
Influenza Vaccine Effectiveness in Preventing Severe Outcomes in Patients Hospitalized with Laboratory-Confirmed Influenza during the 2017–2018 Season. A Retrospective Cohort Study in Catalonia (Spain)

 ,
,  ,
,  and
and
Abstract
:1. Introduction
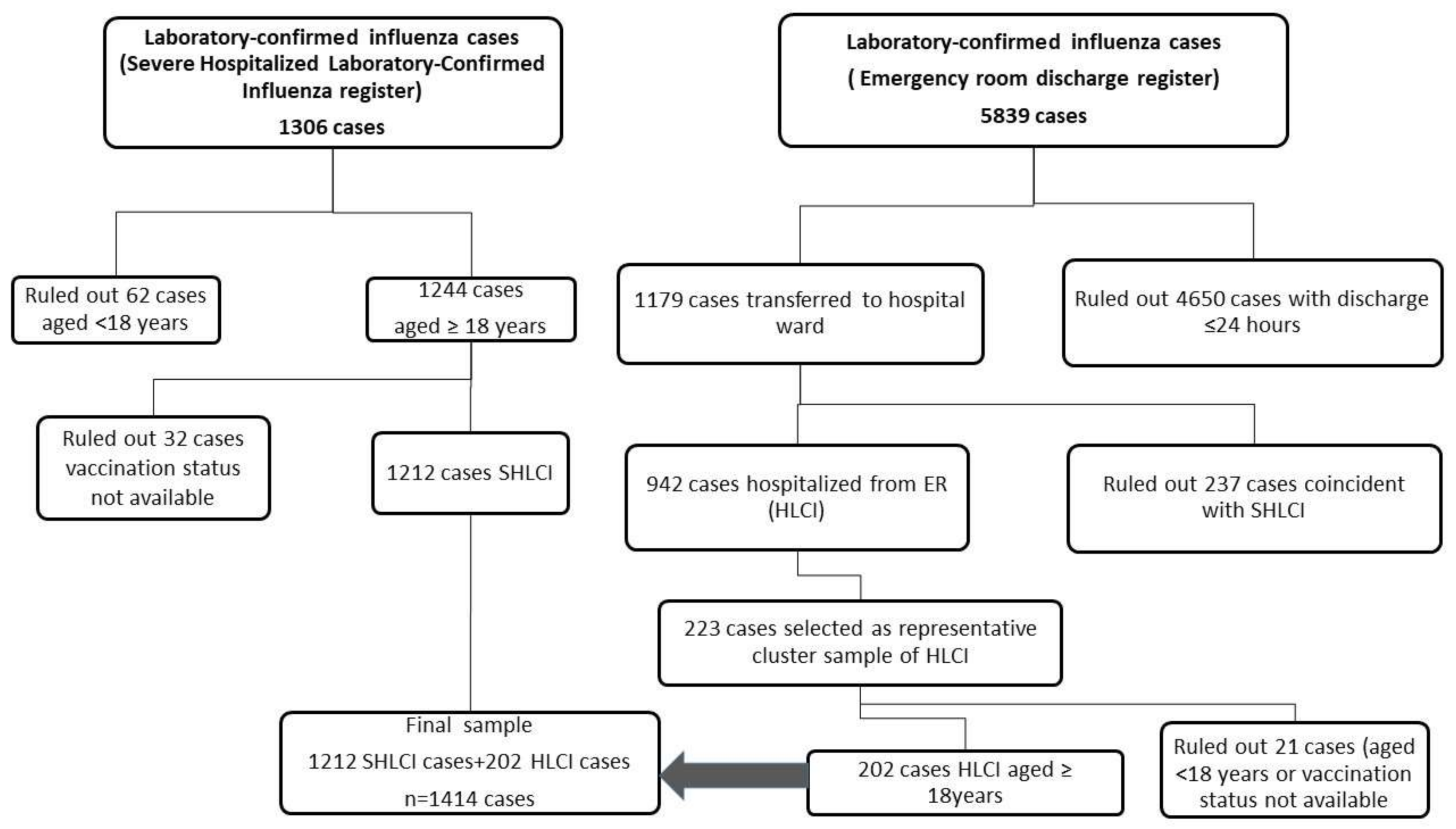
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Coleman, B.L.; Fadel, S.A.; Fitzpatrick, T.; Thomas, S.-M. Risk factors for serious outcomes associated with influenza illness in high- versus low- and middle-income countries: Systematic literature review and meta-analysis. Influenza Other Respi. Viruses 2018, 12, 22–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagshaw, S.M.; Tran, D.T.; Opgenorth, D.; Wang, X.; Zuege, D.J.; Ingolfsson, A.; Stelfox, H.T.; Thanh, N.X. Assessment of costs of avoidable delays in intensive care unit discharge. JAMA Netw. Open 2020, 3, e2013913. [Google Scholar] [CrossRef] [PubMed]
- Borràs, E.; Cabezas, C.; Martínez, M.; Urbiztondo, L. Guia Tècnica per a la Campanya de Vacunació Antigripal Estacional 2017. 2017. Available online: https://canalsalut.genact.cat/web/.content/_A-Z/G/Grip/documents/arxius/guia_tecnica_antigripal.pdf (accessed on 15 October 2020).
- Agència de Salut Pública de Catalunya. Pla D’Informació de les Infeccions Respiratòries Agudes a Catalunya (PIDIRAC) 2017–2018. Estratègia de Vigilància Dels Casos Greus Produïts per la Infecció pel Virus de la Grip, Barcelona. Agència de Salut Pública de Catalunya. 2017. Available online: http://hdl.handle.net/11351/3397 (accessed on 15 October 2020).
- Department de Salut, Subdirecció General de Vigilància i Resposta a Emergècies de Salut Pública. Pla d’Informació de les Infeccions Respiratòries Agudes a Catalunya ( PIDIRAC) 2017–2018. 2017. Available online: http://hdl.handle.net/11351/3385 (accessed on 15 October 2020).
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision. 2016. Available online: https://icd.who.int/browse10/2016/en (accessed on 10 January 2020).
- Pla D’informació de les Infeccions Respiratòries Agudes a Catalunya (PIDIRAC) 2018–2019, Barcelona: Subdirecció General de Vigilància i Resposta a Emergècies de Salut Pública. 2019. Available online: http://hdl.handle.net/11351/4318 (accessed on 15 October 2020).
- Torner, N.; Martínez, A.; Basile, L.; Mosquera, M.M.; Antón, A.; Rius, C.; Sala, M.R.; Minguell, S.; Plasencia, E.; Carol, M.; et al. Descriptive study of severe hospitalized cases of laboratory-confirmed influenza during five epidemic seasons (2010–2015). BMC Res. Notes 2018, 11, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martocchio, J.J.; Liao, H. (Eds.) Research in Personnel and Human Resources Management; Emerald Group Publishing Limited: Bingley, UK, 2009; Volume 28. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Summary of Influenza Virus Characterization Data Reported by National Influenza Centers to the European Surveillance System (TESSy) for Weeks 40/2017 to 20/2018. 2018. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/influenza-virus-characterisation-summary-2017-2018.pdf (accessed on 15 October 2020).
- Basile, L.; Torner, N.; Martínez, A.; Mosquera, M.M.; Marcos, M.A.; Jane, M. Seasonal influenza surveillance: Observational study on the 2017–2018 season with predominant B influenza virus circulation. Vacunas 2019, 20, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Oliva, J.; Delgado-Sanz, C.; Larrauri, A. Estimating the burden of seasonal influenza in Spain from surveillance of mild and severe influenza disease, 2010–2016. Influenza Other Respi. Viruses 2018, 12, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Ridenhour, B.J.; Campitelli, M.A.; Kwong, J.C.; Rosella, L.C.; Armstrong, B.G.; Mangtani, P.; Calzavara, A.J.; Shay, D.K. Effectiveness of inactivated influenza vaccines in preventing influenza-associated deaths and hospitalizations among Ontario residents aged ≥ 65 years: Estimates with generalized linear models accounting for healthy vaccinee effects. PLoS ONE 2013, 8, e76318. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.; Chung, J.R.; Monto, A.S.; Martin, E.T.; Belongia, E.A.; McLean, H.Q.; Gaglani, M.; Murthy, K.; Zimmerman, R.K.; Nowalk, M.P.; et al. Influenza vaccine effectiveness in older adults compared with younger adults over five seasons. Vaccine 2018, 36, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Joshi, M.; Chandra, D.; Mittadodla, P.; Bartter, T. The impact of vaccination on influenza-related respiratory failure and mortality in hospitalized elderly patients over the 2013–2014 season. Open Respir. Med. J. 2015, 9, 9–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beumer, M.C.; Koch, R.M.; van Beuningen, D.; OudeLashof, A.M.; van de Veerdonk, F.L.; Kolwijck, E.; van der Hoeven, J.G.; Bergmans, D.C.; Hoedemaekers, C.W.E. Influenza virus and factors that are associated with ICU admission, pulmonary co-infections and ICU mortality. J. Crit. Care 2019, 50, 59–65. [Google Scholar] [CrossRef]
- Martin-Loeches, I.; Lemiale, V.; Geoghegan, P.; McMahon, M.A.; Pickkers, P.; Soares, M.; Perner, A.; Meyhoff, T.S.; Bukan, R.B.; Rello, J.; et al. Influenza and associated co-infections in critically ill immunosuppressed patients. Crit. Care 2019, 23, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arriola, C.; Garg, S.; Anderson, E.J.; Ryan, P.A.; George, A.; Zansky, S.M.; Bennett, N.; Reingold, A.; Bargsten, M.; Miller, L.; et al. Influenza vaccination modifies disease severity among community-dwelling adults hospitalized with influenza. Clin. Infect. Dis. 2017, 65, 1289–1297. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Seasonal Influenza Vaccination and Antiviral Use in EU/EEA Member States–Overview of Vaccine Recommendations for 2017–2018 and Vaccination Coverage Rates for 2015–2016 and 2016–2017 Influenza Seasons. 2018. Available online: https://www.ecdc.europa.eu/en/publications-data/seasonal-influenza-vaccination-antiviral-use-eu-eea-member-states (accessed on 15 October 2020).
- Ministerio de Sanidad Consumo y Bienestar Social; Dirección General de Salud Pública. Coberturas vacunales en España, Madrid. 2019. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/docs/CoberturasVacunacion/Todas_las_tablas.pdf#page=1 (accessed on 30 June 2020).
- Health Protection Surveillance Centre. Influenza and Other Seasonal Respiratory Viruses in Ireland; 2017/2018; Health Protection Surveillance Centre (HSE): Dublin, Ireland, 2018. [Google Scholar]
- Lina, B.; Georges, A.; Burtseva, E.; Nunes, M.C.; Andrew, M.K.; McNeil, S.A.; Ruiz-Palacios, G.M.; Feng, L.; Kyncl, J.; Vanhems, P.; et al. Complicated hospitalization due to influenza: Results from the Global Hospital Influenza Network for the 2017–2018 season. BMC Infect. Dis. 2020, 20, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Pozo-Rodríguez, F.; López-Campos, J.L.; Álvarez-Martínez, C.J.; Castro-Acosta, A.; Agüero, R.; Hueto, J.; Hernández-Hernández, J.; Barrón, M.; Abraira, V.; Forte, A.; et al. Clinical audit of COPD patients requiring hospital admissions in Spain: AUDIPOC Study. PLoS ONE 2012, 7, e42156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arriola, C.S.; Anderson, E.J.; Baumbach, J.; Bennett, N.; Bohm, S.; Hill, M.; Lindegren, M.L.; Lung, K.; Meek, J.; Mermel, E.; et al. Does influenza vaccination modify influenza severity? Data on older adults hospitalized with influenza during the 2012−2013 season in the United States. J. Infect. Dis. 2015, 212, 1200–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garland, A.; Connors, A.F. Optimal timing of transfer out of the intensive care unit. Am. J. Crit. Care 2013, 22, 390–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nates, J.L.; Nunnally, M.; Kleinpell, R.; Blosser, S.; Goldner, J.; Birriel, B.; Fowler, C.S.; Byrum, D.; Miles, W.S.; Bailey, H.; et al. ICU admission, discharge, and triage guidelines. Crit. Care Med. 2016, 44, 1553–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazagatos, C.; Delgado-Sanz, C.; Oliva, J.; Gherasim, A.; Larrauri, A. Exploring the risk of severe outcomes and the role of seasonal influenza vaccination in pregnant women hospitalized with confirmed influenza, Spain, 2010/11–2015/16. PLoS ONE 2018, 13, e0200934. [Google Scholar] [CrossRef] [PubMed]
- Naleway, A.L.; Ball, S.; Kwong, J.C.; Wyant, B.E.; Katz, M.A.; Regan, A.K.; Russell, M.L.; Klein, N.P.; Chung, H.; Simmonds, K.A.; et al. Estimating vaccine effectiveness against hospitalized influenza during pregnancy: Multicountry protocol for a retrospective cohort study. JMIR Res. Protoc. 2019, 8, e11333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bond, H.S.; Sullivan, S.G.; Cowling, B.J. Regression approaches in the test-negative study design for assessment of influenza vaccine effectiveness. Epidemiol. Infect. 2016, 144, 1601–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Patient Parameters | Total Number of Hospitalized Influenza Cases n = 1414 | Vaccinated Cases n = 465 (32.9%) | Unvaccinated Cases n = 949 (67.1%) | p Value a | d-Cohen/ w-Cohen |
|---|---|---|---|---|---|
| Age mean (SD) b | 71.5 (15.2) | 77.6 (11.3) | 68.5 (16.0) | <0.001 | 0.62 |
| Age group | |||||
| ≥60 years | 1118 (79.1%) | 437 (94.0%) | 681 (71.8%) | 0.000 | 0.26 |
| 18–59 years | 296 (20.9%) | 28 (6.0%) | 268 (28.2%) | ||
| Sex | |||||
| Male | 804 (56.9%) | 269 (57.8%) | 535 (56.4%) | 0.600 | 0.01 |
| Female | 610 (43.1%) | 196 (42.2%) | 414 (43.6%) | ||
| Comorbidities (≥1) | |||||
| Yes | 1127 (79.7%) | 406 (87.3%) | 721 (76.0%) | <0.001 | 0.13 |
| No | 287 (20.3%) | 59 (12.7%) | 228 (24.0%) | ||
| COPD c | |||||
| Yes | 461 (32.6%) | 190 (40.9%) | 271 (28.6%) | <0.001 | 0.12 |
| No | 953 (67.4%) | 275 (59.1%) | 678 (71.4%) | ||
| Obesity (BMI > 40) d | |||||
| Yes | 111 (7.85%) | 37 (8.0%) | 74 (7.8%) | 0.909 | 0.003 |
| No | 1303 (92.1%) | 428 (92.0%) | 875 (92.2%) | ||
| Diabetes | |||||
| Yes | 385 (27.2%) | 141 (30.3%) | 244 (25.7%) | 0.069 | 0.05 |
| No | 1029 (72.8%) | 324 (69.7%) | 705 (74.3%) | ||
| Chronic renal disease | |||||
| Yes | 275 (19.4%) | 106 (22.8%) | 169 (17.8%) | 0.028 | 0.06 |
| No | 1139 (80.6%) | 359 (77.2%) | 780 (82.2%) | ||
| Immunodeficiency | |||||
| Yes | 230 (16.3%) | 68 (14.6%) | 162 (17.1%) | 0.242 | 0.03 |
| No | 1184 (83.7%) | 397 (85.4%) | 787 (82.9%) | ||
| Cardiovascular disease | |||||
| Yes | 614 (43.4%) | 237 (51.0%) | 377 (39.7%) | <0.001 | 0.10 |
| No | 800 (56.6%) | 228 (49.0%) | 572 (60.3%) | ||
| Chronic liver disease | |||||
| Yes | 88 (6.22%) | 28 (6.0%) | 60 (6.3%) | 0.836 | 0.006 |
| No | 1326 (93.8%) | 437 (94.0%) | 889 (93.7%) | ||
| Other comorbidities e | |||||
| Yes | 165 (11.7%) | 66 (14.2%) | 99 (10.4%) | 0.041 | 0.06 |
| No | 1249 (88.3%) | 399 (85.8%) | 850 (89.6%) | ||
| NI f treatment | |||||
| Yes | 1299 (91.9%) | 437 (94.0%) | 862 (90.9%) | 0.045 | 0.05 |
| NI f treatment (timing) | |||||
| ≤48 h from onset of symptoms | 511 (36.9%) | 169 (36.3%) | 342 (36.1%) | 0.075 | 0.05 |
| >48 h from onset of symptoms | 759 (54.8%) | 257 (55.3%) | 502 (53.0%) | 0.046 | |
| No | 114 (8.1%) | 28 (6.0%) | 86 (9.1%) | ||
| Type of influenza virus | |||||
| B | 859 (60.9%) | 295 (63.4%) | 564 (59.7%) | 0.174 | 0.04 |
| A | 551 (39.1%) | 170 (36.6%) | 381 (40.3%) | ||
| Outcome variables: | |||||
| ICU admission | |||||
| Yes | 214 (15.1%) | 52 (11.2%) | 162 (17.1%) | 0.005 | 0.08 |
| No | 1200 (84.9%) | 413 (88.8%) | 787 (82.9%) | ||
| LOS g | |||||
| Mean days (SD) | 12.8 (15.9) | 12.1 (14.1) | 13.1 (16.8) | 0.228 | 0.06 |
| ICU LOS h | |||||
| Mean days (SD) | 9.35 (10.4) | 9.49 (9.30) | 9.31 (10.8) | 0.917 | 0.02 |
| Patient Parameters | SHLCI a n = 1227 | HLCI b n = 187 | p Value | d-Cohen/ w-Cohen |
|---|---|---|---|---|
| Age, mean (SD) c | 71.1 (15.3) | 68.5 (16.0) | 0.008 * | 0.17 |
| Age group | ||||
| ≥60 years | 959 (78.2%) | 159 (85.0%) | 0.040 | 0.06 |
| 18–59 years | 268 (21.8%) | 28 (15.0%) | ||
| Sex | ||||
| Male | 709 (57.8%) | 95 (50.8%) | 0.086 | 0.05 |
| Female | 518 (42.2%) | 92 (49.2%) | ||
| Comorbidities (≥1) | ||||
| Yes | 956 (77.9%) | 171 (91.4%) | <0.001 | 0.11 |
| No | 271 (22.1%) | 16 (8.56%) | ||
| Influenza vaccination | ||||
| Yes | 440 (35.9%) | 25 (13.4%) | <0.001 | 0.16 |
| No | 787 (64.1%) | 162 (86.6%) | ||
| NI d treatment | ||||
| Yes | 1146 (93.4%) | 153 (81.8%) | <0.001 | 0.14 |
| No | 81 (6.60%) | 34 (18.2%) | ||
| NI d treatment (timing) | ||||
| ≤48 h from symptom onset | 452 (37.7%) | 59 (31.7%) | <0.001 | 0.14 |
| >48 h from symptom onset | 665 (55.5%) | 94 (50.5%) | ||
| No | 81 (6.8%) | 33 (17.7%) |
| Patient Parameters | ICU Admission n = 214 (15.1%) | No ICU Admission n = 1200 (84.9%) | p Value | d-Cohen/ w-Cohen |
|---|---|---|---|---|
| Influenza vaccination | ||||
| Yes | 52 (11.2%) | 413 (88.8%) | 0.003 | 0.08 |
| No | 162 (17.1%) | 787 (82.9%) | ||
| Age | ||||
| Years, mean (SD) b | 64.0 (13.6) | 72.8 (15.1) | <0.001 * | 0.59 |
| Age group | ||||
| ≥60 years | 141 (12.6%) | 977 (87.4%) | <0.001 | 0.14 |
| 18–59 years | 73 (24.7%) | 223 (75.3%) | ||
| Sex | ||||
| Male | 135 (16.8%) | 669 (83.2%) | 0.046 | 0.05 |
| Female | 79 (13.0%) | 531 (87.0%) | ||
| Comorbidities | ||||
| Yes | 164 (14.6%) | 963 (85.4%) | 0.230 | 0.03 |
| No | 50 (17.4%) | 237 (82.6%) | ||
| COPD c | ||||
| Yes | 74 (16.1%) | 387 (83.9%) | 0.502 | 0.02 |
| No | 140 (14.7%) | 813 (85.3%) | ||
| Obesity (BMI > 30) d | ||||
| Yes | 23 (20.7%) | 88 (79.3%) | 0.098 | 0.05 |
| No | 191 (14.7%) | 1112 (85.3%) | ||
| Diabetes | ||||
| Yes | 60 (15.6%) | 325 (84.4%) | 0.767 | 0.01 |
| No | 154 (15.0%) | 875 (85.0%) | ||
| Chronic renal disease | ||||
| Yes | 31 (11.3%) | 244 (88.7%) | 0.043 | 0.05 |
| No | 183 (16.1%) | 956 (83.9%) | ||
| Immunodeficiency | ||||
| Yes | 33 (14.3%) | 197 (85.7%) | 0.728 | 0.01 |
| No | 181 (15.3%) | 1003 (84.7%) | ||
| Cardiovascular disease | ||||
| Yes | 79 (12.9%) | 535 (87.1%) | 0.037 | 0.05 |
| No | 135 (16.9%) | 665 (83.1%) | ||
| Chronic liver disease | ||||
| Yes | 24 (27.3%) | 64 (72.7%) | 0.002 | 0.09 |
| No | 190 (14.3%) | 1136 (85.7%) | ||
| Other comorbidities e | ||||
| Yes | 27 (16.4%) | 138 (83.6%) | 0.630 | 0.01 |
| No | 187 (15.0%) | 1062 (85.0%) | ||
| NI f treatment | ||||
| Yes | 199 (15.3%) | 1100 (84.7%) | 0.552 | 0.02 |
| No | 15 (13.2%) | 99 (86.8%) | ||
| NI f treatment (timing) | ||||
| ≤48 h from symptom onset | 62 (12.1%) | 449 (87.9%) | 0.750 | 0.06 |
| >48 h from symptom onset | 128 (16.9%) | 631 (83.1%) | 0.323 | |
| No | 15 (13.2%) | 99 (86.8%) | ||
| Influenza virus type | ||||
| A | 92 (16.7%) | 459 (83.3%) | ||
| B | 122 (14.2%) | 737 (85.8%) | 0.205 | 0.04 |
| LOS g | ||||
| Mean days (SD) b | 22.4 (20.3) | 11.1 (14.4) | <0.001 * | 0.73 |
| All Patients | ICU Admission | No ICU Admission | aVE a | p Value |
|---|---|---|---|---|
| n = 1414 | n = 214 (15.1%) | n = 1200 (84.9%) | (95%CI) b | |
| Influenza vaccination Vaccinated (465; 32.9%) | 52 (11.2%) | 413 (88.8%) | 31% (1; 52) | 0.04 |
| Unvaccinated (949; 67.1%) | 162 (17.1%) | 787 (82.9%) | Ref. | |
| Influenza B n = 859 (60.7%) | ||||
| Vaccinated (295; 34.3%) | 33 (11.2%) | 262 (88.8%) | 25% (−18; 52) | 0.21 |
| Unvaccinated (564; 65.7%) | 89 (15.8%) | 475 (84.2%) | Ref. | |
| Influenza A n = 551 (38.9%) | ||||
| Vaccinated (170; 30.9%) | 19 (11.2%) | 151 (88.8%) | 40% (−11; 68) | 0.09 |
| Unvaccinated (381; 69.1%) | 73 (19.2%) | 308 (80.8%) | Ref. | |
| Female, age <60 years n = 125 (8.8%) | ||||
| Vaccinated (14; 11.2%) | 1 (7.1%) | 13 (92.9%) | 72% (−135; 97) | 0.24 |
| Unvaccinated (111; 88.8%) | 28 (25.2%) | 83 (74.8%) | Ref. | |
| Female, age ≥60 years n = 485 (34.3%) | ||||
| Vaccinated (182; 37.5%) | 17 (9.3%) | 165 (90.7%) | 23% (−48; 60) | 0.43 |
| Unvaccinated (303; 62.5%) | 33 (10.9%) | 270 (89.1%) | Ref. | |
| Male, age <60 years n = 171 (24.2%) | ||||
| Vaccinated (14; 8.2%) | 3 (21.4%) | 11 (78.6%) | 29% (−74; 82) | 0.62 |
| Unvaccinated (157; 91.8%) | 41(26.1%) | 116 (73.9%) | Ref. | |
| Male, age ≥60 years n = 633 (44.7%) | ||||
| Vaccinated (255; 40.3%) | 31 (12.2%) | 224 (87.8%) | 32% (−10; 58) | 0.12 |
| Unvaccinated (378; 59.7%) | 60(15.9%) | 318 (84.1%) | Ref. | |
| ICU Admission | No ICU Admission | VE * | aVE ** | p Value | |
|---|---|---|---|---|---|
| All Patients n = 1414 | n = 214 (15.1%) | n = 1200 (84.9%) | (95% CI) | (95% CI) | |
| Influenza vaccination | |||||
| Vaccinated (465; 32.9%) | 52 (11.2%) | 413 (88.8%) | 39% (15; 56) | 31% (1; 52) | 0.040 |
| Unvaccinated (949; 67.1%) | 162 (17.1%) | 787 (82.9%) | Ref. | ||
| SHLCI a n = 1227 | 210 (17.1%) | 1017 (82.9%) | |||
| Vaccinated (440: 35.9%) | 52 (11.8%) | 388 (88.2%) | 47% (25; 62) | 40% (13; 58) | 0.007 |
| Unvaccinated (787; 64.1%) | 158 (20.1%) | 629 (79.9%) | |||
| HLCI b n = 187 | 4 (2.1%) | 183 (97.9%) | |||
| Vaccinated (25; 13.3%) | 0 (0.0%) | 25 (100%) | 31% (−578; 99.5) *** | Not computable | ---- |
| Unvaccinated (162; 86.7%) | 4 (2.5%) | 158 (97.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acosta, L.; Soldevila, N.; Torner, N.; Martínez, A.; Ayneto, X.; Rius, C.; Jané, M.; Domínguez, A.; the Influenza Surveillance Network of Catalonia, PIDIRAC. Influenza Vaccine Effectiveness in Preventing Severe Outcomes in Patients Hospitalized with Laboratory-Confirmed Influenza during the 2017–2018 Season. A Retrospective Cohort Study in Catalonia (Spain). Viruses 2021, 13, 1465. https://doi.org/10.3390/v13081465
Acosta L, Soldevila N, Torner N, Martínez A, Ayneto X, Rius C, Jané M, Domínguez A, the Influenza Surveillance Network of Catalonia, PIDIRAC. Influenza Vaccine Effectiveness in Preventing Severe Outcomes in Patients Hospitalized with Laboratory-Confirmed Influenza during the 2017–2018 Season. A Retrospective Cohort Study in Catalonia (Spain). Viruses. 2021; 13(8):1465. https://doi.org/10.3390/v13081465
Chicago/Turabian StyleAcosta, Lesly, Nuria Soldevila, Nuria Torner, Ana Martínez, Xavier Ayneto, Cristina Rius, Mireia Jané, Angela Domínguez, and the Influenza Surveillance Network of Catalonia, PIDIRAC. 2021. "Influenza Vaccine Effectiveness in Preventing Severe Outcomes in Patients Hospitalized with Laboratory-Confirmed Influenza during the 2017–2018 Season. A Retrospective Cohort Study in Catalonia (Spain)" Viruses 13, no. 8: 1465. https://doi.org/10.3390/v13081465
APA StyleAcosta, L., Soldevila, N., Torner, N., Martínez, A., Ayneto, X., Rius, C., Jané, M., Domínguez, A., & the Influenza Surveillance Network of Catalonia, PIDIRAC. (2021). Influenza Vaccine Effectiveness in Preventing Severe Outcomes in Patients Hospitalized with Laboratory-Confirmed Influenza during the 2017–2018 Season. A Retrospective Cohort Study in Catalonia (Spain). Viruses, 13(8), 1465. https://doi.org/10.3390/v13081465