
High Drug Resistance Levels Compromise the Control of HIV Infection in Pediatric and Adult Populations in Bata, Equatorial Guinea

 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Samples Collection
2.3. Confirmation of HIV Diagnosis and ART-Failure Identification
2.4. Resistance Analysis
2.5. HIV-1 Variants’ Characterization
2.6. Statistics Analysis
2.7. Accession Numbers
3. Results
3.1. Study Population
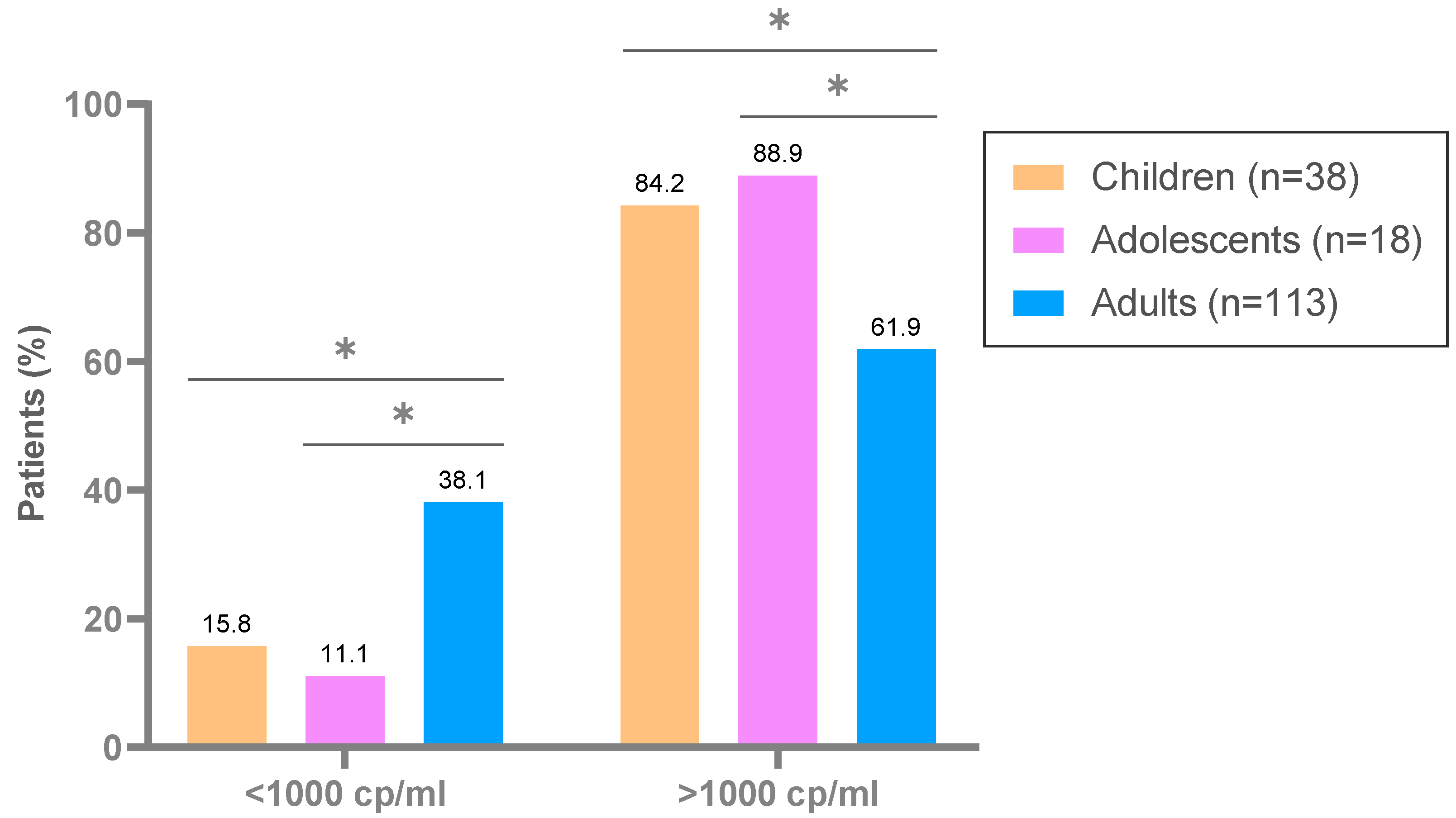
3.2. ART-Failures and Treatment Delay in HIV-Infected and Treated Population
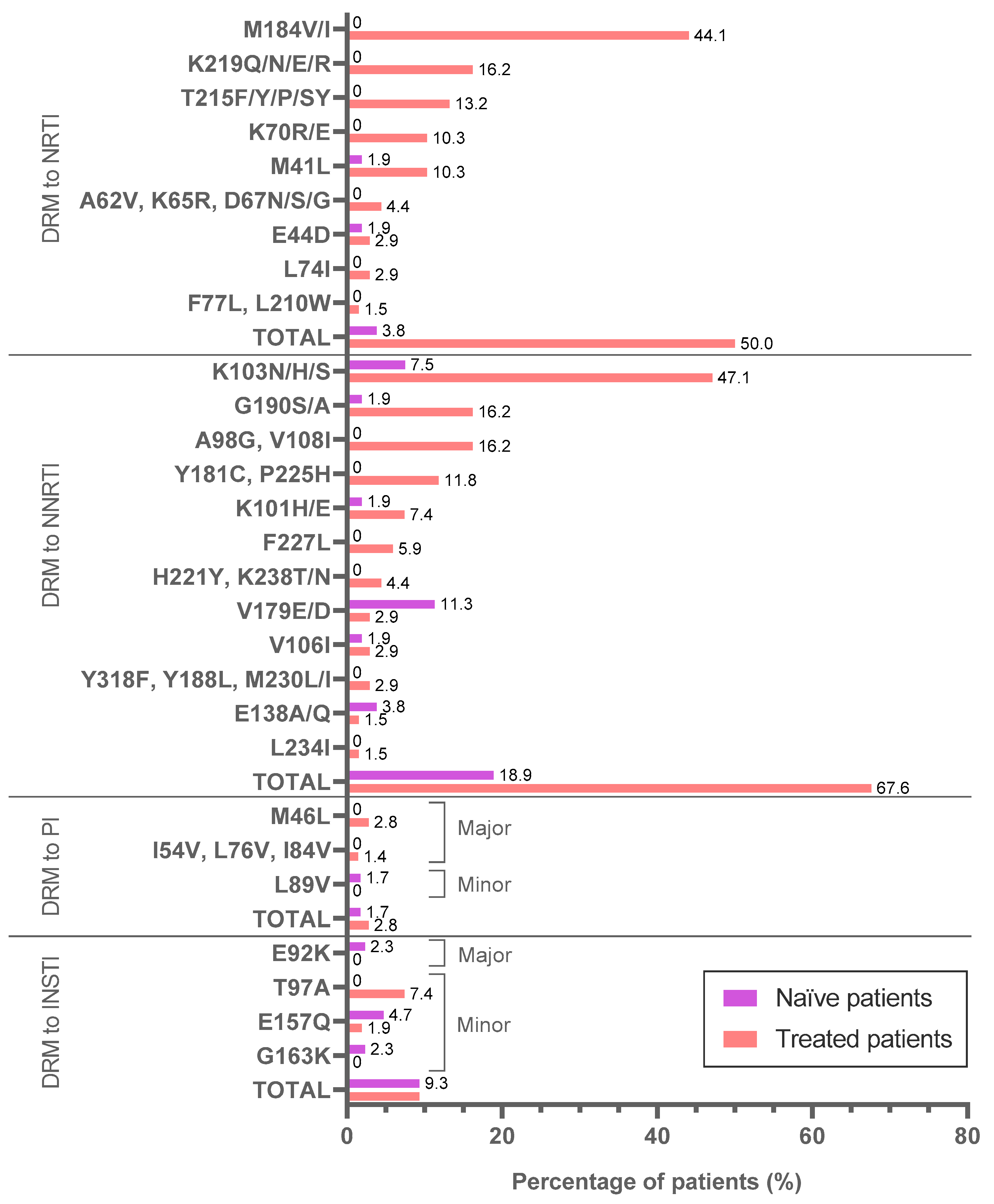
3.3. DRM among 61 Naïve and 80 Treated Patients
3.4. Transmitted Pretreatment Drug Resistance Mutations by Different Tools
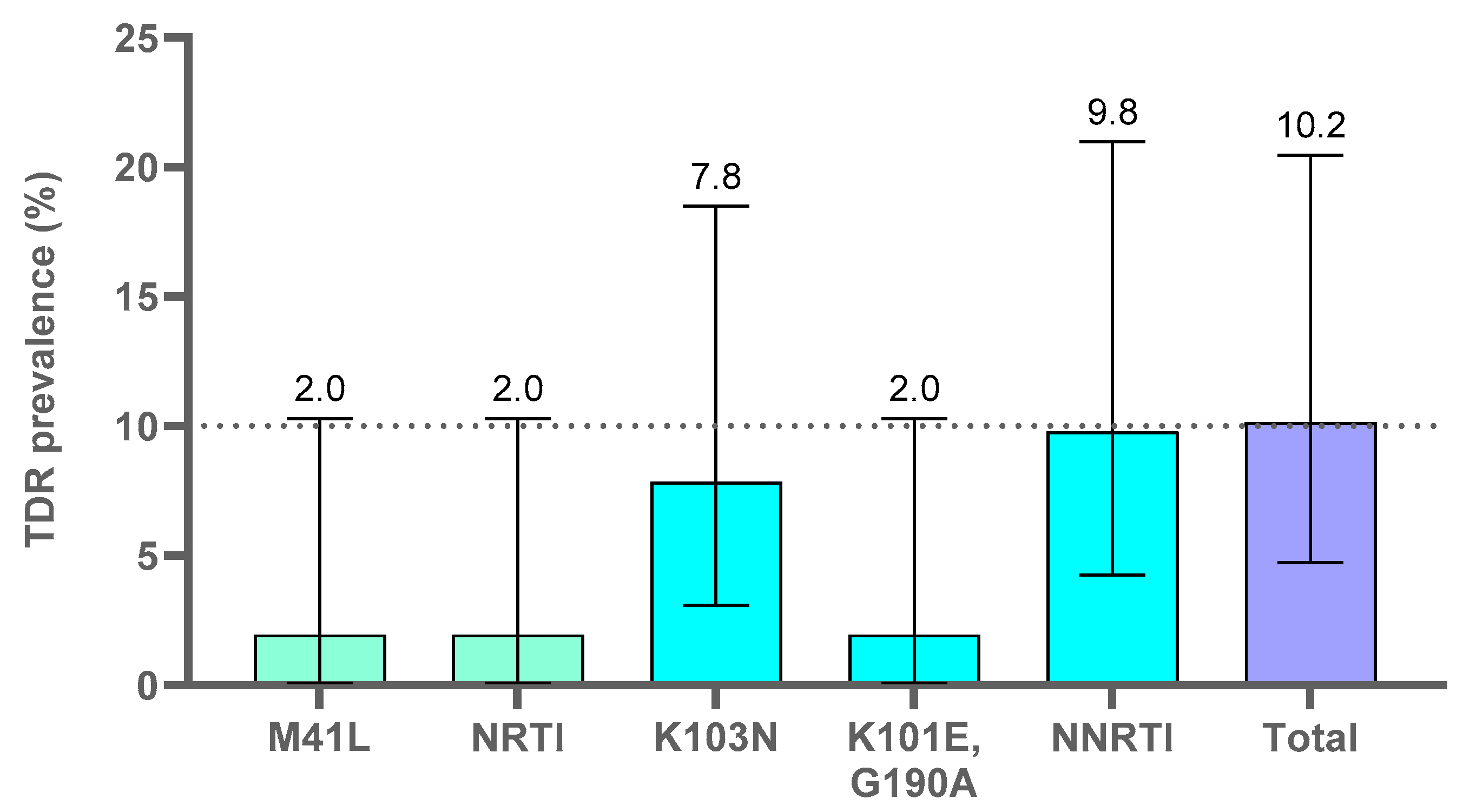
3.4.1. Transmitted PDR Mutations Analysis with the Cprv8.0 Tool (WHO TDR List 2009)
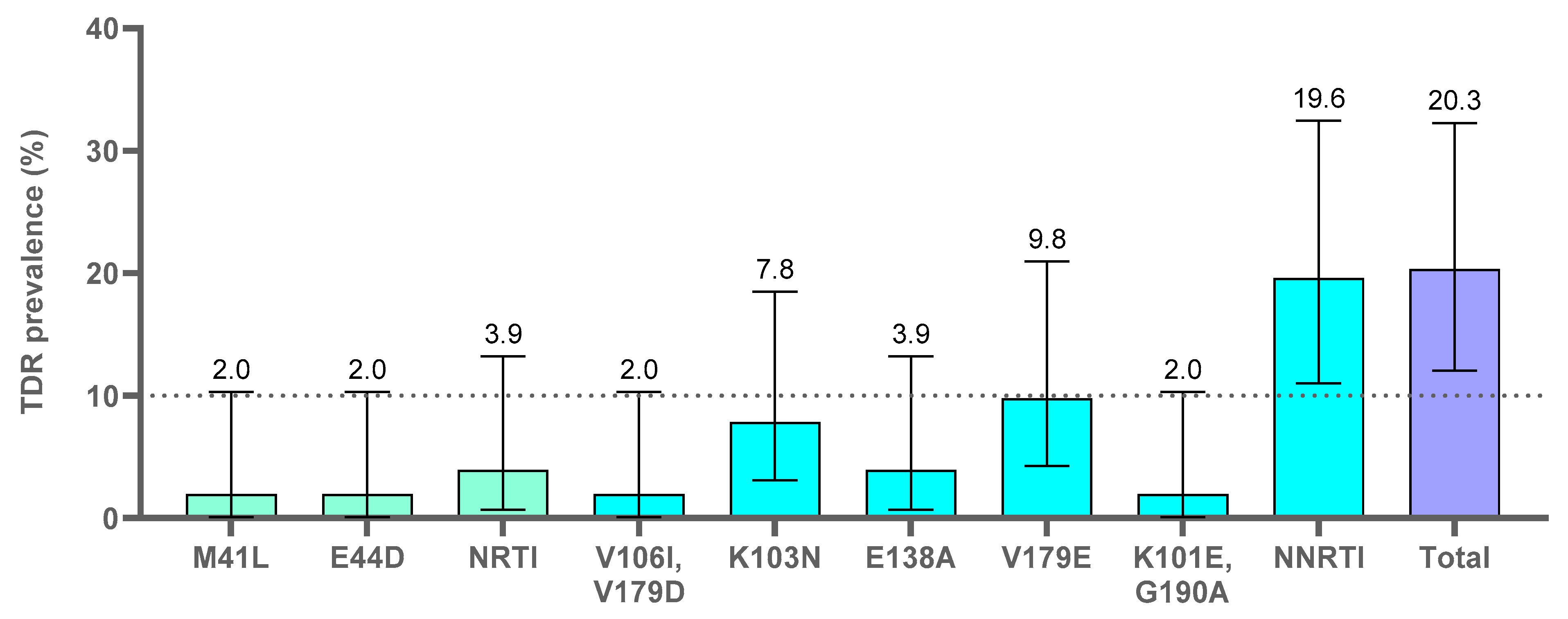
3.4.2. Transmitted PDR Mutations Analysis with the Stanfordv9.0 Tool
3.5. Mother-to-Child DRM Transmission in the Study Cohort
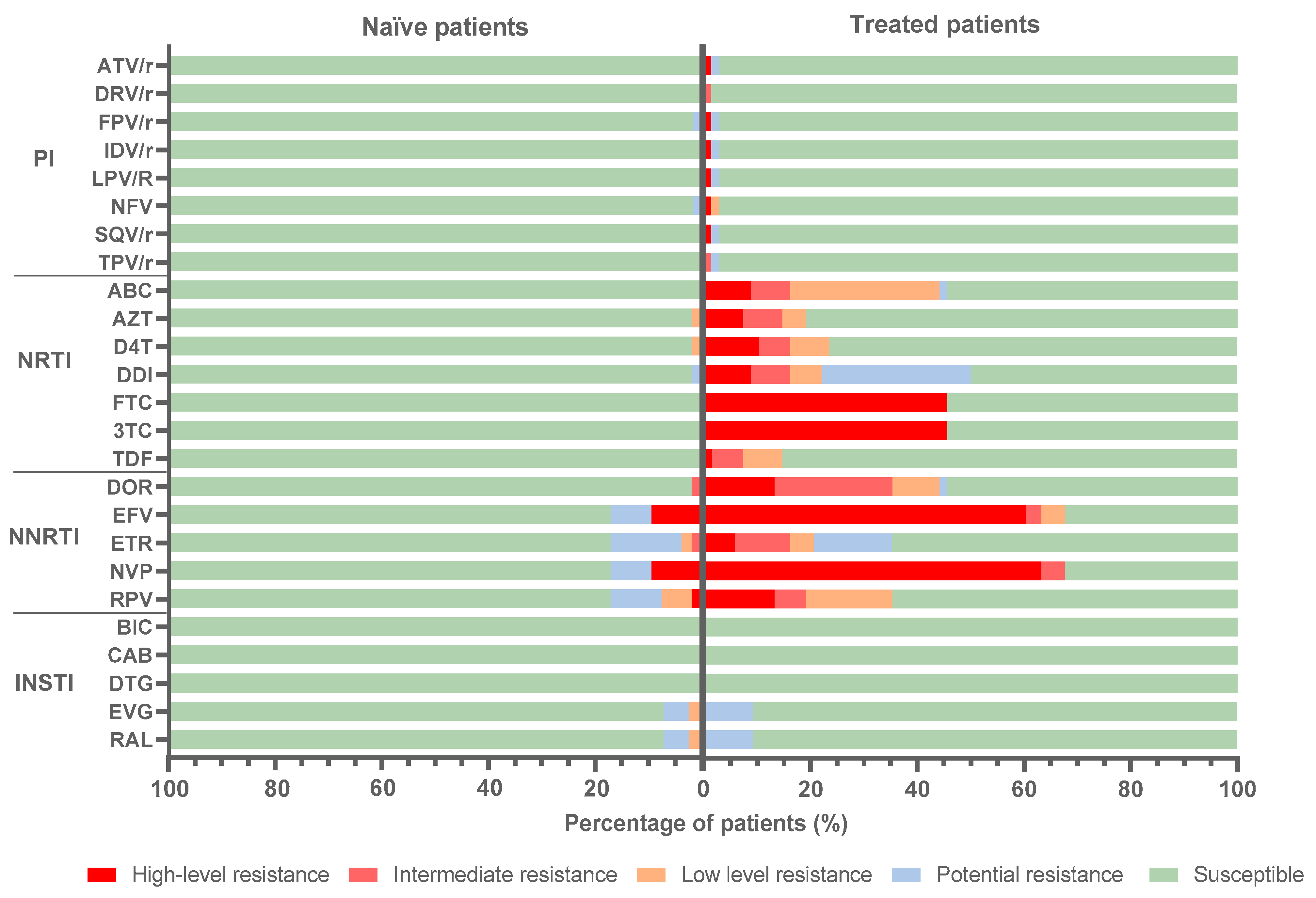
3.6. Predicted Antiretroviral Susceptibility
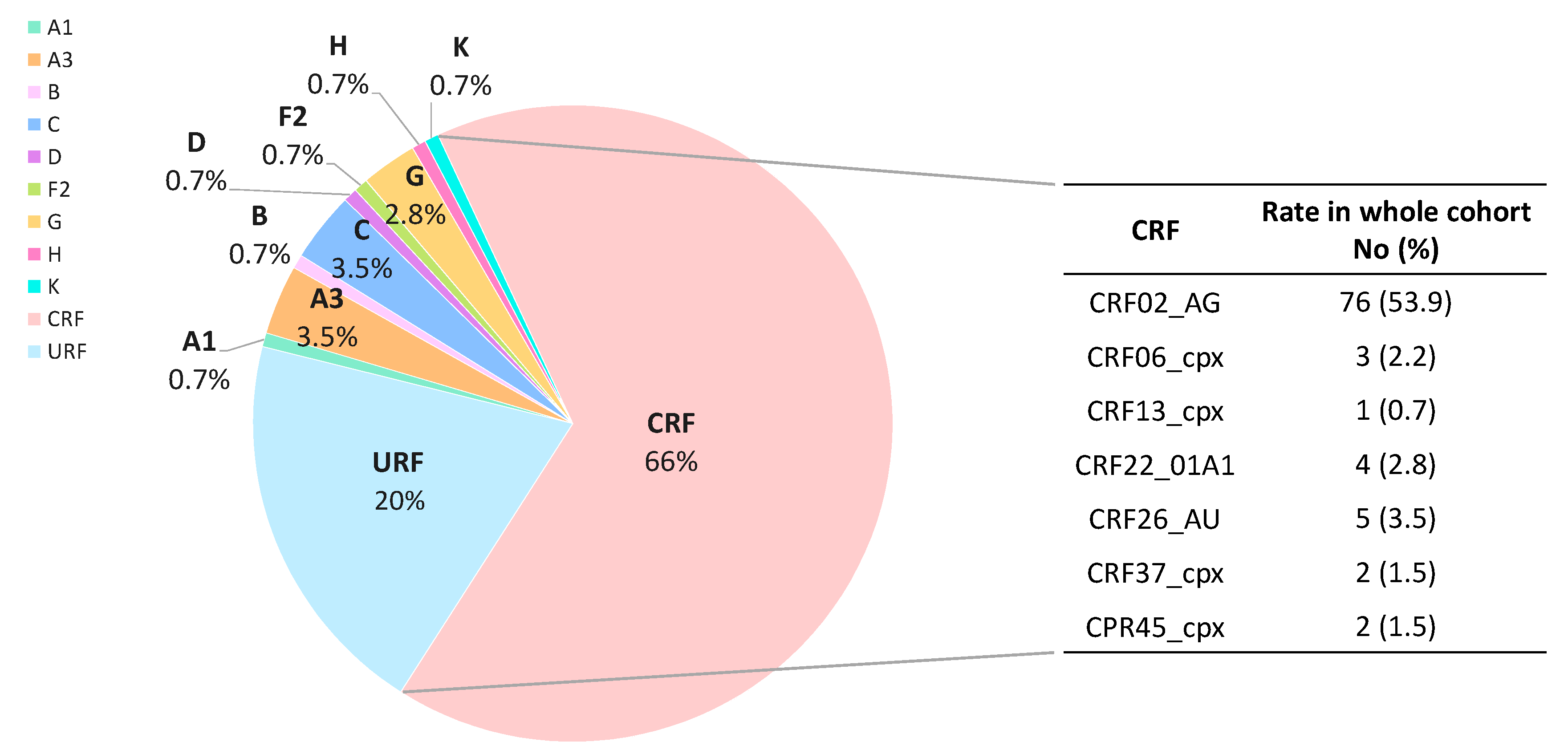
3.7. HIV-1 Viral Variants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joint United Nations Programme on HIV/AIDS (UNAIDS). Danger: UNAIDS Global AIDS Update 2022; Joint United Nations Programme on HIV/AIDS (UNAIDS): Geneva, Switzerland, 2022; Available online: https://www.unaids.org/en/resources/documents/2022/in-danger-global-aids-update (accessed on 1 September 2022).
- Joint United Nations Programme on HIV/AIDS (UNAIDS). AIDSinfo Web. People Living with HIV in Equatorial Guinea. Epidemiological Estimates 2022. Available online: https://aidsinfo.unaids.org (accessed on 1 September 2022).
- Ministerio de Asuntos Sociales e Igualdad de Género de Guinea Ecuatorial (MINASIG). Informe Nacional de Guinea Ecuatorial. 2019. Available online: https://www.unwomen.org/sites/default/files/Headquarters/Attachments/Sections/CSW/64/National-reviews/Equatorial%20Guinea.pdf (accessed on 1 September 2022).
- Ministerio de Sanidad y Bienestar Social de Guinea Ecuatorial (MINSAB). Encuesta Demográfica y de Salud (EDSGE-I). 2011. Available online: https://dhsprogram.com/pubs/pdf/fr271/fr271.pdf (accessed on 1 September 2022).
- UNICEF. Situación Social de los Menores Afectados Por el VIH/SIDA en Guinea Ecuatorial. 2019. Available online: https://www.unicef.org/equatorialguinea/media/666/file/menores-afectados-por-vihsida-portada-web.pdf (accessed on 1 September 2022).
- Joint United Nations Programme on HIV/AIDS (UNAIDS). AIDSinfo Web. Global Treatment Cascade. Special Analysis 2022. Available online: https://aidsinfo.unaids.org (accessed on 1 September 2022).
- Joint United Nations Programme on HIV/AIDS (UNAIDS). AIDSinfo Web. Treatment Cascade in West and Central Africa. Epidemiological Estimates 2022. Available online: https://aidsinfo.unaids.org (accessed on 1 September 2022).
- Bandera, A.; Gori, A.; Clerici, M.; Sironi, M. Phylogenies in ART: HIV reservoirs, HIV latency and drug resistance. Curr. Opin. Pharmacol. 2019, 48, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Clutter, D.S.; Jordan, M.R.; Bertagnolio, S.; Shafer, R.W. HIV-1 drug resistance and resistance testing. Infect. Genet. Evol. 2016, 46, 292–307. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.E.; Camacho, R.J.; Otelea, D.; Kuritzkes, D.R.; Fleury, H.; Kiuchi, M.; Heneine, W.; Kantor, R.; Jordan, M.R.; Schapiro, J.M. Drug resistance mutations for surveillance of transmitted HIV-1 drug-resistance: 2009 update. PLoS ONE 2009, 4, e4724. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). HIV Drug Resistance Surveillance Guidance. 2015 Update. Available online: https://apps.who.int/iris/handle/10665/204471 (accessed on 1 September 2022).
- World Health Organization (WHO). HIV Drug Resistance Report 2021. Technical Report. Available online: https://www.who.int/publications/i/item/9789240038608 (accessed on 1 September 2022).
- Salmanton-García, J.; Herrador, Z.; Ruiz-Seco, P.; Nzang-Esono, J.; Bendomo, V.; Bashmakovic, E.; Nseng-Nchama, G.; Benito, A.; Aparicio, P. Self-reported adherence to antiretroviral therapy in HIV+ population from Bata, Equatorial Guinea. AIDS Care 2016, 28, 543–553. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Updated Recommendations on First-Line and Second-Line Antiretroviral Regimens and Post-Exposure Prophylaxis and Recommendations on Early Infant Diagnosis of HIV: Interim Guidelines; Supplement to the 2016 Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/277395/WHO-CDS-HIV-18.51-eng.pdf?sequence=1&isAllowed=y (accessed on 1 September 2022).
- Ministerio de Sanidad y Bienestar Social de Guinea Ecuatorial (MINSAB). Guía Integrada Del uso de Antirretrovirales Para la Prevención y el Tratamiento de La infección VIH, 1st ed.; Ministerio de Sanidad y Bienestar Social de Guinea Ecuatorial (MINSAB): Malabo, Equatorial Guinea, 2018.
- Phillips, A.N.; Stover, J.; Cambiano, V.; Nakagawa, F.; Jordan, M.R.; Pillay, D.; Doherty, M.; Revill, P.; Bertagnolio, S. Impact of HIV Drug Resistance on HIV/AIDS-associated mortality, new infections, and antiretroviral therapy program costs in sub-Saharan Africa. J. Infect. Dis. 2017, 215, 1362–1365. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Action Plan on HIV Drug Resistance 2017–2021. 2017. Available online: https://www.who.int/publications/i/item/978-92-4-151284-8 (accessed on 1 September 2022).
- Sigaloff, K.C.; Calis, J.C.; Geelen, S.P.; van Vugt, M.; de Wit, T.F. HIV-1-resistance-associated mutations after failure of first-line antiretroviral treatment among children in resource-poor regions: A systematic review. Lancet Infect. Dis. 2011, 11, 769–779. [Google Scholar] [CrossRef]
- Hemelaar, J.; Elangovan, R.; Yun, J.; Dickson-Tetteh, L.; Fleminger, I.; Kirtley, S.; Williams, B.; Gouws-Williams, E.; Ghys, P.D.; WHO–UNAIDS Network for HIV Isolation Characterisation. Global and regional molecular epidemiology of HIV-1, 1990-2015: A systematic review, global survey, and trend analysis. Lancet Infect. Dis. 2019, 19, 143–155. [Google Scholar] [CrossRef]
- Geretti, A.M. HIV-1 subtypes: Epidemiology and significance for HIV management. Curr. Opin. Infect. Dis. 2006, 19, 1–7. [Google Scholar] [CrossRef]
- Troyano-Hernáez, P.; Reinosa, R.; Holguín, A. Genetic diversity and low therapeutic impact of variant-specific markers in HIV-1 pol proteins. Front. Microbiol. 2022, 13, 866705. [Google Scholar] [CrossRef]
- Theys, K.; Libin, P.J.K.; van Laethem, K.; Abecasis, A.B. An evolutionary model-based approach to quantify the genetic barrier to drug resistance in fast-evolving viruses and its application to HIV-1 subtypes and integrase inhibitors. Antimicrob. Agents Chemother. 2019, 63, e00539-19. [Google Scholar] [CrossRef]
- Martinez-Cajas, J.L.; Pai, N.P.; Klein, M.B.; Wainberg, M.A. Differences in resistance mutations among HIV-1 non-subtype B infections: A systematic review of evidence (1996–2008). J. Int. AIDS Soc. 2009, 12, 11. [Google Scholar] [CrossRef] [PubMed]
- Holguín, A.; Suñe, C.; Hamy, F.; Soriano, V.; Klimkait, T. Natural polymorphisms in the protease gene modulate the replicative capacity of non-B HIV-1 variants in the absence of drug pressure. J. Clin. Virol. 2006, 36, 264–271. [Google Scholar] [CrossRef]
- Holguín, A.; Ramirez de Arellano, E.; Rivas, P.; Soriano, V. Efficacy of antiretroviral therapy in individuals infected with HIV-1 non-B subtypes. AIDS Rev. 2006, 8, 98–107. [Google Scholar]
- Alvarez, P.; Martín, L.; Prieto, L.; Obiang, J.; Vargas, A.; Avedillo, P.; Rojo, P.; Fernández McPhee, C.; Benito, A.; Ramos, J.T.; et al. HIV-1 variability and viral load technique could lead to false positive HIV-1 detection and to erroneous viral quantification in infected specimens. J. Infect. 2015, 71, 368–376. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). WHO Manual for HIV Drug Resistance Testing Using Dried Blood Spot Specimens, 3rd ed.; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/9789240009424 (accessed on 1 September 2022).
- De Mulder, M.; Holguín, A. Dried blood spots for monitoring HIV infection in Public Health Programs in developing countries. Enferm. Infecc. Microbiol. Clín. 2013, 31, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, P.; Fernández McPhee, C.; Prieto, L.; Martín, L.; Obiang, J.; Avedillo, P.; Vargas, A.; Rojo, P.; Benito, A.; Ramos, J.T.; et al. HIV-1 variants and drug resistance in pregnant women from Bata (Equatorial Guinea): 2012-2013. PLoS ONE 2016, 11, e0165333. [Google Scholar] [CrossRef]
- Djoko, C.F.; Wolfe, N.D.; Vidal, N.; Tamoufe, U.; Montavon, C.; LeBreton, M.; Pike, B.L.; Fair, J.; Mbacham, W.F.; Benito, A.; et al. HIV type 1 pol gene diversity and genotypic antiretroviral drug resistance mutations in Malabo, Equatorial Guinea. AIDS Res. Hum. Retrovir. 2010, 26, 1027–1031. [Google Scholar] [CrossRef]
- Ortiz, M.; Sanchez, I.; Gonzalez, M.P.; León, M.I.; Abeso, N.; Asumu, E.; García-Sáiz, A. Molecular epidemiology of HIV type 1 subtypes in Equatorial Guinea. AIDS Res. Hum. Retrovir. 2001, 17, 851–855. [Google Scholar] [CrossRef]
- Yebra, G.; de Mulder, M.; Holguín, A. Description of HIV-1 group M molecular epidemiology and drug resistance prevalence in Equatorial Guinea from migrants in Spain. PLoS ONE 2013, 8, e64293. [Google Scholar] [CrossRef]
- Cepheid. Xpert® HIV-1 Qual. 2018. Available online: http://www.cepheid.com/en/cepheid-solutions/clinical-ivd-tests/virology/xpert-hiv-1-qual (accessed on 13 June 2022).
- Cepheid. Xpert® HIV-1 Viral Load. 2018. Available online: http://www.cepheid.com/en/cepheid-solutions/clinical-ivd-tests/virology/xpert-hiv-1-viralload (accessed on 13 June 2022).
- Rubio-Garrido, M.; Ndarabu, A.; Reina, G.; Barquín, D.; Fernández-Alonso, M.; Carlos, S.; Holguín, Á. Utility of POC Xpert HIV-1 Tests for detection-quantification of complex HIV recombinants using dried blood spots from Kinshasa, D.R.Congo. Sci. Rep. 2019, 9, 5679. [Google Scholar] [CrossRef]
- Mwinga, K.; Vermund, S.H.; Chen, Y.Q.; Mwatha, A.; Read, J.S.; Urassa, W.; Carpenetti, N.; Valentine, M.; Goldenberg, R.L. Selected hematologic and biochemical measurements in African HIV-infected and uninfected pregnant women and their infants: The HIV Prevention Trials Network 024 protocol. BMC Pediatr. 2009, 9, 49. [Google Scholar] [CrossRef] [PubMed]
- Robins, E.B.; Blum, S. Hematologic reference values for African American children and adolescents. Am. J. Hematol. 2007, 82, 611–614. [Google Scholar] [CrossRef] [PubMed]
- Billett, H.H. Hemoglobin and Hematocrit. In Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed.; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths: Boston, MA, USA, 1990; Chapter 151; ISBN 978-04-0990-077-4. [Google Scholar]
- Fernández McPhee, C.; Álvarez, P.; Prieto, L.; Obiang, J.; Avedillo, P.; Vargas, A.; Rojo, P.; Abad, C.; Ramos, J.T.; Holguín, A. HIV-1 infection using dried blood spots can be confirmed by Bio-Rad Geenius™ HIV 1/2 confirmatory assay. J. Clin. Virol. 2015, 63, 66–69. [Google Scholar] [CrossRef]
- France Recherche Nord & Sud Sida-HIV Hépatites (ANRS). ANRS AC11 Resistance Study Group PCR and Sequencing Procedures: HIV-1; National Agency for AIDS Research: Paris, France, 2015. [Google Scholar]
- Holguín, Á.; Yebra, G.; Martín, L.; de Pineda, A.T.; Ruiz, L.E.; Quezada, A.Y.; Nieto, A.I.; Escobar, G. Transmitted drug-resistance in human immunodeficiency virus-infected adult population in El Salvador, Central America. Clin. Microbiol. Infect. 2013, 19, e523–e532. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rubio-Garrido, M.; Reina, G.; Ndarabu, A.; Rodriguez-Galet, A.; Valadés-Alcaraz, A.; Barquín, D.; Carlos, S.; Holguín, Á. High drug resistance levels could compromise the control of HIV infection in paediatric and adolescent population in Kinshasa, the Democratic Republic of Congo. PLoS ONE 2021, 16, e0248835. [Google Scholar] [CrossRef]
- Tzou, P.L.; Rhee, S.Y.; Descamps, D.; Clutter, D.S.; Hare, B.; Mor, O.; Grude, M.; Parkin, N.; Jordan, M.R.; Bertagnolio, S.; et al. Integrase strand transfer inhibitor (INSTI)-resistance mutations for the surveillance of transmitted HIV-1 drug resistance. J. Antimicrob. Chemother. 2020, 75, 170–182. [Google Scholar] [CrossRef]
- Rubio-Garrido, M.; González-Alba, J.M.; Reina, G.; Ndarabu, A.; Barquín, D.; Carlos, S.; Galán, J.C.; Holguín, Á. Current and historic HIV-1 molecular epidemiology in paediatric and adult population from Kinshasa in the Democratic Republic of Congo. Sci. Rep. 2020, 10, 18461. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Guideline on When to Start Antiretroviral Therapy and on Pre-Exposure Prophylaxis for HIV. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/186275/9789241509565_eng.pdf (accessed on 1 September 2022).
- Joint United Nations Programme on HIV/AIDS (UNAIDS). AIDSinfo. Trend of AIDS-Related Deaths. Epidemilogical Estimates. 2022. Available online: https://aidsinfo.unaids.org/ (accessed on 1 September 2022).
- Joint United Nations Programme on HIV/AIDS (UNAIDS). AIDSinfo. Progress towards 95-95-95 Target. Special Analysis. 2022. Available online: https://aidsinfo.unaids.org/ (accessed on 1 September 2022).
- Robertson, M.M.; Braunstein, S.L.; Hoover, D.R.; Li, S.; Nash, D. Assessing linear CD4 decline quantifying diagnosis delay after HIV seroconversion: Assessing the linearity assumption of CD4 decline. Ann. Epidemiol. 2020, 52, 1–6. [Google Scholar] [CrossRef]
- Thanawuth, N.; Chongsuvivatwong, V. Late HIV diagnosis and delay in CD4 count measurement among HIV-infected patients in Southern Thailand. AIDS Care 2008, 20, 43–50. [Google Scholar] [CrossRef]
- Joint United Nations Programme on HIV/AIDS (UNAIDS). AIDSinfo. Treatment Cascade. Late Diagnosis in West and Central African Region. 2021. Available online: https://aidsinfo.unaids.org/ (accessed on 6 October 2022).
- Joint United Nations Programme on HIV/AIDS (UNAIDS). AIDSinfo. Vertical Transmission Rate in Equatorial Guinea (Data Sheet). 2021. Available online: https://www.unaids.org/en/regionscountries/countries/equatorialguinea (accessed on 6 October 2022).
- Urick, B.; Fong, Y.; Okiira, C.; Nabukeera-Barungi, N.; Nansera, D.; Ochola, E.; Nteziyaremye, J.; Bigira, V.; Ssewanyana, I.; Olupot-Olupot, P.; et al. Rapid serological test ineffectively screen for HIV exposure in HIV-positive infants. J. Acquir. Immune Defic. Syndr. 2018, 77, 331–336. [Google Scholar] [CrossRef]
- Joint United Nations Programme on HIV/AIDS (UNAIDS). AIDSinfo. Elimination of Vertical Transmission. Vertical Transmission rate in West and Central Africa (Data Sheet). 2021. Available online: https://aidsinfo.unaids.org/ (accessed on 6 October 2022).
- Newell, M.L.; Coovadia, H.; Cortina-Borja, M.; Rollins, N.; Gaillard, P.; Dabis, F.; Ghent International AIDS Society (IAS) Working Group on HIV Infection in Women and Children. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: A pooled analysis. Lancet 2004, 364, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Creek, T.; Tanuri, A.; Smith, M.; Seipone, K.; Smit, M.; Legwaila, K.; Motswere, C.; Maruping, M.; Nkoane, T.; Ntumy, R.; et al. Early diagnosis of human immunodeficiency virus in infants using polymerase chain reaction on dried blood spots in Botswana’s national program for prevention of mother-to-child transmission. Pediatr. Infect. Dis. J. 2008, 27, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Tato, L.M.; Vargas, A.; Álvarez, P.; Avedillo, P.; Nzi, E.; Abad, C.; Guillén, S.; FerThnández-McPhee, C.; Ramos, J.T.; Holguín, Á.; et al. Early diagnosis of human immunodeficiency virus-1 in infants: The prevention of mother-to-child transmission program in Equatorial Guinea. Enferm. Infecc. Microbiol. Clín. 2016, 34, 566–570. [Google Scholar] [CrossRef] [PubMed]
- The Global Alliance to End AIDS in Children by 2030. UNAIDS 2022. Available online: https://www.unaids.org/sites/default/files/media_asset/global-alliance-end-AIDS-in-children_en.pdf (accessed on 1 September 2022).
- Monitoring HIV Impact Using Population-Based Surveys. UNAIDS/WHO 2015. Available online: https://www.unaids.org/sites/default/files/media_asset/JC2763_PopulationBasedSurveys_en.pdf (accessed on 1 September 2022).
- Boerma, R.S.; Boender, T.S.; Bussink, A.P.; Calis, J.C.; Bertagnolio, S.; Rinke de Wit, T.F.; Boele van Hensbroek, M.; Sigaloff, K.C. Suboptimal Viral Suppression Rates Among HIV-Infected Children in Low- and Middle-Income Countries: A Meta-analysis. Clin. Infect. Dis. 2016, 63, 1645–1654. [Google Scholar] [CrossRef] [PubMed]
- Jenabian, M.A.; Costiniuk, C.T.; Mboumba Bouassa, R.S.; Chapdeleine Mekue Mouafo, L.; Brogan, T.V.; Bélec, L. Tackling virological failure in HIV-infected children living in Africa. Expert Rev. Anti-Infect. Ther. 2015, 13, 1213–1223. [Google Scholar] [CrossRef]
- Yeganeh, N.; Kerin, T.; Ank, B.; Watts, D.H.; Camarca, M.; Joao, E.C.; Pilotto, J.H.; Veloso, V.G.; Bryson, Y.; Gray, G.; et al. Human Immunodeficiency Virus Antiretroviral Resistance and Transmission in Mother-Infant Pairs Enrolled in a Large Perinatal Study. Clin. Infect. Dis. 2018, 66, 1770–1777. [Google Scholar] [CrossRef]
- Inzaule, S.C.; Osi, S.J.; Akinbiyi, G.; Emeka, A.; Khamofu, H.; Mpazanje, R.; Ilesanmi, O.; Ndembi, N.; Odafe, S.; Sigaloff, K.; et al. High prevalence of HIV drug resistance among newly diagnosed infants aged <18 months: Results from a nationwide surveillance in Nigeria. J. Acquir. Immune Defic. Syndr. 2018, 77, e1–e7. [Google Scholar] [CrossRef]
- Dourado de Andrade, S.; Sabidó, M.; Monteiro, W.M.; Benzaken, A.S.; Tanuri, A. Drug resistance in antiretroviral-naïve children newly diagnosed with HIV-1 in Manaus, Amazonas. J. Antimicrob. Chemother. 2017, 72, 1774–1783. [Google Scholar] [CrossRef]
- Scarsi, K.K.; Havens, J.P.; Podany, A.T.; Avedissian, S.N.; Fletcher, C.V. HIV-1 Integrase Inhibitors: A comparative review of efficacy and safety. Drugs 2020, 80, 1649–1676. [Google Scholar] [CrossRef]
- Turkova, A.; White, E.; Mujuru, H.A.; Kekitiinwa, A.R.; Kityo, C.M.; Violari, A.; Lugemwa, A.; Cressey, T.R.; Musoke, P.; Variava, E.; et al. Dolutegravir as first- or second-line treatment for HIV-1 infection in children. N. Engl. J. Med. 2021, 385, 2531–2543. [Google Scholar] [CrossRef]
- Kaleebu, P.; Ross, A.; Morgan, D.; Yirrell, D.; Oram, J.; Rutebemberwa, A.; Lyagoba, F.; Hamilton, L.; Biryahwaho, B.; Whitworth, J. Relationship between HIV-1 Env subtypes A and D and disease progression in a rural Ugandan cohort. Aids 2001, 15, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Araújo, L.A.; Junqueira, D.M.; de Medeiros, R.M.; Matte, M.C.; Almeida, S.E. Naturally occurring resistance mutations to HIV-1 entry inhibitors in subtypes B, C, and CRF31_BC. J. Clin. Virol. 2012, 54, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Joint United Nations Programme on HIV/AIDS (UNAIDS). Understanding Fast-Track: Accelerating Action to End the AIDS Epidemic by 2030. 2020. Available online: https://www.unaids.org/sites/default/files/media_asset/201506_JC2743_Understanding_FastTrack_en.pdf (accessed on 1 September 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | P Value | |||
|---|---|---|---|---|---|---|---|
| Epidemiological and Clinical Features | Children (<12 y) No. (%) | Adolescents (12 y–17 y) No. (%) | Adults (≥ 18 y) No. (%) | Total cohort No. (%) | 1 vs. 2 | 1 vs. 3 | 2 vs. 3 |
| Whole Study Cohort (n = 237) | |||||||
| Total | 40 (16.9) | 18 (7.6) | 179 (75.5) | 237 (100) | |||
| Female | 26 (65) | 9 (50) | 140 (78.2) | 175 (73.8) | ns | ns | * |
| Median age, years [range] | 6 (0.6–11) | 14 (12–17) | 34 (17–64) | 30 (0.6–64) | *** | *** | *** |
| Route of transmission | |||||||
| Vertical | 22 (55) | 6 (33.3) | 0 | 28 (11.9) | ns | *** | *** |
| Sexual | 0 | 0 | 102 (57) | 102 (43) | ns | *** | *** |
| Transfusion | 3 (7.5) | 2 (11.1) | 0 | 5 (2.1) | ns | * | * |
| Unknown | 15 (37.5) | 10 (55.6) | 77 (43) | 102 (43) | |||
| ARV exposure | |||||||
| Exposed/naïve | 2 (5) | 0 | 66 (36.9) | 68 (28.7) | ns | *** | ** |
| Under ART | 38 (95) | 18 (100) | 113 (63.1) | 169 (71.3) | ns | *** | ** |
| Delayed diagnosis | |||||||
| <200 cells/mm3 | 2 (5) | 3 (16.7) | 36 (20.1) | 41 (17.3) | ns | * | ns |
| >200 cells/mm3 | 23 (57.5) | 11 (61.1) | 92 (51.4) | 126 (53.2) | ns | * | ns |
| Unknown | 15 (37.5) | 4 (22.2) | 51 (28.5) | 70 (29.5) | |||
| Comorbidities | |||||||
| 0 | 11 (27.5) | 1 (5.5) | 3 (1.7) | 15 (6.3) | ns | *** | ns |
| 1 | 2 (5) | 3 (16.7) | 74 (41.3) | 79 (33.3) | ns | * | ns |
| 2 | 0 | 0 | 33 (18.4) | 33 (13.9) | ns | * | ns |
| 3 | 0 | 0 | 9 (5) | 9 (3.8) | ns | ns | ns |
| 4 | 0 | 0 | 1 (0.6) | 1 (0.5) | ns | ns | ns |
| Unknown | 27 (67.5) | 14 (77.8) | 59 (33) | 100 (42.2) | |||
| Subjects with available pol HIV-1 Sequence (n = 141) | 32 (80) | 13 (72.2) | 96 (53.6) | 141 (59.5) | |||
| PR | 29 (90.6) | 11 (84.6) | 91 (94.8) | 131 (92.9) | |||
| RT | 30 (93.8) | 10 (76.9) | 81 (84.4) | 121 (85.8) | |||
| IN | 24 (75) | 9 (69.2) | 64 (66.7) | 97 (68.8) | |||
| HIV-1 variants (n = 141) | |||||||
| Subtype B | 1 (3.1) | 0 | 0 | 1 (0.7) | ns | ns | ns |
| Non-B variants | 31 (96.9) | 13 (100) | 96 (100) | 140 (99.3) | ns | ns | ns |
| Art-Treated Patients at Sampling (n = 169) | |||||||
| HIV-1 viral load | |||||||
| <1000 cp/mL | 6 (15.8) | 2 (11.1) | 43 (38.1) | 51 (30.2) | ns | * | * |
| >1000 cp/mL | 32 (84.2) | 16 (88.9) | 70 (61.9) | 118 (69.8) | ns | * | * |
| Delayed ART | 5 (13.5) | 3 (17.6) | 16 (23.9) | 24 (19.8) | |||
| Immediate# | 32 (84.2) | 12 (66.6) | 37 (32.7) | 81 (47.9) | ns | * | ns |
| <1 year | 0 | 2 (11.1) | 14 (12.4) | 16 (9.5) | ns | * | ns |
| 1–3 years | 4 (10.6) | 1 (5.6) | 9 (8) | 14 (8.3) | ns | ns | ns |
| >3 years | 1 (2.6) | 2 (11.1) | 7 (6.2) | 10 (5.9) | ns | ns | ns |
| Unknown | 1 (2.6) | 1 (5.6) | 46 (40.7) | 48 (28.4) | |||
| Number of ART regimens at sampling | |||||||
| 1 | 15 (39.5) | 6 (33.3) | 26 (23) | 47 (27.8) | ns | ns | ns |
| 2 | 12 (31.6) | 5 (27.8) | 23 (20.4) | 40 (23.7) | ns | ns | ns |
| 3 | 8 (21) | 5 (27.8) | 18 (15.9) | 31 (18.4) | ns | ns | ns |
| 4 | 2 (5.3) | 2 (11.1) | 3 (2.7) | 7 (4.1) | ns | ns | ns |
| Unknown | 1 (2.6) | 0 | 43 (38) | 44 (26) | |||
| Median time under ART in 121 ‡ treated subjects, years [range] | 2.3 (0.1–9.9) | 3.3 (0.3–10.4) | 4.7 (0.1–15.5) | 3.6 (0.1–15.5) | ns | ns | ns |
| NRTI experience † | 37 (100) | 18 (100) | 70 (100) | 125 (100) | |||
| AZT | 37 (100) | 11 (61.1) | 24 (34.3) | 72 (57.6) | ** | *** | ns |
| 3TC | 36 (97.3) | 17 (94.4) | 65 (92.9) | 118 (94.4) | ns | ns | ns |
| TDF | 7 (18.9) | 15 (83.3) | 63 (90) | 85 (68) | *** | *** | ns |
| FTC | 1 (2.7) | 10 (55.6) | 26 (37.1) | 37 (29.6) | *** | *** | ns |
| D4T | 5 (13.5) | 3 (16.7) | 19 (27.1) | 27 (21.6) | ns | ns | ns |
| ABC | 3 (8.1) | 0 | 0 | 3 (2.4) | ns | * | ns |
| NNRTI experience † | 37 (100) | 15 (83.3) | 67 (95.7) | 119 (95.2) | * | ns | ns |
| EFV | 29 (78.4) | 13 (72.2) | 58 (82.9) | 100 (80) | ns | ns | ns |
| NVP | 26 (70.3) | 8 (44.4) | 29 (41.4) | 63 (50.4) | ns | * | ns |
| PI experience † | 3 (8.1) | 4 (22.2) | 13 (18.6) | 20 (16) | ns | ns | ns |
| LPV/r | 3 (8.1) | 4 (22.2) | 13 (18.6) | 20 (16) | ns | ns | ns |
| INSTI experience † | 2 (5.4) | 1 (5.6) | 25 (35.7) | 28 (22.4) | ns | * | * |
| DTG | 2 (5.4) | 1 (5.6) | 25 (35.7) | 28 (22.4) | ns | * | * |
| Mother-Child Pair | HIV-1 Variant | DRM to NRTI | DRM to NNRTI | Major-DRM to PI | DRM to INSTI | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mother | Child | Mother | Child | Mother | Child | Mother | Child | Mother | Child | |
| P1 | A3 | A3 | K70R M184V K219Q | M184V | K103N Y181C | K103N P225H | none | none | None | none |
| P2 | CRF02_AG | CRF02_AG | M41L | M41L | none | K103N | none | none | None | none |
| P3 | URF_02BA | CRF02_AG | A62V | M184V | none | K103N | none | none | None | --- |
| P4 | CRF37_cpx | CRF37_cpx | none | none | none | K103N | M46L | none | --- | none |
| P5 | CRF02_AG | G | none | M184V | K103N V108I | K103S G190A | none | none | --- | --- |
| P6 | CRF02_AG | CRF02_AG | M184V | none | K103N P225H | K103N V108I | none | none | T97A (minor) | --- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Galet, A.; Ventosa-Cubillo, J.; Bendomo, V.; Eyene, M.; Mikue-Owono, T.; Nzang, J.; Ncogo, P.; Gonzalez-Alba, J.M.; Benito, A.; Holguín, Á. High Drug Resistance Levels Compromise the Control of HIV Infection in Pediatric and Adult Populations in Bata, Equatorial Guinea. Viruses 2023, 15, 27. https://doi.org/10.3390/v15010027
Rodríguez-Galet A, Ventosa-Cubillo J, Bendomo V, Eyene M, Mikue-Owono T, Nzang J, Ncogo P, Gonzalez-Alba JM, Benito A, Holguín Á. High Drug Resistance Levels Compromise the Control of HIV Infection in Pediatric and Adult Populations in Bata, Equatorial Guinea. Viruses. 2023; 15(1):27. https://doi.org/10.3390/v15010027
Chicago/Turabian StyleRodríguez-Galet, Ana, Judit Ventosa-Cubillo, Verónica Bendomo, Manuel Eyene, Teresa Mikue-Owono, Jesús Nzang, Policarpo Ncogo, José María Gonzalez-Alba, Agustín Benito, and África Holguín. 2023. "High Drug Resistance Levels Compromise the Control of HIV Infection in Pediatric and Adult Populations in Bata, Equatorial Guinea" Viruses 15, no. 1: 27. https://doi.org/10.3390/v15010027
APA StyleRodríguez-Galet, A., Ventosa-Cubillo, J., Bendomo, V., Eyene, M., Mikue-Owono, T., Nzang, J., Ncogo, P., Gonzalez-Alba, J. M., Benito, A., & Holguín, Á. (2023). High Drug Resistance Levels Compromise the Control of HIV Infection in Pediatric and Adult Populations in Bata, Equatorial Guinea. Viruses, 15(1), 27. https://doi.org/10.3390/v15010027