
SARS-CoV-2 Infection and Possible Neonatal Neurological Outcomes: A Literature Review


 ,
,
Abstract
:1. Introduction
2. Methods
3. Perinatal SARS-CoV-2 Infection and Immune Response in Neonates
3.1. Clinical Presentations in Newborns
3.2. Diagnosis of SARS-CoV-2 in Neonates
4. Viral Infections and Long-Term Neonatal Outcomes
5. Severe Encephalitis with Cytotoxic Brain Edema in a Newborn with COVID-19
Ischemic Lesions in the Brain
6. Childhood Multisystem Inflammatory Syndrome (MIS-C)
6.1. Shock and Electrolyte Abnormalities
6.2. Ophthalmic Manifestations
7. SARS-CoV-2 Variants and Potential Differences in Neonates’ Immunological Systems
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Lauxmann, M.A.; Santucci, N.E.; Autrán-Gómez, A.M. The SARS-CoV-2 coronavirus and the COVID-19 outbreak. Int. Braz J Urol 2020, 46, 6–18. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.; Quigley, M.A.; Placzek, A.; Knight, M.; Ladhani, S.; Draper, E.S.; Sharkey, D.; Doherty, C.; Mactier, H.; Kurinczuk, J.J. Characteristics and outcomes of neonatal SARS-CoV-2 infection in the UK: A prospective national cohort study using active surveillance. Lancet Child Adolesc. Health 2021, 5, 113–121. [Google Scholar] [CrossRef]
- Barrero-Castillero, A.; Beam, K.S.; Bernardini, L.B.; Ramos, E.G.C.; Davenport, P.E.; Duncan, A.R.; Fraiman, Y.S.; Frazer, L.C.; Healy, H.; Herzberg, E.M.; et al. COVID-19: Neonatal–perinatal perspectives. J. Perinatol. 2021, 41, 940–951. [Google Scholar] [CrossRef] [PubMed]
- Stafstrom, C.E.; Jantzie, L.L. COVID-19: Neurological Considerations in Neonates and Children. Children 2020, 7, 133. [Google Scholar] [CrossRef]
- Kallimath, A.; Garegrat, R.; Patnaik, S.; Suryawanshi, P. Shock and dyselectrolytemia in a neonate with late-onset COVID-19 infection. BMJ Case Rep. 2021, 14, e246100. [Google Scholar] [CrossRef]
- Lu, Q.; Shi, Y. Coronavirus disease (COVID-19) and neonate: What neonatologist need to know. J. Med. Virol. 2020, 92, 564–567. [Google Scholar] [CrossRef] [Green Version]
- Condie, L.O. Neurotropic mechanisms in COVID-19 and their potential influence on neuropsychological outcomes in children. Child Neuropsychol. 2020, 26, 577–596. [Google Scholar] [CrossRef]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef]
- Mullins, E.; Hudak, M.L.; Banerjee, J.; Getzlaff, T.; Townson, J.; Barnette, K.; Playle, R.; Perry, A.; Bourne, T.; Lees, C.C.; et al. Pregnancy and neonatal outcomes of COVID-19: Coreporting of common outcomes from PAN-COVID and AAP-SONPM registries. Ultrasound Obstet. Gynecol. 2021, 57, 573–581. [Google Scholar] [CrossRef]
- Khoury, R.; Bernstein, P.S.; Debolt, C.; Stone, J.; Sutton, D.M.; Simpson, L.L.; Limaye, M.A.; Roman, A.S.; Fazzari, M.; Penfield, C.A.; et al. Characteristics and outcomes of 241 births to women with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection at Five New York City Medical Centers. Obstet. Gynecol. 2020, 136, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Kayem, G.; Lecarpentier, E.; Deruelle, P.; Bretelle, F.; Azria, E.; Blanc, J.; Bohec, C.; Bornes, M.; Ceccaldi, P.-F.; Chalet, Y.; et al. A snapshot of the COVID-19 pandemic among pregnant women in France. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101826. [Google Scholar] [CrossRef] [PubMed]
- SONPM National Registry for Surveillance and Epidemiology of Perinatal COVID-19 Infection: Section on Neonatal-Pernatal Medicine. Am. Acad. Pediatrics 2020. Available online: https://my.visme.co/view/ojq9qq8e-npc-19-registry (accessed on 27 February 2022).
- Dhochak, N.; Singhal, T.; Kabra, S.K.; Lodha, R. Pathophysiology of COVID-19: Why Children Fare Better than Adults? Indian J. Pediatrics 2020, 87, 537–546. [Google Scholar] [CrossRef]
- Bunyavanich, S.; Do, A.; Vicencio, A. Nasal Gene Expression of Angiotensin-Converting Enzyme 2 in Children and Adults. JAMA J. Am. Med. Assoc. 2020, 323, 2427. [Google Scholar] [CrossRef] [PubMed]
- Goh, X.L.; Low, Y.F.; Ng, C.H.; Amin, Z.; Ng, Y.P.M. Incidence of SARS-CoV-2 Vertical Transmission: A Meta-Analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 112–113. Available online: https://pubmed.ncbi.nlm.nih.gov/32586828/ (accessed on 30 March 2022). [CrossRef]
- Definition and Categorization of the Timing of Mother-to-Child Transmission of SARS-CoV-2. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-mother-to-child-transmission-2021.1 (accessed on 28 February 2022).
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Abasse, S.; Essabar, L.; Costin, T.; Mahisatra, V.; Kaci, M.; Braconnier, A.; Serhal, R.; Collet, L.; Fayssoil, A. Neonatal COVID-19 Pneumonia: Report of the First Case in a Preterm Neonate in Mayotte, an Overseas Department of France. Children 2020, 7, 87. [Google Scholar] [CrossRef]
- Kamali Aghdam, M.; Jafari, N.; Eftekhari, K. Novel coronavirus in a 15-day-old neonate with clinical signs of sepsis, a case report. Infect. Dis. 2020, 52, 427–429. [Google Scholar] [CrossRef] [Green Version]
- Alzamora, M.C.; Paredes, T.; Caceres, D.; Webb, C.M.; Webb, C.M.; Valdez, L.M.; La Rosa, M. Severe COVID-19 during Pregnancy and Possible Vertical Transmission. Am. J. Perinatol. 2020, 37, 861–865. [Google Scholar] [CrossRef] [Green Version]
- Ayed, A.; Embaireeg, A.; Benawadh, A.; Al-Fouzan, W.; Hammoud, M.; Al-Hathal, M.; Alzaydai, A.; Ahmad, A.; Ayed, M. Maternal and perinatal characteristics and outcomes of pregnancies complicated with COVID-19 in Kuwait. BMC Pregnancy Childbirth 2020, 20, 754. [Google Scholar] [CrossRef]
- Bandyopadhyay, T.; Sharma, A.; Kumari, P.; Maria, A.; Choudhary, R. Possible Early Vertical Transmission of COVID-19 from an Infected Pregnant Female to Her Neonate: A Case Report. J. Trop. Pediatrics 2021, 67, fmaa094. [Google Scholar] [CrossRef] [PubMed]
- Bordbar, A.; Kashaki, M.; Rezaei, F.; Jafari, R. Vertical transmission of COVID-19 in a 1-day-old neonate. Travel Med. Infect. Dis. 2020, 38, 101879. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Costa, S.; Sanguinetti, M.; Cattani, P.; Posteraro, B.; Marchetti, S.; Carducci, B.; Lanzone, A.; Tamburrini, E.; Vento, G.; et al. Neonatal Late Onset Infection with Severe Acute Respiratory Syndrome Coronavirus 2. Am. J. Perinatol. 2020, 37, 869–872. [Google Scholar] [PubMed]
- Cakir, U.; Demirel, M.A.; Yuksek, S.K.; Tugcu, A.U.; Tufan, N.; Tayman, C. Case Report of Severe COVID-19 Pneumonia in a Term Newborn. J. Trop. Pediatr. 2021, 67, fmab023. [Google Scholar] [CrossRef] [PubMed]
- Carosso, A.; Cosma, S.; Borella, F.; Marozio, L. Pre-labor anorectal swab for SARS-CoV-2 in COVID-19 pregnant patients: Is it time to think about it? Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 249, 98–99. [Google Scholar] [CrossRef]
- Munoz, A.C.; Nawaratne, U.; McMann, D.; Ellsworth, M.; Meliones, J.; Boukas, K. Late-Onset Neonatal Sepsis in a Patient with COVID-19. N. Engl. J. Med. 2020, 382, e49. [Google Scholar] [CrossRef]
- Demirjian, A.; Singh, C.; Tebruegge, M.; Herbert, R.; Draz, N.; Mirfenderesky, M.; Jones, V.; Hinstridge, P.; Seneviratne, R.; Myers, R.; et al. Probable Vertical Transmission of SARS-CoV-2 Infection. Pediatric Infect. Dis. J. 2020, 39, 257–260. [Google Scholar] [CrossRef]
- Díaz, C.A.; Maestro, M.L.; Pumarega, M.T.M.; Antón, B.F.; Alonso, C.P. First case of neonatal infection due to COVID-19 in Spain. An. Pediatría (Engl. Ed.) 2020, 92, 236–237. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7195017/pdf/main.pdf (accessed on 26 March 2022).
- Dong, L.; Tian, J.; He, S.; Zhu, C.; Wang, J.; Liu, C.; Yang, J. Possible Vertical Transmission of SARS-CoV-2From an Infected Mother to Her Newborn. JAMA J. Am. Med. Assoc. 2020, 323, 1844–1846. [Google Scholar]
- Dumpa, V.; Kamity, R.; Vinci, A.N.; Noyola, E.; Noor, A. Neonatal Coronavirus 2019 (COVID-19) Infection: A Case Report and Review of Literature. Cureus 2020, 12, e8165. [Google Scholar] [CrossRef] [PubMed]
- Eghbalian, F.; Esfahani, A.M.; Jenabi, E. COVID-19 Virus in a 6-Day-Old Girl Neonate: A Case Report. Clin. Pediatr. 2020, 59, 1288–1289. [Google Scholar] [CrossRef] [PubMed]
- Farmer, M.L. A Neonate with Vertical Transmission of COVID-19 and Acute Respiratory Failure. Adv. Neonatal Care, 2021; Publish Ahead of Print. [Google Scholar] [CrossRef] [PubMed]
- Fenizia, C.; Biasin, M.; Cetin, I.; Vergani, P.; Mileto, D.; Spinillo, A.; Gismondo, M.R.; Perotti, F.; Callegari, C.; Mancon, A.; et al. In-utero mother-to-child SARS-CoV-2 transmission: Viral detection and fetal immune response. medRxiv 2020. [Google Scholar] [CrossRef]
- Brabin, A.G.; Iglesias-Bouzas, M.I.; Nieto-Moro, M.; de Azagra-Garde, A.M.; García-Salido, A. Apnea neonatal como manifestación inicial de infección por SARS-CoV-2. Clin. Infect. Dis. 2020, 71, 1547–1551. [Google Scholar]
- Gordon, M.; Kagalwala, T.; Rezk, K.; Rawlingson, C.; Ahmed, M.I.; Guleri, A. Rapid systematic review of neonatal COVID-19 including a case of presumed vertical transmission. BMJ Paediatr. Open 2020, 4, e000718. [Google Scholar] [CrossRef]
- Gregorio-Hernández, R.; Escobar-Izquierdo, A.B.; Cobas-Pazos, J.; Martínez-Gimeno, A. Point-of-care lung ultrasound in three neonates with COVID-19. Eur. J. Pediatrics 2020, 179, 1279–1285. [Google Scholar] [CrossRef]
- Han, M.S.; Seong, M.-W.; Heo, E.Y.; Park, J.H.; Kim, N.; Shin, S.; Cho, S.I.; Park, S.S.; Choi, E.H. Sequential Analysis of Viral Load in a Neonate and Her Mother Infected with SARS-CoV-2. 2020. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7184375/ (accessed on 28 February 2022).
- Hu, X.; Gao, J.; Luo, X.; Feng, L.; Liu, W.; Chen, J.; Benachi, A.; De Luca, D.; Chen, L. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vertical Transmission in Neonates Born to Mothers with Coronavirus Disease 2019 (COVID-19). Pneumonia 2020. Available online: http://www.gov.cn/zhengce/zhengceku/2020-01/ (accessed on 26 March 2022).
- Huseynova, R.A.; ABin Mahmoud, L.; Huseynov, O.; Almalkey, M.; Amer Almotiri, A.; Sumaily, H.H.; AbdelRahim, A. A neonate born to an infected COVID-19 mother was tested positive just 24 hours after its birth. Clin. Case Rep. 2021, 9, 1954–1957. [Google Scholar] [CrossRef]
- Kirtsman, M.; Diambomba, Y.; Poutanen, S.M.; Malinowski, A.K.; Vlachodimitropoulou, E.; Parks, W.T.; Erdman, L.; Morris, S.K.; Shah, P.S. Probable congenital SARS-CoV-2 infection in a neonate born to a woman with active SARS-CoV-2 infection. 2020, 15, 647. Available online: https://downloads.aap.org/AAP/PDF/COVID%2019%20Initial%20Newborn%20 (accessed on 26 March 2022). [CrossRef]
- Kulkarni, R.; Rajput, U.; Dawre, R.; Valvi, C.; Nagpal, R.; Magdum, N.; Vankar, H.; Sonkawade, N.; Das, A.; Vartak, S.; et al. Early-onset symptomatic neonatal COVID-19 infection with high probability of vertical transmission. Infection 2020, 49, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.H.S.; Prasath, A.; Blanco, C.; Kenney, P.O.; Ostwald, C.M.; Meyer, T.S.; Clementi, C.; Maciejewski, R.; Wilby, M.; Reynolds, A.; et al. Respiratory failure in an extremely premature neonate with covid-19. Children 2021, 8, 477. [Google Scholar] [CrossRef] [PubMed]
- Lorenz NTASSHRR-ERGGK. Neonatal Early-Onset Infection with SARS-CoV-2 in a Newborn Presenting with Encephalitic Symptoms. Pediatric Infect. Dis. J. 2020, 39, e212. Available online: https://journals.lww.com/pidj/Fulltext/2020/08000/Neonatal_Early_Onset_Infection_With_SARS_CoV_2_in.36.aspx (accessed on 28 February 2022). [CrossRef] [PubMed]
- Martin, P.J.; Felker, M.; Radhakrishnan, R. MR Imaging Findings in a Neonate with COVID-19-Associated Encephalitis. Pediatr. Neurol. 2021, 119, 48–49. [Google Scholar] [CrossRef] [PubMed]
- Oscar, M.-P.; Manon, V.; Cruz, M.S.; Forcen, A.L.; Alice, P.; Mar, M.-C.; Baud, D. Association Between Mode of Delivery AmongPregnant Women with COVID-19 and Maternaland Neonatal Outcomes in Spain. JAMA J. Am. Med. Assoc. 2020, 324, 294–296. [Google Scholar]
- Marzollo, R.; Aversa, S.; Prefumo, F.; Saccani, B.; Perez, C.R.; Sartori, E.; Motta, M. Possible Coronavirus Disease 2019 Pandemic and Pregnancy: Vertical Transmission Is Not Excluded. Pediatr. Infect. Dis. J. 2020, 39, e261–e262. [Google Scholar] [CrossRef]
- Meslin, P.; Guiomard, C.; Chouakria, M.; Porcher, J.; Duquesne, F.; Tiprez, C.; Zemouri, N. Coronavirus Disease 2019 in Newborns and Very Young Infantsa Series of Six Patients in France. Available online: https://journals.lww.com/pidj/Fulltext/2020/07000/Coronavirus_Disease_2019_in_Newborns_and_Very.33.aspx (accessed on 28 February 2022).
- Mohagheghi, P.; Hakimelahi, J.; Khalajinia, Z.; Moghadam, P.S.; Moghadam, S. Case Series COVID-19 Infection in Iranian Newborns and their Mothers: A Case Series. Tanaffos 2021, 20, 172–179. [Google Scholar]
- Ng, K.F.; Bandi, S.; Bird, P.W.; Tang, J.W.-T. COVID-19 in Neonates and Infants: Progression and Recovery. JAMA J. Am. Med. Assoc. 2020, 323, 1313–1314. [Google Scholar] [CrossRef]
- Yekta Oncel, M.; Mungan Akın, I.; Kenan Kanburoglu, M.; Tayman, C.; Coskun, S.; Narter, F.; Er, I.; Oncan, T.G.; Memisoglu, A.; Cetinkaya, M.; et al. A multicenter study on epidemiological and clinical characteristics of 125 newborns born to women infected with COVID-19 by Turkish Neonatal Society. Eur. J. Pediatrics 2021, 180, 733–742. [Google Scholar] [CrossRef]
- Pakdel, M.; Pouralizadeh, N.; Faramarzi, R.; Boskabadi, H.; Mamouri, G. Neonates with COVID-19 infection: Is there any different treatment process? J. Pediatric Surg. Case Rep. 2022, 77, 102148. [Google Scholar] [CrossRef]
- Patanè Lmdgmrscpmgflmgamcg. Vertical Transmission of Coronavirus Disease 2019: Severe Acute Respiratory Syndrome Coronavirus 2 RNA on the Fetal Side of the Placenta in Pregnancies with Coronavirus Disease 2019–Positive Mothers and Neonates at Birth. 2020. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7233206/ (accessed on 28 February 2022).
- Patil, U.P.; Maru, S.; Krishnan, P.; Carroll-Bennett, R.; Sanchez, J.; Noble, L.; Wasserman, R. Newborns of COVID-19 mothers: Short-term outcomes of colocating and breastfeeding from the pandemic’s epicenter. J. Perinatol. 2020, 40, 1455–1458. [Google Scholar] [CrossRef] [PubMed]
- Piersigilli, F.; Carkeek, K.; Hocq, C.; van Grambezen, B.; Hubinont, C.; Chatzis, O.; Van der Linden, D.; Danhaive, O. COVID-19 in a 26-week preterm neonate. Lancet Child Adolesc. Health 2020, 4, 476–478. [Google Scholar] [CrossRef]
- Precit, M.R.; Yee, R.; Anand, V.; Mongkolrattanothai, K.; Pandey, U.; Bard, J.D. A Case Report of Neonatal Acute Respiratory Failure Due to Severe Acute Respiratory Syndrome Coronavirus-2. J. Pediatr. Infect. Dis. Soc. 2020, 9, 390–392. [Google Scholar] [CrossRef] [PubMed]
- Thapa, B.; Acharya, S.; Karki, S. Vertical Transmission of COVID-19: A Case Report and Review of Literature. J. Nepal Health Res. Counc. 2021, 19, 203–205. [Google Scholar] [CrossRef] [PubMed]
- Urban, A.; Dyrda, M. Mother and neonate suffering from COVID-19 infection. Is there any risk of vertical transmission? A case report. Ginekol. Pol. 2021, 92, 701–703. [Google Scholar] [CrossRef] [PubMed]
- Jin, W.; Dan, W.; Guo-Ce, C.; Xu-Wei, T.; Ling-Kong, Z. SARS-CoV-2 infection with gastrointestinal symptoms as the first manifestation in a neonate. Chin. J. Contemp. Pediatrics 2020, 22, 211–214. [Google Scholar]
- Wang, S.; Guo, L.; Chen, L.; Liu, W.; Cao, Y.; Zhang, J.; Feng, L. A case report of neonatal COVID-19 infection in China. Clin. Infect. Dis. 2020, 71, 853–857. [Google Scholar] [CrossRef]
- Yu, N.; Li, W.; Kang, Q.; Xiong, Z.; Wang, S.; Lin, X.; Liu, Y.; Xiao, J.; Liu, H.; Deng, D.; et al. Clinical features and obstetric and neonatal outcomes of pregnant patients with COVID-19 in Wuhan, China: A retrospective, single-centre, descriptive study. Lancet Infect. Dis. 2020, 20, 559–564. [Google Scholar] [CrossRef] [Green Version]
- Rai, P.; Kumar, B.K.; Deekshit, V.K.; Karunasagar, I.; Karunasagar, I. Detection Technologies and Recent Developments in the Diagnosis of COVID-19 Infection. Available online: http://health.gov.on.ca/en/pro/programs/ (accessed on 27 March 2022).
- Auriti, C.; de Rose, D.U.; Mondì, V.; Stolfi, I.; Tzialla, C. Neonatal SARS-CoV-2 infection: Practical tips. Pathogens 2021, 10, 611. [Google Scholar] [CrossRef]
- Chan, J.F.-W.; Yip, C.C.-Y.; To, K.K.-W.; Tang, T.H.-C.; Wong, S.C.-Y.; Leung, K.-H.; Fung, A.Y.-F.; Ng, A.C.-K.; Zou, Z.; Tsoi, H.-W.; et al. Improved Molecular Diagnosis of COVID-19 by the Novel, Highly Sensitive and Specific COVID-19-RdRp/Hel Real-Time Reverse Transcription-PCR Assay Validated In Vitro and with Clinical Specimens. J. Clin. Microbiol. 2020, 58, e00310-20. [Google Scholar] [CrossRef] [Green Version]
- Pu, R.; Liu, S.; Ren, X.; Shi, D.; Ba, Y.; Huo, Y.; Zhang, W.; Ma, L.; Liu, Y.; Yang, Y.; et al. The screening value of RT-LAMP and RT-PCR in the diagnosis of COVID-19: Systematic review and meta-analysis. J. Virol. Methods 2022, 300, 114392. [Google Scholar] [CrossRef] [PubMed]
- Muller, W.J. Treatment of perinatal viral infections to improve neurologic outcomes. Pediatr. Res. 2017, 81, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Qiu, K.; He, Q.; Lei, Q.; Lu, W. Mechanisms of Blood-Brain Barrier Disruption in Herpes Simplex Encephalitis. J. Neuroimmune Pharmacol. 2019, 14, 157–172. [Google Scholar] [CrossRef] [PubMed]
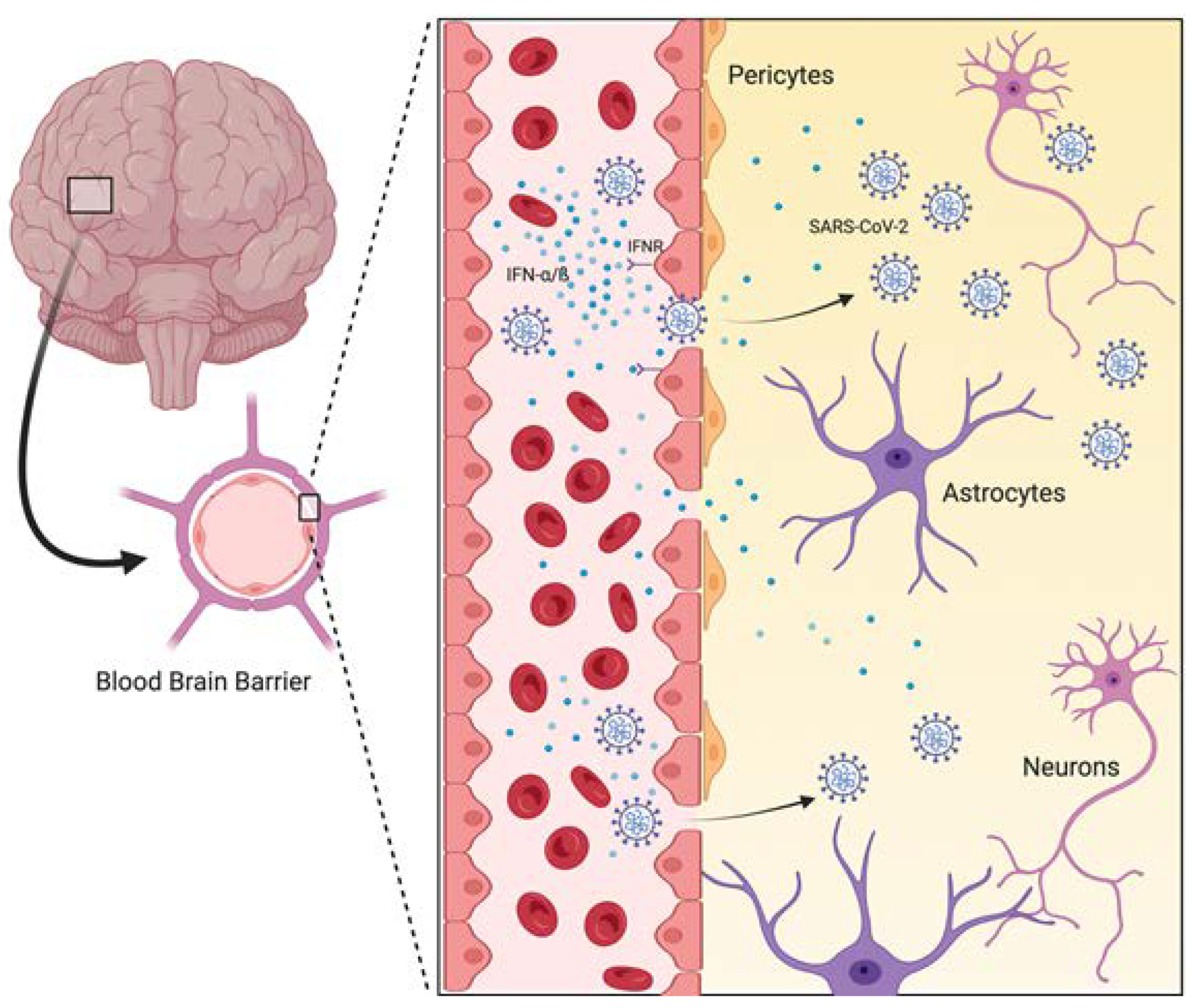
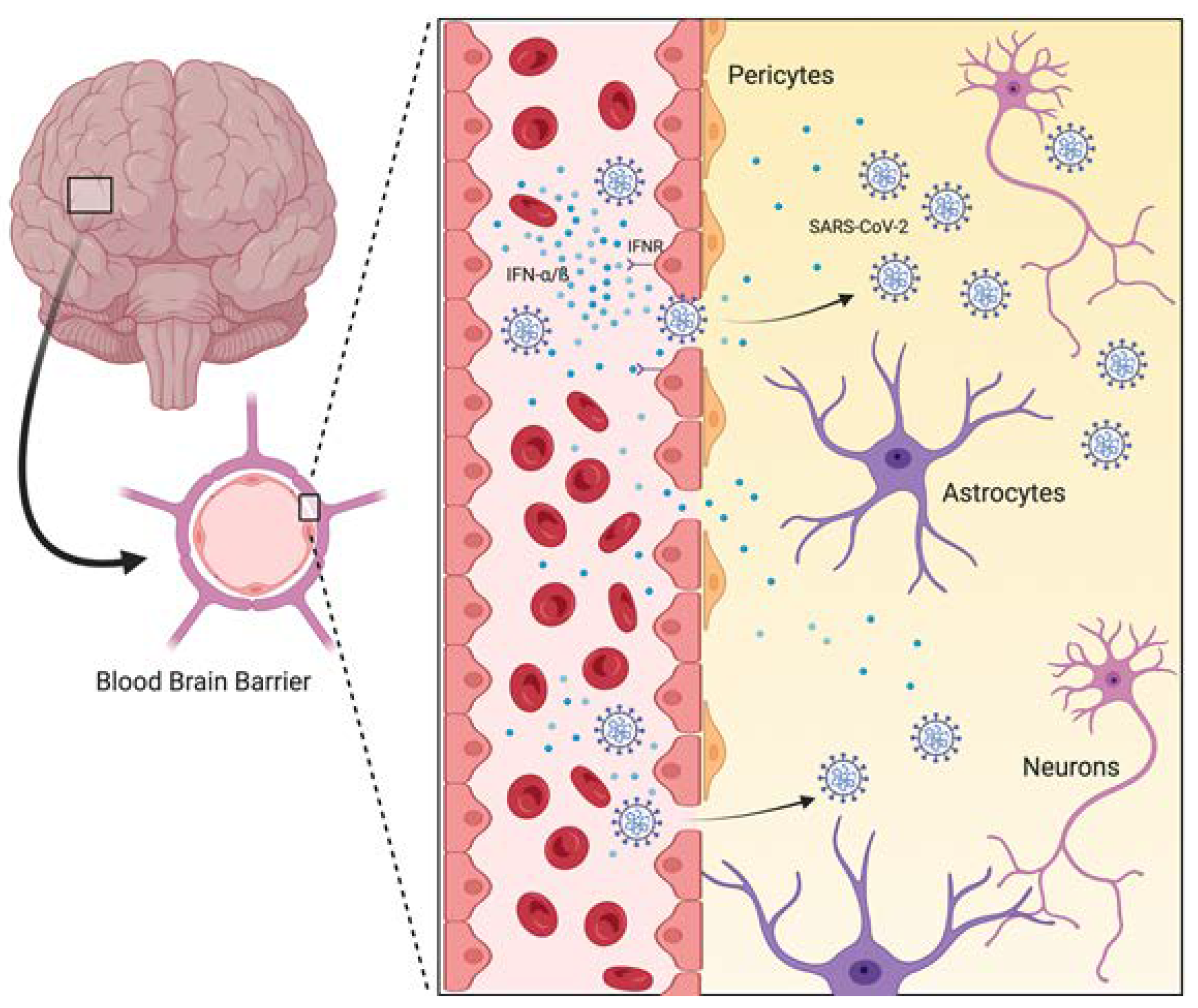
- Chen, Z.; Li, G. Immune response and blood–brain barrier dysfunction during viral neuroinvasion. Innate Immun. 2021, 27, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Buzhdygan, T.P.; DeOre, B.J.; Baldwin-Leclair, A.; Bullock, T.A.; McGary, H.M.; Khan, J.A.; Razmpour, R.; Hale, J.F.; Galie, P.A.; Potula, R.; et al. The SARS-CoV-2 spike protein alters barrier function in 2D static and 3D microfluidic in-vitro models of the human blood–brain barrier. Neurobiol. Dis. 2020, 146, 105131. [Google Scholar] [CrossRef]
- de Vries, L.S. Viral Infections and the Neonatal Brain. Semin. Pediatric Neurol. 2019, 32, 100769. [Google Scholar] [CrossRef]
- Bentz, G.L.; Jarquin-Pardo, M.; Chan, G.; Smith, M.S.; Sinzger, C.; Yurochko, A.D. Human Cytomegalovirus (HCMV) Infection of Endothelial Cells Promotes Naïve Monocyte Extravasation and Transfer of Productive Virus To Enhance Hematogenous Dissemination of HCMV. J. Virol. 2006, 80, 11539–11555. [Google Scholar] [CrossRef] [Green Version]
- Chan, G.; Nogalski, M.T.; Stevenson, E.V.; Yurochko, A.D. Human cytomegalovirus induction of a unique signalsome during viral entry into monocytes mediates distinct functional changes: A strategy for viral dissemination. J. Leukoc. Biol. 2012, 92, 743–752. [Google Scholar] [CrossRef] [Green Version]
- Desforges, M.; Le Coupanec, A.; Stodola, J.K.; Meessen-Pinard, M.; Talbot, P.J. Human coronaviruses: Viral and cellular factors involved in neuroinvasiveness and neuropathogenesis. Virus Res. 2014, 194, 145–158. [Google Scholar] [CrossRef]
- Bullen, C.K.; Hogberg, H.T.; Bahadirli-Talbott, A.; Bishai, W.R.; Hartung, T.; Keuthan, C.; Looney, M.M.; Pekosz, A.; Romero, J.C.; Sille, F.C.M.; et al. Infectability of Human BrainSphere Neurons Suggests Neurotropism of SARS-CoV-2. Altex 2020, 37, 665–671. [Google Scholar]
- Mutnal, M.B.; Cheeran, M.C.-J.; Hu, S.; Lokensgard, J.R. Murine Cytomegalovirus Infection of Neural Stem Cells Alters Neurogenesis in the Developing Brain. PLoS ONE 2011, 6, e16211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuler-Faccini, L.; Ribeiro, E.M.; Feitosa, I.M.L.; Horovitz, D.D.; Cavalcanti, D.P.; Pessoa, A.; Doriqui, M.J.R.; Neri, J.I.; de Pina Neto, J.M.; Wanderley, H.Y.C.; et al. Possível Associação Entre a Infecção Pelo Vírus Zika e a Microcefalia-Brasil, 2015. Morbidity Mortality Weekly Rep. 2016. Available online: http://www.cdc.gov/media/releases/2016/t0116-zika-virus-travel.html (accessed on 27 March 2022).
- Brasil, P.; Pereira, J.P.; Moreira, M.E.; Ribeiro Nogueira, R.M.; Damasceno, L.; Wakimoto, M.; Rabello, R.S.; Valderramos, S.G.; Halai, U.-A.; Salles, T.S.; et al. Zika Virus Infection in Pregnant Women in Rio de Janeiro. N. Engl. J. Med. 2016, 375, 2321–2334. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Hammack, C.; Ogden, S.C.; Wen, Z.; Qian, X.; Li, Y.; Yao, B.; Shin, J.; Zhang, F.; Lee, E.M.; et al. Zika virus infects human cortical neural progenitors and attenuates their growth. Cell Stem Cell 2016, 18, 587–590. [Google Scholar] [CrossRef] [Green Version]
- Fragoso, D.C.; Marx, C.; Dutra, B.G.; da Silva, C.J.; da Silva, P.M.; Junior, A.C.M.M.; Tobara, M.C.; Silva, C.D.A.; Dias, L.; Polycarpo, A.C.; et al. COVID-19 as a Cause of Acute Neonatal Encephalitis and Cerebral Cytotoxic Edema. Pediatr. Infect. Dis. J. 2021, 40, e270–e271. [Google Scholar] [CrossRef]
- Brum, A.C.; Glasman, M.P.; de Luca, M.C.; Rugilo, C.A.; Urquizu Handal, M.I.; Picon, A.O.; Cook, C.; Vain, N.E. Ischemic Lesions in the Brain of a Neonate with SARS-CoV-2 Infection. Pediatric Infect. Dis. J. 2021, 40, e340–e343. [Google Scholar] [CrossRef] [PubMed]
- Jensen, F.E. Neonatal Seizures: An Update on Mechanisms and Management. Clin. Perinatol. 2009, 36, 881–900. [Google Scholar] [CrossRef] [Green Version]
- Penner, J.; Abdel-Mannan, O.; Grant, K.; Maillard, S.; Kucera, F.; Hassell, J.; Eyre, M.; Berger, Z.; Hacohen, Y.; Moshal, K.; et al. 6-month multidisciplinary follow-up and outcomes of patients with paediatric inflammatory multisystem syndrome (PIMS-TS) at a UK tertiary paediatric hospital: A retrospective cohort study. Lancet Child Adolesc. Health 2021, 5, 473–482. [Google Scholar] [CrossRef]
- Kabeerdoss, J.; Pilania, R.K.; Karkhele, R.; Kumar, T.S.; Danda, D.; Singh, S. Severe COVID-19, multisystem inflammatory syndrome in children, and Kawasaki disease: Immunological mechanisms, clinical manifestations and management. Rheumatol. Int. 2021, 41, 19–32. [Google Scholar] [CrossRef]
- Hoste, L.; van Paemel, R.; Haerynck, F. Multisystem inflammatory syndrome in children related to COVID-19: A systematic review. Eur. J. Pediatr. 2021, 180, 2019–2034. [Google Scholar] [CrossRef]
- Jiang, N.M.; Cowan, M.; Moonah, S.N.; Petri, W.A. The Impact of Systemic Inflammation on Neurodevelopment. Trends Mol. Med. 2018, 24, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Chimal, L.G.; Cuevas, G.G.; Di-Luciano, A.; Chamartín, P.; Amadeo, G.; Martínez-Castellanos, M.A. Ophthalmic manifestations associated with SARS-CoV-2 in newborn infants: A preliminary report. J. AAPOS 2021, 25, 102–104. [Google Scholar] [CrossRef] [PubMed]
- Bian, L.; Gao, F.; Zhang, J.; He, Q.; Mao, Q.; Xu, M.; Liang, Z. Effects of SARS-CoV-2 variants on vaccine efficacy and response strategies. Expert Rev. Vaccines 2021, 20, 365–373. [Google Scholar] [CrossRef]
- WHO. Tracking SARS-CoV-2 Variants. 2021. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 20 April 2022).
- Tao, K.; Tzou, P.L.; Nouhin, J.; Gupta, R.K.; de Oliveira, T.; Kosakovsky Pond, S.L.; Fera, D.; Shafer, R.W. The biological and clinical significance of emerging SARS-CoV-2 variants. Nat. Rev. Genet. 2021, 22, 757–773. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8447121/ (accessed on 23 March 2022). [CrossRef] [PubMed]
- LoTempio, J.; Billings, E.; Draper, K.; Ralph, C.; Moshgriz, M.; Duong, N.; Bard, J.D.; Cai, X.; Wessel, D.; DeBiasi, R.L.; et al. Novel SARS-CoV-2 spike variant identified through viral genome sequencing of the pediatric Washington DC COVID-19 outbreak. medRxiv 2021. [Google Scholar] [CrossRef]
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.K.; Thomson, E.C.; Harrison, E.M.; Ludden, C.; Reeve, R.; Rambaut, A.; COVID-19 Genomics UK (COG-UK) Consortium; et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol. 2021, 19, 409–424. Available online: https://www.nature.com/articles/s41579-021-00573-0 (accessed on 23 March 2022). [CrossRef] [PubMed]
- Cosar, B.; Karagulleoglu, Z.Y.; Unal, S.; Ince, A.T.; Uncuoglu, D.B.; Tuncer, G.; Kilinc, B.R.; Ozkan, Y.E.; Ozkoc, H.C.; Demir, I.N.; et al. SARS-CoV-2 Mutations and Their Viral Variants. Cytokine Growth Factor Rev. 2021. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8252702/ (accessed on 4 December 2021). [CrossRef]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Haider, N.; Abbasi, A.F.; Jaferi, U.; Prakash, S.; Balendra, V. The emerging SARS-CoV-2 variants of concern. Ther. Adv. Infect. Dis. 2021, 8, 204993612110243. [Google Scholar] [CrossRef]
- Khateeb, J.; Li, Y.; Zhang, H. Emerging SARS-CoV-2 variants of concern and potential intervention approaches. Crit. Care 2021, 25, 244. [Google Scholar] [CrossRef]
- Pham, D.V.; Do, H.H.; Nguyen, A.V.; Nguyen, N.T.; Hoang, N.V.; Hoang, N.-A. The first newborn patient with SARS-CoV-2 variant B.1.1.7 identified in Viet Nam: Treatment and care practices. West. Pac. Surveill. Response J. 2021, 12, 77–81. [Google Scholar] [CrossRef]
- Boly, T.J.; Reyes-Hernandez, M.E.; Daniels, E.C.; Kibbi, N.; Bermick, J.R.; Elgin, T.G. Hyperglycemia and Cytopenias as Signs of SARS-CoV-2 Delta Variant Infection in Preterm Infants. Pediatrics 2022. [Google Scholar] [CrossRef] [PubMed]
- Siegel, D.A. Trends in COVID-19 Cases, Emergency Department Visits, and Hospital Admissions among Children and Adolescents Aged 0–17 Years—United States, August 2020–August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1249–1254. Available online: https://www.cdc.gov/mmwr/volumes/70/wr/mm7036e1.htm?s_cid=mm7036e1_w (accessed on 23 March 2022). [CrossRef] [PubMed]

{kind=link}
| Clinical Features | Premature | Term | Total |
|---|---|---|---|
| Asymptomatic | 8 | 12 | 20 |
| Symptomatic | 27 | 40 | 67 |
| Fever | 3 | 20 | 23 |
| Respiratory | |||
| Cough | 2 | 5 | 7 |
| Respiratory distress | 19 | 21 | 40 |
| Tachypnea | 9 | 10 | 19 |
| Coryza | 0 | 4 | 4 |
| Gastrointestinal | |||
| Vomiting | 1 | 4 | 5 |
| Intolerance to feeding | 5 | 11 | 16 |
| Abdominal distension | 2 | 2 | 4 |
| Neurological | |||
| Lethargy | 3 | 5 | 7 |
| Irritability | 0 | 3 | 3 |
| Hypotonia | 0 | 4 | 4 |
| Apnea | 5 | 1 | 6 |
| Seizure | 0 | 5 | 5 |
| Cardiovascular | |||
| Tachycardia | 0 | 4 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Moraes, F.M.; de Souza, J.W.P.S.; Alves, L.P.; de Siqueira, M.F.R.; dos Santos, A.P.A.; de Carvalho Berardo, M.M.; Granja, M.G.; de Castro-Faria-Neto, H.C. SARS-CoV-2 Infection and Possible Neonatal Neurological Outcomes: A Literature Review. Viruses 2022, 14, 1037. https://doi.org/10.3390/v14051037
de Moraes FM, de Souza JWPS, Alves LP, de Siqueira MFR, dos Santos APA, de Carvalho Berardo MM, Granja MG, de Castro-Faria-Neto HC. SARS-CoV-2 Infection and Possible Neonatal Neurological Outcomes: A Literature Review. Viruses. 2022; 14(5):1037. https://doi.org/10.3390/v14051037
Chicago/Turabian Stylede Moraes, Flávia Maciel, Julia Werneck Paulino Soares de Souza, Letícia Pires Alves, Milena Ferreira Ribeiro de Siqueira, Ana Paula Aguiar dos Santos, Mariana Monteiro de Carvalho Berardo, Marcelo Gomes Granja, and Hugo Caire de Castro-Faria-Neto. 2022. "SARS-CoV-2 Infection and Possible Neonatal Neurological Outcomes: A Literature Review" Viruses 14, no. 5: 1037. https://doi.org/10.3390/v14051037