
COVID-19 Modulates Inflammatory and Renal Markers That May Predict Hospital Outcomes among African American Males

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval
2.2. Study Design and Patients
2.3. Multi-Analyte Immunoassay and Enzyme-Linked Immunosorbent Assay (ELISA)
2.4. Statistical Analysis
3. Results
3.1. Patient Cohort
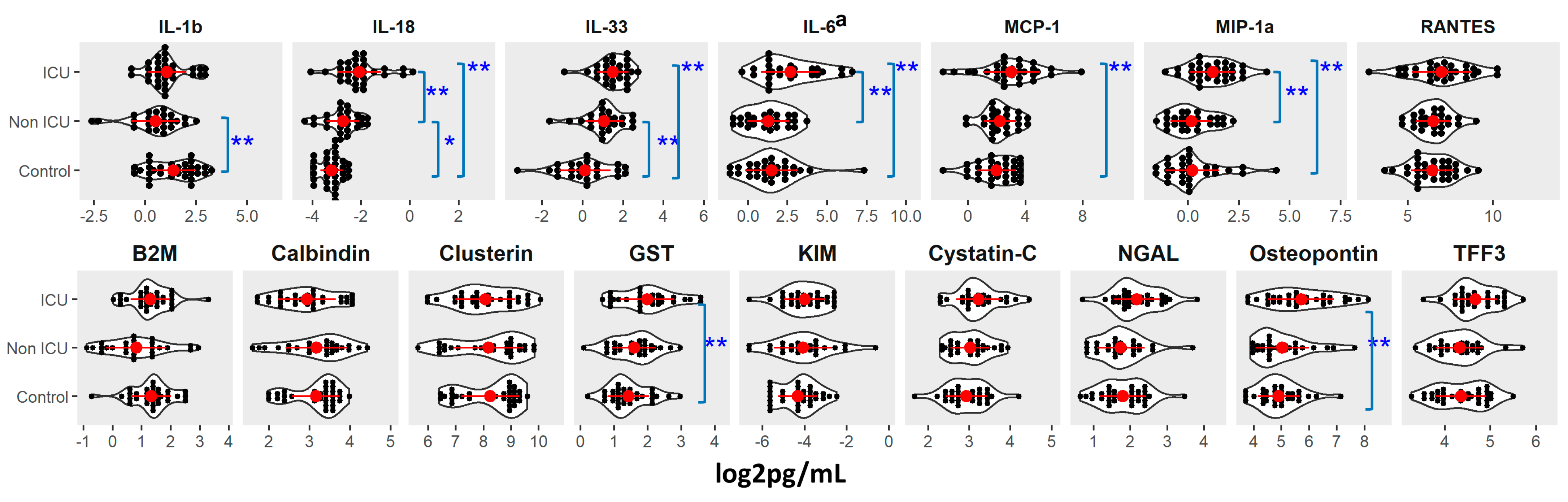
3.2. Association of Cytokines and Renal Injury Markers with Demographics and Baseline Comorbidities
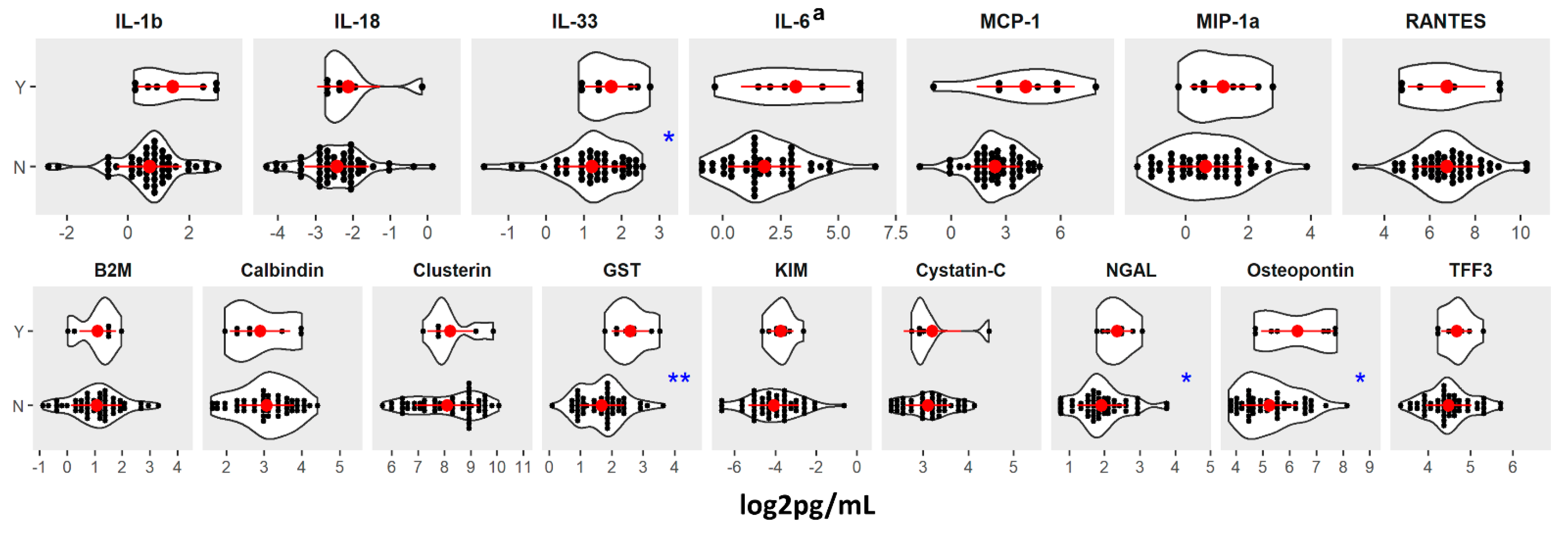
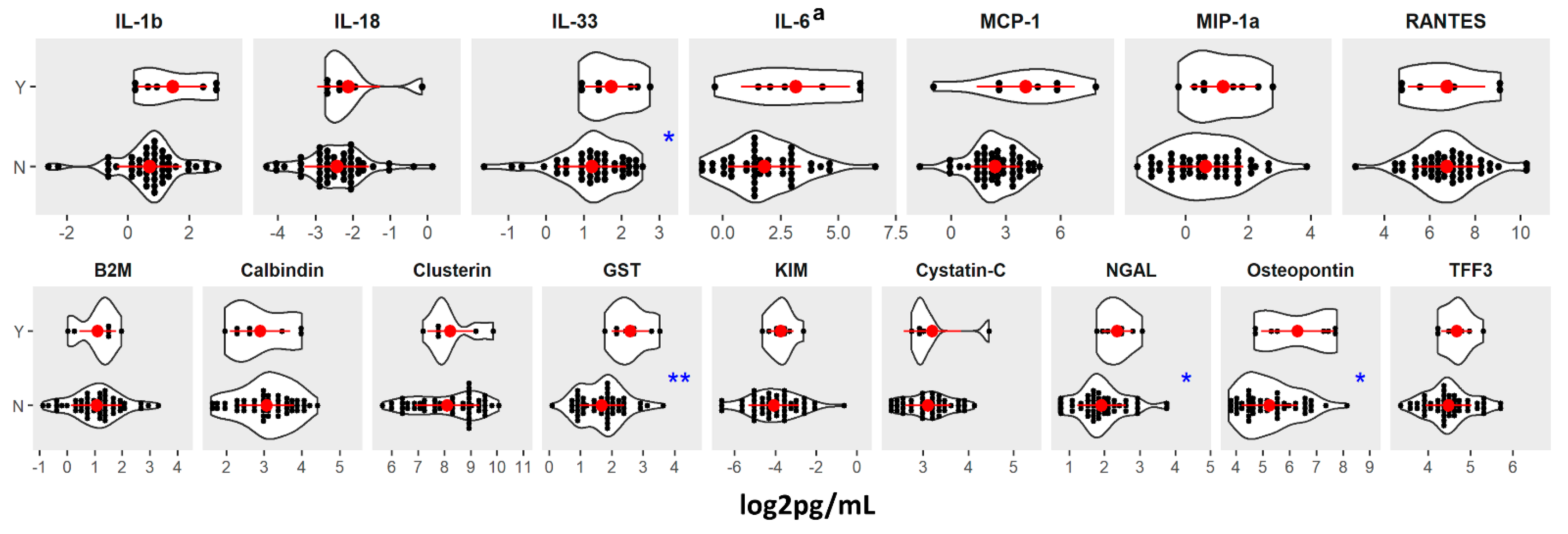
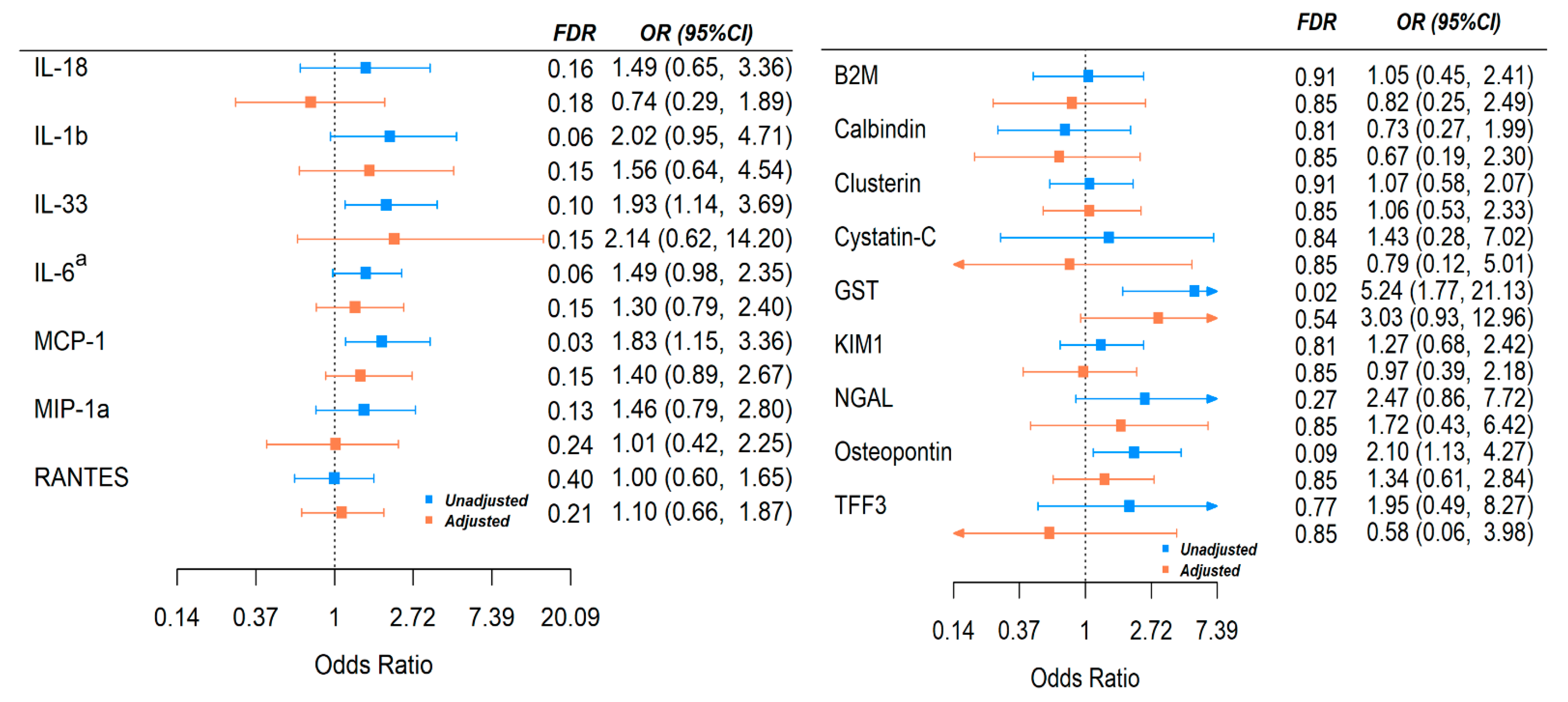
3.3. Association between Cytokines, Renal Injury Markers, and Risk of COVID-19 in-Hospital Death
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jamilloux, Y.; Henry, T.; Belot, A.; Viel, S.; Fauter, M.; El Jammal, T.; Walzer, T.; François, B.; Sève, P. Should we stimulate or suppress immune responses in COVID-19? Cytokine and anti-cytokine interventions. Autoimmun. Rev. 2020, 19, 102567. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 illness in native and immunosuppressed states: A clinical-therapeutic staging proposal. J. Heart Lung Transpl. 2020, 39, 405–407. [Google Scholar] [CrossRef] [Green Version]
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T.; Li, P.; Zhou, Y.; Lin, Y.F.; Duan, Q.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J. Infect. 2020, 80, 656–665. [Google Scholar] [CrossRef]
- Henderson, L.A.; Canna, S.W.; Schulert, G.S.; Volpi, S.; Lee, P.Y.; Kernan, K.F.; Caricchio, R.; Mahmud, S.; Hazen, M.M.; Halyabar, O.; et al. On the Alert for Cytokine Storm: Immunopathology in COVID-19. Arthritis Rheumatol. 2020, 72, 1059–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hojyo, S.; Uchida, M.; Tanaka, K.; Hasebe, R.; Tanaka, Y.; Murakami, M.; Hirano, T. How COVID-19 induces cytokine storm with high mortality. Inflamm Regen 2020, 40, 37. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. Efficacy of Tocilizumab in Patients Hospitalized with Covid-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Huet, T.; Beaussier, H.; Voisin, O.; Jouveshomme, S.; Dauriat, G.; Lazareth, I.; Sacco, E.; Naccache, J.M.; Bezie, Y.; Laplanche, S.; et al. Anakinra for severe forms of COVID-19: A cohort study. Lancet Rheumatol. 2020, 2, e393–e400. [Google Scholar] [CrossRef]
- Rampino, T.; Gregorini, M.; Perotti, L.; Ferrari, F.; Pattonieri, E.F.; Grignano, M.A.; Valente, M.; Garrone, A.; Islam, T.; Libetta, C.; et al. Hemoperfusion with CytoSorb as Adjuvant Therapy in Critically Ill Patients with SARS-CoV2 Pneumonia. Blood Purif. 2021, 50, 566–571. [Google Scholar] [CrossRef]
- Raza, A.; Estepa, A.; Chan, V.; Jafar, M.S. Acute Renal Failure in Critically Ill COVID-19 Patients With a Focus on the Role of Renal Replacement Therapy: A Review of What We Know So Far. Cureus 2020, 12, e8429. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Paek, J.H.; Kim, Y.; Park, W.Y.; Jin, K.; Hyun, M.; Lee, J.Y.; Kim, H.A.; Kwon, Y.S.; Park, J.S.; Han, S. Severe acute kidney injury in COVID-19 patients is associated with in-hospital mortality. PLoS ONE 2020, 15, e0243528. [Google Scholar] [CrossRef]
- Ahmadian, E.; Hosseiniyan Khatibi, S.M.; Razi Soofiyani, S.; Abediazar, S.; Shoja, M.M.; Ardalan, M.; Zununi Vahed, S. COVID-19 and kidney injury: Pathophysiology and molecular mechanisms. Rev. Med. Virol. 2020, 31, e2176. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://doi.org/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed on 1 August 2021).
- Bwire, G.M. Coronavirus: Why Men are More Vulnerable to COVID-19 Than Women? SN Compr. Clin. Med. 2020, 2, 874–876. [Google Scholar] [CrossRef]
- Quan, D.; Luna Wong, L.; Shallal, A.; Madan, R.; Hamdan, A.; Ahdi, H.; Daneshvar, A.; Mahajan, M.; Nasereldin, M.; Van Harn, M.; et al. Impact of Race and Socioeconomic Status on Outcomes in Patients Hospitalized with COVID-19. J. Gen. Intern Med. 2021, 36, 1302–1309. [Google Scholar] [CrossRef] [PubMed]
- Price-Haywood, E.G.; Burton, J.; Fort, D.; Seoane, L. Hospitalization and Mortality among Black Patients and White Patients with Covid-19. N. Engl. J. Med. 2020, 382, 2534–2543. [Google Scholar] [CrossRef]
- Suleyman, G.; Fadel, R.A.; Malette, K.M.; Hammond, C.; Abdulla, H.; Entz, A.; Demertzis, Z.; Hanna, Z.; Failla, A.; Dagher, C.; et al. Clinical Characteristics and Morbidity Associated With Coronavirus Disease 2019 in a Series of Patients in Metropolitan Detroit. JAMA Netw. Open 2020, 3, e2012270. [Google Scholar] [CrossRef]
- Raharja, A.; Tamara, A.; Kok, L.T. Association between Ethnicity and Severe COVID-19 Disease: A Systematic Review and Meta-analysis. J. Racial Ethn. Health Disparities 2020, 8, 1563–1572. [Google Scholar] [CrossRef]
- Pan, D.; Sze, S.; Minhas, J.S.; Bangash, M.N.; Pareek, N.; Divall, P.; Williams, C.M.; Oggioni, M.R.; Squire, I.B.; Nellums, L.B.; et al. The impact of ethnicity on clinical outcomes in COVID-19: A systematic review. EClinicalMedicine 2020, 23, 100404. [Google Scholar] [CrossRef] [PubMed]
- Anaele, B.I.; Doran, C.; McIntire, R. Visualizing COVID-19 Mortality Rates and African-American Populations in the USA and Pennsylvania. J. Racial Ethn. Health Disparities 2021, 8, 1356–1363. [Google Scholar] [CrossRef]
- Escobar, G.J.; Adams, A.S.; Liu, V.X.; Soltesz, L.; Chen, Y.I.; Parodi, S.M.; Ray, G.T.; Myers, L.C.; Ramaprasad, C.M.; Dlott, R.; et al. Racial Disparities in COVID-19 Testing and Outcomes: Retrospective Cohort Study in an Integrated Health System. Ann. Intern. Med. 2021, 174, 786–793. [Google Scholar] [CrossRef]
- Wu, K.H.; Hornsby, W.E.; Klunder, B.; Krause, A.; Driscoll, A.; Kulka, J.; Bickett-Hickok, R.; Fellows, A.; Graham, S.; Kaleba, E.O.; et al. Exposure and risk factors for COVID-19 and the impact of staying home on Michigan residents. PLoS ONE 2021, 16, e0246447. [Google Scholar] [CrossRef] [PubMed]
- Andrasfay, T.; Goldman, N. Reductions in 2020 US life expectancy due to COVID-19 and the disproportionate impact on the Black and Latino populations. Proc. Natl. Acad. Sci. USA 2021, 118, e2014746118. [Google Scholar] [CrossRef] [PubMed]
- Laguna-Goya, R.; Utrero-Rico, A.; Talayero, P.; Lasa-Lazaro, M.; Ramirez-Fernandez, A.; Naranjo, L.; Segura-Tudela, A.; Cabrera-Marante, O.; Rodriguez de Frias, E.; Garcia-Garcia, R.; et al. IL-6-based mortality risk model for hospitalized patients with COVID-19. J. Allergy Clin. Immunol. 2020, 146, 799–807.e9. [Google Scholar] [CrossRef] [PubMed]
- Satis, H.; Ozger, H.S.; Aysert Yildiz, P.; Hizel, K.; Gulbahar, O.; Erbas, G.; Aygencel, G.; Guzel Tunccan, O.; Ozturk, M.A.; Dizbay, M.; et al. Prognostic value of interleukin-18 and its association with other inflammatory markers and disease severity in COVID-19. Cytokine 2021, 137, 155302. [Google Scholar] [CrossRef]
- Munitz, A.; Edry-Botzer, L.; Itan, M.; Tur-Kaspa, R.; Dicker, D.; Marcoviciu, D.; Goren, M.G.; Mor, M.; Lev, S.; Gottesman, T.; et al. Rapid seroconversion and persistent functional IgG antibodies in severe COVID-19 patients correlates with an IL-12p70 and IL-33 signature. Sci. Rep. 2021, 11, 3461. [Google Scholar] [CrossRef]
- Burke, H.; Freeman, A.; Cellura, D.C.; Stuart, B.L.; Brendish, N.J.; Poole, S.; Borca, F.; Phan, H.T.T.; Sheard, N.; Williams, S.; et al. Inflammatory phenotyping predicts clinical outcome in COVID-19. Respir. Res. 2020, 21, 245. [Google Scholar] [CrossRef] [PubMed]
- Hue, S.; Beldi-Ferchiou, A.; Bendib, I.; Surenaud, M.; Fourati, S.; Frapard, T.; Rivoal, S.; Razazi, K.; Carteaux, G.; Delfau-Larue, M.H.; et al. Uncontrolled Innate and Impaired Adaptive Immune Responses in Patients with COVID-19 Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2020, 202, 1509–1519. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Jiang, L.; Li, X.; Lin, F.; Wang, Y.; Li, B.; Jiang, T.; An, W.; Liu, S.; Liu, H.; et al. Clinical and pathological investigation of patients with severe COVID-19. JCI Insight 2020, 5, 138070. [Google Scholar] [CrossRef] [PubMed]
- Chi, Y.; Ge, Y.; Wu, B.; Zhang, W.; Wu, T.; Wen, T.; Liu, J.; Guo, X.; Huang, C.; Jiao, Y.; et al. Serum Cytokine and Chemokine Profile in Relation to the Severity of Coronavirus Disease 2019 in China. J. Infect. Dis. 2020, 222, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Jontvedt Jorgensen, M.; Holter, J.C.; Christensen, E.E.; Schjalm, C.; Tonby, K.; Pischke, S.E.; Jenum, S.; Skeie, L.G.; Nur, S.; Lind, A.; et al. Increased interleukin-6 and macrophage chemoattractant protein-1 are associated with respiratory failure in COVID-19. Sci. Rep. 2020, 10, 21697. [Google Scholar] [CrossRef]
- Xu, Z.S.; Shu, T.; Kang, L.; Wu, D.; Zhou, X.; Liao, B.W.; Sun, X.L.; Zhou, X.; Wang, Y.Y. Temporal profiling of plasma cytokines, chemokines and growth factors from mild, severe and fatal COVID-19 patients. Signal Transduct. Target Ther. 2020, 5, 100. [Google Scholar] [CrossRef] [PubMed]
- Abers, M.S.; Delmonte, O.M.; Ricotta, E.E.; Fintzi, J.; Fink, D.L.; de Jesus, A.A.A.; Zarember, K.A.; Alehashemi, S.; Oikonomou, V.; Desai, J.V.; et al. An immune-based biomarker signature is associated with mortality in COVID-19 patients. JCI Insight 2021, 6, e144455. [Google Scholar] [CrossRef] [PubMed]
- Komaru, Y.; Doi, K.; Nangaku, M. Urinary Neutrophil Gelatinase-Associated Lipocalin in Critically Ill Patients With Coronavirus Disease 2019. Crit. Care Explor. 2020, 2, e0181. [Google Scholar] [CrossRef]
- Bolt, H.M.; Thier, R. Relevance of the deletion polymorphisms of the glutathione S-transferases GSTT1 and GSTM1 in pharmacology and toxicology. Curr. Drug Metab. 2006, 7, 613–628. [Google Scholar] [CrossRef]
- Saadat, M. An evidence for correlation between the glutathione S-transferase T1 (GSTT1) polymorphism and outcome of COVID-19. Clin. Chim. Acta 2020, 508, 213–216. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | Non-ICU | ICU | p | ||
|---|---|---|---|---|---|
| (N = 31) | (N = 26) | (N = 30) | |||
| BMI | ≤30 | 11 (35.5%) | 10 (38.5%) | 14 (46.7%) | 0.678 |
| >30 | 20 (64.5%) | 16 (61.5%) | 16 (53.3%) | ||
| Smoke | Never/unknown | 8 (25.8%) | 15 (50.0%) | 9 (34.6%) | 0.025 |
| Former smoker | 8 (25.8%) | 11 (36.7%) | 12 (46.2%) | ||
| Current smoker | 15 (48.4%) | 4 (13.3%) | 5 (19.2%) | ||
| Substance abuse | Yes | 14 (45.2%) | 6 (23.1%) | 4 (13.3%) | 0.022 |
| No | 17 (54.8%) | 20 (76.9%) | 26 (86.7%) | ||
| Age | 50–60 | 11 (35.5%) | 8 (30.8%) | 7 (23.3%) | 0.624 |
| 61–70 | 14 (45.2%) | 10 (38.5%) | 17 (56.7%) | ||
| >70 | 6 (19.4%) | 8 (30.8%) | 6 (20.0%) | ||
| qSOFA | <1 | NA | 16 (61.5%) | 4 (13.3%) | <0.001 |
| ≥1 | NA | 10 (38.5%) | 26 (86.7%) | ||
| Medical History | |||||
| Cardiovascular and thoracic | Yes | 30 (96.8%) | 24 (92.3%) | 28 (93.3%) | 0.735 |
| No | 1 (3.2%) | 2 (7.7%) | 2 (6.7%) | ||
| Hypertension | Yes | 28 (90.3%) | 24 (92.3%) | 26 (86.7%) | 0.827 |
| No | 3 (9.7%) | 2 (7.7%) | 4 (13.3%) | ||
| Heart failure | Yes | 10 (32.3%) | 5 (19.2%) | 9 (30.0%) | 0.57 |
| No | 21 (67.7%) | 21 (80.8%) | 21 (70.0%) | ||
| Respiratory and pulmonary | Yes | 13 (41.9%) | 6 (23.1%) | 16 (53.3%) | 0.068 |
| No | 18 (58.1%) | 20 (76.9%) | 14 (46.7%) | ||
| G.I./digestive | Yes | 16 (51.6%) | 8 (30.8%) | 12 (40.0%) | 0.29 |
| No | 15 (48.4%) | 18 (69.2%) | 18 (60.0%) | ||
| Endocrine | Yes | 17 (54.8%) | 21 (80.8%) | 16 (53.3%) | 0.064 |
| No | 14 (45.2%) | 5 (19.2%) | 14 (46.7%) | ||
| T2D | Yes | 14 (45.2%) | 19 (73.1%) | 14 (46.7%) | 0.075 |
| No | 17 (54.8%) | 7 (26.9%) | 16 (53.3%) | ||
| Thyroid | Yes | 2 (6.5%) | 2 (7.7%) | 3 (10.0%) | 0.891 |
| No | 29 (93.5%) | 24 (92.3%) | 27 (90.0%) | ||
| Neurological | Yes | 14 (45.2%) | 12 (46.2%) | 6 (20.0%) | 0.06 |
| No | 17 (54.8%) | 14 (53.8%) | 24 (80.0%) | ||
| Genitourinary | Yes | 22 (71.0%) | 20 (76.9%) | 25 (83.3%) | 0.538 |
| No | 9 (29.0%) | 6 (23.1%) | 5 (16.7%) | ||
| Dialysis | Yes | 24 (77.4%) | 22 (84.6%) | 21 (70.0%) | 0.432 |
| No | 7 (22.6%) | 4 (15.4%) | 9 (30.0%) | ||
| Circulatory and vascular | Yes | 23 (74.2%) | 14 (53.8%) | 12 (40.0%) | 0.025 |
| No | 8 (25.8%) | 12 (46.2%) | 18 (60.0%) | ||
| Cancer history | Yes | 5 (16.1%) | 1 (3.8%) | 0 (0%) | 0.036 |
| No | 26 (83.9%) | 25 (96.2%) | 30 (100%) | ||
| Hospital Death | ||||
|---|---|---|---|---|
| Yes | No | |||
| (N = 8) | (N = 48) | |||
| BMI | ≤30 | 5 (63%) | 27 (56%) | >0.999 |
| >30 | 3 (38%) | 21 (44%) | ||
| Smoke | Never/unknown | 4 (50%) | 20 (42%) | 0.54 |
| Former smoker | 4 (50%) | 19 (40%) | ||
| Current smoker | 0 (0%) | 9 (19%) | ||
| Substance abuse | Yes | 2 (25%) | 8 (17%) | 0.623 |
| No | 6 (75%) | 40 (83%) | ||
| Age | 50–60 | 1 (13%) | 14 (29%) | 0.478 |
| 61–70 | 4 (50%) | 23 (48%) | ||
| >70 | 3 (38%) | 11 (23%) | ||
| qSOFA | <1 | 0 (0%) | 20 (42%) | 0.041 |
| ≥1 | 8 (100%) | 28 (58%) | ||
| Charleston comorbidity index | 1–2 | 0 (0%) | 6 (13%) | 0.588 |
| 3–4 | 1 (13%) | 10 (21%) | ||
| >4 | 7 (88%) | 32 (67%) | ||
| Medical History | ||||
| Cardiovascular and thoracic | Yes | 8 (100%) | 44 (92%) | >0.999 |
| No | 0 (0%) | 4 (8%) | ||
| Hypertension | Yes | 7 (88%) | 43 (90%) | >0.999 |
| No | 1 (13%) | 5 (10%) | ||
| Heart failure | Yes | 0 (0%) | 14 (29%) | 0.18 |
| No | 8 (100%) | 34 (71%) | ||
| Respiratory and pulmonary | Yes | 4 (50%) | 18 (38%) | 0.698 |
| No | 4 (50%) | 30 (63%) | ||
| G.I./digestive | Yes | 2 (25%) | 18 (38%) | 0.697 |
| No | 6 (75%) | 30 (63%) | ||
| Endocrine | Yes | 6 (75%) | 31 (65%) | 0.703 |
| No | 2 (25%) | 17 (35%) | ||
| T2D | Yes | 4 (50%) | 29 (60%) | 0.704 |
| No | 4 (50%) | 19 (40%) | ||
| Thyroid | Yes | 2 (25%) | 3 (6%) | 0.144 |
| No | 6 (75%) | 45 (94%) | ||
| Neurological | Yes | 1 (13%) | 17 (35%) | 0.414 |
| No | 7 (88%) | 31 (65%) | ||
| Genitourinary | Yes | 7 (88%) | 38 (79%) | >0.999 |
| No | 1 (13%) | 10 (21%) | ||
| Dialysis | Yes | 5 (63%) | 8 (17%) | 0.012 |
| No | 3 (38%) | 40 (83%) | ||
| Circulatory and vascular | Yes | 3 (38%) | 23 (48%) | 0.712 |
| No | 5 (63%) | 25 (52%) | ||
| Cancer history | Yes | 0 (0%) | 1 (2%) | >0.999 |
| No | 8 (100%) | 47 (98%) | ||
| Symptoms | ||||
| SOB | Yes | 7 (88%) | 30 (65%) | 0.411 |
| No | 1 (13%) | 16 (35%) | ||
| Cough | Yes | 4 (50%) | 26 (57%) | >0.999 |
| No | 4 (50%) | 20 (43%) | ||
| Fever/chills | Yes | 6 (75%) | 22 (48%) | 0.253 |
| No | 2 (25%) | 24 (52%) | ||
| Headache | Yes | 0 (0%) | 3 (7%) | >0.999 |
| No | 8 (100%) | 43 (93%) | ||
| Nausea/diarrhea/vomiting | Yes | 3 (38%) | 15 (33%) | >0.999 |
| No | 5 (63%) | 31 (67%) | ||
| Congestion | Yes | 0 (0%) | 2 (4%) | >0.999 |
| No | 8 (100%) | 44 (96%) | ||
| Fatigue/body ache/weakness | Yes | 7 (88%) | 19 (42%) | 0.024 |
| No | 1 (13%) | 26 (58%) | ||
| Change in scent/smell/lack of appetite | Yes | 0 (0%) | 9 (20%) | 0.324 |
| No | 8 (100%) | 36 (80%) | ||
| Experimental/Relevant Medications | ||||
| Plaquenil/HCQ | Yes | 8 (100%) | 32 (68%) | 0.091 |
| No | 0 (0%) | 15 (32%) | ||
| Remdesivir | Yes | 0 (0%) | 2 (4%) | >0.999 |
| No | 8 (100%) | 43 (96%) | ||
| Steroids | Yes | 8 (100%) | 35 (74%) | 0.178 |
| No | 0 (0%) | 12 (26%) | ||
| Azithromycin | Yes | 1 (13%) | 12 (26%) | 0.664 |
| No | 7 (88%) | 35 (74%) | ||
| Cytokine Inhibitors | Yes | 2 (25%) | 3 (6%) | 0.149 |
| No | 6 (75%) | 44 (94%) | ||
| NSAIDS | Yes | 2 (25%) | 14 (30%) | >0.999 |
| No | 6 (75%) | 33 (70%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fonseca, W.; Asai, N.; Yagi, K.; Malinczak, C.-A.; Savickas, G.; Johnson, C.C.; Murray, S.; Zoratti, E.M.; Lukacs, N.W.; Li, J.; et al. COVID-19 Modulates Inflammatory and Renal Markers That May Predict Hospital Outcomes among African American Males. Viruses 2021, 13, 2415. https://doi.org/10.3390/v13122415
Fonseca W, Asai N, Yagi K, Malinczak C-A, Savickas G, Johnson CC, Murray S, Zoratti EM, Lukacs NW, Li J, et al. COVID-19 Modulates Inflammatory and Renal Markers That May Predict Hospital Outcomes among African American Males. Viruses. 2021; 13(12):2415. https://doi.org/10.3390/v13122415
Chicago/Turabian StyleFonseca, Wendy, Nobuhiro Asai, Kazuma Yagi, Carrie-Anne Malinczak, Gina Savickas, Christine C. Johnson, Shannon Murray, Edward M. Zoratti, Nicholas W. Lukacs, Jia Li, and et al. 2021. "COVID-19 Modulates Inflammatory and Renal Markers That May Predict Hospital Outcomes among African American Males" Viruses 13, no. 12: 2415. https://doi.org/10.3390/v13122415
APA StyleFonseca, W., Asai, N., Yagi, K., Malinczak, C.-A., Savickas, G., Johnson, C. C., Murray, S., Zoratti, E. M., Lukacs, N. W., Li, J., & Schuler IV, C. F. (2021). COVID-19 Modulates Inflammatory and Renal Markers That May Predict Hospital Outcomes among African American Males. Viruses, 13(12), 2415. https://doi.org/10.3390/v13122415