
Human Papillomavirus Infections and Increased Risk of Incident Osteoporosis: A Nationwide Population-Based Cohort Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Primary Endpoint and Covariates
2.4. Statistical Analysis
3. Results
3.1. Basline Characteristics of Study Populations
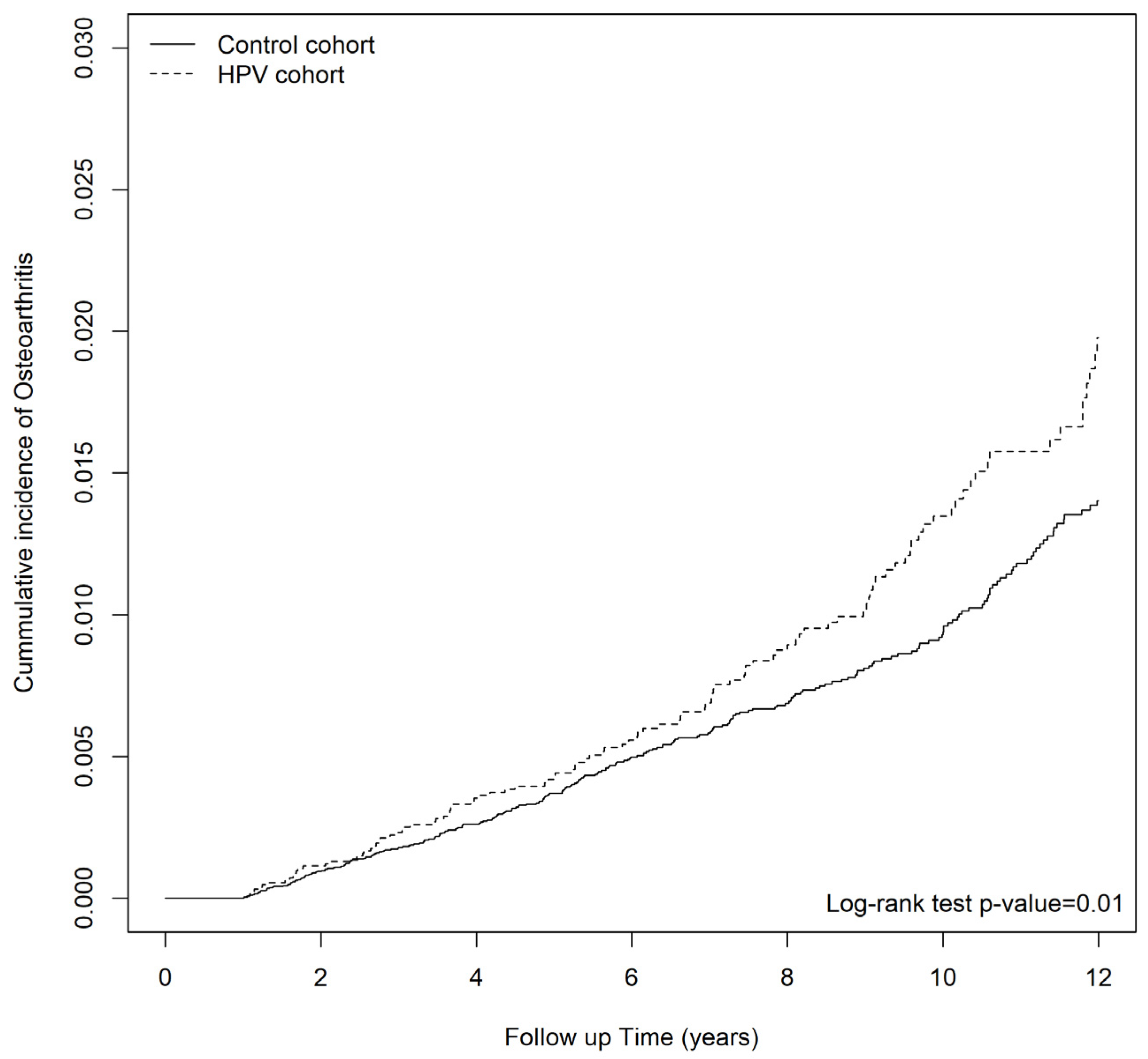
3.2. Incidence of Osteoporosis in Patients with HPV Infections
3.3. Factors Associated with HPV-Associated Osteoporosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sözen, T.; Özışık, L.; Başaran, N. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef]
- Sornay-Rendu, E.; Munoz, F.; Garnero, P.; Duboeuf, F.; Delmas, P.D. Identification of osteopenic women at high risk of fracture: The OFELY study. J. Bone Miner. Res. 2005, 20, 1813–1819. [Google Scholar] [CrossRef]
- Szulc, P.; Munoz, F.; Duboeuf, F.; Marchand, F.; Delmas, P.D. Bone mineral density predicts osteoporotic fractures in elderly men: The MINOS study. Osteoporos. Int. 2005, 16, 1184–1192. [Google Scholar] [CrossRef]
- Brainsky, A.; Glick, H.; Lydick, E.; Epstein, R.; Fox, K.M.; Hawkes, W.; Kashner, T.M.; Zimmerman, S.I.; Magaziner, J. The economic cost of hip fractures in community-dwelling older adults: A prospective study. J. Am. Geriatr. Soc. 1997, 45, 281–287. [Google Scholar] [CrossRef]
- Moradi, S.; Shab-Bidar, S.; Alizadeh, S.; Djafarian, K. Association between sleep duration and osteoporosis risk in middle-aged and elderly women: A systematic review and meta-analysis of observational studies. Metabolism 2017, 69, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.H.; Liu, W.W.; Tsao, C.H.; Ma, K.S. Obstructive sleep apnea in patients with rheumatoid arthritis: The multidisciplinary approach and multidimensional assessment. Int. J. Rheum. Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.H.; Lee, Y.T.; Ma, K.S. Corticosteroids and disease-modifying antirheumatic drugs for coronavirus disease 2019 in patients with rheumatoid arthritis. Int. J. Rheum. Dis. 2023. [Google Scholar] [CrossRef]
- Melton, L.J., 3rd; Atkinson, E.J.; O’Connor, M.K.; O’Fallon, W.M.; Riggs, B.L. Bone density and fracture risk in men. J. Bone Miner. Res. 1998, 13, 1915–1923. [Google Scholar] [CrossRef] [PubMed]
- Ginaldi, L.; De Martinis, M. Osteoimmunology and Beyond. Curr. Med. Chem. 2016, 23, 3754–3774. [Google Scholar] [CrossRef]
- Biver, E.; Calmy, A.; Rizzoli, R. Bone health in HIV and hepatitis B or C infections. Ther. Adv. Musculoskelet. Dis. 2017, 9, 22–34. [Google Scholar] [CrossRef]
- Chen, C.H.; Lin, C.L.; Kao, C.H. Association Between Chronic Hepatitis B Virus Infection and Risk of Osteoporosis: A Nationwide Population-Based Study. Medicine 2015, 94, e2276. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.M.; Wang, C.Y.; Chen, Y.Y.; Wang, J.H.; Liang, C.C.; Huang, H.K. Herpes zoster and the risks of osteoporosis and fracture: A nationwide cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Qiao, W.; Lau, H.E.; Xie, H.; Poon, V.K.-M.; Chan, C.C.-S.; Chu, H.; Yuan, S.; Yuen, T.T.-T.; Chik, K.K.-H.; Tsang, J.O.-L.; et al. Author Correction: SARS-CoV-2 infection induces inflammatory bone loss in golden Syrian hamsters. Nat. Commun. 2022, 13, 3139. [Google Scholar] [CrossRef]
- Ma, K.S.-K.; Lee, C.-C.; Liu, K.-J.; Wei, J.C.-C.; Lee, Y.-T.; Wang, L.-T. Safety and Seroconversion of Immunotherapies against SARS-CoV-2 Infection: A Systematic Review and Meta-Analysis of Clinical Trials. Pathogens 2021, 10, 1537. [Google Scholar] [CrossRef] [PubMed]
- Weinstock, H.; Berman, S.; Cates, W., Jr. Sexually transmitted diseases among American youth: Incidence and prevalence estimates, 2000. Perspect. Sex. Reprod. Health 2004, 36, 6–10. [Google Scholar] [CrossRef]
- Withrow, D.; Alter, D.A. The economic burden of obesity worldwide: A systematic review of the direct costs of obesity. Obes. Rev. 2011, 12, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Snijders, P.J.; Steenbergen, R.D.; Heideman, D.A.; Meijer, C.J. HPV-mediated cervical carcinogenesis: Concepts and clinical implications. J. Pathol. 2006, 208, 152–164. [Google Scholar] [CrossRef]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statistics, 2002. CA Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef]
- Marra, E.; Kovaleva, A.; Bruisten, S.M.; Vermeulen, W.; Boyd, A.; Schim van der Loeff, M.F. Incidence and Clearance of Anal High-risk Human Papillomavirus Infections and Their Determinants Over 5 Years Among Human Immunodeficiency Virus-negative Men Who Have Sex With Men. Clin. Infect. Dis. 2019, 68, 1556–1565. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Palefsky, J.M.; Goldstone, S.; Moreira, E.D., Jr.; Penny, M.E.; Aranda, C.; Vardas, E.; Moi, H.; Jessen, H.; Hillman, R.; et al. Efficacy of quadrivalent HPV vaccine against HPV Infection and disease in males. N. Engl. J. Med. 2011, 364, 401–411. [Google Scholar] [CrossRef]
- Steinbach, A.; Riemer, A.B. Immune evasion mechanisms of human papillomavirus: An update. Int. J. Cancer 2018, 142, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Demoulin, S.A.; Somja, J.; Duray, A.; Guénin, S.; Roncarati, P.; Delvenne, P.O.; Herfs, M.F.; Hubert, P.M. Cervical (pre)neoplastic microenvironment promotes the emergence of tolerogenic dendritic cells via RANKL secretion. Oncoimmunology 2015, 4, e1008334. [Google Scholar] [CrossRef] [PubMed]
- Boyce, B.F.; Xing, L. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch. Biochem. Biophys. 2008, 473, 139–146. [Google Scholar] [CrossRef]
- Beristain, A.G.; Narala, S.R.; Di Grappa, M.A.; Khokha, R. Homotypic RANK signaling differentially regulates proliferation, motility and cell survival in osteosarcoma and mammary epithelial cells. J. Cell Sci. 2012, 125, 943–955. [Google Scholar] [CrossRef]
- Ma, K.S.; Tsai, S.Y. Big Data-driven personal protective equipment stockpiling framework under Universal Healthcare for Disease Control and Prevention in the COVID-19 Era. Int. J. Surg. 2020, 79, 290–291. [Google Scholar] [CrossRef]
- Juang, S.-E.; Ma, K.S.-K.; Kao, P.-E.; Wei, J.C.-C.; Yip, H.-T.; Chou, M.-C.; Hung, Y.-M.; Chin, N.-C. Human Papillomavirus Infection and the Risk of Erectile Dysfunction: A Nationwide Population-Based Matched Cohort Study. J. Pers. Med. 2022, 12, 699. [Google Scholar] [CrossRef]
- Chen, H.-H.; Ma, K.S.-K.; Dong, C.; Chang, W.-J.; Gao, K.-R.; Perng, W.-T.; Huang, J.-Y.; Wei, J.C.-C. Risk of primary Sjogren’s Syndrome following human papillomavirus infections: A nationwide population-based cohort study. Front. Immunol. 2022, 13, 967040. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.C.; Ma, K.S.; Chen, H.H.; Huang, J.Y.; Wei, J.C. Relationship between Helicobacter pylori infection and psoriasis: A nationwide population-based longitudinal cohort study. Medicine 2020, 99, e20632. [Google Scholar] [CrossRef]
- Ma, K.S.; Wu, M.C.; Thota, E.; Wang, Y.H.; Alqaderi, H.E.; Wei, J.C. Tonsillectomy as a risk factor of periodontitis: A population-based cohort study. J. Periodontol. 2022, 93, 721–731. [Google Scholar] [CrossRef]
- Ma, K.S.; Thota, E.; Huang, J.Y.; Huang, Y.F.; Wei, J.C. Onset of oral lichen planus following dental treatments: A nested case-control study. Oral Dis. 2021, 29, 1269–1281. [Google Scholar] [CrossRef]
- Huang, H.-H.; Ma, K.S.-K.; Wu, M.-Y.; Hung, Y.-M.; Tsao, C.-H.; Wei, J.C.-C.; Wen, W.-S.; Wang, Y.-H.; Hung, S.-Y.; Chao, M.M. Patients with obstructive sleep apnea are at great risk of flavor disorders: A 15-year population-based cohort study. Clin. Oral Investig. 2023, 27, 183–192. [Google Scholar] [CrossRef]
- Camacho, P.M.; Petak, S.M.; Binkley, N.; Diab, D.L.; Eldeiry, L.S.; Farooki, A.; Harris, S.T.; Hurley, D.L.; Kelly, J.; Lewiecki, E.M.; et al. American Association of Clinical Endocrinologists/American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis—2020 Update. Endocr. Pract. 2020, 26, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Cosman, F.; de Beur, S.J.; LeBoff, M.S.; Lewiecki, E.M.; Tanner, B.; Randall, S.; Lindsay, R. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.S.; Wei, J.C.; Chung, W.H. Correspondence to ‘Hypersensitivity reactions with allopurinol and febuxostat: A study using the Medicare claims data’. Ann. Rheum. Dis. 2022, 81, e107. [Google Scholar] [CrossRef]
- Akkawi, I.; Zmerly, H. Osteoporosis: Current Concepts. Joints 2018, 6, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Lane, N.E. Epidemiology, etiology, and diagnosis of osteoporosis. Am. J. Obstet. Gynecol. 2006, 194, S3–S11. [Google Scholar] [CrossRef]
- Reyes, C.; García-Gil, M.; Elorza, J.M.; Fina-Avilés, F.; Mendez-Boo, L.; Hermosilla, E.; Coma, E.; Carbonell, C.; Medina-Peralta, M.; Ramos, R.; et al. Socioeconomic status and its association with the risk of developing hip fractures: A region-wide ecological study. Bone 2015, 73, 127–131. [Google Scholar] [CrossRef]
- Johnston, C.B.; Dagar, M. Osteoporosis in Older Adults. Med. Clin. N. Am. 2020, 104, 873–884. [Google Scholar] [CrossRef]
- Zhu, S.M.; Liu, Y.M.; An, E.D.; Chen, Q.L. Influence of systemic immune and cytokine responses during the acute phase of zoster on the development of postherpetic neuralgia. J. Zhejiang Univ. Sci. B 2009, 10, 625–630. [Google Scholar] [CrossRef]
- De Benedetti, F.; Rucci, N.; Del Fattore, A.; Peruzzi, B.; Paro, R.; Longo, M.; Vivarelli, M.; Muratori, F.; Berni, S.; Ballanti, P.; et al. Impaired skeletal development in interleukin-6-transgenic mice: A model for the impact of chronic inflammation on the growing skeletal system. Arthritis Rheum. 2006, 54, 3551–3563. [Google Scholar] [CrossRef]
- Shiau, S.; Broun, E.C.; Arpadi, S.M.; Yin, M.T. Incident fractures in HIV-infected individuals: A systematic review and meta-analysis. Aids 2013, 27, 1949–1957. [Google Scholar] [CrossRef]
- Titanji, K.; Vunnava, A.; Sheth, A.N.; Delille, C.; Lennox, J.L.; Sanford, S.E.; Foster, A.; Knezevic, A.; Easley, K.A.; Weitzmann, M.N.; et al. Dysregulated B cell expression of RANKL and OPG correlates with loss of bone mineral density in HIV infection. PLoS Pathog. 2014, 10, e1004497. [Google Scholar] [CrossRef] [PubMed]
- Baeg, M.K.; Yoon, S.K.; Ko, S.H.; Han, K.D.; Choi, H.J.; Bae, S.H.; Choi, J.Y.; Choi, M.G. Males seropositive for hepatitis B surface antigen are at risk of lower bone mineral density: The 2008-2010 Korea National Health and Nutrition Examination Surveys. Hepatol. Int. 2016, 10, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, L.; He, X.; Farmer, P.; Rubin, J.; Drissi, H.; van Wijnen, A.J.; Lian, J.B.; Stein, G.S.; Nanes, M.S. Expression of the osteoblast differentiation factor RUNX2 (Cbfa1/AML3/Pebp2alpha A) is inhibited by tumor necrosis factor-alpha. J. Biol. Chem. 2002, 277, 2695–2701. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.T.; Ma, K.S. Correspondence to ‘Normal human enthesis harbours conventional CD4+ and CD8+ T cells with regulatory features and inducible IL-17A and TNF expression’. Ann Rheum Dis. 2022, 81, e254. [Google Scholar] [CrossRef] [PubMed]
- Moody, C.A.; Laimins, L.A. Human papillomavirus oncoproteins: Pathways to transformation. Nat. Rev. Cancer 2010, 10, 550–560. [Google Scholar] [CrossRef]
- Fuller, K.; Murphy, C.; Kirstein, B.; Fox, S.W.; Chambers, T.J. TNFα Potently Activates Osteoclasts, through a Direct Action Independent of and Strongly Synergistic with RANKL. Endocrinology 2002, 143, 1108–1118. [Google Scholar] [CrossRef]
- Hofbauer, L.C.; Lacey, D.L.; Dunstan, C.R.; Spelsberg, T.C.; Riggs, B.L.; Khosla, S. Interleukin-1beta and tumor necrosis factor-alpha, but not interleukin-6, stimulate osteoprotegerin ligand gene expression in human osteoblastic cells. Bone 1999, 25, 255–259. [Google Scholar] [CrossRef]
- Cenci, S.; Weitzmann, M.N.; Roggia, C.; Namba, N.; Novack, D.; Woodring, J.; Pacifici, R. Estrogen deficiency induces bone loss by enhancing T-cell production of TNF-alpha. J. Clin. Investig. 2000, 106, 1229–1237. [Google Scholar] [CrossRef]
- Li, Y.; Li, A.; Strait, K.; Zhang, H.; Nanes, M.S.; Weitzmann, M.N. Endogenous TNFalpha lowers maximum peak bone mass and inhibits osteoblastic Smad activation through NF-kappaB. J. Bone Miner. Res. 2007, 22, 646–655. [Google Scholar] [CrossRef]
- Schlecht, H.P.; Fugelso, D.K.; Murphy, R.K.; Wagner, K.T.; Doweiko, J.P.; Proper, J.; Dezube, B.J.; Panther, L.A. Frequency of occult high-grade squamous intraepithelial neoplasia and invasive cancer within anal condylomata in men who have sex with men. Clin. Infect. Dis. 2010, 51, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Workowski, K.A.; Bolan, G.A. Sexually transmitted diseases treatment guidelines, 2015. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2015, 64, 1–137. [Google Scholar]
- Gilson, R.; Nugent, D.; Werner, R.N.; Ballesteros, J.; Ross, J. 2019 IUSTI-Europe guideline for the management of anogenital warts. J. Eur. Acad. Dermatol. Venereol. JEADV 2020, 34, 1644–1653. [Google Scholar] [CrossRef] [PubMed]
- Lacey, C.J.; Woodhall, S.C.; Wikstrom, A.; Ross, J. 2012 European guideline for the management of anogenital warts. J. Eur. Acad. Dermatol. Venereol. 2013, 27, e263–e270. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.S.-K. Chapter 24—Screening programs incorporating big data analytics. In Big Data Analytics for Healthcare; Keikhosrokiani, P., Ed.; Academic Press: Cambridge, MA, USA, 2022; pp. 313–327. [Google Scholar]
- Ma, K.S.; Chang, H.C.; Krupat, E. Teaching evidence-based medicine with electronic databases for preclinical education. Adv. Physiol. Educ. 2021, 45, 849–855. [Google Scholar] [CrossRef]
- Ma, K.S. Integrating travel history via big data analytics under universal healthcare framework for disease control and prevention in the COVID-19 pandemic. J. Clin. Epidemiol. 2021, 130, 147–148. [Google Scholar] [CrossRef]
- Ma, K.S.; Lee, C.M.; Chen, P.H.; Yang, Y.; Dong, Y.W.; Wang, Y.H.; Wei, J.C.; Zheng, W.J. Risk of Autoimmune Diseases Following Optic Neuritis: A Nationwide Population-Based Cohort Study. Front. Med. 2022, 9, 903608. [Google Scholar] [CrossRef]
- Ma, K.S.; Thota, E.; Huang, J.Y.; Wei, J.C.; Resnick, C.M. Increased risk of temporomandibular joint disorders and craniofacial deformities in patients with juvenile idiopathic arthritis: A population-based cohort study. Int. J. Oral Maxillofac. Surg. 2022, 51, 1482–1487. [Google Scholar] [CrossRef]
- Ma, K.S.; Lai, J.N.; Thota, E.; Yip, H.T.; Chin, N.C.; Wei, J.C.; Van Dyke, T.E. Bidirectional Relationship Between Osteoarthritis and Periodontitis: A Population-Based Cohort Study Over a 15-year Follow-Up. Front. Immunol. 2022, 13, 909783. [Google Scholar] [CrossRef]
- Chan, S.Y.; Lu, L.Y.; Lin, S.Y.; Ma, K.S. Pain neuroscience education for fibromyalgia. Int. J. Rheum. Dis. 2023. [Google Scholar] [CrossRef]


{kind=link}
| HPV | |||||
|---|---|---|---|---|---|
| No (N = 51,744) | Yes (N = 12,936) | ||||
| Variables | n | % | n | % | SMD |
| Gender | 0.031 | ||||
| Female | 25,596 | 49.47 | 6198 | 47.91 | |
| Male | 26,148 | 50.53 | 6738 | 52.09 | |
| Age, year | |||||
| 50–60 | 24,335 | 47.03 | 5958 | 46.06 | 0.019 |
| 60–70 | 14,546 | 28.11 | 3496 | 27.03 | 0.024 |
| 70–80 | 9547 | 18.45 | 2661 | 20.57 | 0.054 |
| >80 | 3316 | 6.41 | 821 | 6.35 | 0.003 |
| mean, (SD) | 63.13 | (9.81) | 63.26 | (9.87) | 0.013 |
| Socioeconomic status (Monthly salaries in New Taiwan Dollar) | |||||
| <20,000 | 25,843 | 49.94 | 6835 | 52.84 | 0.058 |
| 20,001–40,000 | 17,163 | 33.17 | 3754 | 29.02 | 0.090 |
| >40,000 | 8738 | 16.89 | 2347 | 18.14 | 0.033 |
| Out-patient visit frequency mean, (SD) | 30.8 | (26.3) | 32.2 | (23.8) | 0.055 |
| Comorbidities | |||||
| Hypertension | 30,535 | 59.01 | 7460 | 57.67 | 0.027 |
| Diabetes | 17,663 | 34.14 | 4330 | 33.47 | 0.014 |
| Hyperlipidemia | 22,185 | 42.87 | 5406 | 41.79 | 0.022 |
| COPD | 15,937 | 30.80 | 3947 | 30.51 | 0.006 |
| IBD | 2871 | 5.55 | 713 | 5.51 | 0.002 |
| HBV | 3050 | 5.89 | 748 | 5.78 | 0.005 |
| HCV | 1370 | 2.65 | 346 | 2.67 | 0.002 |
| Cirrhosis | 25,165 | 48.63 | 6050 | 46.77 | 0.037 |
| Celiac disease | 5 | 0.01 | 1 | 0.01 | 0.002 |
| RA | 3654 | 7.06 | 916 | 7.08 | 0.001 |
| CKD | 2595 | 5.02 | 639 | 4.94 | 0.003 |
| Syphilis | 261 | 0.50 | 65 | 0.50 | <0.001 |
| HIV | 60 | 0.12 | 17 | 0.13 | 0.004 |
| Chlamydia | 2 | 0.004 | 0 | - | 0.009 |
| Gonococcal | 172 | 0.33 | 38 | 0.29 | 0.007 |
| Hyperthyroidism | 2388 | 4.62 | 596 | 4.61 | <0.001 |
| Hyperparathyroidism | 73 | 0.14 | 20 | 0.15 | 0.004 |
| Vitamin D deficiency | 17 | 0.03 | 3 | 0.02 | 0.006 |
| Premature menopause | 1 | 0.002 | 1 | 0.01 | 0.008 |
| Male hypogonadism | 23 | 0.04 | 9 | 0.07 | 0.011 |
| Adrenal cortical steroids | 1 | 0.002 | 0 | - | 0.006 |
| Smoking | 699 | 1.35 | 182 | 1.41 | 0.005 |
| Alcohol | 2088 | 4.04 | 521 | 4.03 | <0.001 |
| Co-medications | |||||
| Long-term use of glucocorticoids | 2011 | 3.89 | 526 | 4.07 | 0.009 |
| Phenobarbital, phenytoin, or carbamazepine | 368 | 0.71 | 99 | 0.77 | 0.006 |
| Heparin or warfarin | 418 | 0.81 | 101 | 0.78 | 0.003 |
| Cyclosporine | 40 | 0.08 | 9 | 0.07 | 0.003 |
| TCAs or SSRIs | 1662 | 3.21 | 435 | 3.36 | 0.008 |
| PPIs | 1676 | 3.24 | 444 | 3.43 | 0.011 |
| Furosemide | 1431 | 2.77 | 348 | 2.69 | 0.005 |
| Thiazide | 1816 | 3.51 | 457 | 3.53 | 0.001 |
| Statin | 5327 | 10.29 | 1338 | 10.34 | 0.002 |
| Beta blockers | 9682 | 18.71 | 2422 | 18.72 | <0.001 |
| Osteoporosis | |||||||
|---|---|---|---|---|---|---|---|
| Variable | n | PY | IR | cHR | (95% CI) | aHR | (95% CI) |
| HPV infections | |||||||
| non-HPV | 277 | 302,947 | 0.91 | 1.00 | 1.00 | ||
| HPV | 116 | 91,893 | 1.26 | 1.33 | (1.07, 1.65) * | 1.32 | (1.06, 1.65) * |
| Gender | |||||||
| Female | 315 | 197,533 | 1.59 | 1.00 | 1.00 | ||
| Male | 78 | 197,307 | 0.40 | 0.25 | (0.19, 0.32) *** | 0.23 | (0.18, 0.3) *** |
| Age, year | |||||||
| 50–60 | 51 | 196,324 | 0.26 | 1.00 | 1.00 | ||
| 60–70 | 150 | 114,244 | 1.31 | 5.04 | (3.67, 6.92) *** | 4.29 | (3.10, 5.93) *** |
| 70–80 | 151 | 68,370 | 2.21 | 9.05 | (6.59, 12.4) *** | 7.32 | (5.23, 10.26) *** |
| >80 | 41 | 15,902 | 2.58 | 12.7 | (8.42, 19.3) *** | 9.63 | (6.22, 14.88) *** |
| Socioeconomic status (Monthly salaries in New Taiwan Dollar) | |||||||
| <20,000 | 249 | 195,413 | 1.27 | 1.00 | 1.00 | ||
| 20,001–40,000 | 137 | 132,988 | 1.03 | 0.79 | (0.64, 0.98) * | 1.06 | (0.86, 1.32) |
| >40,000 | 7 | 66,439 | 0.11 | 0.08 | (0.04, 0.18) *** | 0.30 | (0.14, 0.64) ** |
| Out-patient visit frequency | 1.02 | (1.01, 1.02) | 1.01 | (1.01, 1.01) *** | |||
| Comorbidities | |||||||
| Hypertension | |||||||
| No | 126 | 179,675 | 7.01 | 1.00 | 1.00 | ||
| Yes | 267 | 215,165 | 12.41 | 1.89 | (1.53, 2.34) *** | 0.88 | (0.69, 1.12) |
| Diabetes | |||||||
| No | 237 | 275,713 | 8.60 | 1.00 | 1.00 | ||
| Yes | 156 | 119,127 | 13.10 | 1.63 | (1.33, 2.00) *** | 1.00 | (0.8, 1.24) |
| Hyperlipidemia | |||||||
| No | 234 | 256,496 | 9.12 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 159 | 138,343 | 11.49 | 1.47 | (1.20, 1.81) *** | 0.98 | (0.77, 1.24) |
| COPD | |||||||
| No | 241 | 294,227 | 8.19 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 152 | 100,612 | 15.11 | 2.10 | (1.71, 2.58) *** | 1.35 | (1.08, 1.68) ** |
| IBD | |||||||
| No | 380 | 377,908 | 10.06 | 1.00 | (reference) | ||
| Yes | 13 | 16,931 | 7.68 | 0.86 | (0.50, 1.50) | ||
| HBV | |||||||
| No | 384 | 378,125 | 10.16 | 1.00 | (reference) | ||
| Yes | 9 | 16,714 | 5.38 | 0.62 | (0.32, 1.2) | ||
| HCV | |||||||
| No | 385 | 387,298 | 9.94 | 1.00 | (reference) | ||
| Yes | 8 | 7541 | 10.61 | 1.25 | (0.62, 2.52) | ||
| Cirrhosis | |||||||
| No | 213 | 219,518 | 9.70 | 1.00 | (reference) | ||
| Yes | 180 | 175,322 | 10.27 | 1.13 | (0.92, 1.37) | ||
| Celiac disease | |||||||
| No | 393 | 394,806 | 9.95 | 1.00 | (reference) | ||
| Yes | 0 | 33 | 0.00 | 0.00 | (0, Inf) | ||
| RA | |||||||
| No | 360 | 371,950 | 9.68 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 33 | 22,889 | 14.42 | 1.66 | (1.16, 2.37) ** | 0.99 | (0.69, 1.43) |
| CKD | |||||||
| No | 369 | 381,138 | 9.68 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 24 | 13,701 | 17.52 | 2.11 | (1.39, 3.19) *** | 1.22 | (0.8, 1.88) |
| Syphilis | |||||||
| No | 392 | 393,410 | 9.96 | 1.00 | (reference) | ||
| Yes | 1 | 1430 | 7.00 | 0.80 | (0.11, 5.68) | ||
| HIV | |||||||
| No | 393 | 394,460 | 9.96 | 1.00 | (reference) | ||
| Yes | 0 | 379 | 0.00 | 0.00 | (0, Inf) | ||
| Chlamydia | |||||||
| No | 393 | 394,834 | 9.95 | 1.00 | (reference) | ||
| Yes | 0 | 5 | 0.00 | 0.00 | (0, Inf) | ||
| Gonococcal | |||||||
| No | 393 | 393,856 | 9.98 | 1.00 | (reference) | ||
| Yes | 0 | 983 | 0.00 | 0.00 | (0, Inf) | ||
| Hyperthyroidism | |||||||
| No | 376 | 380,661 | 9.88 | 1.00 | (reference) | ||
| Yes | 17 | 14,178 | 11.99 | 1.37 | (0.84, 2.23) | ||
| Hyperparathyroidism | |||||||
| No | 392 | 394,411 | 9.94 | 1.00 | (reference) | ||
| Yes | 1 | 429 | 23.33 | 2.65 | (0.37, 18.87) | ||
| Vitamin D deficiency | |||||||
| No | 392 | 394,734 | 9.93 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 1 | 105 | 95.23 | 10.4 | (1.45, 73.69) * | 18.3 | (2.56, 131.09) ** |
| Premature menopause | |||||||
| No | 393 | 394,822 | 9.95 | 1.00 | (reference) | ||
| Yes | 0 | 18 | 0.00 | 0.00 | (0, Inf) | ||
| Male hypogonadism | |||||||
| No | 393 | 394,663 | 9.96 | 1.00 | (reference) | ||
| Yes | 0 | 176 | 0.00 | 0.00 | (0, Inf) | ||
| Adrenal cortical steroids | |||||||
| No | 393 | 394,839 | 9.95 | 1.00 | (reference) | ||
| Yes | 0 | 0 | 0.00 | NA | (NA, NA)NA | ||
| Smoking | |||||||
| No | 391 | 391,790 | 9.98 | 1.00 | (reference) | ||
| Yes | 2 | 3049 | 6.56 | 0.88 | (0.22, 3.56) | ||
| Alcohol | |||||||
| No | 389 | 384,044 | 10.13 | 1.00 | (reference) | ||
| Yes | 4 | 10,795 | 3.71 | 0.44 | (0.16, 1.17) | ||
| Co-medications | |||||||
| Long-term use of glucocorticoids | |||||||
| No | 355 | 382,271 | 9.29 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 38 | 12,568 | 30.24 | 3.47 | (2.48, 4.85) *** | 2.05 | (1.44, 2.92) *** |
| Phenobarbital, phenytoin, or carbamazepine | |||||||
| No | 388 | 392,217 | 9.89 | 1.00 | (reference) | ||
| Yes | 5 | 2622 | 19.07 | 1.98 | (0.82, 4.79) | ||
| Heparin or warfarin | |||||||
| No | 390 | 392,544 | 9.94 | 1.00 | (reference) | ||
| Yes | 3 | 2295 | 13.07 | 1.51 | (0.49, 4.71) | ||
| Cyclosporine | |||||||
| No | 393 | 394,557 | 9.96 | 1.00 | (reference) | ||
| Yes | 0 | 282 | 0.00 | 0.00 | (0, Inf) | ||
| TCAs or SSRIs | |||||||
| No | 368 | 384,588 | 9.57 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 25 | 10,251 | 24.39 | 2.79 | (1.86, 4.19) *** | 1.60 | (1.05, 2.43) * |
| PPIs | |||||||
| No | 383 | 386,939 | 9.90 | 1.00 | (reference) | ||
| Yes | 10 | 7900 | 12.66 | 1.64 | (0.87, 3.08) | ||
| Furosemide | |||||||
| No | 376 | 387,563 | 9.70 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 17 | 7276 | 23.37 | 2.84 | (1.74, 4.62) *** | 1.14 | (0.69, 1.91) |
| Thiazide | |||||||
| No | 369 | 382,117 | 9.66 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 24 | 12,722 | 18.86 | 2.05 | (1.36, 3.10) *** | 1.13 | (0.74, 1.74) |
| Statin | |||||||
| No | 349 | 365,283 | 9.55 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 44 | 29,556 | 14.89 | 1.86 | (1.35, 2.55) *** | 1.23 | (0.87, 1.73) |
| Beta blockers | |||||||
| No | 307 | 326,634 | 9.40 | 1.00 | (reference) | 1.00 | (reference) |
| Yes | 86 | 68,205 | 12.61 | 1.40 | (1.10, 1.78) ** | 0.85 | (0.65, 1.10) |
| non-HPV | HPV | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | N | PY | IR | n | PY | IR | cHR | (95% CI) | aHR | (95% CI) |
| Gender | ||||||||||
| Female | 227 | 154,018 | 14.7 | 88 | 43,514 | 20.2 | 1.33 | (1.04,1.70) * | 1.33 | (1.04,1.71) * |
| Male | 50 | 148,928 | 3.4 | 28 | 48,378 | 5.8 | 1.65 | (1.04,2.62) * | 1.29 | (0.80,2.08) |
| Age, year | ||||||||||
| 50–60 | 41 | 153,573 | 2.7 | 10 | 42,751 | 2.3 | 0.87 | (0.43,1.73) | 0.88 | (0.44,1.76) |
| 60–70 | 107 | 88,263 | 12.1 | 43 | 25,980 | 16.6 | 1.28 | (0.90,1.83) | 1.45 | (1.01,2.08) * |
| 70–80 | 97 | 49,295 | 19.7 | 54 | 19,075 | 28.3 | 1.33 | (0.95,1.86) | 1.51 | (1.07,2.12) * |
| >80 | 32 | 11,816 | 27.1 | 9 | 4086 | 22.0 | 0.76 | (0.36,1.59) | 0.95 | (0.45,2.01) |
| Socioeconomic status (Monthly salaries in New Taiwan Dollar) | ||||||||||
| <20,000 | 167 | 146,307 | 11.4 | 82 | 49,106 | 16.7 | 1.39 | (1.06,1.81) * | 1.32 | (1.01,1.73) * |
| 20,001–40,000 | 108 | 106,808 | 10.1 | 29 | 26,179 | 11.1 | 1.07 | (0.71,1.62) | 1.22 | (0.81,1.85) |
| >40,000 | 2 | 49,832 | 0.4 | 5 | 16,607 | 3.0 | 7.47 | (1.45,38.56) * | 8.22 | (1.59,42.38) * |
| Comorbidities | ||||||||||
| Hypertension | ||||||||||
| No | 86 | 139,008 | 6.2 | 40 | 40,667 | 9.8 | 1.56 | (1.07,2.26) * | 1.50 | (1.02,2.20) * |
| Yes | 191 | 163,939 | 11.7 | 76 | 51,226 | 14.8 | 1.21 | (0.93,1.58) | 1.27 | (0.97,1.67) |
| Diabetes | ||||||||||
| No | 163 | 212,619 | 7.7 | 74 | 63,094 | 11.7 | 1.48 | (1.13,1.95) ** | 1.42 | (1.07,1.88) * |
| Yes | 114 | 90,328 | 12.6 | 42 | 28,798 | 14.6 | 1.09 | (0.77,1.56) | 1.22 | (0.85,1.74) |
| Hyperlipidemia | ||||||||||
| No | 168 | 197,826 | 8.5 | 66 | 58,670 | 11.2 | 1.28 | (0.96,1.71) | 1.29 | (0.97,1.73) |
| Yes | 109 | 105,120 | 10.4 | 50 | 33,223 | 15.0 | 1.36 | (0.97,1.90) | 1.35 | (0.96,1.89) |
| COPD | ||||||||||
| No | 171 | 227,344 | 7.5 | 70 | 66,883 | 10.5 | 1.35 | (1.02,1.78) * | 1.41 | (1.06,1.87) * |
| Yes | 106 | 75,603 | 14.0 | 46 | 25,009 | 18.4 | 1.22 | (0.86,1.73) | 1.24 | (0.87,1.77) |
| IBD | ||||||||||
| No | 267 | 29,0246 | 9.2 | 113 | 87,662 | 12.9 | 1.35 | (1.08,1.68) ** | 1.36 | (1.09,1.70) ** |
| Yes | 10 | 12,700 | 7.9 | 3 | 4231 | 7.1 | 0.89 | (0.24,3.24) | 1.38 | (0.36,5.27) |
| HBV | ||||||||||
| No | 271 | 290,425 | 9.3 | 113 | 87,700 | 12.9 | 1.33 | (1.07,1.65) * | 1.33 | (1.07,1.67) * |
| Yes | 6 | 12,521 | 4.8 | 3 | 4193 | 7.2 | 1.33 | (0.33,5.35) | 1.55 | (0.38,6.37) |
| HCV | ||||||||||
| No | 272 | 297,353 | 9.1 | 113 | 89,945 | 12.6 | 1.32 | (1.06,1.64) * | 1.33 | (1.06,1.66) * |
| Yes | 5 | 5594 | 8.9 | 3 | 1948 | 15.4 | 1.76 | (0.42,7.43) | 2.46 | (0.41,14.64) |
| Cirrhosis | ||||||||||
| No | 143 | 168,617 | 8.5 | 70 | 50,900 | 13.8 | 1.58 | (1.19,2.11) ** | 1.58 | (1.18,2.12) ** |
| Yes | 134 | 134,329 | 10.0 | 46 | 40,992 | 11.2 | 1.06 | (0.76,1.48) | 1.06 | (0.76,1.50) |
| RA | ||||||||||
| No | 250 | 285,616 | 8.8 | 110 | 86,334 | 12.7 | 1.40 | (1.12,1.75) ** | 1.40 | (1.12,1.76) ** |
| Yes | 27 | 17,330 | 15.6 | 6 | 5558 | 10.8 | 0.64 | (0.26,1.54) | 0.73 | (0.29,1.81) |
| CKD | ||||||||||
| No | 259 | 292,591 | 8.9 | 110 | 88,547 | 12.4 | 1.35 | (1.08,1.68) ** | 1.34 | (1.07,1.68) * |
| Yes | 18 | 10,355 | 17.4 | 6 | 3346 | 17.9 | 1.00 | (0.4,2.53) | 1.50 | (0.56,4.00) |
| Hyperthyroidism | ||||||||||
| No | 263 | 292,224 | 9.0 | 113 | 88,437 | 12.8 | 1.36 | (1.09,1.70) ** | 1.37 | (1.10,1.72) ** |
| Yes | 14 | 10,723 | 13.1 | 3 | 3455 | 8.7 | 0.64 | (0.19,2.25) | 0.65 | (0.18,2.34) |
| Alcohol | ||||||||||
| No | 275 | 294,914 | 9.3 | 114 | 89,130 | 12.8 | 1.32 | (1.06,1.64) * | 1.32 | (1.06,1.65) * |
| Yes | 2 | 8033 | 2.5 | 2 | 2762 | 7.2 | 2.77 | (0.39,19.84) | 0.77 | (0.10,5.65) |
| Co-medications | ||||||||||
| Long-term use of glucocorticoids | ||||||||||
| No | 254 | 293,679 | 8.6 | 101 | 88,592 | 11.4 | 1.26 | (1.00,1.59) * | 1.27 | (1.00,1.6) * |
| Yes | 23 | 9268 | 24.8 | 15 | 3300 | 45.4 | 1.75 | (0.91,3.35) | 2.17 | (1.11,4.22) * |
| Phenobarbital, phenytoin, or carbamazepine | ||||||||||
| No | 273 | 301,023 | 9.1 | 115 | 91,194 | 12.6 | 1.34 | (1.07,1.66) ** | 1.35 | (1.08,1.68) ** |
| Yes | 4 | 1924 | 20.8 | 1 | 699 | 14.3 | 0.63 | (0.07,5.7) | 0.00 | (0,Inf) |
| Heparin or warfarin | ||||||||||
| No | 274 | 301,212 | 9.1 | 116 | 91,332 | 12.7 | 1.34 | (1.08,1.66) ** | 1.35 | (1.08,1.68) ** |
| Yes | 3 | 1734 | 17.3 | 0 | 561 | 0.0 | 0.00 | (0,Inf) | 0.00 | (0,Inf) |
| TCAs or SSRIs | ||||||||||
| No | 259 | 295,564 | 8.8 | 109 | 89,025 | 12.2 | 1.34 | (1.07,1.68) ** | 1.35 | (1.08,1.70) ** |
| Yes | 18 | 7383 | 24.4 | 7 | 2868 | 24.4 | 0.93 | (0.39,2.23) | 0.99 | (0.39,2.47) |
| PPIs | ||||||||||
| No | 270 | 297,150 | 9.1 | 113 | 89,789 | 12.6 | 1.33 | (1.07,1.66) * | 1.34 | (1.07,1.67) * |
| Yes | 7 | 5797 | 12.1 | 3 | 2104 | 14.3 | 0.96 | (0.25,3.73) | 2.08 | (0.41,10.71) |
| Furosemide | ||||||||||
| No | 266 | 297,458 | 8.9 | 110 | 90,105 | 12.2 | 1.31 | (1.05,1.64) * | 1.31 | (1.04,1.64) * |
| Yes | 11 | 5488 | 20.0 | 6 | 1787 | 33.6 | 1.60 | (0.59,4.32) | 2.02 | (0.70,5.78) |
| Thiazide | ||||||||||
| No | 262 | 293,245 | 8.9 | 107 | 88,872 | 12.0 | 1.29 | (1.03,1.62) * | 1.30 | (1.03,1.63) * |
| Yes | 15 | 9702 | 15.5 | 9 | 3020 | 29.8 | 1.87 | (0.82,4.27) | 2.14 | (0.89,5.14) |
| Statin | ||||||||||
| No | 246 | 280,748 | 8.8 | 103 | 84,535 | 12.2 | 1.34 | (1.06,1.68) * | 1.36 | (1.07,1.71) * |
| Yes | 31 | 22,199 | 14.0 | 13 | 7357 | 17.7 | 1.18 | (0.62,2.26) | 1.10 | (0.56,2.15) |
| Beta blockers | ||||||||||
| No | 210 | 251,618 | 8.3 | 97 | 75,016 | 12.9 | 1.50 | (1.18,1.91) ** | 1.49 | (1.17,1.91) ** |
| Yes | 67 | 51,329 | 13.1 | 19 | 16,876 | 11.3 | 0.81 | (0.49,1.35) | 0.91 | (0.54,1.52) |
| Osteoporosis | |||||||
|---|---|---|---|---|---|---|---|
| Variable | n | PY | IR | cHR | (95% CI) | aHR | (95% CI) |
| Non-HPV | 277 | 302,947 | 0.91 | 1.00 | 1.00 | ||
| Treatment for HPV infections | |||||||
| with treatment † | 31 | 32,546 | 0.95 | 1.18 | (0.81,1.71) | 1.14 | (0.78,1.66) |
| without treatment * | 85 | 59,346 | 1.43 | 1.39 | (1.09,1.77) ** | 1.40 | (1.09,1.80) ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, K.S.-K.; Chin, N.-C.; Tu, T.-Y.; Wu, Y.-C.; Yip, H.-T.; Wei, J.C.-C.; Chang, R.-i. Human Papillomavirus Infections and Increased Risk of Incident Osteoporosis: A Nationwide Population-Based Cohort Study. Viruses 2023, 15, 1021. https://doi.org/10.3390/v15041021
Ma KS-K, Chin N-C, Tu T-Y, Wu Y-C, Yip H-T, Wei JC-C, Chang R-i. Human Papillomavirus Infections and Increased Risk of Incident Osteoporosis: A Nationwide Population-Based Cohort Study. Viruses. 2023; 15(4):1021. https://doi.org/10.3390/v15041021
Chicago/Turabian StyleMa, Kevin Sheng-Kai, Ning-Chien Chin, Ting-Yu Tu, Yao-Cheng Wu, Hei-Tung Yip, James Cheng-Chung Wei, and Ren-in Chang. 2023. "Human Papillomavirus Infections and Increased Risk of Incident Osteoporosis: A Nationwide Population-Based Cohort Study" Viruses 15, no. 4: 1021. https://doi.org/10.3390/v15041021
APA StyleMa, K. S.-K., Chin, N.-C., Tu, T.-Y., Wu, Y.-C., Yip, H.-T., Wei, J. C.-C., & Chang, R.-i. (2023). Human Papillomavirus Infections and Increased Risk of Incident Osteoporosis: A Nationwide Population-Based Cohort Study. Viruses, 15(4), 1021. https://doi.org/10.3390/v15041021