1. Introduction
Oropharyngeal squamous cell carcinoma (OPSCC) is a cancer of the throat. The oropharynx is the part of the throat, or pharynx, that opens onto the oral cavity. It includes the tonsils, the soft palate and base of the tongue, and the posterior wall of the pharynx. Over 18,000 new cases of OPSCC are diagnosed yearly in the US, mostly in men [
1]. Approximately 70% of these cases are associated with the human papillomavirus (HPV). These HPV-infected oropharyngeal cancers now outnumber cervical cancer cases in the US and constitute the largest category of HPV-associated cancers [
1].
Progress has been made in understanding the function of HPV in the development of OPSCC and other head and neck cancers, using transgenic mice carrying the E6 and E7 oncogenes driven by a Keratin-14 promoter [
2,
3]. These studies have revealed the importance of the Notch and FancD2 pathways and elucidated the roles of E6 and E7 [
3,
4]. However, no genetically tractable, infection-based, whole-virus model of oropharyngeal neoplasia has been available.
A papillomavirus capable of infecting laboratory mice, MmuPV1, was identified in immune-deficient mice in India in 2010 [
5]. This virus has been shown to infect both cutaneous and mucosal tissues [
5,
6,
7], where it can cause both skin and cervical cancer in immune-competent mice—particularly after immune-suppressive UVB irradiation [
7,
8,
9]. In the mouse, deliberate primary infection with MmuPV1 elsewhere has been shown to lead to secondary infection in the oropharynx, at the base of the tongue [
10]. The oropharynx in mice and humans share key anatomical features such as the soft palate, the pharynx, the base of the tongue, and stratified squamous cell epithelium. However, mice do not have tonsils. One-third of human HPV-infected oropharyngeal tumors are nontonsillar. Of these, 77% are in the base of the tongue [
11].
No model involving deliberate infection of the oropharynx has been described, perhaps due to the physical challenges involved in efficiently infecting the mouse pharynx. Anesthesia is the first hurdle. Infection of the oropharynx requires that a mouse be anesthetized. Anesthetics commonly used with mice include injectable agents such as ketamine and xylazine, generally provided intraperitoneally, and inhaled agents such as isoflurane, provided via a nose cone [
12]. The disadvantages of injectables include (1) the duration of anesthesia cannot be controlled easily; (2) doses that result in 100% of mice reaching a surgical plane can be fatal in a subset of animals; and (3) commonly used injectables including ketamine are controlled substances in the US and some European countries. By contrast, isoflurane “is the animal inhalation anesthetic agent of choice for both short and lengthy procedures due to its short induction and recovery time and the reliability of its effects” [
12], and it is not a controlled substance in the US or Europe. However, a major limitation to the use of isoflurane is that standard isoflurane anesthesia adapters cover the head and do not allow manipulation of the oral cavity and pharynx.
The second hurdle for oropharyngeal infection is delivering the virus to the basal cells of the pharynx, which is complicated by the pharynx’s location and structure. One common infection method involves extensive injury, using a needle or cytobrush to create wounds in the epithelium down to the basal layer of cells that the virus infects, followed by topical administration of the virus [
7,
8,
13]. Accurate manipulation of a needle or cytobrush in the confines of the mouse throat and topical administration of the virus on the sloped surfaces are a challenge, and injury to the epithelium may be painful. A second method used in the reproductive tract involves chemical injury hours before topical administration of the virus [
13]. This method is time consuming and is limited both by the throat’s topology and by the types of chemicals a mouse can safely consume or aspirate.
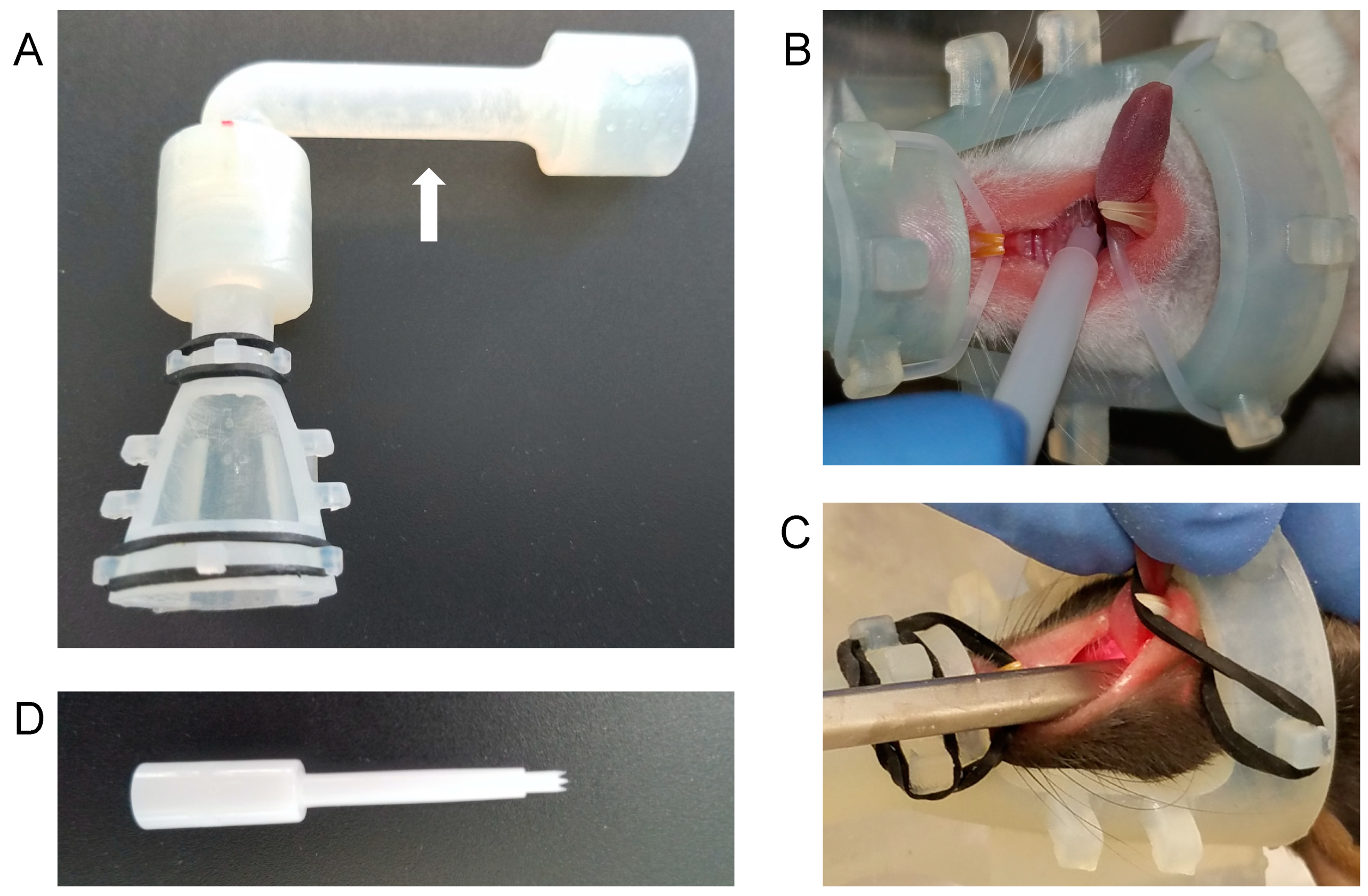
We have designed an anesthesia cone that braces the mouse’s head while stabilizing the upper body against any firm support. The device maintains isoflurane anesthesia while holding the mouse’s oral cavity open for manipulation. We have also repurposed an allergy testing device to infect with MmuPV1 efficiently and reproducibly, with minimal pain, in the oropharynx. These tools have allowed us to easily and reliably generate dysplastic oropharyngeal lesions, including tumors, in two immune-deficient strains of mice.
2. Materials and Methods
2.1. Animals
Animal experiments (Protocol M005871) were approved 17/7/2017 by the School of Medicine and Public Health Animal Care and Use Committee (IACUC) of the University of Wisconsin-Madison and conducted in accordance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals. Mice were fed an irradiated diet (Teklad 2918) or provided with an Uniprim diet (Envigo, TD06596) as needed to combat the C. bovis infection. Both infected mice and uninfected controls were given Uniprim if either group showed signs of bacterial infection. Nude mice (Fox1nu) were purchased from Envigo. NOD scid gamma (NSG) mice (Nod.Cg-Prkdc ScidII2rgtmWjl/SzJ; stock 005557) were purchased from the Jackson Laboratory and bred in the breeding core (BRMS, UW-Madison).
2.2. High-Titer Crude MmuPV1 Virus Preparation
Virus stocks were prepared from homogenized, papillomavirus-induced warts. Warts were soaked in PBS (250 mg warts/mL) overnight at 4 °C, then homogenized (PowerGen 125; Fisher Scientific, Pittsburgh, USA). After that, the homogenate was incubated with benzonase (1 µL/mL; Sigma-Aldrich; St. Louis, MO, USA) and Triton X-100 (10 µL/mL; Sigma-Aldrich). Collagenase (~5 mg/mL; type I; Worthington, Lakewood, NJ) was added to the mixture, which was then incubated for approximately 48 h at 4 °C, followed by centrifugation for 15 min at 4255× g. The supernatant was collected and treated with additional benzonase (1 µL/mL) and centrifuged for 10 min at 5000× g at 4 °C. The supernatant containing the virus was collected, and an aliquot was treated with a viral release buffer (0.1% Proteinase K, 0.5% SDS, 25 mM EDTA) and 1 ul of additional Proteinase K at 55 °C for 30 min. The released viral DNA was then analyzed by gel electrophoresis next to DNA standards for quantification, using 0.82 ng DNA = 108 viral genome equivalents.
2.3. Nose Cone Design and Fabrication
The “Mickey’s Space Helmet” nose cone design was encoded using an Autodesk Inventor 2019 (Autodesk, San Rafael, CA, USA), using dimensions taken from 6- to 10-week-old mice. The window for oral manipulation is 15.75 × 16 mm. The adapter is compatible with an anesthesia tube with an inside diameter of 2 cm. Silicone o-rings are used to keep the mouth open via the teeth, including a 1 mm cross-section, 2.5 cm diameter silicone o-ring (“135 Pcs 1 mm Wire Diameter Silicone Rubber O-ring Seals Rings VMQ Rubber Temperature Resistant Assortment Set,” zenlis4) for the mandibular incisors, and a 1 mm cross-section, 1.5 cm diameter silicone o-ring for the maxillary incisors. Mickey’s Space Helmet is available for purchase from Jeffery Consulting, LLC (
https://jefferyconsulting.com/).
2.4. Anesthesia and Infection
Mice were anesthetized using isoflurane provided via Mickey’s Space Helmet. A Greer Pick (Stallergenes-Greer, London, UK) was plunged into the virus stock (108 to 8 × 109 genome equivalents/µL) in a microfuge tube and used to mix the virus suspension. The Pick was removed by sliding along the side of the tube to remove excess virus stock. The Pick was then jabbed into a soft palate or the base of the tongue and rotated for approximately one quarter-turn.
2.5. Oropharyngeal Endoscopy
The endoscopy was performed using a 1.9 mm scope in an operating sheath (Karl Storz, El Segundo, USA) while mice were anesthetized in Mickey’s Space Helmet.
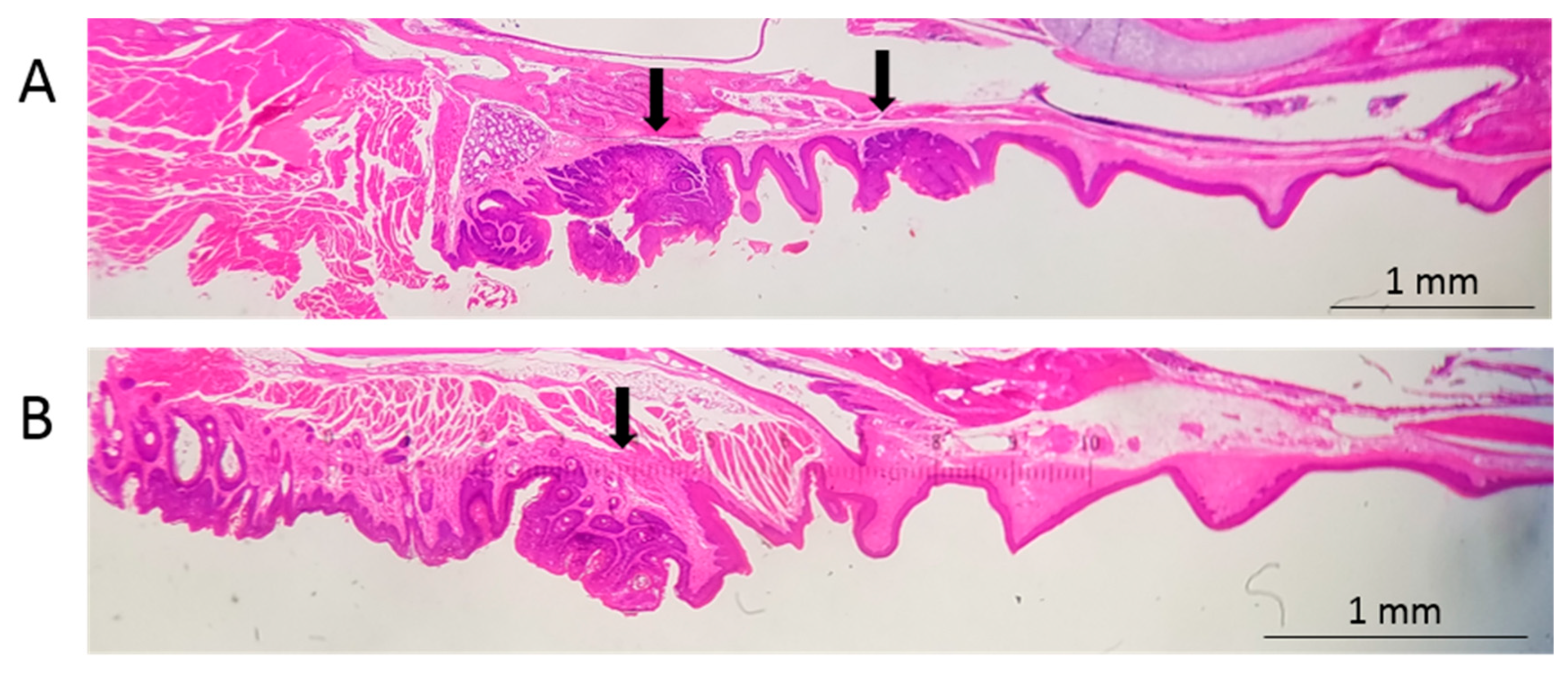
2.6. Tissue Analysis
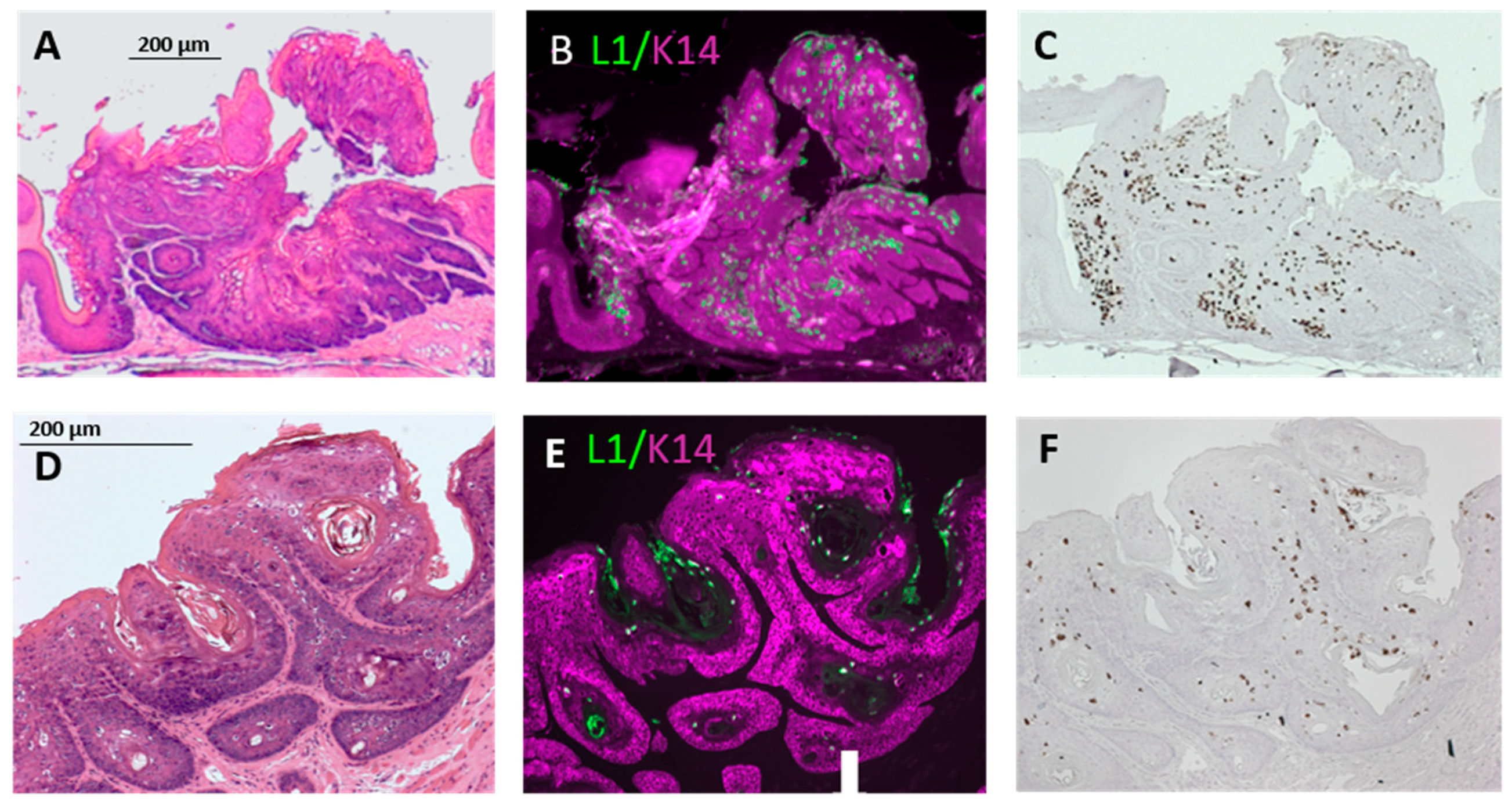
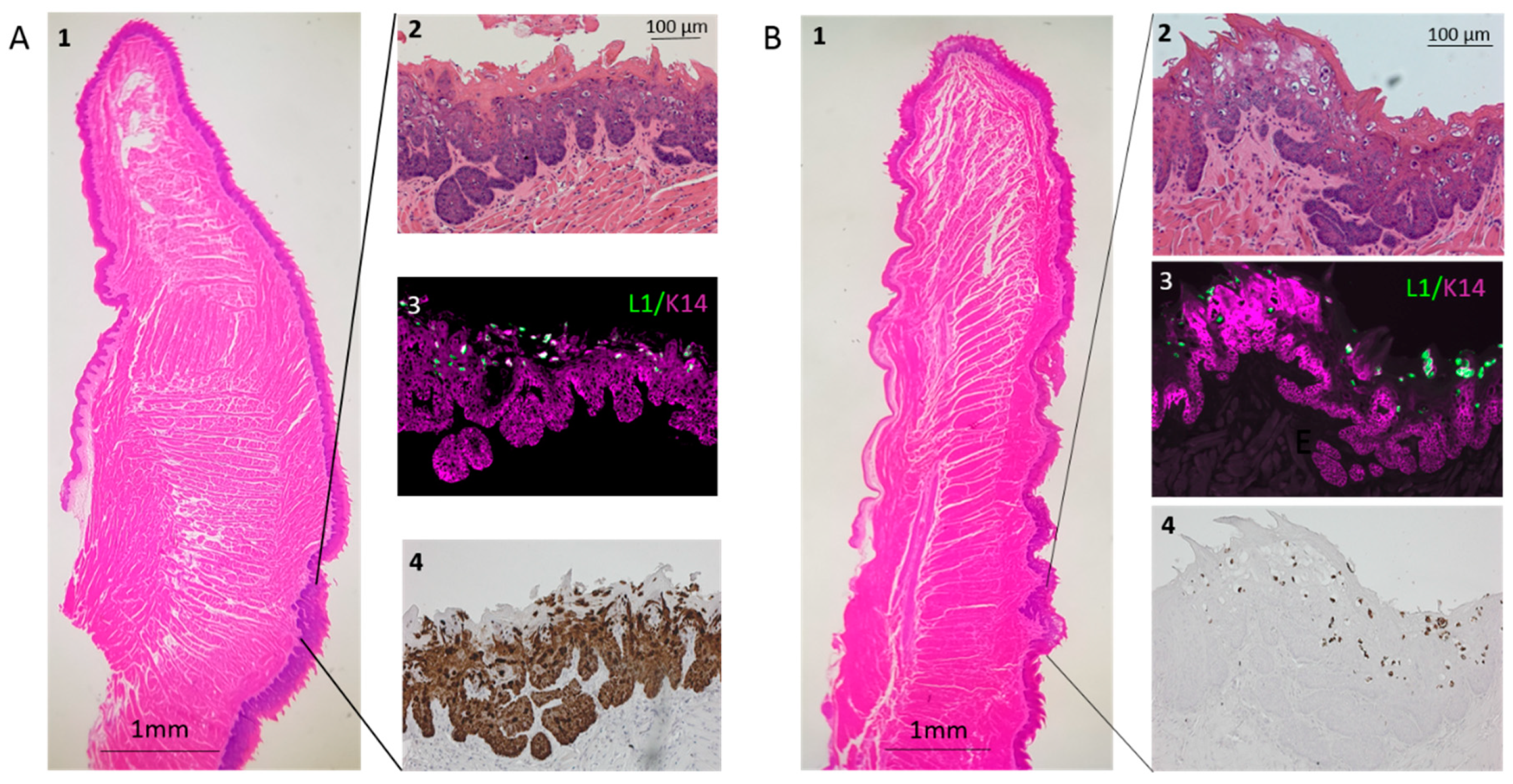
Tongues were fixed in 4% paraformaldehyde in PBS overnight at 4 °C. Maxillae were fixed in Surgipath Decalcifier I (Leica Biosystems, Buffalo Grove, USA) overnight at 4 °C twice (with fresh decalcifier for the second incubation). Tissues were then transferred to 70% ethanol and processed. Processed tissues were embedded in paraffin. Sections (5 µm) were stained with hematoxylin (Shandon Instant Hematoxylin; #6765015, Thermo Fisher Scientific, Kalamazoo, MI, USA) and eosin (Eosin Y, #17372-87-1, mixed 10:1 with Phloxine B, #18472-87-1, Sigma-Aldrich, St. Louis, MO, USA) or analyzed immunohistochemically for the MmuPV1 L1 capsid protein or Keratin-14 as previously described [
14]. Lesions arising in nude mice were evaluated by an experienced pathologist (D.B.). The significance of the differences among the degrees of dysplasia in nude and NSG mice was determined by the chi-squared statistical test, using Mstat software (Mstat version 6.5.1, McArdle Laboratory for Cancer Research;
https://mcardle.wisc.edu/mstat/).
2.7. RNA/DNA in Situ Hybridization
The MmuPV1 nucleic acid was detected using RNAscope [
15] 2.5 HD Assay-BROWN (Advanced Cell Diagnostics, Newark, CA, USA) according to the manufacturer’s instructions. Paraffin sections (5 µm) were hybridized with probes specific for MmuPV1 E6/E7. (MusPV-E6-E7; catalog no. 409771; Advanced Cell Diagnostics, Newark, CA, USA).
4. Discussion
We have developed a facile, robust, efficient protocol for generating and tracking papilloma-virus-infected oropharyngeal squamous cell tumors. Our protocol takes advantage of two innovations: A nose cone that maintains isoflurane anesthesia during oropharyngeal infection, and the Greer Pick skin allergy testing device that infects the oropharynx with MmuPV1 directly—without prior scarification. Using these tools, we consistently obtain dysplastic lesions in both the base of the tongue and in the soft palate, which often develops noninvasive, exophytic oropharyngeal squamous cell tumors.
Used clinically and sold in sterile packaging, the Pick is a convenient and versatile tool for infection. The nose cone we have designed, Mickey’s Space Helmet, provides oral access while supplying isoflurane, a fast-acting anesthetic. Devices that maintain nasal isoflurane anesthesia are available. However, these are intended for simple intubation of the lungs and do not stabilize the mouse or hold its mouth open; they are also bulky and therefore difficult to use for procedures requiring a biosafety cabinet; and they are relatively expensive (e.g., Mouse Endotracheal Intubation Kit, Kent Scientific, $675).
Mickey’s Space Helmet provides safe anesthesia during both infection and endoscopy. No other anesthesia device, to our knowledge, provides isoflurane while stabilizing the upper body and holding the mouth open for hands-free manipulation. This cone has been used successfully to maintain mice weighing 15 to 64 g under anesthesia, as long as desired. Mickey’s Space Helmet can be used in any procedure requiring access to the oral cavity or throat, and therefore should be useful in a variety of preclinical mouse trials—particularly those that require frequent anesthesia, such as longitudinal studies of treatment effects.
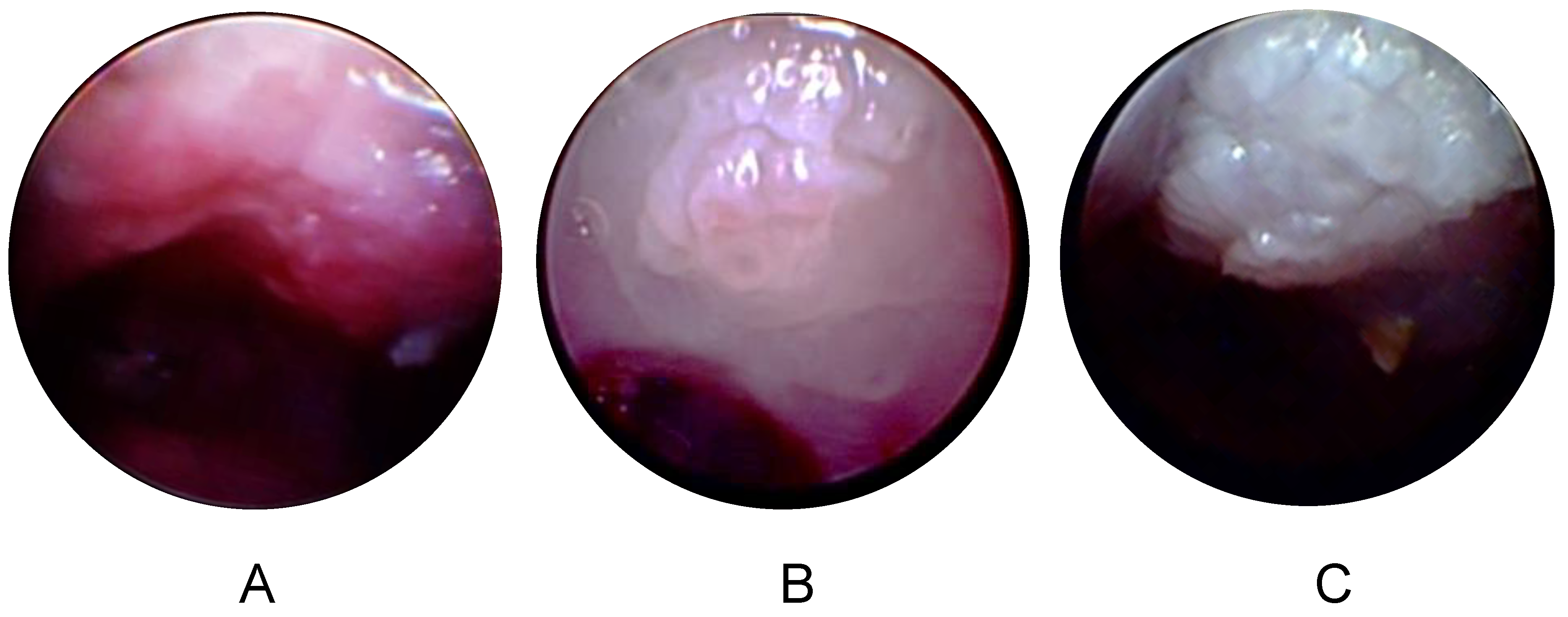
Longitudinal endoscopic imaging of oropharyngeal tumors is a significant advance in the MmuPV1 field. Lesion size, morphology, and other tissue characteristics can be assessed at multiple timepoints without sacrificing a large number of animals. We have demonstrated that Mickey’s Space Helmet facilitates visualization of tumor growth over time using white light endoscopy. In the future, our model could be extended to include narrow band imaging (NBI). NBI is a technology that filters all light wavelengths except for blue and green bands centered at 415 and 540 nm, respectively, to highlight blood vessels at various depths within the mucosa [
18]. This greatly improves diagnostic accuracy and edge detection of even small HPV-associated lesions in the head and neck due to characteristic vascular patterns of papillomas and HPV+ SCC [
19,
20]. Thus, NBI may improve assessment of the presence and extent of tumors in our model, especially at early stages of tumorigenesis.
Standard treatment for OPSCC includes radiation and chemotherapy, which are associated with dose-related morbidities. Patients with papillomavirus-associated oropharyngeal tumors have a better prognosis than those with HPV− OPSCC [
21]. HPV+ OPSCC is generally more sensitive to treatment and may respond to de-escalated treatments. However, treatment for HPV+ and HPV− OPSCC is almost identical [
21]. Treatments tailored to the unique etiology of HPV+ disease can be tested using our infection-based model of papillomavirus tumorigenesis. This model can also be used to assess the effect of potential environmental factors, such as tobacco-associated carcinogens.
While HPV+ OPSCC is generally more responsive to the treatment than HPV− OPSCC, recent meta-analysis suggests that HPV+ OPSCCs differ in responsiveness depending on the particular tissue within the oropharynx where they developed [
11]. The presence of HPV in some oropharyngeal lesions, including those of the soft palate, appears not to affect patient outcome. Our model of papillomavirus-induced soft palate tumorigenesis can be used to rigorously determine whether papillomavirus-specific treatments affect outcome in this part of the oropharynx.
One limitation to our model is that mice do not have tonsils, a lymphatic tissue. Lymphatic tissue may affect papillomavirus-induced oropharyngeal cancer development and patient outcome [
11]; therefore, insights from mouse oropharyngeal models may not extend directly to tonsillar cancers. As in humans, however, the base of the tongue in mice is particularly susceptible to papillomavirus-associated carcinogenesis. Cladel et al. showed that secondary infections of MmuPV1 preferentially target the base of the tongue [
10], and Mestre et al. recently found that greater than 90% of spontaneous SCCs in the oral and pharyngeal epithelia of HPV16-transgenic mice occur in the base of the tongue [
22]. The authors found squamous-columnar transformation zone markers (Keratin-7 and p63) in the von Ebner’s salivary glands near the circumvallate papilla in the base of the tongue. These markers were also identified in dysplastic lesions (diffuse p63, scattered Keratin-7), suggesting that the base of the tongue contains a transformation zone similar to those observed in the cervix and anus [
22,
23]. Thus, the susceptibility of the base of the mouse tongue to HPV-induced carcinogenesis might be associated with structures known to be associated with HPV carcinogenesis in other susceptible tissues in mice and humans [
23].
MmuPV1 was discovered as a cutaneous virus. It has since been shown to be capable of infecting a wide variety of tissues, including the cervix, the anus, and the oropharynx. Viral infection leads to carcinogenesis in the cervix, even in immune-competent animals such as mice of the FVB strain [
24]. While deliberately infecting the oropharynx, we saw carcinogenesis in the rostral tongue and the outer cheek. This broad tropism contrasts with the HPV strains associated with neoplasia, which generally target mucosal or cutaneous tissues and rarely cross-infect [
25]. Despite this difference in tropism, MmuPV1 appears to mimic many of the known features of neoplasia associated with more limited HPV strains: MmuPV1 cutaneous papillomas are classic warts, and MmuPV1-induced cervical cancer closely resembles human cervical cancer pathogenesis [
5,
9].
A desirable improvement to this model would be the ability to induce tumors in immune-competent strains. Such strains could be used to analyze the role of the immune system and, more generally, to analyze genes involved in oropharyngeal tumorigenesis—as most strains used for genetic analyses (e.g., FVB, B6) are immune-competent [
4,
26]. Additionally, the ability to study cancerous lesions, or to understand the factors needed to progress from in situ to the invasive disease, would increase the model’s versatility. Studies such as the analysis of tobacco carcinogens might reveal cofactors that can overcome immune defenses and/or lead to malignancy. Similarly, infecting immune-competent mice that carry mutations or genes known to promote papillomavirus oncogene-driven head-and-neck cancers (e.g., dominant-negative MAML, in the Notch pathway) [
4] might yield an immune-competent, malignant model.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}