
Short-Term Outcomes of Phage-Antibiotic Combination Treatment in Adult Patients with Periprosthetic Hip Joint Infection
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
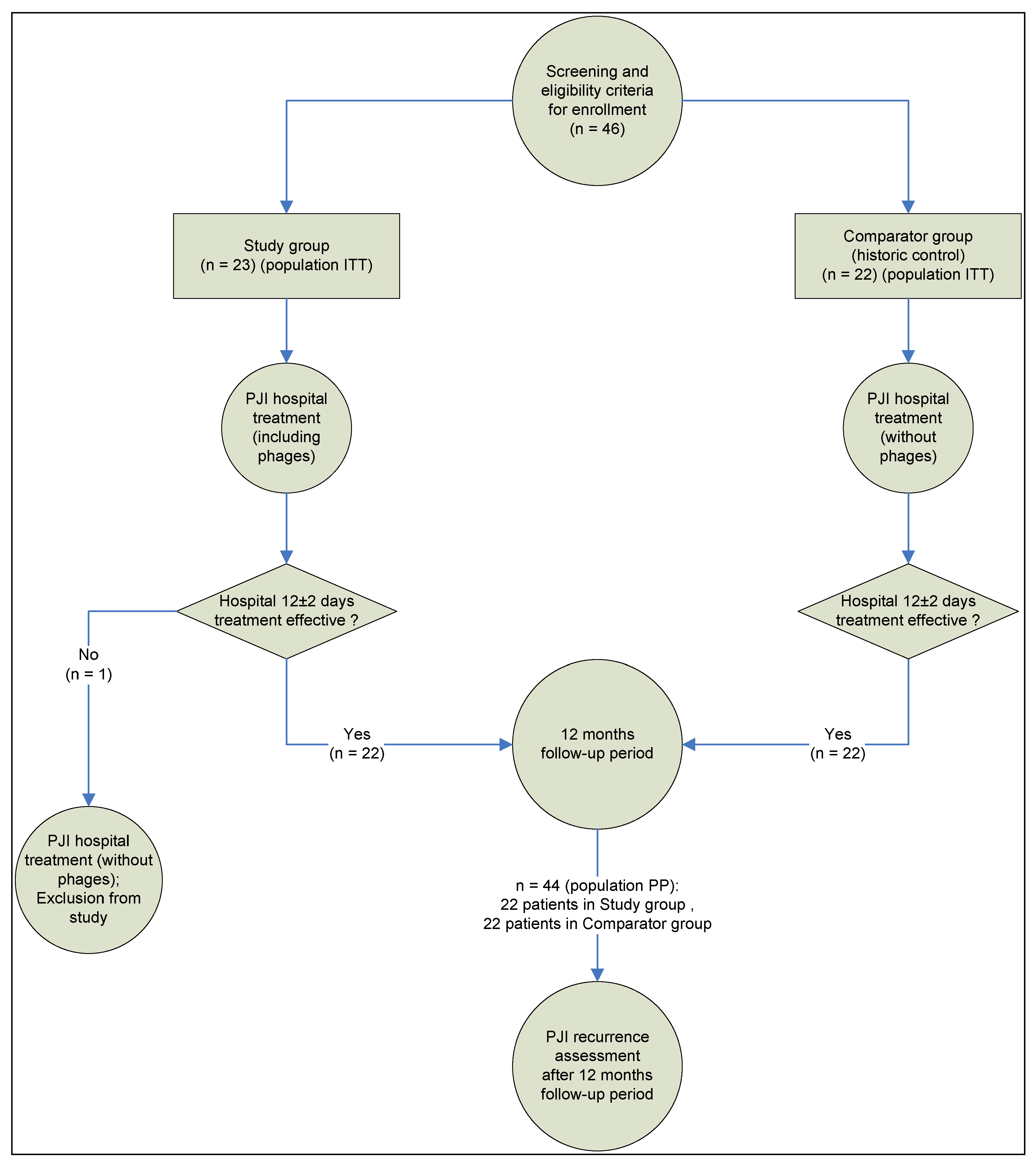
2.1. Study Design
2.2. Patients
- (1)
- Informed consent for surgical treatment.
- (2)
- Patients of any gender aged from 18 to 70 years.
- (3)
- Clinically and laboratory confirmed signs of early post-operative, late chronic, or acute hematogenous PJI, according to previously published classification [34], with the main signs of PJI according to the MSIS criteria [35]: a fistula communicating with the prosthesis; an identified pathogen (in this study, Staphylococcaceae) isolated by culture from two or more separate pre-operative punctures or intraoperative biopsies of periprosthetic tissues; and auxiliary criteria such as acute inflammation markers: an increased erythrocyte sedimentation rate (ESR) and an elevated serum C-reactive protein (CRP) concentration.
- (4)
- (5)
- (6)
- In vitro determined susceptibility of the isolated staphylococcus bacteria to a staphylococcal phage preparation with a titer of at least 104 plaque forming units/mL (PFU/mL).
- (7)
- Eligibility of the patient for the phage therapy protocol within the first ten days after revision surgery.
- (1)
- Patients under the age of 18 and over 70 years.
- (2)
- The absence of the main signs of PJI in the patient according to the MSIS criteria [35].
- (3)
- A lack of anatomical conditions for cemented endoprosthesis implantation (the possibility of cement pressurization): pronounced anatomical bone defects of the proximal femur type IIIA, IIIB, or IV according to Paprosky [36] and anatomical bone defects of the acetabulum type IIB, IIC, III, IIIA, or IIIB [37].
- (4)
- PJI of non-staphylococcal etiology.
- (5)
- Life-threatening conditions requiring urgent surgery before revision arthroplasty.
- (6)
- Lack of sensitivity of isolated Staphylococcus spp. to a staphylococcal phage preparation, defined as a bacteriophage titer of less than 104 PFU/mL, before revision arthroplasty.
- (1)
- Life-threatening conditions requiring urgent surgery within 12 ± 2 days after completed revision arthroplasty;
- (2)
- Lack of sensitivity of isolated staphylococcus bacteria to a staphylococcal phage preparation, defined as a bacteriophage titer less than 104 PFU/mL, after completed revision arthroplasty.
2.3. Surgical Treatment and Antibiotic Therapy Protocols
- Cefazolin at a dose of 2.0 g, three times a day for up to two weeks;
- Vancomycin at a dose of 1.0 g, twice a day for up to four weeks + daptomycin at a dose of 0.5 g, once a day for up to 3 weeks;
- Ciprofloxacin at a dose of 0.4 g, twice a day for up to four weeks;
- Cefazolin at a dose of 2.0 g, three times a day + daptomycin at a dose of 0.5 g, once a day for up to two weeks;
- Vancomycin at a dose of 1.0 g, twice a day for up to one week + cefazolin at a dose of 2.0 g, three times a day for up to three weeks;
- Vancomycin at a dose of 1.0 g, twice a day + rifampicin at a dose of 0.6 g, once a day for up to two weeks.
2.4. Phage Preparations
2.5. Original Protocol of Phage-Antibiotic Combination Therapy
- Ciprofloxacin at a dose of 0.5 g, twice a day for twenty-one days; and rifampicin at a dose of 450 mg, twice a day for ten weeks;
- Trimethoprim/sulfamethoxazole at a dose of 480 mg, twice a day for one month; then doxycycline at a dose of 100 mg, twice a day for eight weeks.
2.6. Evaluation of the Treatment Efficacy
- Bacteriological tests: detection and identification of the pathogen was carried out using bacteriological culture. As a study object, we used punctates (in the pre-operative period), biopsies from the inflammation site (open intra-operative biopsy), and wound fluid from drains (in the post-operative period). Microorganisms were identified using a “VITEK 2 Compact” automatic analyzer (Biomerieux, Craponne, France) or API® strips (Biomerieux, Craponne, France).
- Laboratory tests: all patients participating in the study underwent C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) tests, for laboratory monitoring of an infectious inflammatory process, on days 3 ± 1, 7 ± 1, and 12 ± 2 after surgery. CRP was evaluated with an immunoturbidimetric assay on an Integra Cobas 400 (Roche Diagnostics, Rotkreuz, Switzerland), ESR was evaluated by the Westergren method using an SRS/100II (Greiner Bio-One, Kremsmünster, Austria) automatic analyzer.
- Patient follow-up for PJI relapse: the treatment outcome of PJI was followed up for 12 months after surgery, and the discharge of patients from the hospital using physical examinations and phone interviews recorded as in-person and remote consultations. During surveying patients, their disease history was collected, with focus being placed on pain in the operated hip joint, temperature rises, edema, hyperemia of the post-operative scar or operated hip, possible prescription of antibiotic therapy to the patient, and revision surgery. The treatment efficacy was evaluated based on the rate of PJI relapse according to the criteria of surgical site infection: recovery from PJI considered as no PJI relapse within 12 months; no recovery from PJI considered as PJI relapse within 12 months.
2.7. Statistics
- (1)
- The odds ratio for the risk of PJI relapse within 12 months after surgery with one-stage treatment of PJI.
- (2)
- The contents of laboratory markers of the infectious and inflammatory processes (C-reactive protein and erythrocyte sedimentation rate) initially, and on days 3 ± 1, 7 ± 1, and 12 ± 2 after surgery.
- Null hypothesis, H0: p1 − p0 = 0
- Alternative hypothesis, Ha: p1 − p0 ≠ 0,
- (1)
- The expected response rate to treatment in the SG (based on our previously reported pilot results) [33]: 91.7% ≈ 91%.
- (2)
- (3)
- Power of the study: 80%.
- (4)
- Significance level: 1% (alpha = 0.1).
- (5)
- Patient number ratio between the groups: 1:1 (n0 = n1).
3. Results
3.1. Patients
3.2. Primary Endpoint Results
3.3. Secondary Endpoint Results
3.4. Microbiological Test Results
3.5. Adverse Events and Patients Withdrawal
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosteius, T.; Jansen, O.; Fehmer, T.; Baecker, H.; Citak, M.; Schildhauer, T.A.; Geßmann, J. Evaluating the Microbial Pattern of Periprosthetic Joint Infections of the Hip and Knee. J. Med. Microbiol. 2018, 67, 1608–1613. [Google Scholar] [CrossRef]
- Bozhkova, S.A.; Kasimova, A.R.; Tikhilov, R.M.; Polyakova, E.M.; Rukina, A.N.; Shabanova, V.V.; Liventsov, V.N. Adverse Trends in the Etiology of Orthopedic Infection: Results of 6-Year Monitoring of the Structure and Resistance of Leading Pathogens. Traumatol. Orthop. Russ. 2018, 24, 20–31. [Google Scholar] [CrossRef]
- Mullen, A.; Wieland, H.J.; Wieser, E.S.; Spannhake, E.W.; Marinos, R.S. Perioperative Participation of Orthopedic Patients and Surgical Staff in a Nasal Decolonization Intervention to Reduce Staphylococcus Spp Surgical Site Infections. Am. J. Infect. Control 2017, 45, 554–556. [Google Scholar] [CrossRef]
- Fink, B.; Schuster, P.; Braun, R.; Tagtalianidou, E.; Schlumberger, M. The Diagnostic Value of Routine Preliminary Biopsy in Diagnosing Late Prosthetic Joint Infection after Hip and Knee Arthroplasty. Bone Jt. J. 2020, 102-B, 329–335. [Google Scholar] [CrossRef]
- Pavlov, V.V.; Petrova, N.V.; Sheraliev, T.U. Two-Stage Treatment of Periprostetic Infection: Mid-Term Results. Traumatol. Orthop. Russ. 2019, 25, 109–116. [Google Scholar] [CrossRef]
- Antonelli, B.; Chen, A.F. Reducing the Risk of Infection after Total Joint Arthroplasty: Preoperative Optimization. Arthroplasty 2019, 1, 4. [Google Scholar] [CrossRef] [PubMed]
- Pichkhadze, I.M.; Kuz’menkov, K.A.; Zhadin, A.V.; Tsiskarashvili, A.V.; Pichkhadze, E.I.; Daneliya, L.M.; Rekvava, G.R.; Shulashov, B.N.; Pichkhadze, I.M.; Kuzmenkov, K.A.; et al. Treatment of Patients with Pyo-Inflammatory Complications after Hip Replacement. N.N. Priorov J. Traumatol. Orthop. 2009, 16, 45–50. [Google Scholar] [CrossRef]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-Joint Infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef]
- De la Fuente-Núñez, C.; Reffuveille, F.; Fernández, L.; Hancock, R.E. Bacterial Biofilm Development as a Multicellular Adaptation: Antibiotic Resistance and New Therapeutic Strategies. Curr. Opin. Microbiol. 2013, 16, 580–589. [Google Scholar] [CrossRef]
- Afinogenova, A.G. Microbial Biofilms of Wounds: Status of the Issue. Traumatol. Orthop. Russ. 2011, 17, 119–125. [Google Scholar] [CrossRef]
- Jaffe, D.; Costales, T.; Greenwell, P.; Christian, M.; Henn, R. Methicillin-Resistant Staphylococcus Aureus Infection Is a Risk Factor for Unplanned Return to the Operating Room in the Surgical Treatment of a Septic Knee. J. Knee Surg. 2017, 30, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Janz, V.; Trampuz, A.; Perka, C.F.; Wassilew, G.I. Reduced Culture Time and Improved Isolation Rate through Culture of Sonicate Fluid in Blood Culture Bottles. THC 2017, 25, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Kurd, M.F.; Ghanem, E.; Steinbrecher, J.; Parvizi, J. Two-Stage Exchange Knee Arthroplasty: Does Resistance of the Infecting Organism Influence the Outcome? Clin. Orthop. Relat. Res. 2010, 468, 2060–2066. [Google Scholar] [CrossRef] [PubMed]
- Leung, F.; Richards, C.J.; Garbuz, D.S.; Masri, B.A.; Duncan, C.P. Two-Stage Total Hip Arthroplasty: How Often Does It Control Methicillin-Resistant Infection? Clin. Orthop. Relat. Res. 2011, 469, 1009–1015. [Google Scholar] [CrossRef]
- Kuo, F.-C.; Yen, S.-H.; Peng, K.-T.; Wang, J.-W.; Lee, M.S. Methicillin-Resistant Staphylococcal Periprosthetic Joint Infections Can Be Effectively Controlled by Systemic and Local Daptomycin. BMC Infect. Dis. 2015, 16, 48. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-J.; Lee, M.S.; Lee, C.-H.; Lin, P.-C.; Kuo, F.-C. Daptomycin Treatment in Patients with Resistant Staphylococcal Periprosthetic Joint Infection. BMC Infect Dis. 2017, 17, 736. [Google Scholar] [CrossRef]
- Vlassov, V.V.; Tikunova, N.V.; Morozova, V.V. Bacteriophages as Therapeutic Preparations: What Restricts Their Application in Medicine. Biochemistry 2020, 85, 1587–1600. [Google Scholar] [CrossRef]
- Sillankorva, S.; Neubauer, P.; Azeredo, J. Phage Control of Dual Species Biofilms of Pseudomonas Fluorescens and Staphylococcus Lentus. Biofouling 2010, 26, 567–575. [Google Scholar] [CrossRef]
- Sillankorva, S.; Oliveira, R.; Vieira, M.J.; Azeredo, J. Real-Time Quantification of Pseudomonas Fluorescens Cell Removal from Glass Surfaces Due to Bacteriophage ΦS1 Application. J. Appl. Microbiol. 2008, 105, 196–202. [Google Scholar] [CrossRef]
- Hanlon, G.W.; Denyer, S.P.; Olliff, C.J.; Ibrahim, L.J. Reduction in Exopolysaccharide Viscosity as an Aid to Bacteriophage Penetration through Pseudomonas Aeruginosa Biofilms. Appl. Environ. Microbiol. 2001, 67, 2746–2753. [Google Scholar] [CrossRef] [Green Version]
- Hughes, K.A.; Sutherland, I.W.; Clark, J.; Jones, M.V. Bacteriophage and Associated Polysaccharide Depolymerases—Novel Tools for Study of Bacterial Biofilms. J. Appl. Microbiol. 1998, 85, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.A.; Sutherland, I.W.; Jones, M.V. Biofilm Susceptibility to Bacteriophage Attack: The Role of Phage-Borne Polysaccharide Depolymerase. Microbiology 1998, 144, 3039–3047. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, I.W.; Hughes, K.A.; Skillman, L.C.; Tait, K. The Interaction of Phage and Biofilms. FEMS Microbiol. Lett. 2004, 232, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.K.; Collins, J.J. Dispersing Biofilms with Engineered Enzymatic Bacteriophage. Proc. Natl. Acad. Sci. USA 2007, 104, 11197–11202. [Google Scholar] [CrossRef]
- Tkhilaishvili, T.; Wang, L.; Tavanti, A.; Trampuz, A.; Di Luca, M. Antibacterial Efficacy of Two Commercially Available Bacteriophage Formulations, Staphylococcal Bacteriophage and PYO Bacteriophage, Against Methicillin-Resistant Staphylococcus Aureus: Prevention and Eradication of Biofilm Formation and Control of a Systemic Infection of Galleria Mellonella Larvae. Front. Microbiol. 2020, 11, 110. [Google Scholar] [CrossRef] [PubMed]
- Clarke, A.; De Soir, S.; Jones, J. The Safety and Efficacy of Phage Therapy for Bone and Joint Infections: A Systematic Review. Antibiotics 2020, 9, 795. [Google Scholar] [CrossRef]
- Walter, N.; Deng, L.; Brochhausen, C.; Alt, V.; Rupp, M. Behandlung von Knochen- und Protheseninfektionen mit Bakteriophagen: Ein systematisches Review. Orthopäde 2022, 51, 138–145. [Google Scholar] [CrossRef]
- Międzybrodzki, R.; Borysowski, J.; Weber-Dąbrowska, B.; Fortuna, W.; Letkiewicz, S.; Szufnarowski, K.; Pawełczyk, Z.; Rogóż, P.; Kłak, M.; Wojtasik, E.; et al. Clinical Aspects of Phage Therapy. In Advances in Virus Research; Elsevier: Amsterdam, The Netherlands, 2012; Volume 83, pp. 73–121. ISBN 978-0-12-394438-2. [Google Scholar]
- Ferry, T.; Boucher, F.; Fevre, C.; Perpoint, T.; Chateau, J.; Petitjean, C.; Josse, J.; Chidiac, C.; L’hostis, G.; Leboucher, G.; et al. Innovations for the Treatment of a Complex Bone and Joint Infection Due to XDR Pseudomonas Aeruginosa Including Local Application of a Selected Cocktail of Bacteriophages. J. Antimicrob. Chemother. 2018, 73, 2901–2903. [Google Scholar] [CrossRef] [PubMed]
- Rogóż, P.; Amanatullah, D.F.; Międzybrodzki, R.; Manasherob, R.; Tikunova, N.V.; Weber-Dąbrowska, B.; Fortuna, W.; Letkiewicz, S.; Górski, A. Phage Therapy in Orthopaedic Implant-Associated Infections. In Phage Therapy: A Practical Approach; Górski, A., Międzybrodzki, R., Borysowski, J., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 189–211. ISBN 978-3-030-26735-3. [Google Scholar]
- Patey, O.; McCallin, S.; Mazure, H.; Liddle, M.; Smithyman, A.; Dublanchet, A. Clinical Indications and Compassionate Use of Phage Therapy: Personal Experience and Literature Review with a Focus on Osteoarticular Infections. Viruses 2018, 11, 18. [Google Scholar] [CrossRef]
- Doub, J.B.; Ng, V.Y.; Johnson, A.J.; Slomka, M.; Fackler, J.; Horne, B.; Brownstein, M.J.; Henry, M.; Malagon, F.; Biswas, B. Salvage Bacteriophage Therapy for a Chronic MRSA Prosthetic Joint Infection. Antibiotics 2020, 9, 241. [Google Scholar] [CrossRef]
- Samokhin, A.G.; Fedorov, E.A.; Kozlova, Y.N.; Tikunova, N.V.; Pavlov, V.V.; Morozova, V.V.; Kretien, S.O. Application of the Lytic Bacteriophages during Surgical Treatment of the Periprosthetic Infection of the Hip Joint Endoprosthesis (Pilot Study). MPSE 2016, 6. [Google Scholar] [CrossRef]
- Tsukayama, D.T.; Estrada, R.; Gustilo, R.B. Infection after Total Hip Arthroplasty. A Study of the Treatment of One Hundred and Six Infections*. J. Bone Jt. Surg. 1996, 78, 512–523. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New Definition for Periprosthetic Joint Infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. Relat. Res. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [PubMed]
- Paprosky, W.; Lawrence, J.; Cameron, H. Femoral Defect Classification: Clinical Application. Orthop. Rev. 1990, 19, 9–17. [Google Scholar]
- Paprosky, W.G.; Perona, P.G.; Lawrence, J.M. Acetabular Defect Classification and Surgical Reconstruction in Revision Arthroplasty. J. Arthroplast. 1994, 9, 33–44. [Google Scholar] [CrossRef]
- Parvizi, J.; Gehrke, T.; Chen, A.F. Proceedings of the International Consensus on Periprosthetic Joint Infection. Bone Jt. J. 2013, 95-B, 1450–1452. [Google Scholar] [CrossRef]
- Parvizi, J.; Fassihi, S.C.; Enayatollahi, M.A. Diagnosis of Periprosthetic Joint Infection Following Hip and Knee Arthroplasty. Orthop. Clin. N. Am. 2016, 47, 505–515. [Google Scholar] [CrossRef]
- Kutter, E. Phage Host Range and Efficiency of Plating. In Bacteriophages; Clokie, M.R.J., Kropinski, A.M., Eds.; Methods in Molecular Biology; Humana Press: Totowa, NJ, USA, 2009; Volume 501, pp. 141–149. ISBN 978-1-58829-682-5. [Google Scholar]
- Samokhin, A.G.; Kozlova, J.N.; Korneev, D.V.; Taranov, O.S.; Fedorov, E.A.; Pavlov, V.V.; Morozova, V.V.; Tikunova, N.V. Experimental Study of the Antibacterial Activity of the Lytic Staphylococcus Aureus Bacteriophage Ph20 and Lytic Pseudomonas Aeruginosa Bacteriophage Ph57 during Modelling of Its Impregnation into Poly(Methylmetacrylate) Orthopedic Implants (Bone Cement). Ann. RAMS 2018, 73, 59–68. [Google Scholar] [CrossRef]
- Pavlov, V.V.; Samokhin, A.G.; Fedorov, E.A.; Prokhorenko, V.M.; Kretien, S.O.; Kozlova, Y.N.; Tikunova, N.V.; Morozova, V.V. Method of Evaluating Efficiency of Phagotherapy in Treatment of Infections Diseases. Patent RU2624511C1. Available online: https://patents.google.com/patent/RU2624511C1/en (accessed on 6 December 2022).
- Appelmans, R. Le Dosage Du Bacteriophage. Compt. Rend. Soc. Biol. 1921, 1098, 701. [Google Scholar]
- Renz, N.; Trampuz, A. Pocket Guide to Diagnosis & Treatment of Periprosthetic Joint Infection; PRO-IMPLANT Foundation: Berlin, Germany, 2015; Available online: https://pro-implant.org/tools/pocket-guide/1 (accessed on 6 December 2022).
- Newcombe, R.G. Two-Sided Confidence Intervals for the Single Proportion: Comparison of Seven Methods. Statist. Med. 1998, 17, 857–872. [Google Scholar] [CrossRef]
- Wilson, E.B. Probable Inference, the Law of Succession, and Statistical Inference. J. Am. Stat. Assoc. 1927, 22, 209–212. [Google Scholar] [CrossRef]
- Chow, S.-C.; Shao, J.; Wang, H.; Lokhnygina, Y. (Eds.) Sample Size Calculations in Clinical Research. In Chapman & Hall/CRC Biostatistics Series, 3rd ed.; Taylor & Francis: Boca Raton, FL, USA, 2017; p. 492. ISBN 978-1-138-74098-3. [Google Scholar]
- Lora-Tamayo, J.; Euba, G.; Cobo, J.; Horcajada, J.P.; Soriano, A.; Sandoval, E.; Pigrau, C.; Benito, N.; Falgueras, L.; Palomino, J.; et al. Short- versus Long-Duration Levofloxacin plus Rifampicin for Acute Staphylococcal Prosthetic Joint Infection Managed with Implant Retention: A Randomised Clinical Trial. Int. J. Antimicrob. Agents 2016, 48, 310–316. [Google Scholar] [CrossRef]
- Byren, I.; Rege, S.; Campanaro, E.; Yankelev, S.; Anastasiou, D.; Kuropatkin, G.; Evans, R. Randomized Controlled Trial of the Safety and Efficacy of Daptomycin versus Standard-of-Care Therapy for Management of Patients with Osteomyelitis Associated with Prosthetic Devices Undergoing Two-Stage Revision Arthroplasty. Antimicrob. Agents Chemother. 2012, 56, 5626–5632. [Google Scholar] [CrossRef]
- Ferry, T.; Kolenda, C.; Batailler, C.; Gustave, C.-A.; Lustig, S.; Malatray, M.; Fevre, C.; Josse, J.; Petitjean, C.; Chidiac, C.; et al. Phage Therapy as Adjuvant to Conservative Surgery and Antibiotics to Salvage Patients With Relapsing S. Aureus Prosthetic Knee Infection. Front. Med. 2020, 7, 570572. [Google Scholar] [CrossRef] [PubMed]
- Ferry, T.; Batailler, C.; Petitjean, C.; Chateau, J.; Fevre, C.; Forestier, E.; Brosset, S.; Leboucher, G.; Kolenda, C.; Laurent, F.; et al. The Potential Innovative Use of Bacteriophages Within the DAC® Hydrogel to Treat Patients With Knee Megaprosthesis Infection Requiring “Debridement Antibiotics and Implant Retention” and Soft Tissue Coverage as Salvage Therapy. Front. Med. 2020, 7, 342. [Google Scholar] [CrossRef] [PubMed]
- Vogt, D.; Sperling, S.; Tkhilaishvili, T.; Trampuz, A.; Pirnay, J.-P.; Willy, C. „Beyond antibiotic therapy“—Zukünftige antiinfektiöse Strategien—Update 2017. Unfallchirurg 2017, 120, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Jurado, R.L. Why Shouldn’t We Determine the Erythrocyte Sedimentation Rate? Clin. Infect. Dis. 2001, 33, 548–549. [Google Scholar] [CrossRef] [PubMed]
- Torres-Barceló, C.; Arias-Sánchez, F.I.; Vasse, M.; Ramsayer, J.; Kaltz, O.; Hochberg, M.E. A Window of Opportunity to Control the Bacterial Pathogen Pseudomonas Aeruginosa Combining Antibiotics and Phages. PLoS ONE 2014, 9, e106628. [Google Scholar] [CrossRef] [PubMed]
- Torres-Barceló, C.; Hochberg, M.E. Evolutionary Rationale for Phages as Complements of Antibiotics. Trends Microbiol. 2016, 24, 249–256. [Google Scholar] [CrossRef]
- Diallo, K.; Dublanchet, A. Benefits of Combined Phage–Antibiotic Therapy for the Control of Antibiotic-Resistant Bacteria: A Literature Review. Antibiotics 2022, 11, 839. [Google Scholar] [CrossRef]
- Tait, K.; Skillman, L.C.; Sutherland, I.W. The Efficacy of Bacteriophage as a Method of Biofilm Eradication. Biofouling 2002, 18, 305–311. [Google Scholar] [CrossRef]
- Chaudhry, W.N.; Concepción-Acevedo, J.; Park, T.; Andleeb, S.; Bull, J.J.; Levin, B.R. Synergy and Order Effects of Antibiotics and Phages in Killing Pseudomonas Aeruginosa Biofilms. PLoS ONE 2017, 12, e0168615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumaran, D.; Taha, M.; Yi, Q.; Ramirez-Arcos, S.; Diallo, J.-S.; Carli, A.; Abdelbary, H. Does Treatment Order Matter? Investigating the Ability of Bacteriophage to Augment Antibiotic Activity against Staphylococcus Aureus Biofilms. Front. Microbiol. 2018, 9, 127. [Google Scholar] [CrossRef] [PubMed]
- Tkhilaishvili, T.; Winkler, T.; Müller, M.; Perka, C.; Trampuz, A. Bacteriophages as Adjuvant to Antibiotics for the Treatment of Periprosthetic Joint Infection Caused by Multidrug-Resistant Pseudomonas Aeruginosa. Antimicrob. Agents Chemother. 2019, 64, e00924-19. [Google Scholar] [CrossRef]
- Necel, A.; Bloch, S.; Topka-Bielecka, G.; Janiszewska, A.; Łukasiak, A.; Nejman-Faleńczyk, B.; Węgrzyn, G. Synergistic Effects of Bacteriophage VB_Eco4-M7 and Selected Antibiotics on the Biofilm Formed by Shiga Toxin-Producing Escherichia Coli. Antibiotics 2022, 11, 712. [Google Scholar] [CrossRef]
- Łusiak-Szelachowska, M.; Weber-Dąbrowska, B.; Górski, A. Bacteriophages and Lysins in Biofilm Control. Virol. Sin. 2020, 35, 125–133. [Google Scholar] [CrossRef]
- Tkhilaishvili, T.; Lombardi, L.; Klatt, A.-B.; Trampuz, A.; Di Luca, M. Bacteriophage Sb-1 Enhances Antibiotic Activity against Biofilm, Degrades Exopolysaccharide Matrix and Targets Persisters of Staphylococcus Aureus. Int. J. Antimicrob. Agents 2018, 52, 842–853. [Google Scholar] [CrossRef]
- Das, A.K. Randomised Clinical Trials in Surgery: A Look at the Ethical and Practical Issues. Indian J. Surg. 2011, 73, 245–250. [Google Scholar] [CrossRef]
- Savulescu, J.; Wartolowska, K.; Carr, A. Randomised Placebo-Controlled Trials of Surgery: Ethical Analysis and Guidelines. J. Med. Ethics 2016, 42, 776–783. [Google Scholar] [CrossRef]
- Cooper, J.D. Randomized Clinical Trials for New Surgical Operations: Square Peg in a Round Hole? J. Thorac. Cardiovasc. Surg. 2010, 140, 743–746. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Groups | Early Post-Operative Infection | Late Chronic Infection | Acute Hematogenous Infection |
|---|---|---|---|
| Study group (n = 23) | 5 | 13 | 5 |
| Comparator group (n = 22) | 6 | 12 | 4 |
| Patient Groups | Number of Patients, n (%) | |||||
|---|---|---|---|---|---|---|
| S. epidermidis (MSSE) | S. epidermidis (MRSE) | S. aureus (MSSA) | S. haemolyticus (MSSH) | S. aureus (MRSA) | Total per Group | |
| Study group (SG) | 8 (34.8%) | 6 (26.1%) | 8 (34.8%) | 0 (0.0%) | 1 (4.3%) | 23 (100.0%) |
| Comparator group (CG) | 4 (18.2%) | 3 (13.6%) | 13 (59.1%) | 2 (9.1%) | 0 (0.0%) | 22 (100.0%) |
| Total | 12 (26.7%) | 9 (20.0%) | 21 (46.7%) | 2 (4.4%) | 1 (2.2%) | 45 (100.0%) |
| Patient Groups | Total | |||
|---|---|---|---|---|
| Study Group | Comparator Group | |||
| PJI relapse within 12 months | No | 21 (95.5%) | 14 (63.6%) | 35 (79.5%) |
| Yes | 1 (4.5%) | 8 (36.4%) | 9 (20.5%) | |
| Total | 22 (100%) | 22 (100%) | 44 (100%) | |
| Value | 95% Confidence Interval | ||
|---|---|---|---|
| Lower Bound | Upper Bound | ||
| Odds Ratio for PJI relapse within 12 months (Yes/No) | 0.083 | 0.009 | 0.742 |
| Relative risk for PJI relapse within 12 months (SG) | 0.185 | 0.029 | 1.199 |
| Relative risk for PJI relapse within 12 months (CG) | 2.222 | 1.393 | 3.545 |
| Number of Valid Cases | 44 | ||
| Mean | Standard Deviation | Maximum | Minimum | Median | Percentile 25 | Percentile 75 | Number of Patients | ||
|---|---|---|---|---|---|---|---|---|---|
| Baseline CRP | SG | 43.5 | 43.95 | 167.45 | 3.19 | 29.8 | 13.62 | 56.40 | 23 |
| CG | 37.7 | 44.35 | 196.08 | 1.60 | 24.6 | 14.84 | 36.78 | 22 | |
| CRP on day 3 ± 1 | SG | 104.9 | 59.65 | 236.70 | 22.38 | 86.8 | 57.99 | 158.66 | 23 |
| CG | 57.5 | 30.32 | 124.21 | 22.76 | 44.1 | 34.40 | 69.32 | 22 | |
| CRP on day 7 ± 1 | SG | 45.3 | 24.95 | 87.45 | 8.44 | 45.5 | 20.57 | 56.75 | 22 |
| CG | 42.8 | 49.61 | 162.44 | 4.02 | 23.5 | 10.82 | 53.44 | 22 | |
| CRP on day 12 ± 2 | SG | 21.4 | 12.86 | 46.75 | 1.95 | 17.2 | 13.61 | 28.85 | 22 |
| CG | 39.9 | 60.02 | 250.56 | 1.97 | 16.0 | 9.06 | 46.22 | 22 | |
| Baseline ESR | SG | 56.6 | 28.36 | 101 | 2 | 54.0 | 34.00 | 82.00 | 23 |
| CG | 44.2 | 33.49 | 115 | 5 | 39.0 | 16.00 | 65.00 | 22 | |
| ESR on day 3 ± 1 | SG | 74.2 | 24.91 | 116 | 37 | 82.0 | 49.00 | 95.00 | 23 |
| CG | 47.3 | 25.31 | 107 | 14 | 42.0 | 28.00 | 59.00 | 22 | |
| ESR on day 7 ± 1 | SG | 82.2 | 17.77 | 109 | 40 | 85.0 | 75.00 | 96.00 | 22 |
| CG | 52.3 | 30.10 | 127 | 14 | 47.0 | 30.00 | 65.00 | 22 | |
| ESR on day 12 ± 2 | SG | 70.4 | 18.21 | 101 | 31 | 70.5 | 62.00 | 82.00 | 22 |
| CG | 47.9 | 26.17 | 108 | 11 | 41.0 | 32.00 | 60.00 | 22 | |
| Patient Number | Pathogen in Wound Fluid on Day 4 ± 1 (Yes/No) | Identified Pathogen | Phage Titer |
|---|---|---|---|
| 89457 | No | 1.8 × 102 PFU/mL | |
| 89730 | No | 2.1 × 102 PFU/mL | |
| 89866 | No | 2.3 × 103 PFU/mL | |
| 90491 | No | 1.9 × 104 PFU/mL | |
| 90783 | No | 1.8 × 103 PFU/mL | |
| 87408 | No | 2.2 × 102 PFU/mL | |
| 90660 | No | 2.3 × 102 PFU/mL | |
| 94252 | No | 1.7 × 104 PFU/mL | |
| 93001 | No | 2.8 × 103 PFU/mL | |
| 95127 | No | 1.8 × 104 PFU/mL | |
| 96583 | No | 2.1 × 102 PFU/mL | |
| 97182 | Yes | MRSE and P. mirabilis | 0 (zero) PFU/mL |
| 97604 | No | 1.6 × 103 PFU/mL | |
| 92082 | No | 2.1 × 103 PFU/mL | |
| 85770 | No | 1.9 × 104 PFU/mL | |
| 29765 | No | 2.4 × 102 PFU/mL | |
| 78175 | No | 2.2 × 102 PFU/mL | |
| 86917 | No | 1.8 × 103 PFU/mL | |
| 107497 | No | 1.7 × 103 PFU/mL | |
| 86966 | No | 1.9 × 102 PFU/mL | |
| 108819 | No | 2.1 × 104 PFU/mL | |
| 116277 | No | 1.8 × 103 PFU/mL | |
| 116463 | No | 2.3 × 102 PFU/mL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fedorov, E.; Samokhin, A.; Kozlova, Y.; Kretien, S.; Sheraliev, T.; Morozova, V.; Tikunova, N.; Kiselev, A.; Pavlov, V. Short-Term Outcomes of Phage-Antibiotic Combination Treatment in Adult Patients with Periprosthetic Hip Joint Infection. Viruses 2023, 15, 499. https://doi.org/10.3390/v15020499
Fedorov E, Samokhin A, Kozlova Y, Kretien S, Sheraliev T, Morozova V, Tikunova N, Kiselev A, Pavlov V. Short-Term Outcomes of Phage-Antibiotic Combination Treatment in Adult Patients with Periprosthetic Hip Joint Infection. Viruses. 2023; 15(2):499. https://doi.org/10.3390/v15020499
Chicago/Turabian StyleFedorov, Eugeny, Alexander Samokhin, Yulia Kozlova, Svetlana Kretien, Taalai Sheraliev, Vera Morozova, Nina Tikunova, Alexey Kiselev, and Vitaliy Pavlov. 2023. "Short-Term Outcomes of Phage-Antibiotic Combination Treatment in Adult Patients with Periprosthetic Hip Joint Infection" Viruses 15, no. 2: 499. https://doi.org/10.3390/v15020499