


Perspectives on the Psychological and Physiological Effects of Forest Therapy: A Systematic Review with a Meta-Analysis and Meta-Regression

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Literature Searches
2.2. Eligibility Criteria for Study Selection
2.3. Data Extraction and Measurement Outcomes
2.4. Data Analysis and Statistical Analysis
3. Results
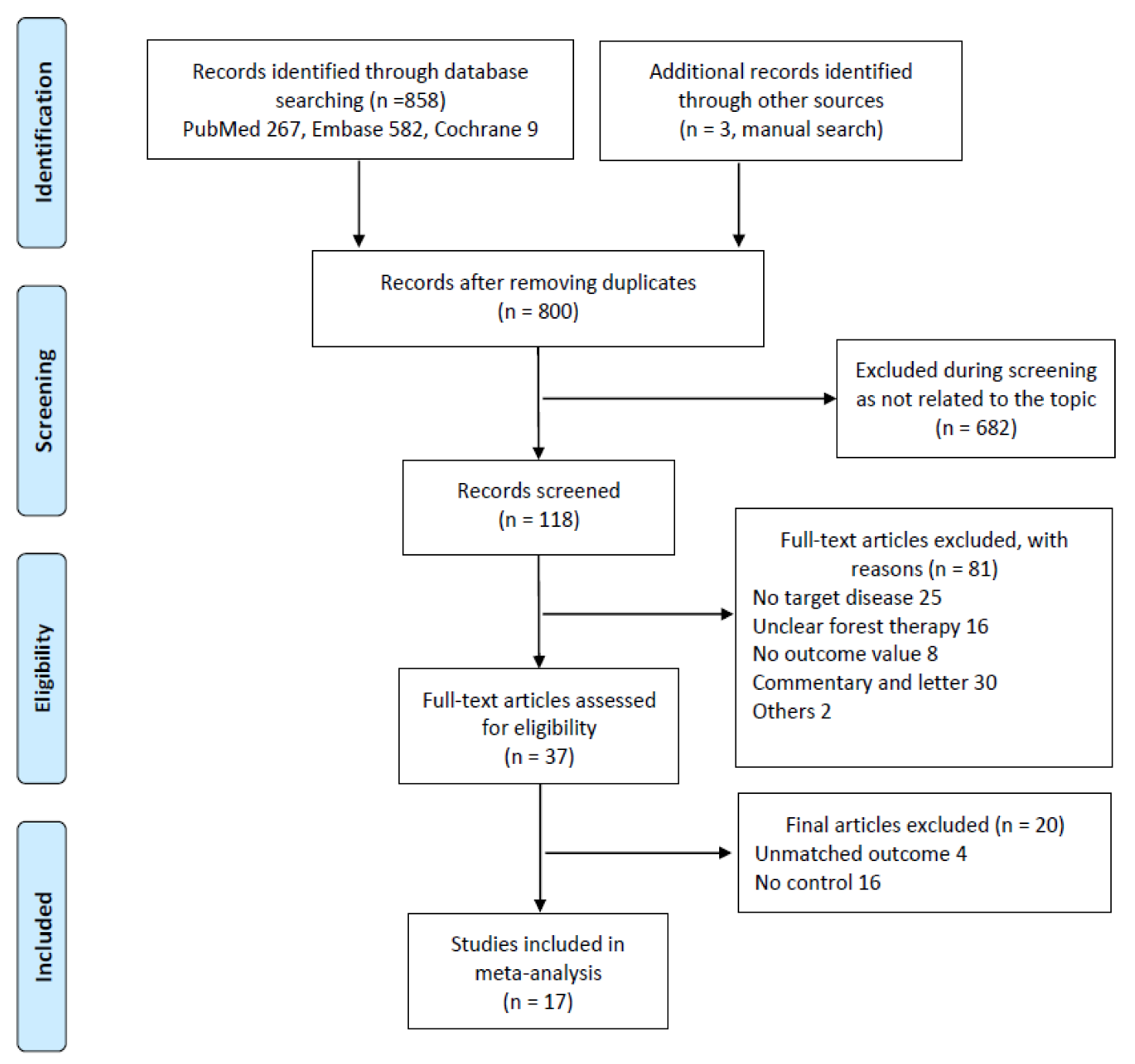
3.1. Study Selection
3.2. Quality Assessment
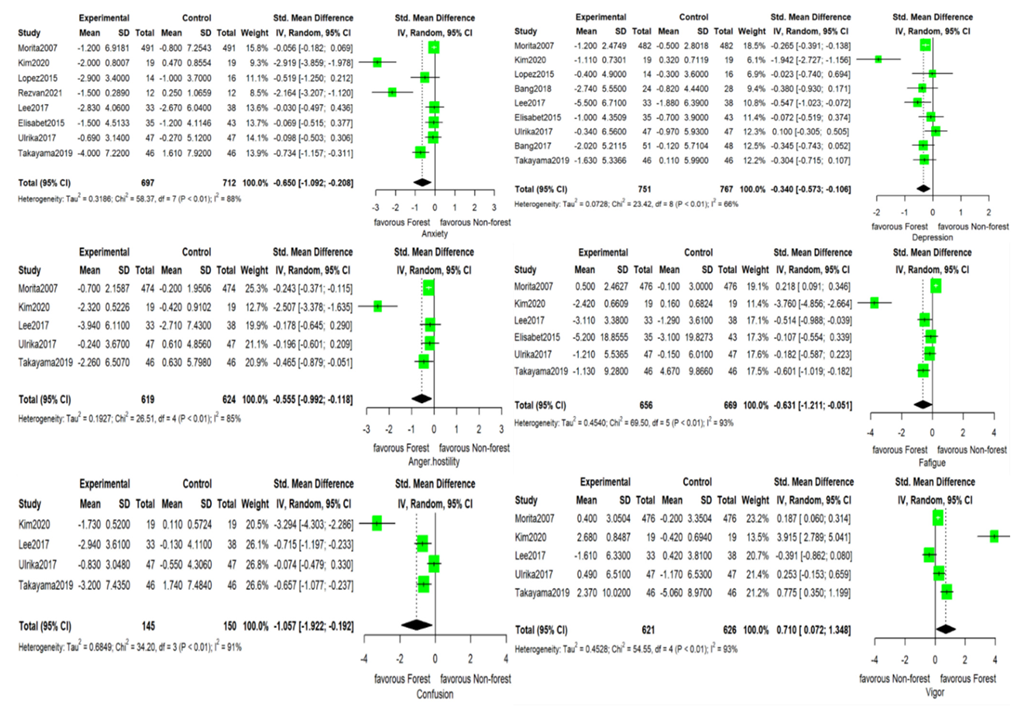
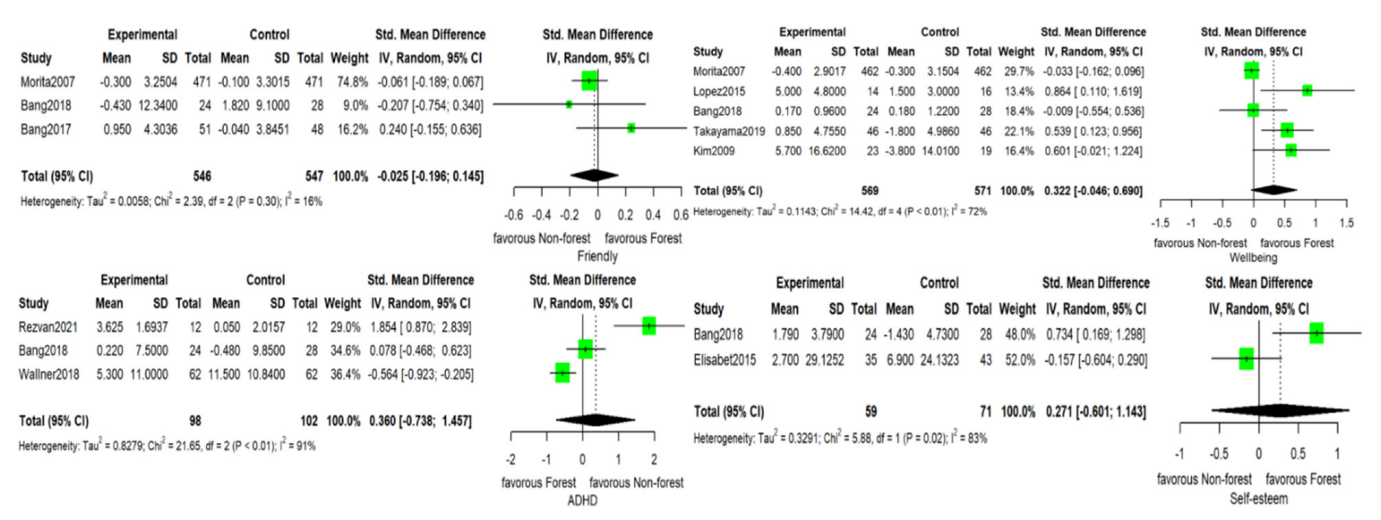
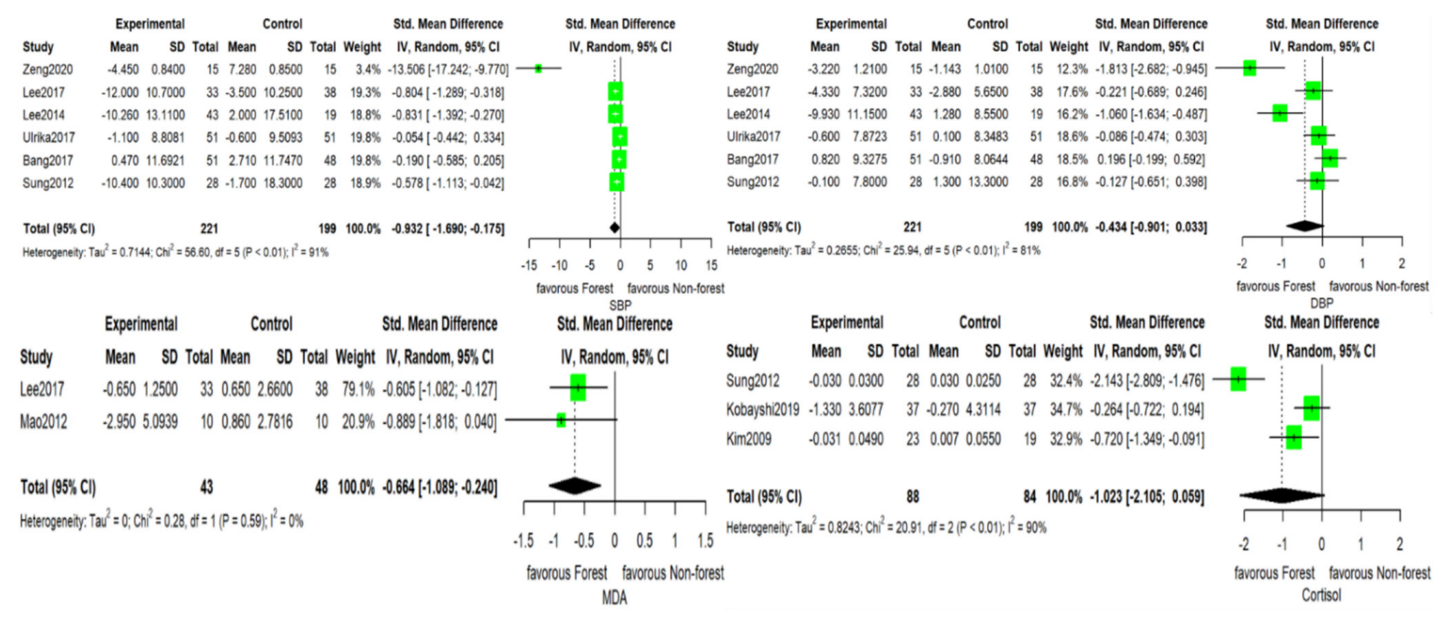
3.3. Outcomes
3.4. Effect Size Modifiers
3.5. Risk of Bias Assessment
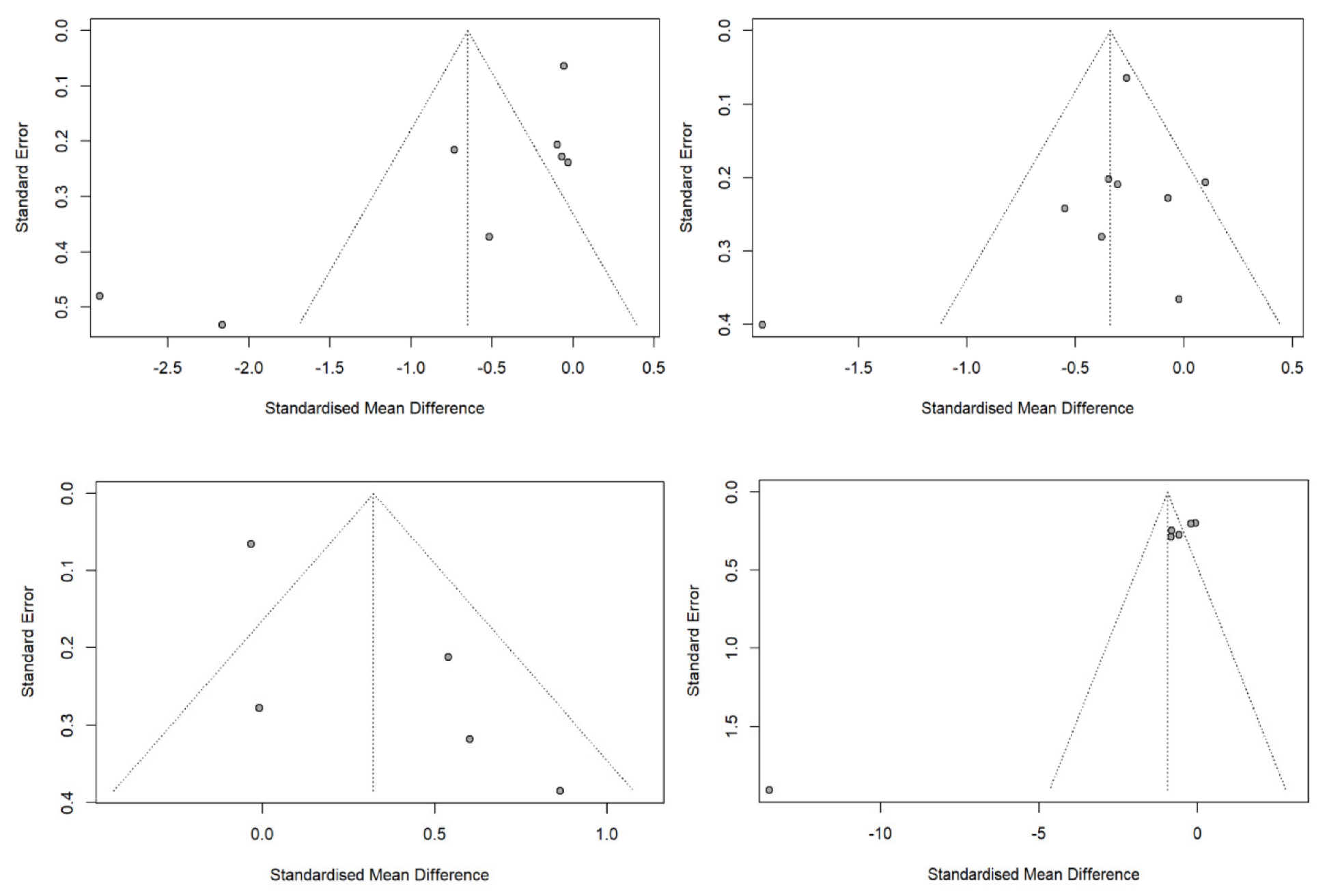
3.6. Publication Bias and Effect Size Modifiers
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Urban Green Spaces and Health: A Review of Evidence; World Health Organization: Copenhagen, Denmark, 2016. [Google Scholar]
- Reichert, M.; Braun, U.; Lautenbach, S.; Zipf, A.; Ebner-Priemer, U.; Tost, H.; Meyer-Lindenberg, A. Studying the impact of built environments on human mental health in everyday life: Methodological developments, state-of-the-art and technological frontiers. Curr. Opin. Psychol. 2020, 32, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.R.; Kim, S.J. Intervention meta-analysis: Application and practice using R software. Epidemiol. Health 2019, 41, e2019008. [Google Scholar] [CrossRef]
- Van den Berg, A.E.; Hartig, T.; Staats, H. Preference for nature in urbanized societies: Stress, restoration, and the pursuit of sustainability. J. Soc. Issues 2007, 63, 79–96. [Google Scholar] [CrossRef] [Green Version]
- Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrus, G.; Dadvand, P.; Sanesi, G. The role and value of urban forests and green infrastructure in promoting human health and wellbeing. In The Urban Forest; Springer: New York, NY, USA, 2017; pp. 217–230. [Google Scholar]
- Morita, E.; Fukuda, S.; Nagano, J.; Hamajima, N.; Yamamoto, H.; Iwai, Y.; Nakashima, T.; Ohira, H.; Shirakawa, T. Psychological effects of forest environments on healthy adults: Shinrin-yoku (forest-air bathing, walking) as a possible method of stress reduction. Public Health 2007, 121, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and well-being benefits of spending time in forests: Systematic review. Environ. Health Prev. Med. 2017, 22, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.G.; Khil, T.G.; Lim, Y.; Park, K.; Shin, M.; Shin, W.S. The psychological effects of a campus forest therapy program. Int. J. Environ. Res. Public Health 2020, 17, 3409. [Google Scholar] [CrossRef]
- Stigsdotter, U.K.; Corazon, S.S.; Sidenius, U.; Kristiansen, J.; Grahn, P. It is not all bad for the grey city—A crossover study on physiological and psychological restoration in a forest and an urban environment. Health Place 2017, 46, 145–154. [Google Scholar] [CrossRef]
- Bang, K.S.; Kim, S.; Song, M.K.; Kang, K.I.; Jeong, Y. The effects of a health promotion program using urban forests and nursing student mentors on the perceived and psychological health of elementary school children in vulnerable populations. Int. J. Environ. Res. Public Health 2018, 15, 1977. [Google Scholar] [CrossRef]
- Kim, W.; Lim, S.K.; Chung, E.J.; Woo, J.M. The effect of cognitive behavior therapy-based psychotherapy applied in a forest environment on physiological changes and remission of major depressive disorder. Psychiatry Investig. 2009, 6, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Sonntag-Öström, E.; Nordin, M.; Dolling, A.; Lundell, Y.; Nilsson, L.; Slunga Järvholm, L. Can rehabilitation in boreal forests help recovery from exhaustion disorder? The randomised clinical trial ForRest. Scand. J. For. Res. 2015, 30, 732–748. [Google Scholar] [CrossRef]
- Takayama, N.; Morikawa, T.; Bielinis, E. Relation between psychological restorativeness and lifestyle, quality of life, resilience, and stress-coping in forest settings. Int. J. Environ. Res. Public Health 2019, 16, 1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Pousa, S.; Bassets Pagès, G.; Monserrat-Vila, S.; de Gracia Blanco, M.; Hidalgo Colomé, J.; Garre-Olmo, J. Sense of well-being in patients with fibromyalgia: Aerobic exercise program in a mature forest—A pilot study. Evid. Based Complement. Alternat. Med. 2015, 2015, 614783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallner, P.; Kundi, M.; Arnberger, A.; Eder, R.; Allex, B.; Weitensfelder, L.; Hutter, H.P. Reloading pupils’ batteries: Impact of green spaces on cognition and wellbeing. Int. J. Environ. Res. Public Health 2018, 15, 1205. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, H.; Song, C.; Ikei, H.; Park, B.J.; Kagawa, T.; Miyazaki, Y. Combined effect of walking and forest environment on salivary cortisol concentration. Front. Public Health 2019, 7, 376. [Google Scholar] [CrossRef] [Green Version]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M. Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef] [Green Version]
- Sung, J.; Woo, J.M.; Kim, W.; Lim, S.K.; Chung, E.J. The effect of cognitive behavior therapy-based “forest therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [Google Scholar] [CrossRef]
- Lee, K.J.; Hur, J.; Yang, K.S.; Lee, M.K.; Lee, S.J. Acute biophysical responses and psychological effects of different types of forests in patients with metabolic syndrome. Environ. Behav. 2018, 50, 298–323. [Google Scholar] [CrossRef]
- Mao, G.X.; Lan, X.G.; Cao, Y.B.; Chen, Z.M.; He, Z.H.; Lv, Y.D.; Wang, Y.Z.; Hu, X.L.; Wang, G.F.; Jing, Y. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang Province, China. Biomed. Environ. Sci. 2012, 25, 317–324. [Google Scholar] [CrossRef]
- Antonelli, M.; Barbieri, G.; Donelli, D. Effects of forest bathing (shinrin-yoku) on levels of cortisol as a stress biomarker: A systematic review and meta-analysis. Int. J. Biometeorol. 2019, 63, 1117–1134. [Google Scholar] [CrossRef] [PubMed]
- Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.S.; Suzuki, S. Blood pressure-lowering effect of Shinrin-yoku (Forest bathing): A systematic review and meta-analysis. BMC Complement. Altern. Med. 2017, 17, 409. [Google Scholar] [CrossRef] [Green Version]
- Bang, K.S.; Lee, I.; Kim, S.; Lim, C.S.; Joh, H.K.; Park, B.J.; Song, M.K. The effects of a campus forest-walking program on undergraduate and graduate students’ physical and psychological health. Int. J. Environ. Res. Public Health 2017, 14, 728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-yoku (forest bathing) and nature therapy: A state-of-the-art review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef] [Green Version]
- Kamioka, H.; Tsutani, K.; Mutoh, Y.; Honda, T.; Shiozawa, N.; Okada, S.; Park, S.J.; Kitayuguchi, J.; Kamada, M.; Okuizumi, H. A systematic review of randomized controlled trials on curative and health enhancement effects of forest therapy. Psychol. Res. Behav. Manag. 2012, 5, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Ikei, H.; Miyazaki, Y. Physiological effects of nature therapy: A review of the research in Japan. Int. J. Environ. Res. Public Health 2016, 13, 781. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Lee, D.C. Cardiac and pulmonary benefits of forest walking versus city walking in elderly women: A randomised, controlled, open-label trial. Eur. J. Integr. Med. 2014, 6, 5–11. [Google Scholar] [CrossRef]
- Zeng, C.; Lyu, B.; Deng, S.; Yu, Y.; Li, N.; Lin, W.; Li, D.; Chen, Q. Benefits of a three-day bamboo forest therapy session on the physiological responses of university students. Int. J. Environ. Res. Public Health 2020, 17, 3238. [Google Scholar] [CrossRef]
- Ameli, R.; Skeath, P.; Abraham, P.A.; Panahi, S.; Kazman, J.B.; Foote, F.; Deuster, P.A.; Ahmad, N.; Berger, A. A nature-based health intervention at a military healthcare center: A randomized, controlled, cross-over study. PeerJ 2021, 9, e10519. [Google Scholar] [CrossRef]
- Dyakov, Y.; Dzhavakhiya, V.; Korpela, T. Comprehensive and Molecular Phytopathology; Elsevier: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Vieira, A.J.; Beserra, F.P.; Souza, M.; Totti, B.; Rozza, A. Limonene: Aroma of innovation in health and disease. Chem. Biol. Interact. 2018, 283, 97–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.; Song, B.; Cho, K.S.; Lee, I.S. Therapeutic potential of volatile terpenes and terpenoids from forests for inflammatory diseases. Int. J. Mol. Sci. 2020, 21, 2187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterfalvi, A.; Miko, E.; Nagy, T.; Reger, B.; Simon, D.; Miseta, A.; Czéh, B.; Szereday, L. Much more than a pleasant scent: A review on essential oils supporting the immune system. Molecules 2019, 24, 4530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mena-Martín, F.J.; Martín-Escudero, J.C.; Simal-Blanco, F.; Arzua-Mouronte, D.; Sanz, J.J.C.; Hortega Study Investigators. Influence of sympathetic activity on blood pressure and vascular damage evaluated by means of urinary albumin excretion. J. Clin. Hypertens. 2006, 8, 619–624. [Google Scholar] [CrossRef]
- Henry, J.P. Biological basis of the stress response. Integr. Physiol. Behav. Sci. 1992, 27, 66–83. [Google Scholar] [CrossRef]
- Taelman, J.; Vandeput, S.; Spaepen, A.; Huffel, S.V. Influence of mental stress on heart rate and heart rate variability. In Proceedings of the 4th European conference of the International Federation for Medical and Biological Engineering, Antwerp, Belgium, 2009; pp. 1366–1369. Available online: https://link.springer.com/book/10.1007/978-3-540-89208-3 (accessed on 1 May 2022).
- Ahrens, T.; Deuschle, M.; Krumm, B.; van der Pompe, G.; den Boer, J.A.; Lederbogen, F. Pituitary-adrenal and sympathetic nervous system responses to stress in women remitted from recurrent major depression. Psychosom. Med. 2008, 70, 461–467. [Google Scholar] [CrossRef]
- Kim, H.G.; Cheon, E.J.; Bai, D.S.; Lee, Y.H.; Koo, B.H. Stress and heart rate variability: A meta-analysis and review of the literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Diorio, D.; Viau, V.; Meaney, M.J. The role of the medial prefrontal cortex (cingulate gyrus) in the regulation of hypothalamic-pituitary-adrenal responses to stress. J. Neurosci. 1993, 13, 3839–3847. [Google Scholar] [CrossRef] [Green Version]
- Lapate, R.C.; Rokers, B.; Tromp, D.; Orfali, N.; Oler, J.; Doran, S.; Adluru, N.; Alexander, A.; Davidson, R. Awareness of emotional stimuli determines the behavioral consequences of amygdala activation and amygdala-prefrontal connectivity. Sci. Rep. 2016, 6, 25826. [Google Scholar] [CrossRef] [Green Version]
- McClelland, D.C.; Floor, E.; Davidson, R.J.; Saron, C. Stressed power motivation, sympathetic activation, immune function, and illness. J. Human Stress 1980, 6, 11–19. [Google Scholar] [CrossRef]
- Silva, J.A.C.E.; Steffen, R.E. Urban environment and psychiatric disorders: A review of the neuroscience and biology. Metabolism 2019, 100, 153940. [Google Scholar] [CrossRef]
- Lederbogen, F.; Kirsch, P.; Haddad, L.; Streit, F.; Tost, H.; Schuch, P.; Wüst, S.; Pruessner, J.C.; Rietschel, M.; Deuschle, M. City living and urban upbringing affect neural social stress processing in humans. Nature 2011, 474, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Farrow, M.R.; Washburn, K. A review of field experiments on the effect of forest bathing on anxiety and heart rate variability. Glob. Adv. Health Med. 2019, 8, 2164956119848654. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Ikei, H.; Kobayashi, M.; Miura, T.; Taue, M.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Effect of forest walking on autonomic nervous system activity in middle-aged hypertensive individuals: A pilot study. Int. J. Environ. Res. Public Health 2015, 12, 2687–2699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Kobayashi, M.; Inagaki, H.; Hirata, Y.; Li, Y.; Hirata, K.; Shimizu, T.; Suzuki, H.; Katsumata, M.; Wakayama, Y. A day trip to a forest park increases human natural killer activity and the expression of anti-cancer proteins in male subjects. J. Biol. Regul. Homeost. Agents 2010, 24, 157–165. [Google Scholar]
- Khiewkhern, S.; Promthet, S.; Sukprasert, A.; Eunhpinitpong, W.; Bradshaw, P. Effectiveness of aromatherapy with light thai massage for cellular immunity improvement in colorectal cancer patients receiving chemotherapy. Asian Pac. J. Cancer Prev. 2013, 14, 3903–3907. [Google Scholar] [CrossRef] [Green Version]
- Komori, T.; Fujiwara, R.; Tanida, M.; Nomura, J.; Yokoyama, M.M. Effects of citrus fragrance on immune function and depressive states. Neuroimmunomodulation 1995, 2, 174–180. [Google Scholar] [CrossRef]
- Muñoz, S. Children in the Outdoors. London: Sustainable Development Research Centre (2009). 2018. Available online: https://www.ltl.org.uk/wp-content/uploads/2019/02/children-in-the-outdoors.pdf (accessed on 1 May 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| References | Country | Study Design | Number of Participants (Mean Age) | Population (Number in Control Group, Number in Experimental Group) | Total Time of Intervention (min) | Intervention | Outcome Measurements | |
|---|---|---|---|---|---|---|---|---|
| Experimental Group | Control Group | |||||||
| Ameli et al., 2021 [18] | USA | Crossover | 12 (35) | Healthy male volunteers from a US military facility | 20 | Walking in a forested woodland | Walking around a university campus | Level of anxiety (DT), level of concentration (MAAS) |
| Zeng et al., 2020 [22] | China | RCT | 120 (21) | Healthy university students (30, 90) | 45 | Walking in bamboo forests in Sichuan Province | Walking in downtown Chengdu | Heart rate, DBP, SBP |
| Kim et al., 2020 [10] | Korea | RCT | 38 (22) | Healthy university students (19, 19) | 90 | Walking and stretching in forests | Daily routine activities | POMS * |
| Takayama et al., 2019 [15] | Japan | RCT | 46 (21) | Healthy male university students (23, 23) | 15 | Walking along forest roads | Walking around downtown major traffic routes or near the main train station | POMS, sense of wellbeing (SVS) |
| Kobayashi et al., 2019 [24] | Japan | Crossover | 74 (22.4) | Healthy male university students | 15 | Walking in one of the seven forests | Walking near city centers or railway stations | Salivary cortisol concentration |
| Wallner et al., 2018 [16] | Austria | Crossover | 60 (16.6) | Healthy adolescents from three different high schools in Vienna | 60 | Walking in forests | Walking in urban parks | Level of concentration (d2-R test) |
| Bang et al., 2018 [12] | Korea | RCT | 52 (11.78) | Healthy elementary school students (28, 24) | 600 | Walking and playing sports in forests | Studying at a community center | Sense of wellbeing, level of self-esteem (Rosenberg Self-Esteem Scale), depression (K-CDI), sociability, level of concentration (K-CWAS) |
| Lee et al., 2018 [27] | Korea | RCT | 71 (55.73) | Females volunteers diagnosed with or without metabolic syndrome (38, 33) | 120 | Walking, playing folk games, and meditating in a wild forest | Walking, playing folk games, and meditating in a tended park | POMS, SBP, DBP, MDA level |
| Stigsdotter et al., 2017 [11] | Denmark | Crossover | 51 (NA) | Healthy female university students in Copenhagen | 15 | Walking in the Danish Health Forest | Walking in downtown Copenhagen | POMS, SBP, DBP |
| Bang et al., 2017 [29] | Korea | RCT | 99 (24.31) | Graduate and undergraduate students in Seoul (48, 51) | 240 | Walking in forests | Daily routine activities | Depression (BDI), sociability (degree of social relation), SBP, DBP |
| Sonntag-Ostrom et al., 2015 [13] | Sweden | RCT | 86 (44.6) | Participants diagnosed with exhaustion disorder (46, 40) | 2640 | Relaxation exercises and meditation in forests | Daily routine activities | Level of fatigue (Checklist Individual Strength Questionnaire), Level of self-esteem (Self-concept Questionnaire), depression and level of anxiety (HADS) |
| Lopez-Pousa et al., 2015 [17] | Spain | RCT | 30 (62.3) | Participants diagnosed with fibromyalgia (16, 14) | 360 | Walking in a mature forest | Walking in a young forest | Depression (FIQR), level of anxiety (STAI), number of days with a sense of well-being |
| Lee et al., 2014 [21] | Korea | RCT | 62 (70.47) | Healthy female volunteers (19, 43) | 60 | Walking in a Pyunback tree forest in Mokpo city | Walking in the downtown area of Mokpo city | SBP, DBP |
| Sung et al., 2012 [23] | Korea | RCT | 56 (64.5) | Participants diagnosed with stage 1 hypertension (28, 28) | 1440 | Walking and meditating in two forests (Hoeungseong and Saneum) | Walking around nearby urban areas | SBP, DBP, salivary cortisol concentration |
| Mao et al., 2012 [28] | China | RCT | 20 (20.79) | Healthy male university students (10, 10) | 180 | Walking in the broad-evergreen Wuchao Mountain forest in Hangzhou | Walking in Hangzhou city areas | MDA level |
| Kim et al., 2009 [14] | Korea | RCT | 42 (43.78) | Participants diagnosed with MDD (19 hospitalized, 23 outpatients) | 720 | Mindfulness meditation at Hong-Reung arboretum | Mindfulness meditation in a room in Seoul Paik Hospital | Salivary cortisol concentration, sense of wellbeing (SFHSQ) |
| Morita et al., 2007 [8] | Japan | Crossover | 498 (56.2) | 244 healthy male and 254 healthy female volunteers | 150 | Walking and exercising in Tokyo University Forest | Walking and exercising at home | Level of hostility, depression, boredom, sociability, sense of wellbeing, and liveliness (MMF-SF), level of anxiety (STAI) |
| Anxiety | Depression | Well-Being | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | k | SMD | 95% CI | p | k | SMD | 95% CI | p | k | SMD | 95% CI | p | |||
| Total no. of patients | 8 | 0.002 a | −0.002 | 0.007 | 0.331 | 9 | 0.000 a | −0.002 | 0.003 | 0.740 | 5 | −0.001 a | −0.002 | 0.000 | 0.038 † |
| Age | 7 | 0.044 a | 0.001 | 0.087 | 0.043 † | 8 | 0.009 a | −0.009 | 0.027 | 0.312 | 5 | 0.003 a | −0.018 | 0.024 | 0.762 |
| Female participation rate | 7 | 1.629 a | −0.385 | 3.643 | 0.113 | 8 | 0.438 a | −0.541 | 1.417 | 0.381 | 4 | −0.191 a | −1.495 | 1.113 | 0.774 |
| BMI | - | - | - | - | 3 | 0.045 a | −0.080 | 0.170 | 0.479 | - | - | - | - | ||
| Country | 0.719 | 0.049 † | 0.220 | ||||||||||||
| Asia | 4 | −0.779 | −1.493 | −0.066 | 6 | −0.488 | −0.761 | −0.215 | 4 | 0.229 | −0.128 | 0.587 | |||
| Others | 4 | −0.590 | −1.331 | 0.152 | 3 | 0.008 | −0.404 | 0.421 | 1 | 0.865 | −0.085 | 1.814 | |||
| Study design | 0.163 | 0.532 | 0.060 | ||||||||||||
| Cross-sectional | 4 | −1.083 | −1.842 | −0.324 | 3 | −0.473 | −0.936 | −0.011 | 1 | −0.033 | −0.424 | 0.358 | |||
| RCT | 4 | −0.333 | −1.062 | 0.396 | 6 | −0.290 | −0.631 | 0.051 | 4 | 0.462 | 0.126 | 0.798 | |||
| Crossover study | 0.751 | 0.257 | 0.060 | ||||||||||||
| Yes | 3 | −0.578 | −1.388 | 0.232 | 2 | −0.109 | −0.605 | 0.387 | 1 | −0.033 | −0.424 | 0.358 | |||
| No | 5 | −0.745 | −1.379 | −0.110 | 7 | −0.449 | −0.764 | −0.135 | 4 | 0.462 | 0.126 | 0.798 | |||
| Underlying disease | 0.351 | 0.264 | 0.092 | ||||||||||||
| Yes (patients) | 2 | −0.274 | −1.244 | 0.696 | 2 | −0.053 | −0.616 | 0.509 | 2 | 0.716 | 0.133 | 1.298 | |||
| No (healthy) | 6 | −0.807 | −1.367 | 0.248 | 7 | −0.409 | −0.677 | 0.509 | 3 | 0.139 | −0.196 | 0.473 | |||
| Forest program education | 0.679 | 0.124 | 0.844 | ||||||||||||
| Yes | 3 | −0.816 | −1.630 | −0.001 | 5 | −0.535 | −0.881 | −0.189 | 2 | 0.282 | −0.414 | 0.978 | |||
| No | 5 | −0.599 | −1.221 | 0.023 | 4 | −0.148 | −0.500 | 0.204 | 3 | 0.370 | −0.155 | 0.895 | |||
| Forest therapist involvement | 0.801 | 0.240 | 0.558 | ||||||||||||
| Yes | 4 | −0.746 | −1.461 | −0.031 | 5 | −0.506 | −0.871 | −0.141 | 3 | 0.444 | −0.103 | 0.991 | |||
| No | 4 | −0.618 | −1.309 | 0.072 | 4 | −0.210 | −0.543 | 0.124 | 2 | 0.215 | −0.322 | 0.753 | |||
| Forest program time (min) b | 0.691 | 0.217 | 0.437 | ||||||||||||
| <100 | 3 | −0.880 | −1.819 | 0.060 | 3 | −0.183 | −0.663 | 0.297 | 1 | 0.539 | −0.222 | 1.301 | |||
| 100–300 | 3 | −0.830 | −1.753 | 0.094 | 3 | −0.720 | −1.218 | 0.223 | 1 | −0.033 | −0.683 | 0.617 | |||
| ≥300 | 2 | −0.279 | −1.417 | 0.858 | 3 | −0.163 | −0.695 | 0.368 | 3 | 0.440 | −0.079 | 0.959 | |||
| Systolic Blood Pressure | Diastolic Blood Pressure | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | k | SMD | 95% CI | p | k | SMD | 95% CI | p | ||
| Total no. of patients | 6 | −0.138 a | −0.257 | −0.019 | 0.023 † | 6 | −0.012 a | −0.036 | 0.012 | 0.319 |
| Age | 5 | 0.141 a | −0.079 | 0.361 | 0.208 | 5 | 0.004 a | −0.034 | 0.043 | 0.823 |
| Female participation rate | 6 | 14.172 a | 0.465 | 27.878 | 0.043 † | 6 | 1.659 a | −0.699 | 4.018 | 0.168 |
| BMI | 5 | 2.290 a | 0.298 | 4.282 | 0.024 † | 5 | 0.195 a | −0.233 | 0.624 | 0.372 |
| Country | 0.272 | 0.531 | ||||||||
| Asia | 5 | −1.284 | −2.253 | −0.314 | 5 | −0.534 | −1.130 | 0.063 | ||
| Others | 1 | −0.054 | −2.022 | 1.914 | 1 | −0.086 | −1.353 | 1.182 | ||
| Study design | 0.066 | 0.373 | ||||||||
| Cross-sectional | 2 | −2.256 | −4.391 | −0.735 | 2 | −0.810 | −1.762 | 0.143 | ||
| RCT | 4 | −0.598 | −1.623 | 0.428 | 4 | −0.287 | −0.930 | 0.355 | ||
| Crossover study | 0.272 | 0.531 | ||||||||
| Yes | 1 | −0.054 | −2.022 | 1.191 | 1 | −0.086 | −1.353 | 1.182 | ||
| No | 5 | −1.284 | −2.253 | −0.314 | 5 | −0.534 | −1.130 | 0.063 | ||
| Underlying disease | 0.622 | 0.584 | ||||||||
| Yes (patients) | 1 | −0.578 | −2.519 | 1.364 | 1 | −0.127 | −1.383 | 1.129 | ||
| No (healthy) | 5 | −1.120 | −2.057 | −0.183 | 5 | −0.512 | −1.077 | 0.054 | ||
| Forest program education | 0.278 | 0.792 | ||||||||
| Yes | 4 | −1.435 | −2.554 | −0.317 | 4 | −0.398 | −1.046 | 0.250 | ||
| No | 2 | −0.435 | −1.856 | 0.987 | 2 | −0.546 | −1.438 | 0.346 | ||
| Forest therapist involvement | 0.809 | 0.697 | ||||||||
| Yes | 1 | −0.804 | −2.732 | 1.125 | 1 | −0.221 | −1.487 | 1.044 | ||
| No | 5 | −1.068 | −2.007 | −0.130 | 5 | −0.498 | −1.080 | 0.084 | ||
| Forest program time (min) b | 0.766 | 0.793 | ||||||||
| <100 | 4 | −1.429 | −2.668 | −0.190 | 4 | −0.614 | −1.361 | 0.132 | ||
| 100–300 | 1 | −0.804 | −3.050 | 1.442 | 1 | −0.221 | −1.678 | 1.236 | ||
| ≥300 | 1 | −0.578 | −2.835 | 1.680 | 1 | −0.127 | −1.603 | 1.350 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shim, S.R.; Chang, J.; Lee, J.; Byeon, W.; Lee, J.; Lee, K.J. Perspectives on the Psychological and Physiological Effects of Forest Therapy: A Systematic Review with a Meta-Analysis and Meta-Regression. Forests 2022, 13, 2029. https://doi.org/10.3390/f13122029
Shim SR, Chang J, Lee J, Byeon W, Lee J, Lee KJ. Perspectives on the Psychological and Physiological Effects of Forest Therapy: A Systematic Review with a Meta-Analysis and Meta-Regression. Forests. 2022; 13(12):2029. https://doi.org/10.3390/f13122029
Chicago/Turabian StyleShim, Sung Ryul, JinKyung Chang, JooHee Lee, WooJin Byeon, Jeongwon Lee, and Kyung Ju Lee. 2022. "Perspectives on the Psychological and Physiological Effects of Forest Therapy: A Systematic Review with a Meta-Analysis and Meta-Regression" Forests 13, no. 12: 2029. https://doi.org/10.3390/f13122029
APA StyleShim, S. R., Chang, J., Lee, J., Byeon, W., Lee, J., & Lee, K. J. (2022). Perspectives on the Psychological and Physiological Effects of Forest Therapy: A Systematic Review with a Meta-Analysis and Meta-Regression. Forests, 13(12), 2029. https://doi.org/10.3390/f13122029