dentures under simulated masticatory conditions. J. Prosthet. Dent. 2014, 111, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Spazzin, A.O.; Henrique, G.E.P.; Nóbilo, M.A.D.A.; Consani, R.L.X.; Correr-Sobrinho, L.; Mesquita, M.F. Effect of retorque on loosening torque of prosthetic screws under two levels of fit of implant-supported dentures. Braz. Dent. J. 2010, 21, 12–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuruta, K.; Ayukawa, Y.; Matsuzaki, T.; Kihara, M.; Koyano, K. The influence of implant–abutment connection on the screw loosening and microleakage. Int. J. Implant Dent. 2018, 4, 11. [Google Scholar] [CrossRef] [PubMed]
- Stüker, R.A.; Teixeira, E.R.; Beck, J.C.P.; da Costa, N.P. Preload and torque removal evaluation of three different abutment screws for single standing implant restorations. J. Appl. Oral Sci. 2008, 16, 55–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, E.I.; Kozak, D.; Gross, M.D. Effect of repeated closures on opening torque values in seven abutment-implant systems. J. Prosthet. Dent. 2000, 84, 194–199. [Google Scholar] [CrossRef]
- Cashman, P.M.; Schneider, R.L.; Schneider, G.B.; Stanford, C.M.; Clancy, J.M.; Qian, F. In Vitro Analysis of Post-fatigue Reverse-Torque Values at the Dental Abutment/Implant Interface for a Unitarian Abutment Design. J. Prosthodont. 2011, 20, 503–509. [Google Scholar] [CrossRef]
- Bernardes, S.R.; da Gloria Chiarello de Mattos, M.; Hobkirk, J.; Ribeiro, R.F. Loss of preload in screwed implant joints as a function of time and tightening/untightening sequences. Int. J. Oral Maxillofac. Implant. 2014, 29, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Sutter, F.; Weber, F.; Sorensen, F.; Belser, U. The new restorative concept of the ITI dental implant system: Design and engineering FAU—Sutter. Int. J. Periodontics Restor. Dent. 1993, 5, 409–431. [Google Scholar]
- Arshad, M.; Mahgoli, H.; Payaminia, L. Effect of repeated screw joint closing and opening cycles and cyclic loading on abutment screw removal Torque and screw thread morphology: Scanning electron microscopy evaluation. Int. J. Oral Maxillofac. Implant. 2018, 33, 31–40. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 22–38. [Google Scholar] [CrossRef] [PubMed]
- Steinebrunner, L.; Wolfart, S.; Ludwig, K.; Kern, M. Implant-abutment interface design affects fatigue and fracture strength of implants. Clin. Oral Implant. Res. 2008, 19, 1276–1284. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.M.; Huh, J.B.; Yun, M.J.; Jeon, Y.C.; Chang, B.M.; Jeong, C.M. Influence of the implant-abutment connection design and diameter on the screw joint stability. J. Adv. Prosthodont. 2014, 6, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil, F.J.; Herrero-Climent, M.; Lazaro, P.; Rios, J.V. Implant-abutment connections: Influence of the design on the microgap and their fatigue and fracture behavior of dental implants. J. Mater. Sci. Mater. Med. 2014, 25, 1825–1830. [Google Scholar] [CrossRef]
- Tsuge, T.; Hagiwara, Y. Influence of lateral-oblique cyclic loading on abutment screw loosening of internal and external hexagon implants. Dent. Mater. J. 2009, 28, 373–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Connection System | Single Tightening | Multiple Tightening | Cyclic Loading |
|---|---|---|---|
| Vega (45) | 15 | 15 | 15 |
| Essential (45) | 15 | 15 | 15 |
| SK2 (45) | 15 | 15 | 15 |
| KL (45) | 15 | 15 | 15 |
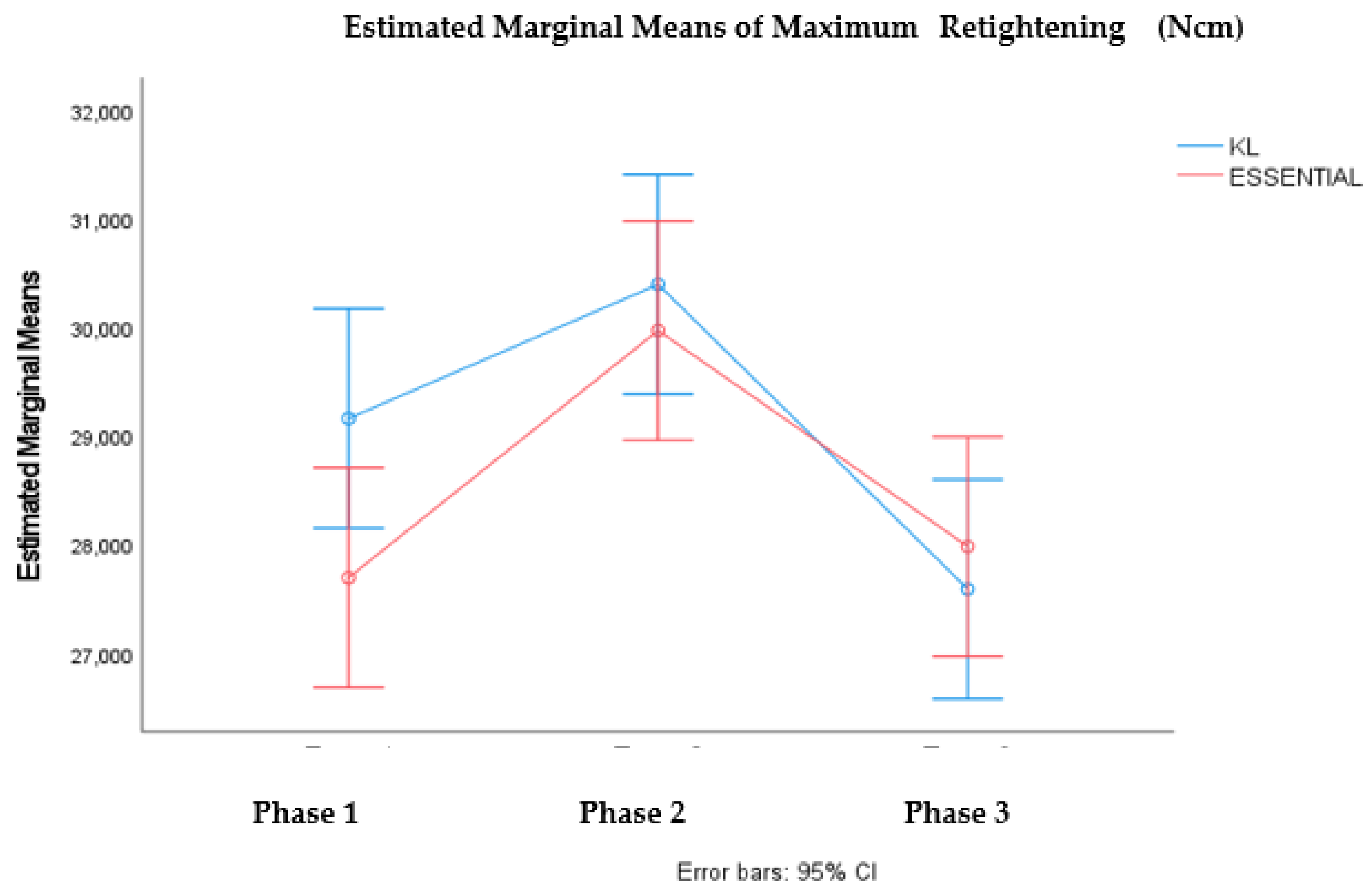
| PHASE | KL | SK2 | ESSENTIAL | VEGA | |
|---|---|---|---|---|---|
| 1. Single tightening | MT | 29.74 Ncm | 26.18 Ncm | 30.49 Ncm * | 26.49 Ncm * |
| MU | 29.16 Ncm | 24.77 Ncm | 27.69 Ncm * | 25.56 Ncm * | |
| 2. Multiple tightening | MT | 32.46 Ncm * | 27.68 Ncm * | 32.69 Ncm * | 27.68 Ncm * |
| MU | 30.39 Ncm * | 25.57 Ncm * | 29.97 Ncm * | 25.40 Ncm * | |
| 3. Multiple tightening + loading | MT | 32.45 Ncm * | 28.27 Ncm * | 32.24 Ncm * | 27.21 Ncm * |
| MU | 27.58 Ncm * | 22.90 Ncm * | 27.98 Ncm * | 25.16 Ncm * |
| PHASE | Group | W † | Df † | p† |
|---|---|---|---|---|
| Maximum tightening (Ncm) | KL | 0.922 | 15 | 0.408 |
| SK2 | 0.923 | 15 | 0.216 | |
| ESSENTIAL | 0.924 | 15 | 0.223 | |
| VEGA | 0.946 | 15 | 0.469 | |
| Untightening (Ncm) | KL | 0.987 | 15 | 0.997 |
| SK2 | 0.930 | 15 | 0.277 | |
| ESSENTIAL | 0.916 | 15 | 0.168 | |
| VEGA | 0.850 | 15 | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vinhas, A.S.; Aroso, C.; Salazar, F.; Relvas, M.; Braga, A.C.; Ríos-Carrasco, B.; Gil, J.; Rios-Santos, J.V.; Fernández-Palacín, A.; Herrero-Climent, M. In Vitro Study of Preload Loss in Different Implant Abutment Connection Designs. Materials 2022, 15, 1392. https://doi.org/10.3390/ma15041392
Vinhas AS, Aroso C, Salazar F, Relvas M, Braga AC, Ríos-Carrasco B, Gil J, Rios-Santos JV, Fernández-Palacín A, Herrero-Climent M. In Vitro Study of Preload Loss in Different Implant Abutment Connection Designs. Materials. 2022; 15(4):1392. https://doi.org/10.3390/ma15041392
Chicago/Turabian StyleVinhas, Ana Sofia, Carlos Aroso, Filomena Salazar, Marta Relvas, Ana Cristina Braga, Blanca Ríos-Carrasco, Javier Gil, José Vicente Rios-Santos, Ana Fernández-Palacín, and Mariano Herrero-Climent. 2022. "In Vitro Study of Preload Loss in Different Implant Abutment Connection Designs" Materials 15, no. 4: 1392. https://doi.org/10.3390/ma15041392
APA StyleVinhas, A. S., Aroso, C., Salazar, F., Relvas, M., Braga, A. C., Ríos-Carrasco, B., Gil, J., Rios-Santos, J. V., Fernández-Palacín, A., & Herrero-Climent, M. (2022). In Vitro Study of Preload Loss in Different Implant Abutment Connection Designs. Materials, 15(4), 1392. https://doi.org/10.3390/ma15041392