
Advances in Pediatric HIV-1 Cure Therapies and Reservoir Assays

Abstract
:1. Introduction
1.1. Pediatric HIV-1 Infection
1.2. Distinctive Features of Perinatal Infection
1.3. Maintenance and Expansion of the Reservoir
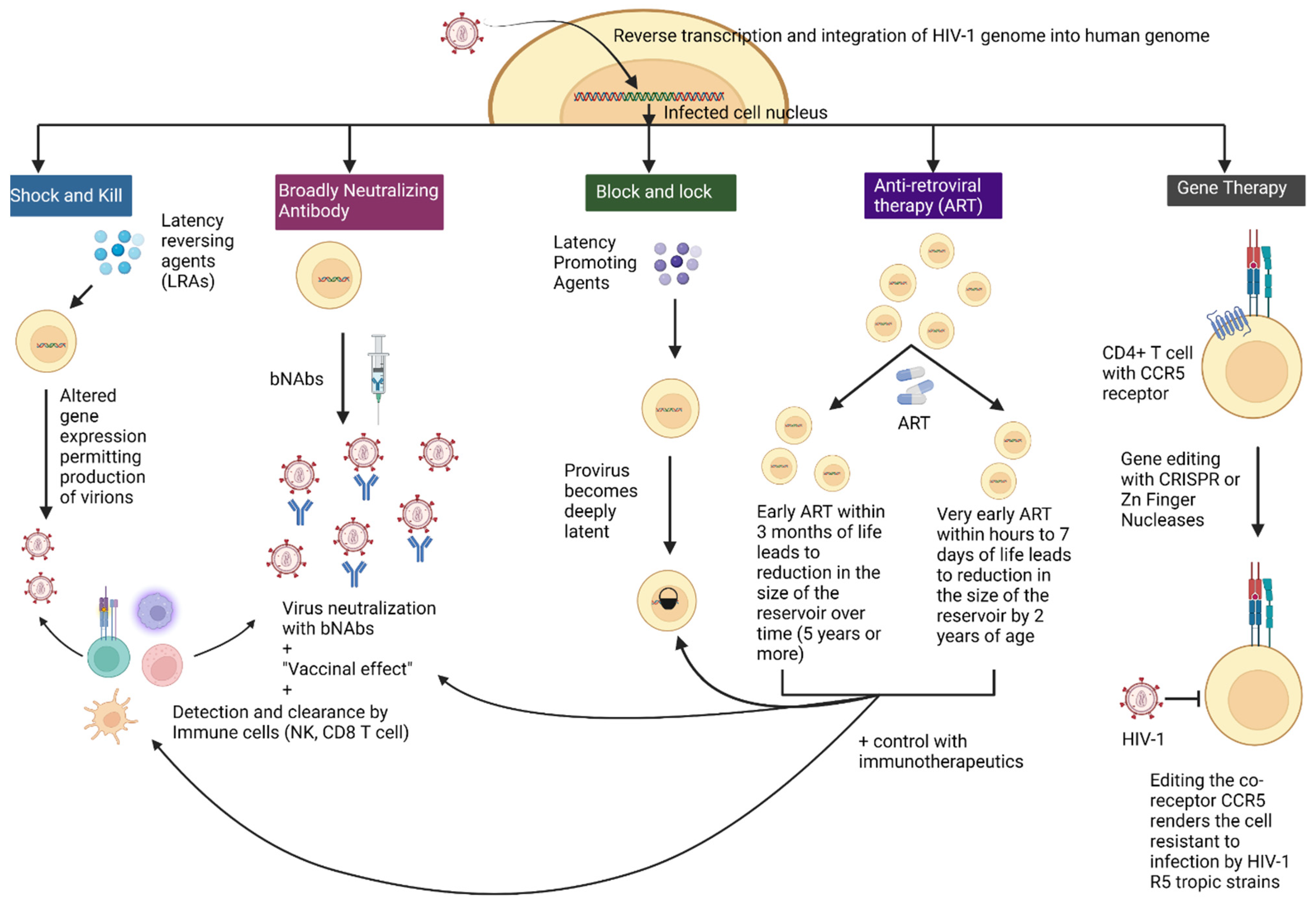
2. Therapies for HIV-1 Infection
2.1. Current Interventions under Investigation for Pediatric HIV-1 Remission and Cure
2.1.1. Very Early and Early Antiretroviral Therapy in Neonates to Reduce HIV-1 Reservoirs to Achieve Remission
2.1.2. Broadly Neutralizing Antibodies for Use in Perinatal HIV-1 Infection to Achieve Remission
2.2. Interventions under Study to Achieve ART Free Remission and Cure
2.2.1. Epigenetic and Provirus Targeted Therapies
2.2.2. Immune System Targeted Treatment
2.2.3. Gene Editing Based Treatment
3. Assays to Measure the HIV-1 Reservoir
3.1. Classical Assays for HIV-1 Reservoir Measurement
3.1.1. Culture Based Assays
Quantitative Viral Outgrowth Assay
Tat/Rev Induced Limiting Dilution Assay
3.2. Molecular Assays
3.2.1. Quantitative PCR
3.2.2. Alu PCR
3.2.3. Single-Plex Droplet Digital PCR
3.3. Recently Developed Assays for Reservoir Measurement
3.3.1. Molecular Assays
3.4. Flow Cytometry
HIV-1 Flow
3.5. Proviral Landscape Analysis
3.5.1. Near Full-Length Individual Proviral Sequencing
3.5.2. Quadruplex Quantitative PCR
3.5.3. Matched Integration Site Analysis and Proviral Sequencing
3.5.4. Parallel HIV-1 RNA, Integration Site and Proviral Sequencing
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS. Global HIV and AIDS Statistics Fact Sheet 2022. Available online: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf (accessed on 8 August 2022).
- Perelson, A.S.; Essunger, P.; Cao, Y.; Vesanen, M.; Hurley, A.; Saksela, K.; Markowitz, M.; Ho, D.D. Decay characteristics of HIV-1-infected compartments during combination therapy. Nature 1997, 387, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Fischl, M.A.; Richman, D.D.; Grieco, M.H.; Gottlieb, M.S.; Volberding, P.A.; Laskin, O.L.; Leedom, J.M.; Groopman, J.E.; Mildvan, D.; Schooley, R.T.; et al. The efficacy of azidothymidine (AZT) in the treatment of patients with AIDS and AIDS-related complex. A double-blind, placebo-controlled trial. N. Engl. J. Med. 1987, 317, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Caliendo, A.M.; Hirsch, M.S. Combination therapy for infection due to human immunodeficiency virus type 1. Clin. Infect. Dis. 1994, 18, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Siliciano, J.D.; Kajdas, J.; Finzi, D.; Quinn, T.C.; Chadwick, K.; Margolick, J.B.; Kovacs, C.; Gange, S.J.; Siliciano, R.F. Long-term follow-up studies confirm the stability of the latent reservoir for HIV-1 in resting CD4+ T cells. Nat. Med. 2003, 9, 727–728. [Google Scholar] [CrossRef] [PubMed]
- Finzi, D.; Hermankova, M.; Pierson, T.; Carruth, L.M.; Buck, C.; Chaisson, R.E.; Quinn, T.C.; Chadwick, K.; Margolick, J.; Brookmeyer, R.; et al. Identification of a reservoir for HIV-1 in patients on highly active antiretroviral therapy. Science 1997, 278, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Finzi, D.; Blankson, J.; Siliciano, J.D.; Margolick, J.B.; Chadwick, K.; Pierson, T.; Smith, K.; Lisziewicz, J.; Lori, F.; Flexner, C.; et al. Latent infection of CD4+ T cells provides a mechanism for lifelong persistence of HIV-1, even in patients on effective combination therapy. Nat. Med. 1999, 5, 512–517. [Google Scholar] [CrossRef]
- Chun, T.W.; Stuyver, L.; Mizell, S.B.; Ehler, L.A.; Mican, J.A.; Baseler, M.; Lloyd, A.L.; Nowak, M.A.; Fauci, A.S. Presence of an inducible HIV-1 latent reservoir during highly active antiretroviral therapy. Proc. Natl. Acad. Sci. USA 1997, 94, 13193–13197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, J.K.; Hezareh, M.; Gunthard, H.F.; Havlir, D.V.; Ignacio, C.C.; Spina, C.A.; Richman, D.D. Recovery of replication-competent HIV despite prolonged suppression of plasma viremia. Science 1997, 278, 1291–1295. [Google Scholar] [CrossRef] [PubMed]
- Siliciano, J.D.; Siliciano, R.F. Assays to Measure Latency, Reservoirs, and Reactivation. Curr. Top. Microbiol. Immunol. 2018, 417, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Ho, Y.C.; Shan, L.; Hosmane, N.N.; Wang, J.; Laskey, S.B.; Rosenbloom, D.I.; Lai, J.; Blankson, J.N.; Siliciano, J.D.; Siliciano, R.F. Replication-competent noninduced proviruses in the latent reservoir increase barrier to HIV-1 cure. Cell 2013, 155, 540–551. [Google Scholar] [CrossRef]
- Eisele, E.; Siliciano, R.F. Redefining the viral reservoirs that prevent HIV-1 eradication. Immunity 2012, 37, 377–388. [Google Scholar] [CrossRef] [Green Version]
- Barton, K.M.; Palmer, S.E. How to Define the Latent Reservoir: Tools of the Trade. Curr. HIV/AIDS Rep. 2016, 13, 77–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Mohsen, M.; Richman, D.; Siliciano, R.F.; Nussenzweig, M.C.; Howell, B.J.; Martinez-Picado, J.; Chomont, N.; Bar, K.J.; Yu, X.G.; Lichterfeld, M.; et al. Recommendations for measuring HIV reservoir size in cure-directed clinical trials. Nat. Med. 2020, 26, 1339–1350. [Google Scholar] [CrossRef]
- Hermankova, M.; Siliciano, J.D.; Zhou, Y.; Monie, D.; Chadwick, K.; Margolick, J.B.; Quinn, T.C.; Siliciano, R.F. Analysis of human immunodeficiency virus type 1 gene expression in latently infected resting CD4+ T lymphocytes in vivo. J. Virol. 2003, 77, 7383–7392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crooks, A.M.; Bateson, R.; Cope, A.B.; Dahl, N.P.; Griggs, M.K.; Kuruc, J.D.; Gay, C.L.; Eron, J.J.; Margolis, D.M.; Bosch, R.J.; et al. Precise Quantitation of the Latent HIV-1 Reservoir: Implications for Eradication Strategies. J. Infect. Dis. 2015, 212, 1361–1365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venanzi Rullo, E.; Cannon, L.; Pinzone, M.R.; Ceccarelli, M.; Nunnari, G.; O’Doherty, U. Genetic Evidence That Naive T Cells Can Contribute Significantly to the Human Immunodeficiency Virus Intact Reservoir: Time to Re-evaluate Their Role. Clin. Infect. Dis. 2019, 69, 2236–2237. [Google Scholar] [CrossRef]
- Pace, M.J.; Agosto, L.; Graf, E.H.; O’Doherty, U. HIV reservoirs and latency models. Virology 2011, 411, 344–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siliciano, R.F.; Greene, W.C. HIV latency. Cold Spring Harb. Perspect. Med. 2011, 1, a007096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coiras, M.; Lopez-Huertas, M.R.; Perez-Olmeda, M.; Alcami, J. Understanding HIV-1 latency provides clues for the eradication of long-term reservoirs. Nat. Rev. Microbiol. 2009, 7, 798–812. [Google Scholar] [CrossRef] [PubMed]
- Dahl, V.; Josefsson, L.; Palmer, S. HIV reservoirs, latency, and reactivation: Prospects for eradication. Antivir. Res. 2010, 85, 286–294. [Google Scholar] [CrossRef]
- Wang, Z.; Simonetti, F.R.; Siliciano, R.F.; Laird, G.M. Measuring replication competent HIV-1: Advances and challenges in defining the latent reservoir. Retrovirology 2018, 15, 21. [Google Scholar] [CrossRef] [PubMed]
- Zerbato, J.M.; McMahon, D.K.; Sobolewski, M.D.; Mellors, J.W.; Sluis-Cremer, N. Naive CD4+ T Cells Harbor a Large Inducible Reservoir of Latent, Replication-competent Human Immunodeficiency Virus Type 1. Clin. Infect. Dis. 2019, 69, 1919–1925. [Google Scholar] [CrossRef] [PubMed]
- Chun, T.W.; Davey, R.T., Jr.; Engel, D.; Lane, H.C.; Fauci, A.S. Re-emergence of HIV after stopping therapy. Nature 1999, 401, 874–875. [Google Scholar] [CrossRef] [PubMed]
- Chun, T.W.; Justement, J.S.; Murray, D.; Hallahan, C.W.; Maenza, J.; Collier, A.C.; Sheth, P.M.; Kaul, R.; Ostrowski, M.; Moir, S.; et al. Rebound of plasma viremia following cessation of antiretroviral therapy despite profoundly low levels of HIV reservoir: Implications for eradication. AIDS 2010, 24, 2803–2808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luzuriaga, K.; Gay, H.; Ziemniak, C.; Sanborn, K.B.; Somasundaran, M.; Rainwater-Lovett, K.; Mellors, J.W.; Rosenbloom, D.; Persaud, D. Viremic relapse after HIV-1 remission in a perinatally infected child. N. Engl. J. Med. 2015, 372, 786–788. [Google Scholar] [CrossRef] [Green Version]
- Ananworanich, J.; Dube, K.; Chomont, N. How does the timing of antiretroviral therapy initiation in acute infection affect HIV reservoirs? Curr. Opin. HIV AIDS 2015, 10, 18–28. [Google Scholar] [CrossRef]
- Jain, V.; Hartogensis, W.; Bacchetti, P.; Hunt, P.W.; Hatano, H.; Sinclair, E.; Epling, L.; Lee, T.H.; Busch, M.P.; McCune, J.M.; et al. Antiretroviral therapy initiated within 6 months of HIV infection is associated with lower T-cell activation and smaller HIV reservoir size. J. Infect. Dis. 2013, 208, 1202–1211. [Google Scholar] [CrossRef] [Green Version]
- Hocqueloux, L.; Avettand-Fenoel, V.; Jacquot, S.; Prazuck, T.; Legac, E.; Melard, A.; Niang, M.; Mille, C.; Le Moal, G.; Viard, J.P.; et al. Long-term antiretroviral therapy initiated during primary HIV-1 infection is key to achieving both low HIV reservoirs and normal T cell counts. J. Antimicrob. Chemother. 2013, 68, 1169–1178. [Google Scholar] [CrossRef] [Green Version]
- Colby, D.J.; Trautmann, L.; Pinyakorn, S.; Leyre, L.; Pagliuzza, A.; Kroon, E.; Rolland, M.; Takata, H.; Buranapraditkun, S.; Intasan, J.; et al. Rapid HIV RNA rebound after antiretroviral treatment interruption in persons durably suppressed in Fiebig I acute HIV infection. Nat. Med. 2018, 24, 923–926. [Google Scholar] [CrossRef]
- Davey, R.T., Jr.; Bhat, N.; Yoder, C.; Chun, T.W.; Metcalf, J.A.; Dewar, R.; Natarajan, V.; Lempicki, R.A.; Adelsberger, J.W.; Miller, K.D.; et al. HIV-1 and T cell dynamics after interruption of highly active antiretroviral therapy (HAART) in patients with a history of sustained viral suppression. Proc. Natl. Acad. Sci. USA 1999, 96, 15109–15114. [Google Scholar] [CrossRef]
- Rothenberger, M.K.; Keele, B.F.; Wietgrefe, S.W.; Fletcher, C.V.; Beilman, G.J.; Chipman, J.G.; Khoruts, A.; Estes, J.D.; Anderson, J.; Callisto, S.P.; et al. Large number of rebounding/founder HIV variants emerge from multifocal infection in lymphatic tissues after treatment interruption. Proc. Natl. Acad. Sci. USA 2015, 112, E1126–E1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Persaud, D.; Pierson, T.; Ruff, C.; Finzi, D.; Chadwick, K.R.; Margolick, J.B.; Ruff, A.; Hutton, N.; Ray, S.; Siliciano, R.F. A stable latent reservoir for HIV-1 in resting CD4(+) T lymphocytes in infected children. J. Clin. Invest. 2000, 105, 995–1003. [Google Scholar] [CrossRef] [PubMed]
- Frange, P.; Faye, A.; Avettand-Fenoel, V.; Bellaton, E.; Descamps, D.; Angin, M.; David, A.; Caillat-Zucman, S.; Peytavin, G.; Dollfus, C.; et al. HIV-1 virological remission lasting more than 12 years after interruption of early antiretroviral therapy in a perinatally infected teenager enrolled in the French ANRS EPF-CO10 paediatric cohort: A case report. Lancet HIV 2016, 3, e49–e54. [Google Scholar] [CrossRef] [Green Version]
- Persaud, D.; Luzuriaga, K. Absence of HIV-1 after treatment cessation in an infant. N. Engl. J. Med. 2014, 370, 678. [Google Scholar] [CrossRef] [PubMed]
- Violari, A.; Cotton, M.F.; Kuhn, L.; Schramm, D.B.; Paximadis, M.; Loubser, S.; Shalekoff, S.; Da Costa Dias, B.; Otwombe, K.; Liberty, A.; et al. A child with perinatal HIV infection and long-term sustained virological control following antiretroviral treatment cessation. Nat. Commun. 2019, 10, 412. [Google Scholar] [CrossRef] [Green Version]
- Ajibola, G.; Garcia-Broncano, P.; Maswabi, K.; Bennett, K.; Hughes, M.D.; Moyo, S.; Mohammed, T.; Jean-Philippe, P.; Sakoi, M.; Batlang, O.; et al. Viral Reservoir in Early-Treated Human Immunodeficiency Virus-Infected Children and Markers for Sustained Viral Suppression. Clin. Infect. Dis. 2021, 73, e997–e1003. [Google Scholar] [CrossRef] [PubMed]
- Nsheha, A.H.; Dow, D.E.; Kapanda, G.E.; Hamel, B.C.; Msuya, L.J. Adherence to antiretroviral therapy among HIV-infected children receiving care at Kilimanjaro Christian Medical Centre (KCMC), Northern Tanzania: A cross-sectional analytical study. Pan. Afr. Med. J. 2014, 17, 238. [Google Scholar] [CrossRef]
- Ricci, G.; Netto, E.M.; Luz, E.; Rodamilans, C.; Brites, C. Adherence to antiretroviral therapy of Brazilian HIV-infected children and their caregivers. Braz. J. Infect. Dis. 2016, 20, 429–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delicio, A.M.; Lajos, G.J.; Amaral, E.; Cavichiolli, F.; Polydoro, M.; Milanez, H. Adverse effects in children exposed to maternal HIV and antiretroviral therapy during pregnancy in Brazil: A cohort study. Reprod. Health 2018, 15, 76. [Google Scholar] [CrossRef]
- Shah, I. Adverse effects of antiretroviral therapy in HIV-1 infected children. J. Trop. Pediatr. 2006, 52, 244–248. [Google Scholar] [CrossRef]
- Barlow-Mosha, L.; Eckard, A.R.; McComsey, G.A.; Musoke, P.M. Metabolic complications and treatment of perinatally HIV-infected children and adolescents. J. Int. AIDS Soc. 2013, 16, 18600. [Google Scholar] [CrossRef] [PubMed]
- Vreeman, R.C.; Scanlon, M.L.; McHenry, M.S.; Nyandiko, W.M. The physical and psychological effects of HIV infection and its treatment on perinatally HIV-infected children. J. Int. AIDS Soc. 2015, 18, 20258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dybul, M.; Attoye, T.; Baptiste, S.; Cherutich, P.; Dabis, F.; Deeks, S.G.; Dieffenbach, C.; Doehle, B.; Goodenow, M.M.; Jiang, A.; et al. The case for an HIV cure and how to get there. Lancet HIV 2021, 8, e51–e58. [Google Scholar] [CrossRef] [PubMed]
- Deeks, S.G.; Archin, N.; Cannon, P.; Collins, S.; Jones, R.B.; de Jong, M.; Lambotte, O.; Lamplough, R.; Ndung’u, T.; Sugarman, J.; et al. Research priorities for an HIV cure: International AIDS Society Global Scientific Strategy 2021. Nat. Med. 2021, 27, 2085–2098. [Google Scholar] [CrossRef]
- Hill, A.L.; Rosenbloom, D.I.; Fu, F.; Nowak, M.A.; Siliciano, R.F. Predicting the outcomes of treatment to eradicate the latent reservoir for HIV-1. Proc. Natl. Acad. Sci. USA 2014, 111, 13475–13480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rainwater-Lovett, K.; Luzuriaga, K.; Persaud, D. Very early combination antiretroviral therapy in infants: Prospects for cure. Curr. Opin. HIV AIDS 2015, 10, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Sáez-Cirión, A.; Bacchus, C.; Hocqueloux, L.; Avettand-Fenoel, V.; Girault, I.; Lecuroux, C.; Potard, V.; Versmisse, P.; Melard, A.; Prazuck, T.; et al. Post-Treatment HIV-1 Controllers with a Long-Term Virological Remission after the Interruption of Early Initiated Antiretroviral Therapy ANRS VISCONTI Study. PLoS Pathog. 2013, 9, e1003211. [Google Scholar] [CrossRef]
- Li, J.Z.; Blankson, J.N. How elite controllers and posttreatment controllers inform our search for an HIV-1 cure. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef]
- Mastrangelo, A.; Banga, R.; Perreau, M. Elite and posttreatment controllers, two facets of HIV control. Curr. Opin. HIV AIDS 2022, 17, 325–332. [Google Scholar] [CrossRef]
- Allers, K.; Hutter, G.; Hofmann, J.; Loddenkemper, C.; Rieger, K.; Thiel, E.; Schneider, T. Evidence for the cure of HIV infection by CCR5Delta32/Delta32 stem cell transplantation. Blood 2011, 117, 2791–2799. [Google Scholar] [CrossRef]
- Hutter, G.; Nowak, D.; Mossner, M.; Ganepola, S.; Mussig, A.; Allers, K.; Schneider, T.; Hofmann, J.; Kucherer, C.; Blau, O.; et al. Long-term control of HIV by CCR5 Delta32/Delta32 stem-cell transplantation. N. Engl. J. Med. 2009, 360, 692–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, R.K.; Abdul-Jawad, S.; McCoy, L.E.; Mok, H.P.; Peppa, D.; Salgado, M.; Martinez-Picado, J.; Nijhuis, M.; Wensing, A.M.J.; Lee, H.; et al. HIV-1 remission following CCR5Delta32/Delta32 haematopoietic stem-cell transplantation. Nature 2019, 568, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Björn-Erik, O.; Jensen, E.K.; Lübke, N.; Wensing, A.; Martinez-Picado, J.; Kaiser, R.; Nijhuis, M.; Salgado, M.; Harrer, T.; Heger, E.; et al. Analytic treatment interruption (ATI) after allogeneic CCR5-D32 HSCT for AML in 2013. In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Seattle, WA, USA, 6 March 2019. [Google Scholar]
- Dickter, J.; Weibel, S.; Cardoso, A.; Li, S.; Gendzekhadze, K.; Feng, Y.; Dadwal, S.; Taplitz, R.; Ross, J.; Aribi, A.; et al. The ‘City of Hope’ Patient: Prolonged HIV-1 remission without antiretrovirals (ART) after allogeneic hematopoietic stem cell transplantation (aHCT) of CCR5-Delta 32/Delta 32 donor cells for acute myelogenous leukemia (AML). In Proceedings of the AIDS, Montreal, QC, Canada, 1 August 2022. [Google Scholar]
- Hsu, J.; Glesby, M.; Shore, T.B.; Small, C.; Gergis, U.; Mayer, S.A.; Phillips, A.A.; Petz, L.D.; Browning, R.; Warshaw, M.; et al. HIV-1 Remission with CCR5∆32∆32 Haplo-Cord Transplant in a U.S. Woman: IMPAACT P1107. In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Denver, CO, USA, 15 February 2022. [Google Scholar]
- Turk, G.; Seiger, K.; Lian, X.; Sun, W.; Parsons, E.M.; Gao, C.; Rassadkina, Y.; Polo, M.L.; Czernikier, A.; Ghiglione, Y.; et al. A Possible Sterilizing Cure of HIV-1 Infection Without Stem Cell Transplantation. Ann. Intern. Med. 2022, 175, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Lian, X.; Gao, C.; Sun, X.; Einkauf, K.B.; Chevalier, J.M.; Chen, S.M.Y.; Hua, S.; Rhee, B.; Chang, K.; et al. Distinct viral reservoirs in individuals with spontaneous control of HIV-1. Nature 2020, 585, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Wilfert, C.M.; Wilson, C.; Luzuriaga, K.; Epstein, L. Pathogenesis of pediatric human immunodeficiency virus type 1 infection. J. Infect. Dis. 1994, 170, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Bryson, Y.J.; Luzuriaga, K.; Sullivan, J.L.; Wara, D.W. Proposed definitions for in utero versus intrapartum transmission of HIV-1. N. Engl. J. Med. 1992, 327, 1246–1247. [Google Scholar] [CrossRef] [PubMed]
- Wara, D.W.; Luzuriaga, K.; Martin, N.L.; Sullivan, J.L.; Bryson, Y.J. Maternal transmission and diagnosis of human immunodeficiency virus during infancy. Ann. N. Y. Acad. Sci. 1993, 693, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Millar, J.R.; Bengu, N.; Fillis, R.; Sprenger, K.; Ntlantsana, V.; Vieira, V.A.; Khambati, N.; Archary, M.; Muenchhoff, M.; Groll, A.; et al. High-frequency failure of combination antiretroviral therapy in paediatric HIV infection is associated with unmet maternal needs causing maternal non-adherence. EClinicalMedicine 2020, 22, 100344. [Google Scholar] [CrossRef] [PubMed]
- Tobin, N.H.; Aldrovandi, G.M. Immunology of pediatric HIV infection. Immunol. Rev. 2013, 254, 143–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goulder, P.J.; Lewin, S.R.; Leitman, E.M. Paediatric HIV infection: The potential for cure. Nat. Rev. Immunol. 2016, 16, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Vieira, V.A.; Herbert, N.; Cromhout, G.; Adland, E.; Goulder, P. Role of Early Life Cytotoxic T Lymphocyte and Natural Killer Cell Immunity in Paediatric HIV Cure/Remission in the Anti-Retroviral Therapy Era. Front. Immunol. 2022, 13, 886562. [Google Scholar] [CrossRef] [PubMed]
- Mold, J.E.; Michaelsson, J.; Burt, T.D.; Muench, M.O.; Beckerman, K.P.; Busch, M.P.; Lee, T.H.; Nixon, D.F.; McCune, J.M. Maternal alloantigens promote the development of tolerogenic fetal regulatory T cells in utero. Science 2008, 322, 1562–1565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kollmann, T.R.; Crabtree, J.; Rein-Weston, A.; Blimkie, D.; Thommai, F.; Wang, X.Y.; Lavoie, P.M.; Furlong, J.; Fortuno, E.S., 3rd; Hajjar, A.M.; et al. Neonatal innate TLR-mediated responses are distinct from those of adults. J. Immunol. 2009, 183, 7150–7160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berendam, S.J.; Nelson, A.N.; Goswami, R.; Persaud, D.; Haigwood, N.L.; Chahroudi, A.; Fouda, G.G.; Permar, S.R. Pediatric HIV: The Potential of Immune Therapeutics to Achieve Viral Remission and Functional Cure. Curr. HIV/AIDS Rep. 2020, 17, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Violari, A.; Cotton, M.F.; Gibb, D.M.; Babiker, A.G.; Steyn, J.; Madhi, S.A.; Jean-Philippe, P.; McIntyre, J.A. Early Antiretroviral Therapy and Mortality among HIV-Infected Infants. N. Engl. J. Med. 2008, 359, 2233–2244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uprety, P.; Patel, K.; Karalius, B.; Ziemniak, C.; Chen, Y.H.; Brummel, S.S.; Siminski, S.; Van Dyke, R.B.; Seage, G.R.; Persaud, D.; et al. Human Immunodeficiency Virus Type 1 DNA Decay Dynamics with Early, Long-term Virologic Control of Perinatal Infection. Clin. Infect. Dis. 2017, 64, 1471–1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maldarelli, F.; Wu, X.; Su, L.; Simonetti, F.R.; Shao, W.; Hill, S.; Spindler, J.; Ferris, A.L.; Mellors, J.W.; Kearney, M.F.; et al. HIV latency. Specific HIV integration sites are linked to clonal expansion and persistence of infected cells. Science 2014, 345, 179–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maldarelli, F. HIV-infected cells are frequently clonally expanded after prolonged antiretroviral therapy: Implications for HIV persistence. J. Virus Erad. 2015, 1, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Wagner, T.A.; McLaughlin, S.; Garg, K.; Cheung, C.Y.; Larsen, B.B.; Styrchak, S.; Huang, H.C.; Edlefsen, P.T.; Mullins, J.I.; Frenkel, L.M. HIV latency. Proliferation of cells with HIV integrated into cancer genes contributes to persistent infection. Science 2014, 345, 570–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bui, J.K.; Sobolewski, M.D.; Keele, B.F.; Spindler, J.; Musick, A.; Wiegand, A.; Luke, B.T.; Shao, W.; Hughes, S.H.; Coffin, J.M.; et al. Proviruses with identical sequences comprise a large fraction of the replication-competent HIV reservoir. PLoS Pathog. 2017, 13, e1006283. [Google Scholar] [CrossRef] [PubMed]
- Bale, M.J.; Katusiime, M.G.; Wells, D.; Wu, X.; Spindler, J.; Halvas, E.K.; Cyktor, J.C.; Wiegand, A.; Shao, W.; Cotton, M.F.; et al. Early Emergence and Long-Term Persistence of HIV-Infected T-Cell Clones in Children. mBio 2021, 12, e00568-21. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.Q.; Orlova-Fink, N.; Einkauf, K.; Chowdhury, F.Z.; Sun, X.; Harrington, S.; Kuo, H.-H.; Hua, S.; Chen, H.-R.; Ouyang, Z.; et al. Clonal expansion of genome-intact HIV-1 in functionally polarized Th1 CD4+ T cells. J. Clin. Investig. 2017, 127, 2689–2696. [Google Scholar] [CrossRef] [PubMed]
- Simonetti, F.R.; Zhang, H.; Soroosh, G.P.; Duan, J.; Rhodehouse, K.; Hill, A.L.; Beg, S.A.; McCormick, K.; Raymond, H.E.; Nobles, C.L.; et al. Antigen-driven clonal selection shapes the persistence of HIV-1-infected CD4+ T cells in vivo. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef] [PubMed]
- Katlama, C.; Lambert-Niclot, S.; Assoumou, L.; Papagno, L.; Lecardonnel, F.; Zoorob, R.; Tambussi, G.; Clotet, B.; Youle, M.; Achenbach, C.J.; et al. Treatment intensification followed by interleukin-7 reactivates HIV without reducing total HIV DNA: A randomized trial. AIDS 2016, 30, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Vandergeeten, C.; Fromentin, R.; DaFonseca, S.; Lawani, M.B.; Sereti, I.; Lederman, M.M.; Ramgopal, M.; Routy, J.P.; Sekaly, R.P.; Chomont, N. Interleukin-7 promotes HIV persistence during antiretroviral therapy. Blood 2013, 121, 4321–4329. [Google Scholar] [CrossRef]
- Purton, J.F.; Tan, J.T.; Rubinstein, M.P.; Kim, D.M.; Sprent, J.; Surh, C.D. Antiviral CD4+ memory T cells are IL-15 dependent. J. Exp. Med. 2007, 204, 951–961. [Google Scholar] [CrossRef]
- Bosque, A.; Famiglietti, M.; Weyrich, A.S.; Goulston, C.; Planelles, V. Homeostatic proliferation fails to efficiently reactivate HIV-1 latently infected central memory CD4+ T cells. PLoS Pathog. 2011, 7, e1002288. [Google Scholar] [CrossRef] [Green Version]
- Chomont, N.; El-Far, M.; Ancuta, P.; Trautmann, L.; Procopio, F.A.; Yassine-Diab, B.; Boucher, G.; Boulassel, M.R.; Ghattas, G.; Brenchley, J.M.; et al. HIV reservoir size and persistence are driven by T cell survival and homeostatic proliferation. Nat. Med. 2009, 15, 893–900. [Google Scholar] [CrossRef]
- Schroder, A.R.; Shinn, P.; Chen, H.; Berry, C.; Ecker, J.R.; Bushman, F. HIV-1 integration in the human genome favors active genes and local hotspots. Cell 2002, 110, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.; Lassen, K.; Monie, D.; Sedaghat, A.R.; Shimoji, S.; Liu, X.; Pierson, T.C.; Margolick, J.B.; Siliciano, R.F.; Siliciano, J.D. Resting CD4+ T cells from human immunodeficiency virus type 1 (HIV-1)-infected individuals carry integrated HIV-1 genomes within actively transcribed host genes. J. Virol. 2004, 78, 6122–6133. [Google Scholar] [CrossRef]
- Einkauf, K.B.; Lee, G.Q.; Gao, C.; Sharaf, R.; Sun, X.; Hua, S.; Chen, S.M.; Jiang, C.; Lian, X.; Chowdhury, F.Z.; et al. Intact HIV-1 proviruses accumulate at distinct chromosomal positions during prolonged antiretroviral therapy. J. Clin. Investig. 2019, 129, 988–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- TAG. Research toward a Cure Trials. Available online: https://www.treatmentactiongroup.org/cure/trials/ (accessed on 15 June 2022).
- WHO. Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring: Recommendations for a Public Health Approach. Available online: https://www.who.int/publications/i/item/9789240031593 (accessed on 15 June 2022).
- Panel on Antiretroviral Therapy and Medical Management of Children Living with HIV. Guidelines for the Use of Antiretroviral Agents in Pediatric HIV Infection. Available online: https://clinicalinfo.hiv.gov/en/guidelines/pediatric-arv (accessed on 15 June 2022).
- Iyun, V.; Technau, K.-G.; Eley, B.; Rabie, H.; Boulle, A.; Fatti, G.; Egger, M.; Tanser, F.; Wood, R.; Fairlie, L.; et al. Earlier Antiretroviral Therapy Initiation and Decreasing Mortality Among HIV-infected Infants Initiating Antiretroviral Therapy Within 3 Months of Age in South Africa, 2006–2017. Pediatric Infect. Dis. J. 2020, 39, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Shiau, S.; Arpadi, S.; Strehlau, R.; Martens, L.; Patel, F.; Coovadia, A.; Abrams, E.J.; Kuhn, L. Initiation of antiretroviral therapy before 6 months of age is associated with faster growth recovery in South African children perinatally infected with human immunodeficiency virus. J. Pediatr. 2013, 162, 1138–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luzuriaga, K.; Tabak, B.; Garber, M.; Chen, Y.H.; Ziemniak, C.; McManus, M.M.; Murray, D.; Strain, M.C.; Richman, D.D.; Chun, T.W.; et al. HIV type 1 (HIV-1) proviral reservoirs decay continuously under sustained virologic control in HIV-1-infected children who received early treatment. J. Infect. Dis. 2014, 210, 1529–1538. [Google Scholar] [CrossRef] [PubMed]
- Persaud, D.; Patel, K.; Karalius, B.; Rainwater-Lovett, K.; Ziemniak, C.; Ellis, A.; Chen, Y.H.; Richman, D.; Siberry, G.K.; Van Dyke, R.B.; et al. Influence of age at virologic control on peripheral blood human immunodeficiency virus reservoir size and serostatus in perinatally infected adolescents. JAMA Pediatr. 2014, 168, 1138–1146. [Google Scholar] [CrossRef] [Green Version]
- Rainwater-Lovett, K.; Ziemniak, C.; Watson, D.; Luzuriaga, K.; Siberry, G.; Petru, A.; Chen, Y.; Uprety, P.; McManus, M.; Ho, Y.C.; et al. Paucity of Intact Non-Induced Provirus with Early, Long-Term Antiretroviral Therapy of Perinatal HIV Infection. PLoS ONE 2017, 12, e0170548. [Google Scholar] [CrossRef] [Green Version]
- Bitnun, A.; Samson, L.; Chun, T.W.; Kakkar, F.; Brophy, J.; Murray, D.; Justement, S.; Soudeyns, H.; Ostrowski, M.; Mujib, S.; et al. Early initiation of combination antiretroviral therapy in HIV-1-infected newborns can achieve sustained virologic suppression with low frequency of CD4+ T cells carrying HIV in peripheral blood. Clin. Infect. Dis. 2014, 59, 1012–1019. [Google Scholar] [CrossRef] [Green Version]
- Ananworanich, J.; Puthanakit, T.; Suntarattiwong, P.; Chokephaibulkit, K.; Kerr, S.J.; Fromentin, R.; Bakeman, W.; Intasan, J.; Mahanontharit, A.; Sirivichayakul, S.; et al. Reduced markers of HIV persistence and restricted HIV-specific immune responses after early antiretroviral therapy in children. AIDS 2014, 28, 1015–1020. [Google Scholar] [CrossRef]
- Martínez-Bonet, M.; Puertas, M.C.; Fortuny, C.; Ouchi, D.; Mellado, M.J.; Rojo, P.; Noguera-Julian, A.; Muñoz-Fernández, M.A.; Martinez-Picado, J. Establishment and Replenishment of the Viral Reservoir in Perinatally HIV-1-infected Children Initiating Very Early Antiretroviral Therapy. Clin. Infect. Dis. 2015, 61, 1169–1178. [Google Scholar] [CrossRef] [Green Version]
- Katusiime, M.G.; Halvas, E.K.; Wright, I.; Joseph, K.; Bale, M.J.; Kirby-McCullough, B.; Engelbrecht, S.; Shao, W.; Hu, W.S.; Cotton, M.F.; et al. Intact HIV Proviruses Persist in Children Seven to Nine Years after Initiation of Antiretroviral Therapy in the First Year of Life. J. Virol. 2020, 94, e01519-19. [Google Scholar] [CrossRef]
- van Zyl, G.U.; Bedison, M.A.; van Rensburg, A.J.; Laughton, B.; Cotton, M.F.; Mellors, J.W. Early Antiretroviral Therapy in South African Children Reduces HIV-1-Infected Cells and Cell-Associated HIV-1 RNA in Blood Mononuclear Cells. J. Infect. Dis. 2015, 212, 39–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veldsman, K.A.; Janse van Rensburg, A.; Isaacs, S.; Naidoo, S.; Laughton, B.; Lombard, C.; Cotton, M.F.; Mellors, J.W.; van Zyl, G.U. HIV-1 DNA decay is faster in children who initiate ART shortly after birth than later. J. Int. AIDS Soc. 2019, 22, e25368. [Google Scholar] [CrossRef] [PubMed]
- McManus, M.; Mick, E.; Hudson, R.; Mofenson, L.M.; Sullivan, J.L.; Somasundaran, M.; Luzuriaga, K.; Investigators, P. Early Combination Antiretroviral Therapy Limits Exposure to HIV-1 Replication and Cell-Associated HIV-1 DNA Levels in Infants. PLoS ONE 2016, 11, e0154391. [Google Scholar] [CrossRef] [Green Version]
- Tagarro, A.; Chan, M.; Zangari, P.; Ferns, B.; Foster, C.; De Rossi, A.; Nastouli, E.; Munoz-Fernandez, M.A.; Gibb, D.; Rossi, P.; et al. Early and Highly Suppressive Antiretroviral Therapy Are Main Factors Associated With Low Viral Reservoir in European Perinatally HIV-Infected Children. J. Acquir. Immune Defic. Syndr. 2018, 79, 269–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dominguez-Rodriguez, S.; Tagarro, A.; Palma, P.; Foster, C.; Puthanakit, T.; Jupimai, T.; Cotugno, N.; Ananworanich, J.; Zangari, P.; Nastouli, E.; et al. Reduced Time to Suppression among Neonates with HIV Initiating Antiretroviral Therapy within 7 Days After Birth. J. Acquir. Immune Defic. Syndr. 2019, 82, 483–490. [Google Scholar] [CrossRef]
- Massanella, M.; Puthanakit, T.; Leyre, L.; Jupimai, T.; Sawangsinth, P.; de Souza, M.; Suntarattiwong, P.; Kosalarksa, P.; Borkird, T.; Kanjanavanit, S.; et al. Continuous Prophylactic Antiretrovirals/Antiretroviral Therapy Since Birth Reduces Seeding and Persistence of the Viral Reservoir in Children Vertically Infected With Human Immunodeficiency Virus. Clin. Infect. Dis. 2021, 73, 427–438. [Google Scholar] [CrossRef]
- Giacomet, V.; Trabattoni, D.; Zanchetta, N.; Biasin, M.; Gismondo, M.; Clerici, M.; Zuccotti, G. No cure of HIV infection in a child despite early treatment and apparent viral clearance. Lancet 2014, 384, 1320. [Google Scholar] [CrossRef]
- Butler, K.M.; Gavin, P.; Coughlan, S.; Rochford, A.; Mc Donagh, S.; Cunningham, O.; Poulsom, H.; Watters, S.A.; Klein, N. Rapid viral rebound after 4 years of suppressive therapy in a seronegative HIV-1 infected infant treated from birth. Pediatr. Infect. Dis. J. 2015, 34, e48–e51. [Google Scholar] [CrossRef]
- Capparelli, E.V.; Ajibola, G.; Maswabi, K.; Holme, M.P.; Bennett, K.; Powis, K.M.; Moyo, S.; Mohammed, T.; Maphorisa, C.; Hughes, M.D.; et al. Safety and Pharmacokinetics of Intravenous 10-1074 and VRC01LS in Young Children. J. Acquir. Immune Defic. Syndr. 2022, 91, 182–188. [Google Scholar] [CrossRef]
- Roger, L.; Shapiro, K.M.; Ajibola, G.; Hughes, M.; Holme, M.P.; Powis, K.M.; Moyo, S.; Nelson, B.S.; Caskey, M.; Gama, L.; et al. Treatment with Broadly Neutralizing Antibodies in Children with HIV in Botswana. In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Denver, CO, USA, 14 February 2022. [Google Scholar]
- Burton, D.R.; Hangartner, L. Broadly Neutralizing Antibodies to HIV and Their Role in Vaccine Design. Annu. Rev. Immunol. 2016, 34, 635–659. [Google Scholar] [CrossRef]
- Flint, S.J.; Racaniello, V.R.; Rall, G.F.; Hatziioannou, T.; Skalka, A.M. Principles of Virology, Volume 2: Pathogenesis and Control; John Wiley & Sons: New York, NY, USA, 2015. [Google Scholar]
- Crowell, T.A.; Colby, D.J.; Pinyakorn, S.; Sacdalan, C.; Pagliuzza, A.; Intasan, J.; Benjapornpong, K.; Tangnaree, K.; Chomchey, N.; Kroon, E.; et al. Safety and efficacy of VRC01 broadly neutralising antibodies in adults with acutely treated HIV (RV397): A phase 2, randomised, double-blind, placebo-controlled trial. Lancet HIV 2019, 6, e297–e306. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Cao, W.; Sun, M.; Li, T. Broadly neutralizing antibodies for HIV-1: Efficacies, challenges and opportunities. Emerg. Microbes Infect. 2020, 9, 194–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaebler, C.; Nogueira, L.; Stoffel, E.; Oliveira, T.Y.; Breton, G.L.; Millard, K.G.; Turroja, M.; Butler, A.; Ramos, V.; Seaman, M.S.; et al. Prolonged viral suppression with anti-HIV-1 antibody therapy. Nature 2022, 606, 368–374. [Google Scholar] [CrossRef]
- Casazza, J.P.; Cale, E.M.; Narpala, S.; Yamshchikov, G.V.; Coates, E.E.; Hendel, C.S.; Novik, L.; Holman, L.A.; Widge, A.T.; Apte, P.; et al. Safety and tolerability of AAV8 delivery of a broadly neutralizing antibody in adults living with HIV: A phase 1, dose-escalation trial. Nature Med. 2022, 28, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Gardner, M.R. Promise and Progress of an HIV-1 Cure by Adeno-Associated Virus Vector Delivery of Anti-HIV-1 Biologics. Front. Cell Infect. Microbiol. 2020, 10, 176. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, C.K.; McFarland, E.J.; Morrison, R.L.; Capparelli, E.V.; Safrit, J.T.; Mofenson, L.M.; Mathieson, B.; Valentine, M.E.; Perlowski, C.; Smith, B.; et al. Safety, Tolerability, and Pharmacokinetics of the Broadly Neutralizing Human Immunodeficiency Virus (HIV)-1 Monoclonal Antibody VRC01 in HIV-Exposed Newborn Infants. J. Infect. Dis. 2020, 222, 628–636. [Google Scholar] [CrossRef] [Green Version]
- Deeks, S.G. HIV: Shock and kill. Nature 2012, 487, 439–440. [Google Scholar] [CrossRef]
- Gunst, J.D.; Pahus, M.H.; Rosás-Umbert, M.; Benfield, T.; Nielsen, H.; Johansen, I.S.; Mohey, R.; Østergaard, L.H.; Schleimann, M. The Impact of 3BNC117 and Romidepsin Treatment at ART Initiation on HIV-1 Persistence. In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Denver, CO, USA, 15 February 2022. [Google Scholar]
- Elliott, J.H.; Wightman, F.; Solomon, A.; Ghneim, K.; Ahlers, J.; Cameron, M.J.; Smith, M.Z.; Spelman, T.; Mcmahon, J.; Velayudham, P.; et al. Activation of HIV Transcription with Short-Course Vorinostat in HIV-Infected Patients on Suppressive Antiretroviral Therapy. PLoS Pathog. 2014, 10, e1004473. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Ma, J.; Kang, W.; Wang, C.; Bai, F.; Zhao, K.; Yao, N.; Liu, Q.; Dang, B.; Wang, B.; et al. The histone deacetylase inhibitor chidamide induces intermittent viraemia in HIV-infected patients on suppressive antiretroviral therapy. HIV Med. 2020, 21, 747–757. [Google Scholar] [CrossRef]
- Rasmussen, T.A.; Tolstrup, M.; Brinkmann, C.R.; Olesen, R.; Erikstrup, C.; Solomon, A.; Winckelmann, A.; Palmer, S.; Dinarello, C.; Buzon, M.; et al. Panobinostat, a histone deacetylase inhibitor, for latent-virus reactivation in HIV-infected patients on suppressive antiretroviral therapy: A phase 1/2, single group, clinical trial—The Lancet HIV. Lancet HIV 2022, 1, E13–E21. [Google Scholar] [CrossRef]
- Curty, G.; Iniguez, L.P.; Soares, M.A.; Nixon, D.F.; de Mulder Rougvie, M. Off-Target Effect of Activation of NF-kappaB by HIV Latency Reversal Agents on Transposable Elements Expression. Viruses 2022, 14, 1571. [Google Scholar] [CrossRef] [PubMed]
- Sarabia, I.; Huang, S.H.; Ward, A.R.; Jones, R.B.; Bosque, A. The Intact Noninducible Latent HIV-1 Reservoir Is Established in an In Vitro Primary T-CM Cell Model of Latency. J. Virol. 2021, 95, e01297-20. [Google Scholar] [CrossRef] [PubMed]
- Vansant, G.; Bruggemans, A.; Janssens, J.; Debyser, Z. Block-And-Lock Strategies to Cure HIV Infection. Viruses 2020, 12, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, A.P. The HIV-1 Tat Protein: Mechanism of Action and Target for HIV-1 Cure Strategies. Curr. Pharm. Des. 2017, 23, 4098–4102. [Google Scholar] [CrossRef] [Green Version]
- Zhou, C.; Rana, T.M. A bimolecular mechanism of HIV-1 Tat protein interaction with RNA polymerase II transcription elongation complexes. J. Mol. Biol. 2002, 320, 925–942. [Google Scholar] [CrossRef]
- Selby, M.J.; Bain, E.S.; Luciw, P.A.; Peterlin, B.M. Structure, sequence, and position of the stem-loop in tar determine transcriptional elongation by tat through the HIV-1 long terminal repeat. Genes Dev. 1989, 3, 547–558. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, T.; Wong-Staal, F. Demonstration of virus-specific transcriptional activator(s) in cells infected with HTLV-III by an in vitro cell-free system. Cell 1986, 47, 29–35. [Google Scholar] [CrossRef]
- Budhiraja, S.; Famiglietti, M.; Bosque, A.; Planelles, V.; Rice, A.P. Cyclin T1 and CDK9 T-loop phosphorylation are downregulated during establishment of HIV-1 latency in primary resting memory CD4+ T cells. J. Virol. 2013, 87, 1211–1220. [Google Scholar] [CrossRef] [Green Version]
- Tyagi, M.; Pearson, R.J.; Karn, J. Establishment of HIV latency in primary CD4+ cells is due to epigenetic transcriptional silencing and P-TEFb restriction. J. Virol. 2010, 84, 6425–6437. [Google Scholar] [CrossRef] [Green Version]
- Mousseau, G.; Clementz, M.A.; Bakeman, W.N.; Nagarsheth, N.; Cameron, M.; Shi, J.; Baran, P.; Fromentin, R.; Chomont, N.; Valente, S.T. An analog of the natural steroidal alkaloid cortistatin A potently suppresses Tat-dependent HIV transcription. Cell Host Microbe 2012, 12, 97–108. [Google Scholar] [CrossRef]
- Bovolenta, C.; Camorali, L.; Lorini, A.L.; Ghezzi, S.; Vicenzi, E.; Lazzarin, A.; Poli, G. Constitutive activation of STATs upon in vivo human immunodeficiency virus infection. Blood 1999, 94, 4202–4209. [Google Scholar] [CrossRef]
- Rivera-Rivera, L.; Perez-Laspiur, J.; Colon, K.; Melendez, L.M. Inhibition of interferon response by cystatin B: Implication in HIV replication of macrophage reservoirs. J. Neurovirol. 2012, 18, 20–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohler, J.J.; Tuttle, D.L.; Coberley, C.R.; Sleasman, J.W.; Goodenow, M.M. Human immunodeficiency virus type 1 (HIV-1) induces activation of multiple STATs in CD4+ cells of lymphocyte or monocyte/macrophage lineages. J. Leukoc. Biol. 2003, 73, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, A.; Yang, B.; Gendelman, H.E.; Persidsky, Y.; Kanmogne, G.D. STAT1 signaling modulates HIV-1-induced inflammatory responses and leukocyte transmigration across the blood-brain barrier. Blood 2008, 111, 2062–2072. [Google Scholar] [CrossRef] [PubMed]
- Gavegnano, C.; Detorio, M.; Montero, C.; Bosque, A.; Planelles, V.; Schinazi, R.F. Ruxolitinib and tofacitinib are potent and selective inhibitors of HIV-1 replication and virus reactivation in vitro. Antimicrob. Agents Chemother. 2014, 58, 1977–1986. [Google Scholar] [CrossRef] [Green Version]
- Marconi, V.C.; Moser, C.; Gavegnano, C.; Deeks, S.G.; Lederman, M.M.; Overton, E.T.; Tsibris, A.; Hunt, P.W.; Kantor, A.; Sekaly, R.P.; et al. Randomized Trial of Ruxolitinib in Antiretroviral-Treated Adults With Human Immunodeficiency Virus. Clin. Infect. Dis. 2022, 74, 95–104. [Google Scholar] [CrossRef]
- Timmons, A.; Fray, E.; Kumar, M.; Wu, F.T.; Dai, W.W.; Bullen, C.K.; Kim, P.; Hetzel, C.; Yang, C.; Beg, S.; et al. HSF1 inhibition attenuates HIV-1 latency reversal mediated by several candidate LRAs In Vitro and Ex Vivo. Proc. Natl. Acad. Sci. USA 2020, 117, 15763–15771. [Google Scholar] [CrossRef]
- Boukli, N.M.; Shetty, V.; Cubano, L.; Ricaurte, M.; Coelho-Dos-Reis, J.; Nickens, Z.; Shah, P.; Talal, A.H.; Philip, R.; Jain, P. Unique and differential protein signatures within the mononuclear cells of HIV-1 and HCV mono-infected and co-infected patients. Clin. Proteom. 2012, 9, 11. [Google Scholar] [CrossRef] [Green Version]
- Vahabpour, R.; Soleymani, S.; Roohvand, F.; Zabihollahi, R.; Bolhassani, A. In Vitro Anti-Viral Effects of Small Heat Shock Proteins 20 and 27: A Novel Therapeutic Approach. Curr. Pharm. Biotechnol. 2019, 20, 1011–1017. [Google Scholar] [CrossRef]
- Peng, W.; Hong, Z.; Chen, X.; Gao, H.; Dai, Z.; Zhao, J.; Liu, W.; Li, D.; Deng, K. Thiostrepton Reactivates Latent HIV-1 through the p-TEFb and NF-κB Pathways Mediated by Heat Shock Response. Antimicrob. Agents Chemother. 2020, 64, e02328-19. [Google Scholar] [CrossRef]
- Anderson, I.; Low, J.S.; Weston, S.; Weinberger, M.; Zhyvoloup, A.; Labokha, A.A.; Corazza, G.; Kitson, R.A.; Moody, C.J.; Marcello, A.; et al. Heat shock protein 90 controls HIV-1 reactivation from latency. Proc Natl Acad Sci USA 2014, 111, E1528–E1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besnard, E.; Hakre, S.; Kampmann, M.; Lim, H.W.; Hosmane, N.N.; Martin, A.; Bassik, M.C.; Verschueren, E.; Battivelli, E.; Chan, J.; et al. The mTOR Complex Controls HIV Latency. Cell Host Microbe 2016, 20, 785–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henrich, T.J.; Schreiner, C.; Cameron, C.; Hogan, L.E.; Richardson, B.; Rutishauser, R.L.; Deitchman, A.N.; Chu, S.; Rogers, R.; Thanh, C.; et al. Everolimus, an mTORC1/2 inhibitor, in ART-suppressed individuals who received solid organ transplantation: A prospective study. Am. J. Transplant. 2021, 21, 1765–1779. [Google Scholar] [CrossRef] [PubMed]
- Meier, A.; Bagchi, A.; Sidhu, H.K.; Alter, G.; Suscovich, T.J.; Kavanagh, D.G.; Streeck, H.; Brockman, M.A.; LeGall, S.; Hellman, J.; et al. Upregulation of PD-L1 on monocytes and dendritic cells by HIV-1 derived TLR ligands. AIDS 2008, 22, 655–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Garcia, M.; Porichis, F.; de Jong, O.G.; Levi, K.; Diefenbach, T.J.; Lifson, J.D.; Freeman, G.J.; Walker, B.D.; Kaufmann, D.E.; Kavanagh, D.G. Expression of PD-L1 and PD-L2 on human macrophages is up-regulated by HIV-1 and differentially modulated by IL-10. J. Leukoc. Biol. 2011, 89, 507–515. [Google Scholar] [CrossRef] [Green Version]
- Fromentin, R.; DaFonseca, S.; Costiniuk, C.T.; El-Far, M.; Procopio, F.A.; Hecht, F.M.; Hoh, R.; Deeks, S.G.; Hazuda, D.J.; Lewin, S.R.; et al. PD-1 blockade potentiates HIV latency reversal ex vivo in CD4(+) T cells from ART-suppressed individuals. Nat. Commun. 2019, 10, 814. [Google Scholar] [CrossRef] [Green Version]
- Evans, V.A.; van der Sluis, R.M.; Solomon, A.; Dantanarayana, A.; McNeil, C.; Garsia, R.; Palmer, S.; Fromentin, R.; Chomont, N.; Sékaly, R.P.; et al. Programmed cell death-1 contributes to the establishment and maintenance of HIV-1 latency. AIDS 2018, 32, 1491–1497. [Google Scholar] [CrossRef]
- Dai, B.; Xiao, L.; Bryson, P.D.; Fang, J.; Wang, P. PD-1/PD-L1 blockade can enhance HIV-1 Gag-specific T cell immunity elicited by dendritic cell-directed lentiviral vaccines. Mol. Ther. 2012, 20, 1800–1809. [Google Scholar] [CrossRef] [Green Version]
- Kawai, T.; Akira, S. Signaling to NF-kappaB by Toll-like receptors. Trends Mol. Med. 2007, 13, 460–469. [Google Scholar] [CrossRef]
- Martinsen, J.T.; Gunst, J.D.; Højen, J.F.; Tolstrup, M.; Søgaard, O.S. The Use of Toll-Like Receptor Agonists in HIV-1 Cure Strategies. Front. Immunol. 2020, 11, 1112. [Google Scholar] [CrossRef]
- Thibault, S.; Imbeault, M.; Tardif, M.R.; Tremblay, M.J. TLR5 stimulation is sufficient to trigger reactivation of latent HIV-1 provirus in T lymphoid cells and activate virus gene expression in central memory CD4+ T cells. Virology 2009, 389, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Novis, C.L.; Archin, N.M.; Buzon, M.J.; Verdin, E.; Round, J.L.; Lichterfeld, M.; Margolis, D.M.; Planelles, V.; Bosque, A. Reactivation of latent HIV-1 in central memory CD4(+) T cells through TLR-1/2 stimulation. Retrovirology 2013, 10, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Offersen, R.; Nissen, S.K.; Rasmussen, T.A.; Ostergaard, L.; Denton, P.W.; Sogaard, O.S.; Tolstrup, M. A Novel Toll-Like Receptor 9 Agonist, MGN1703, Enhances HIV-1 Transcription and NK Cell-Mediated Inhibition of HIV-1-Infected Autologous CD4+ T Cells. J. Virol. 2016, 90, 4441–4453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, A.; Irrinki, A.; Kaur, J.; Cihlar, T.; Kukolj, G.; Sloan, D.D.; Murry, J.P. Toll-Like Receptor 7 Agonist GS-9620 Induces HIV Expression and HIV-Specific Immunity in Cells from HIV-Infected Individuals on Suppressive Antiretroviral Therapy. J. Virol. 2017, 91, e02166-16. [Google Scholar] [CrossRef] [Green Version]
- Riddler, S.A.; Para, M.; Benson, C.A.; Mills, A.; Ramgopal, M.; Dejesus, E.; Brinson, C.; Cyktor, J.; Jacobs, J.; Koontz, D.; et al. Vesatolimod, a Toll-like Receptor 7 Agonist, Induces Immune Activation in Virally Suppressed Adults Living With Human Immunodeficiency Virus–1. Clin. Infect. Dis. 2021, 72, e815–e824. [Google Scholar] [CrossRef]
- Moldt, B.; Chandrashekar, A.; Borducchi, E.N.; Nkolola, J.P.; Stephenson, H.; Nagel, M.; Hung, M.; Goldsmith, J.; Pace, C.S.; Carr, B.; et al. HIV envelope antibodies and TLR7 agonist partially prevent viral rebound in chronically SHIV-infected monkeys. PLOS Pathog. 2022, 18, e1010467. [Google Scholar] [CrossRef]
- Nixon, C.C.; Mavigner, M.; Sampey, G.C.; Brooks, A.D.; Spagnuolo, R.A.; Irlbeck, D.M.; Mattingly, C.; Ho, P.T.; Schoof, N.; Cammon, C.G.; et al. Systemic HIV and SIV latency reversal via non-canonical NF-kappaB signalling in vivo. Nature 2020, 578, 160–165. [Google Scholar] [CrossRef]
- Fulda, S. Molecular pathways: Targeting death receptors and smac mimetics. Clin. Cancer Res. 2014, 20, 3915–3920. [Google Scholar] [CrossRef] [Green Version]
- Mavigner, M.; Liao, L.E.; Brooks, A.D.; Ke, R.; Mattingly, C.; Schoof, N.; McBrien, J.; Carnathan, D.; Liang, S.; Vanderford, T.H.; et al. CD8 lymphocyte depletion enhances the latency reversal activity of the SMAC mimetic AZD5582 in ART-suppressed SIV-infected rhesus macaques. J. Virol. 2021, 95, e01429-20. [Google Scholar] [CrossRef]
- Bricker, K.M.; Obregon-Perko, V.; Williams, B.; Oliver, D.; Uddin, F.; Neja, M.; Hopkins, L.; Dashti, A.; Jean, S.; Wood, J.S.; et al. Altered Response Pattern following AZD5582 Treatment of SIV-Infected, ART-Suppressed Rhesus Macaque Infants. J. Virol. 2022, 96, e0169921. [Google Scholar] [CrossRef]
- Hosseinipour, M.C.; Innes, C.; Naidoo, S.; Mann, P.; Hutter, J.; Ramjee, G.; Sebe, M.; Maganga, L.; Herce, M.E.; deCamp, A.C.; et al. Phase 1 Human Immunodeficiency Virus (HIV) Vaccine Trial to Evaluate the Safety and Immunogenicity of HIV Subtype C DNA and MF59-Adjuvanted Subtype C Envelope Protein. Clin. Infect. Dis. 2021, 72, 50–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenough, T.C.; Cunningham, C.K.; Muresan, P.; McManus, M.; Persaud, D.; Fenton, T.; Barker, P.; Gaur, A.; Panicali, D.; Sullivan, J.L.; et al. Safety and immunogenicity of recombinant poxvirus HIV-1 vaccines in young adults on highly active antiretroviral therapy. Vaccine 2008, 26, 6883–6893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Persaud, D.; Luzuriaga, K.; Ziemniak, C.; Muresan, P.; Greenough, T.; Fenton, T.; Blackford, A.; Ferguson, K.; Neu, N.; Cunningham, C.K. Effect of therapeutic HIV recombinant poxvirus vaccines on the size of the resting CD4+ T-cell latent HIV reservoir. AIDS 2011, 25, 2227–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiu, C.; Cunningham, C.K.; Greenough, T.; Muresan, P.; Sanchez-Merino, V.; Carey, V.; Jackson, J.B.; Ziemniak, C.; Fox, L.; Belzer, M.; et al. Identification of ongoing human immunodeficiency virus type 1 (HIV-1) replication in residual viremia during recombinant HIV-1 poxvirus immunizations in patients with clinically undetectable viral loads on durable suppressive highly active antiretroviral therapy. J. Virol. 2009, 83, 9731–9742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, J.; Wang, D.; Wang, S. The CCR5-Delta32 Genetic Polymorphism and HIV-1 Infection Susceptibility: A Meta-analysis. Open Med. 2018, 13, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Xun, J.; Zhang, X.; Guo, S.; Lu, H.; Chen, J. Editing out HIV: Application of gene editing technology to achieve functional cure. Retrovirology 2021, 18, 39. [Google Scholar] [CrossRef]
- Knipping, F.; Newby, G.A.; Eide, C.R.; McElroy, A.N.; Nielsen, S.C.; Smith, K.; Fang, Y.; Cornu, T.I.; Costa, C.; Gutierrez-Guerrero, A.; et al. Disruption of HIV-1 co-receptors CCR5 and CXCR4 in primary human T cells and hematopoietic stem and progenitor cells using base editing. Mol. Ther. 2022, 30, 130–144. [Google Scholar] [CrossRef]
- Bruner, K.M.; Hosmane, N.N.; Siliciano, R.F. Towards an HIV-1 cure: Measuring the latent reservoir. Trends Microbiol. 2015, 23, 192–203. [Google Scholar] [CrossRef] [Green Version]
- Siliciano, J.D.; Siliciano, R.F. Enhanced culture assay for detection and quantitation of latently infected, resting CD4+ T-cells carrying replication-competent virus in HIV-1-infected individuals. Methods Mol. Biol. 2005, 304, 3–15. [Google Scholar] [CrossRef]
- Eriksson, S.; Graf, E.H.; Dahl, V.; Strain, M.C.; Yukl, S.A.; Lysenko, E.S.; Bosch, R.J.; Lai, J.; Chioma, S.; Emad, F.; et al. Comparative analysis of measures of viral reservoirs in HIV-1 eradication studies. PLoS Pathog. 2013, 9, e1003174. [Google Scholar] [CrossRef]
- Procopio, F.A.; Fromentin, R.; Kulpa, D.A.; Brehm, J.H.; Bebin, A.G.; Strain, M.C.; Richman, D.D.; O’Doherty, U.; Palmer, S.; Hecht, F.M.; et al. A Novel Assay to Measure the Magnitude of the Inducible Viral Reservoir in HIV-infected Individuals. EBioMedicine 2015, 2, 874–883. [Google Scholar] [CrossRef] [Green Version]
- Dhummakupt, A.; Rubens, J.H.; Anderson, T.; Powell, L.; Nonyane, B.A.; Siems, L.V.; Collinson-Streng, A.; Nilles, T.; Jones, R.B.; Tepper, V.; et al. Differences in inducibility of the latent HIV reservoir in perinatal and adult infection. JCI Insight 2020, 5, e134105. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.; Ruggiero, A.; Paxton, W.A.; Pollakis, G. Measuring the Success of HIV-1 Cure Strategies. Front. Cell Infect. Microbiol. 2020, 10, 134. [Google Scholar] [CrossRef] [PubMed]
- Rouzioux, C.; Melard, A.; Avettand-Fenoel, V. Quantification of total HIV1-DNA in peripheral blood mononuclear cells. Methods Mol. Biol. 2014, 1087, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Brady, T.; Kelly, B.J.; Male, F.; Roth, S.; Bailey, A.; Malani, N.; Gijsbers, R.; O’Doherty, U.; Bushman, F.D. Quantitation of HIV DNA integration: Effects of differential integration site distributions on Alu-PCR assays. J. Virol. Methods 2013, 189, 53–57. [Google Scholar] [CrossRef] [Green Version]
- Liszewski, M.K.; Yu, J.J.; O’Doherty, U. Detecting HIV-1 integration by repetitive-sampling Alu-gag PCR. Methods 2009, 47, 254–260. [Google Scholar] [CrossRef] [Green Version]
- O’Doherty, U.; Swiggard, W.J.; Jeyakumar, D.; McGain, D.; Malim, M.H. A sensitive, quantitative assay for human immunodeficiency virus type 1 integration. J. Virol. 2002, 76, 10942–10950. [Google Scholar] [CrossRef] [Green Version]
- Strain, M.C.; Lada, S.M.; Luong, T.; Rought, S.E.; Gianella, S.; Terry, V.H.; Spina, C.A.; Woelk, C.H.; Richman, D.D. Highly precise measurement of HIV DNA by droplet digital PCR. PLoS ONE 2013, 8, e55943. [Google Scholar] [CrossRef]
- Bruner, K.M.; Wang, Z.; Simonetti, F.R.; Bender, A.M.; Kwon, K.J.; Sengupta, S.; Fray, E.J.; Beg, S.A.; Antar, A.A.R.; Jenike, K.M.; et al. A quantitative approach for measuring the reservoir of latent HIV-1 proviruses. Nature 2019, 566, 120–125. [Google Scholar] [CrossRef]
- Falcinelli, S.D.; Ceriani, C.; Margolis, D.M.; Archin, N.M. New Frontiers in Measuring and Characterizing the HIV Reservoir. Front. Microbiol. 2019, 10, 2878. [Google Scholar] [CrossRef]
- Gaebler, C.; Falcinelli, S.D.; Stoffel, E.; Read, J.; Murtagh, R.; Oliveira, T.Y.; Ramos, V.; Lorenzi, J.C.C.; Kirchherr, J.; James, K.S.; et al. Sequence Evaluation and Comparative Analysis of Novel Assays for Intact Proviral HIV-1 DNA. J. Virol. 2021, 95, e01986-20. [Google Scholar] [CrossRef] [PubMed]
- Gaebler, C.; Lorenzi, J.C.C.; Oliveira, T.Y.; Nogueira, L.; Ramos, V.; Lu, C.L.; Pai, J.A.; Mendoza, P.; Jankovic, M.; Caskey, M.; et al. Combination of quadruplex qPCR and next-generation sequencing for qualitative and quantitative analysis of the HIV-1 latent reservoir. J. Exp. Med. 2019, 216, 2253–2264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, J.A.; Kufera, J.T.; Bachmann, N.; Dai, W.; Simonetti, F.R.; Armstrong, C.; Lai, J.; Beg, S.; Siliciano, J.D.; Siliciano, R.F. Measuring the latent reservoir for HIV-1: Quantification bias in near full-length genome sequencing methods. PLoS Pathog. 2022, 18, e1010845. [Google Scholar] [CrossRef] [PubMed]
- Levy, C.N.; Hughes, S.M.; Roychoudhury, P.; Reeves, D.B.; Amstuz, C.; Zhu, H.; Huang, M.L.; Wei, Y.; Bull, M.E.; Cassidy, N.A.J.; et al. A highly multiplexed droplet digital PCR assay to measure the intact HIV-1 proviral reservoir. Cell Rep. Med. 2021, 2, 100243. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, N.A.J.; Fish, C.S.; Levy, C.N.; Roychoudhury, P.; Reeves, D.B.; Hughes, S.M.; Schiffer, J.T.; Benki-Nugent, S.; John-Stewart, G.; Wamalwa, D.; et al. HIV reservoir quantification using cross-subtype multiplex ddPCR. iScience 2022, 25, 103615. [Google Scholar] [CrossRef]
- Lee, G.Q.; Lichterfeld, M. Near-Full-Length Single-Genome HIV-1 DNA Sequencing. Methods Mol. Biol. 2022, 2407, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Patro, S.C.; Brandt, L.D.; Bale, M.J.; Halvas, E.K.; Joseph, K.W.; Shao, W.; Wu, X.; Guo, S.; Murrell, B.; Wiegand, A.; et al. Combined HIV-1 sequence and integration site analysis informs viral dynamics and allows reconstruction of replicating viral ancestors. Proc. Natl. Acad. Sci. USA 2019, 116, 25891–25899. [Google Scholar] [CrossRef]
- Einkauf, K.B.; Osborn, M.R.; Gao, C.; Sun, W.; Sun, X.; Lian, X.; Parsons, E.M.; Gladkov, G.T.; Seiger, K.W.; Blackmer, J.E.; et al. Parallel analysis of transcription, integration, and sequence of single HIV-1 proviruses. Cell 2022, 185, 266–282.e15. [Google Scholar] [CrossRef] [PubMed]
- Uprety, P.; Chadwick, E.G.; Rainwater-Lovett, K.; Ziemniak, C.; Luzuriaga, K.; Capparelli, E.V.; Yenokyan, G.; Persaud, D. Cell-Associated HIV-1 DNA and RNA Decay Dynamics during Early Combination Antiretroviral Therapy in HIV-1-Infected Infants. Clin. Infect. Dis. 2015, 61, 1862–1870. [Google Scholar] [CrossRef] [Green Version]
- Dhummakupt, A.; Siems, L.V.; Singh, D.; Chen, Y.H.; Anderson, T.; Collinson-Streng, A.; Zhang, H.; Patel, P.; Agwu, A.; Persaud, D. The Latent Human Immunodeficiency Virus (HIV) Reservoir Resides Primarily in CD32-CD4+ T Cells in Perinatally HIV-Infected Adolescents With Long-Term Virologic Suppression. J. Infect. Dis. 2019, 219, 80–88. [Google Scholar] [CrossRef]
- Persaud, D.; Palumbo, P.E.; Ziemniak, C.; Hughes, M.D.; Alvero, C.G.; Luzuriaga, K.; Yogev, R.; Capparelli, E.V.; Chadwick, E.G. Dynamics of the resting CD4(+) T-cell latent HIV reservoir in infants initiating HAART less than 6 months of age. AIDS 2012, 26, 1483–1490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Persaud, D.; Ray, S.C.; Kajdas, J.; Ahonkhai, A.; Siberry, G.K.; Ferguson, K.; Ziemniak, C.; Quinn, T.C.; Casazza, J.P.; Zeichner, S.; et al. Slow human immunodeficiency virus type 1 evolution in viral reservoirs in infants treated with effective antiretroviral therapy. AIDS Res. Hum. Retrovir. 2007, 23, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Brumme, Z.L.; Sudderuddin, H.; Ziemniak, C.; Luzuriaga, K.; Jones, B.R.; Joy, J.B.; Cunningham, C.K.; Greenough, T.; Persaud, D. Genetic complexity in the replication-competent latent HIV reservoir increases with untreated infection duration in infected youth. AIDS 2019, 33, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Bruner, K.M.; Murray, A.J.; Pollack, R.A.; Soliman, M.G.; Laskey, S.B.; Capoferri, A.A.; Lai, J.; Strain, M.C.; Lada, S.M.; Hoh, R.; et al. Defective proviruses rapidly accumulate during acute HIV-1 infection. Nat. Med. 2016, 22, 1043–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imamichi, H.; Dewar, R.L.; Adelsberger, J.W.; Rehm, C.A.; O’Doherty, U.; Paxinos, E.E.; Fauci, A.S.; Lane, H.C. Defective HIV-1 proviruses produce novel protein-coding RNA species in HIV-infected patients on combination antiretroviral therapy. Proc. Natl. Acad. Sci. USA 2016, 113, 8783–8788. [Google Scholar] [CrossRef] [Green Version]
- Zanchetta, M.; Walker, S.; Burighel, N.; Bellanova, D.; Rampon, O.; Giaquinto, C.; De Rossi, A. Long-term decay of the HIV-1 reservoir in HIV-1-infected children treated with highly active antiretroviral therapy. J. Infect. Dis. 2006, 193, 1718–1727. [Google Scholar] [CrossRef] [Green Version]
- Zanchetta, M.; Anselmi, A.; Vendrame, D.; Rampon, O.; Giaquinto, C.; Mazza, A.; Accapezzato, D.; Barnaba, V.; De Rossi, A. Early therapy in HIV-1-infected children: Effect on HIV-1 dynamics and HIV-1-specific immune response. Antivir. Ther. 2008, 13, 47–55. [Google Scholar] [CrossRef]
- Foster, C.; Dominguez-Rodriguez, S.; Tagarro, A.; Gkouleli, T.; Heaney, J.; Watters, S.; Bamford, A.; Fidler, K.; Navarro, M.; De Rossi, A.; et al. The CARMA Study: Early Infant Antiretroviral Therapy-Timing Impacts on Total HIV-1 DNA Quantitation 12 Years Later. J. Pediatric. Infect. Dis. Soc. 2021, 10, 295–301. [Google Scholar] [CrossRef]
- Frange, P.; Montange, T.; Le Chenadec, J.; Batalie, D.; Fert, I.; Dollfus, C.; Faye, A.; Blanche, S.; Chace, A.; Fourcade, C.; et al. Impact of Early Versus Late Antiretroviral Treatment Initiation on Naive T Lymphocytes in HIV-1-Infected Children and Adolescents—The-ANRS-EP59-CLEAC Study. Front. Immunol. 2021, 12, 662894. [Google Scholar] [CrossRef]
- Payne, H.; Chan, M.K.; Watters, S.A.; Otwombe, K.; Hsiao, N.Y.; Babiker, A.; Violari, A.; Cotton, M.F.; Gibb, D.M.; Klein, N.J. Early ART-initiation and longer ART duration reduces HIV-1 proviral DNA levels in children from the CHER trial. AIDS Res. Ther. 2021, 18, 63. [Google Scholar] [CrossRef]
- Luzuriaga, K.; Mofenson, L.M. Challenges in the Elimination of Pediatric HIV-1 Infection. N. Engl. J. Med. 2016, 374, 761–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Broncano, P.; Maddali, S.; Einkauf, K.B.; Jiang, C.; Gao, C.; Chevalier, J.; Chowdhury, F.Z.; Maswabi, K.; Ajibola, G.; Moyo, S.; et al. Early antiretroviral therapy in neonates with HIV-1 infection restricts viral reservoir size and induces a distinct innate immune profile. Sci. Transl. Med. 2019, 11, eaax7350. [Google Scholar] [CrossRef] [PubMed]
- Falcinelli, S.D.; Kilpatrick, K.W.; Read, J.; Murtagh, R.; Allard, B.; Ghofrani, S.; Kirchherr, J.; James, K.S.; Stuelke, E.; Baker, C.; et al. Longitudinal Dynamics of Intact HIV Proviral DNA and Outgrowth Virus Frequencies in a Cohort of Individuals Receiving Antiretroviral Therapy. J. Infect. Dis. 2021, 224, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Pardons, M.; Baxter, A.E.; Massanella, M.; Pagliuzza, A.; Fromentin, R.; Dufour, C.; Leyre, L.; Routy, J.P.; Kaufmann, D.E.; Chomont, N. Single-cell characterization and quantification of translation-competent viral reservoirs in treated and untreated HIV infection. PLoS Pathog. 2019, 15, e1007619. [Google Scholar] [CrossRef] [PubMed]
- Hiener, B.; Horsburgh, B.A.; Eden, J.-S.; Barton, K.; Schlub, T.E.; Lee, E.; Von Stockenstrom, S.; Odevall, L.; Milush, J.M.; Liegler, T.; et al. Identification of Genetically Intact HIV-1 Proviruses in Specific CD4 + T Cells from Effectively Treated Participants. Cell Rep. 2017, 21, 813–822. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Trial/Protocol Name | Trial Number | Age Range for Eligibility | Intervention | Country | Goal |
|---|---|---|---|---|---|
| IMPAACT 2008 | NCT03208231 | 0 to 12 weeks of age | Combination of Early ART and VRC01 | Botswana, Brazil, Malawi, Zimbabwe | Early clearance of HIV-1 infected cells in infancy |
| IMPAACT 2015 | NCT03416790 | 13 to 24 years of age | Long-term ART | United States | Central nervous system reservoir characterization |
| IMPAACT 2039 | In development | 3–12 years of age | HIVconsvX vaccines with/without triple bNAbs | To be determined | Safety, Immunogenicity efficacy of HIVconsX vaccines with/without bNABs to control viremia off ART |
| IMPAACT 2028 | NCT05154513 | 1 year and older | Follow up study of HIV persistence biomarkers in remission and cure trials (received Early or Very Early ART) | Botswana, Brazil, Haiti, Kenya, Malawi, South Africa, Tanzania, Thailand, Uganda, United States, Zimbabwe | Reservoir and immune biomarker profile following cure interventions |
| P1107 | NCT02140944 | 12 months and older | Cord blood transplantation with CCR5 delta 32 stem cells | United States | HIV cure |
| P1115 | NCT02140255 | Up to 10 days of life | Very early ART of neonates with/without BNABs | Argentina, Brazil, Haiti, Kenya, Malawi, Puerto Rico, South Africa, United States, Tanzania, Thailand, Uganda, Zambia, Zimbabwe | ART free remission |
| EIT (Early Infant HIV Treatment) | NCT02369406 | 0 to 56 days of life | Very Early ART | Botswana | ART free remission |
| LEOPARD (Latency and Early Neonatal Provision of Antiretroviral Drugs Clinical Trial) | NCT02431975 | Up to 48 h of life | Very Early ART | South Africa | ART free remission |
| Tatelo Study | NCT03707977 | 96 weeks to 7 years | Early ART + combination bNAbs | Botswana | Safety and efficacy of dual bNAb VRC01LS and 10-1074 to control viraemia off ART |
| HIV-Netherlands Australia, Thailand Research Collaboration | NCT00476606 | 1 day to 20 years | Early ART | Thailand | Evaluate immunological and clinical outcomes of early ART |
| HVRRICANE Trial | NCT04301154 | 9 years or older | ART + HIVIS-DNA vaccine + MVA-CMDR boost with or without TLR-4 agonist | South Africa | Safety and effects of using primer boost vaccine regimens with/without TLR 4 agonist |
| Antiretroviral Regime for Viral Eradication in Newborns | NCT02712801 | 0–1 day of life | Very Early ART | China | HIV Cure |
| Profiles | Mississippi Baby (2013) [35] | French Adolescent (2017) [34] | South African Child (2019) [36] |
|---|---|---|---|
| Intervention | Very Early ART | Early ART | Early ART |
| Age at ART initiation | 30 h | 3 months | 2 months |
| Sex | Female | Female | Male |
| Duration of intervention | 18 months | 5.8–6.8 years | 40 weeks |
| Age at remission detection | 23 months | 18.6 years | 9.5 years |
| Duration of remission | 27.6 months | >12 years | 8.5 years |
| Biomarker profile: HIV DNA (Log10 copies per million PBMCs) | Nondetectable (<0.43) | Detectable (2.2) | Detectable (0.69) |
| HIV-1 Serostatus | Seronegative | Seropositive | Indeterminate |
| Low level Viremia | Undetectable | Detectable | Detectable |
| Inducible reservoir | Not detectable | Detectable | Detectable |
| HIV subtype | B | H | C |
| Assay | Measure | Advantages | Disadvantages |
|---|---|---|---|
| Culture based assay | |||
| Quantitative Viral Outgrowth Assay (qVOA) [5,12,22,168,169,170] | Replication competent infectious virus | Minimal estimate of the latent reservoir, reproducible | Long turnaround time (21 days), laborious, not all intact proviruses are induced, large cell number required, expensive |
| Tat-Rev Inducing Limiting Dilution Assay (TILDA) [14,171,172] | Transcriptionally competent virus | Shorter turnaround time than QVOA, no RNA extraction required, sensitive, reproducible, specific to HIV | Cannot differentiate between transcripts from intact and defective proviruses, not all intact proviruses are induced |
| Molecular assay | |||
| Quantitative PCR (qPCR) [10,168,170,173,174] | Total HIV-1 proviral DNA | Low volume required, cost effective, short turnaround time, high throughput | Overestimates size of reservoir, cannot differentiate between intact vs defective and integrated vs non- integrated forms, relative quantification via standard curves |
| Alu PCR [173,175,176,177] | Total integrated HIV-1 proviral DNA | Can differentiate between integrated and non-integrated forms, cost effective, short turnaround time, high throughput | Overestimates size of reservoir, cannot differentiate between intact vs defective, relative quantification via standard curves |
| Droplet digital PCR (ddPCR) [14,170,178] | Total HIV-1 proviral DNA | Low volume required, high sensitivity, high throughput, short turnaround time, cost effective, more accurate than qPCR due to absolute quantification | Overestimates size of reservoir, cannot differentiate between intact vs defective and integrated vs non- integrated forms |
| Intact proviral DNA assay (IPDA) [14,179,180] | Intact and defective proviruses | Low volume required, high sensitivity, high throughput, short turnaround time, cost effective, can differentiate between intact, 5′ defective, 3′ defective and hypermutated | Overestimates size of the reservoir, cannot differentiate between integrated vs non-integrated forms, subtype B specific |
| Quadraplex quantitative PCR (Q4PCR) [181,182,183] | Intact and defective proviruses | Provides information on genetic intactness of provirus, low volume required, sensitive, can differentiate between intact and defective proviruses, high throughput compared to conventional near full- length genome sequencing | Cannot differentiate between integrated vs non-integrated forms, subtype B specific, relies on initial long-distance PCR so not quantitative as a standalone assay, low throughput, expensive |
| 5 Target-Intact Proviral DNA Assay (5T-IPDA) [184] | Intact and defective proviruses | Low volume required, high sensitivity, high throughput, short turnaround time, cost effective, can differentiate between intact and defective proviruses | Overestimates size of reservoir, cannot differentiate between integrated vs non-integrated forms, complex analysis, require 2 sets of controls, subtype B specific |
| Cross Subtype-IPDA (CS-IPDA) [185] | Intact and defective proviruses | Similar to 5T-IPDA and can work across different subtypes A, B, C, D, CRF_01 | Similar to 5T-IPDA |
| Proviral Landscape Analysis | |||
| Near full-length individual proviral sequencing (FLIP-seq) [11,76,183,186] | Intact and defective proviruses | Provides information on genetic intactness of provirus | Low throughput, expensive, complex, time consuming, cannot amplify intact proviruses at the same frequency as defective proviruses due to inefficiency of the initial long-distance PCR |
| Matched integration site and proviral sequencing (MIP-seq)) [85,183,187] | Intact and defective proviruses; integration site of proviruses | Provides information on integration site and clonal expansion, genetic intactness of provirus | Similar to FLIP-seq |
| Parallel HIV-1 RNA, integration site and proviral sequencing (PRIP-seq) [188] | Intact and defective proviruses, integration site and transcriptional competence of provirus | Provides information on the genetic intactness, integration site, clonality and transcriptional competence of a provirus | Similar to FLIP-seq |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khetan, P.; Liu, Y.; Dhummakupt, A.; Persaud, D. Advances in Pediatric HIV-1 Cure Therapies and Reservoir Assays. Viruses 2022, 14, 2608. https://doi.org/10.3390/v14122608
Khetan P, Liu Y, Dhummakupt A, Persaud D. Advances in Pediatric HIV-1 Cure Therapies and Reservoir Assays. Viruses. 2022; 14(12):2608. https://doi.org/10.3390/v14122608
Chicago/Turabian StyleKhetan, Priya, Yufeng Liu, Adit Dhummakupt, and Deborah Persaud. 2022. "Advances in Pediatric HIV-1 Cure Therapies and Reservoir Assays" Viruses 14, no. 12: 2608. https://doi.org/10.3390/v14122608