
Genetic Variants Associated with Drug Resistance of Cytomegalovirus in Hematopoietic Cell Transplantation Recipients
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
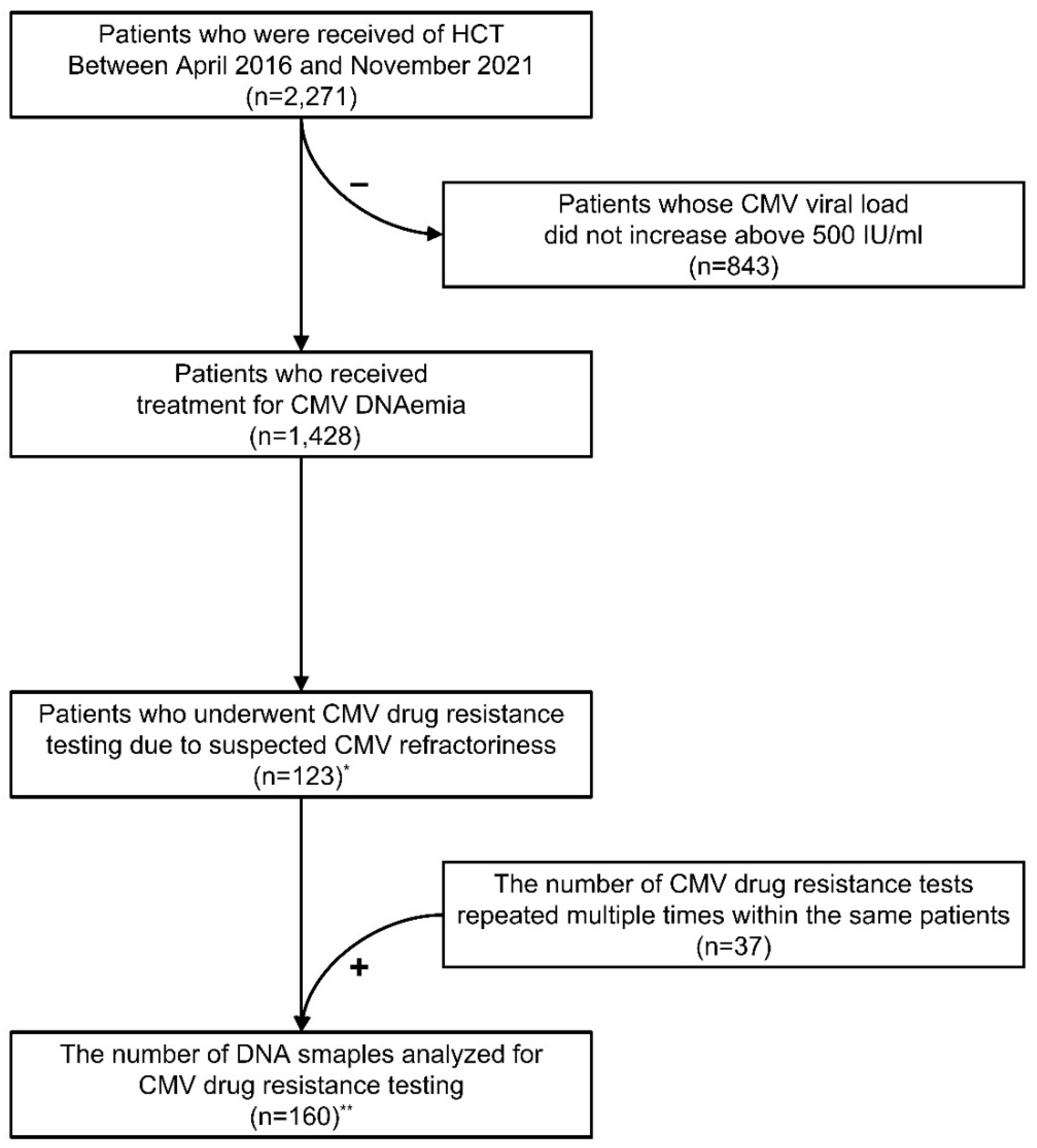
2.1. Patients
2.2. Monitoring of CMV Infection
2.3. Treatment Strategies for CMV Infection
2.4. CMV Drug Resistant Testing
2.5. Statistics
3. Results
3.1. Patient Characteristics
3.2. Identified Variants of UL97 and UL54 Genes
3.3. Clinical Significance of Genetic Variants
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Zanella, M.-C.; Cordey, S.; Kaiser, L. Beyond Cytomegalovirus and Epstein-Barr Virus: A Review of Viruses Composing the Blood Virome of Solid Organ Transplant and Hematopoietic Stem Cell Transplant Recipients. Clin. Microbiol. Rev. 2020, 33, e00027-20. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Chen, H.-P.; Chan, Y.-J.; Wang, F.-D. Clinical significance of post-treatment viral load of cytomegalovirus in patients with hematologic malignancies. J. Microbiol. Immunol. Infect. 2021, 54, 245–252. [Google Scholar] [CrossRef]
- Galitska, G.; Biolatti, M.; De Andrea, M.; Leone, A.; Coscia, A.; Bertolotti, L.; Ala, U.; Bertino, E.; Dell’Oste, V.; Landolfo, S. Biological relevance of Cytomegalovirus genetic variability in congenitally and postnatally infected children. J. Clin. Virol. 2018, 108, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Hai, R.; Liu, F. Detection of congenital cytomegalovirus in newborns using nucleic acid amplification techniques and its public health implications. Virol. Sin. 2017, 32, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Pande, A.; Dubberke, E.R. Cytomegalovirus Infections of the Stem Cell Transplant Recipient and Hematologic Malignancy Patient. Infect. Dis. Clin. N. Am. 2019, 33, 485–500. [Google Scholar] [CrossRef]
- Jung, J.-Y.; Nho, D.; Cho, S.-Y.; Lee, D.-G.; Choi, S.-M.; Kim, H.-J.; Kim, M.; Oh, E.-J. Intra-host diversity of drug-resistant cytomegalovirus: A case report of cytomegalovirus infection after allogeneic hematopoietic cell transplantation. J. Infect. Chemother. 2022, 28, 1415–1418. [Google Scholar] [CrossRef]
- Zöllner, S.K.; Herbrüggen, H.; Kolve, H.; Mihailovic, N.; Schubert, F.; Reicherts, C.; Rössig, C.; Groll, A.H. Cytomegalovirus retinitis in children and adolescents with acute leukemia following allogeneic hematopoietic stem cell transplantation. Transpl. Infect. Dis. 2019, 21, e13089. [Google Scholar] [CrossRef]
- Reusser, P.; Fisher, L.; Buckner, C.; Thomas, E.; Meyers, J. Cytomegalovirus infection after autologous bone marrow transplantation: Occurrence of cytomegalovirus disease and effect on engraftment. Blood 1990, 75, 1888–1894. [Google Scholar] [CrossRef]
- Cantoni, N.; Hirsch, H.H.; Khanna, N.; Gerull, S.; Buser, A.; Bucher, C.; Halter, J.; Heim, D.; Tichelli, A.; Gratwohl, A.; et al. Evidence for a Bidirectional Relationship between Cytomegalovirus Replication and acute Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2010, 16, 1309–1314. [Google Scholar] [CrossRef]
- Giménez, E.; Torres, I.; Albert, E.; Piñana, J.-L.; Hernández-Boluda, J.-C.; Solano, C.; Navarro, D. Cytomegalovirus (CMV) infection and risk of mortality in allogeneic hematopoietic stem cell transplantation (Allo-HSCT): A systematic review, meta-analysis, and meta-regression analysis. Am. J. Transplant. 2019, 19, 2479–2494. [Google Scholar] [CrossRef]
- Green, M.L.; Leisenring, W.; Xie, H.; Mast, T.C.; Cui, Y.; Sandmaier, B.M.; Sorror, M.L.; Goyal, S.; Özkök, S.; Yi, J.; et al. Cytomegalovirus viral load and mortality after haemopoietic stem cell transplantation in the era of pre-emptive therapy: A retrospective cohort study. Lancet Haematol. 2016, 3, e119–e127. [Google Scholar] [CrossRef] [PubMed]
- Ljungman, P.; de la Camara, R.; Robin, C.; Crocchiolo, R.; Einsele, H.; Hill, J.A.; Hubacek, P.; Navarro, D.; Cordonnier, C.; Ward, K.N. Guidelines for the management of cytomegalovirus infection in patients with haematological malignancies and after stem cell transplantation from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect. Dis. 2019, 19, e260–e272. [Google Scholar] [CrossRef] [PubMed]
- Marty, F.M.; Ljungman, P.; Chemaly, R.F.; Maertens, J.; Dadwal, S.S.; Duarte, R.F.; Haider, S.; Ullmann, A.J.; Katayama, Y.; Brown, J.; et al. Letermovir Prophylaxis for Cytomegalovirus in Hematopoietic-Cell Transplantation. N. Engl. J. Med. 2017, 377, 2433–2444. [Google Scholar] [CrossRef]
- Erice, A. Resistance of human cytomegalovirus to antiviral drugs. Clin. Microbiol. Rev. 1999, 12, 286–297. [Google Scholar] [CrossRef]
- Hantz, S.; Garnier-Geoffroy, F.; Mazeron, M.-C.; Garrigue, I.; Merville, P.; Mengelle, C.; Rostaing, L.; Saint Marcoux, F.; Essig, M.; Rerolle, J.-P.; et al. Drug-resistant cytomegalovirus in transplant recipients: A French cohort study. J. Antimicrob. Chemother. 2010, 65, 2628–2640. [Google Scholar] [CrossRef] [PubMed]
- Fischer, L.; Imrich, E.; Sampaio, K.L.; Hofmann, J.; Jahn, G.; Hamprecht, K.; Göhring, K. Identification of resistance-associated HCMV UL97- and UL54-mutations and a UL97-polymporphism with impact on phenotypic drug-resistance. Antivir. Res. 2016, 131, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Campos, A.B.; Ribeiro, J.; Boutolleau, D.; Sousa, H. Human cytomegalovirus antiviral drug resistance in hematopoietic stem cell transplantation: Current state of the art. Rev. Med. Virol. 2016, 26, 161–182. [Google Scholar] [CrossRef]
- Chou, S.; Ercolani, R.J.; Marousek, G.; Bowlin, T.L. Cytomegalovirus UL97 kinase catalytic domain mutations that confer multidrug resistance. Antimicrob. Agents Chemother. 2013, 57, 3375–3379. [Google Scholar] [CrossRef]
- Drouot, E.; Piret, J.; Lebel, M.H.; Boivin, G. Characterization of multiple cytomegalovirus drug resistance mutations detected in a hematopoietic stem cell transplant recipient by recombinant phenotyping. J. Clin. Microbiol. 2014, 52, 4043–4046. [Google Scholar] [CrossRef]
- Danziger-Isakov, L.; Englund, J.; Green, M.; Posfay-Barbe, K.M.; Zerr, D.M. Cytomegalovirus in Pediatric Hematopoietic Stem Cell Transplantation: A Case-Based Panel Discussion of Current Challenges. J. Pediatr. Infect. Dis. Soc. 2018, 7, S72–S74. [Google Scholar] [CrossRef]
- Einsele, H.; Ljungman, P.; Boeckh, M. How I treat CMV reactivation after allogeneic hematopoietic stem cell transplantation. Blood 2020, 135, 1619–1629. [Google Scholar] [CrossRef] [PubMed]
- El Chaer, F.; Shah, D.P.; Chemaly, R.F. How I treat resistant cytomegalovirus infection in hematopoietic cell transplantation recipients. Blood 2016, 128, 2624–2636. [Google Scholar] [CrossRef] [PubMed]
- Chemaly, R.F.; Chou, S.; Einsele, H.; Griffiths, P.; Avery, R.; Razonable, R.R.; Mullane, K.M.; Kotton, C.; Lundgren, J.; Komatsu, T.E.; et al. Definitions of Resistant and Refractory Cytomegalovirus Infection and Disease in Transplant Recipients for Use in Clinical Trials. Clin. Infect. Dis. 2019, 68, 1420–1426. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.; Waldemer, R.H.; Senters, A.E.; Michels, K.S.; Kemble, G.W.; Miner, R.C.; Drew, W.L. Cytomegalovirus UL97 Phosphotransferase Mutations That Affect Susceptibility to Ganciclovir. J. Infect. Dis. 2002, 185, 162–169. [Google Scholar] [CrossRef]
- Yu, U.; Wang, X.; Zhang, X.; Wang, C.; Yang, C.; Zhou, X.; Li, Y.; Huang, X.; Wen, J.; Wen, F.; et al. Cytomegalovirus Infection and the Implications of Drug-Resistant Mutations in Pediatric Allogeneic Hematopoietic Stem Cell Transplant Recipients: A Retrospective Study from a Tertiary Hospital in China. Infect. Dis. Ther. 2021, 10, 1309–1322. [Google Scholar] [CrossRef]
- Shmueli, E.; Or, R.; Shapira, M.Y.; Resnick, I.B.; Caplan, O.; Bdolah-Abram, T.; Wolf, D.G. High rate of cytomegalovirus drug resistance among patients receiving preemptive antiviral treatment after haploidentical stem cell transplantation. J. Infect. Dis. 2014, 209, 557–561. [Google Scholar] [CrossRef]
- Vejrazkova, E.; Pliskova, L.; Hubacek, P.; Kostal, M.; Zavrelova, A.; Radocha, J.; Kutova, R.; Stepanova, V.; Zak, P. Clinical and genotypic CMV drug resistance in HSCT recipients: A single center epidemiological and clinical data. Bone Marrow Transplant. 2019, 54, 146–149. [Google Scholar] [CrossRef]
- Solano, C.; Talaya, A.; Giménez, E.; Albert, E.; Piñana, J.L.; Hernández-Boluda, J.C.; Pérez, A.; Navarro, D. Refractory cytomegalovirus DNAemia after allogeneic hematopoietic stem cell transplantation: When should genotypic drug resistance testing be requested? Bone Marrow Transplant. 2018, 53, 787–790. [Google Scholar] [CrossRef]
- Lurain, N.S.; Bhorade, S.M.; Pursell, K.J.; Avery, R.K.; Yeldandi, V.V.; Isada, C.M.; Robert, E.S.; Kohn, D.J.; Arens, M.Q.; Garrity, E.R.; et al. Analysis and Characterization of Antiviral Drug–Resistant Cytomegalovirus Isolates from Solid Organ Transplant Recipients. J. Infect. Dis. 2002, 186, 760–768. [Google Scholar] [CrossRef]
- Baldanti, F.; Lurain, N.; Gerna, G. Clinical and biologic aspects of human cytomegalovirus resistance to antiviral drugs. Hum. Immunol. 2004, 65, 403–409. [Google Scholar] [CrossRef]
- Campos, A.B.; Ribeiro, J.; Pinho Vaz, C.; Campilho, F.; Branca, R.; Campos, A., Jr.; Baldaque, I.; Medeiros, R.; Boutolleau, D.; Sousa, H. Genotypic resistance of cytomegalovirus to antivirals in hematopoietic stem cell transplant recipients from Portugal: A retrospective study. Antivir. Res. 2017, 138, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Chou, S. Advances in the genotypic diagnosis of cytomegalovirus antiviral drug resistance. Antivir. Res. 2020, 176, 104711. [Google Scholar] [CrossRef] [PubMed]
- Renzette, N.; Pokalyuk, C.; Gibson, L.; Bhattacharjee, B.; Schleiss, M.R.; Hamprecht, K.; Yamamoto, A.Y.; Mussi-Pinhata, M.M.; Britt, W.J.; Jensen, J.D.; et al. Limits and patterns of cytomegalovirus genomic diversity in humans. Proc. Natl. Acad. Sci. USA 2015, 112, E4120–E4128. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-L.; Lin, T.-W.; Lin, H.-C.; Wang, H.-Y.; Chang, P.-Y.; Wang, P.-N.; Yang, S.; Lu, J.-J. Molecular Epidemiology of Cytomegalovirus UL97 and UL54 variants in Taiwan. J. Microbiol. Immunol. Infect. 2021, 54, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Lurain, N.S.; Chou, S. Antiviral Drug Resistance of Human Cytomegalovirus. Clin. Microbiol. Rev. 2010, 23, 689–712. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | No. of Patients (%) | p Value | |||
|---|---|---|---|---|---|
| Total Patients | Resistance Variants | VUSs | Without Any Variants | ||
| Number of patients | 123 (100.0%) | 10 (100.0%) | 48 (100.0%) | 65 (100.0%) | - |
| Age (years; range) | 44; 5–72 | 39; 5–67 | 46; 11–72 | 44; 8–71 | 0.531 |
| Male | 55 (44.7%) | 4 (40.0%) | 23 (47.9%) | 28 (43.1%) | 0.835 |
| Primary disease | |||||
| AML | 50 (40.7%) | 3 (30.0%) | 22 (45.8%) | 25 (38.5%) | 0.567 |
| ALL | 24 (19.5%) | 3 (30.0%) | 11 (22.9%) | 10 (15.4%) | 0.415 |
| MDS | 14 (11.4%) | 2 (20.0%) | 6 (12.5%) | 6 (9.2%) | 0.579 |
| NHL | 11 (8.9%) | 1 (10.0%) | 3 (6.3%) | 7 (10.8%) | 0.702 |
| Aplastic anemia | 9 (7.3%) | 0 | 1 (2.1%) | 8 (12.3%) | 0.077 |
| Others | 15 (12.2%) | 1 (10.0%) | 5 (10.4%) | 9 (13.8%) | 0.839 |
| HCT source | |||||
| Peripheral blood | 106 (86.2%) | 8 (80.0%) | 40 (83.3%) | 58 (89.2%) | 0.561 |
| Cord blood | 17 (13.8%) | 2 (20.0%) | 8 (16.7%) | 7 (10.8%) | - |
| Related donor HCT | 74 (60.2%) | 4 (40.0%) | 30 (62.5%) | 40 (61.5%) | 0.395 |
| HLA-matched HCT | 62 (50.4%) | 6 (60.0%) | 26 (54.2%) | 30 (46.2%) | 0.574 |
| Letermovir prophylaxis | 13 (10.6%) | 1 (10.0%) | 4 (8.3%) | 8 (12.3%) | 0.792 |
| CMV D/R serostatus | |||||
| D+/R+ | 66 (53.7%) | 3 (30.0%) | 26 (54.2%) | 37 (56.9%) | 0.282 |
| D+/R- | 4 (3.3%) | 0 | 2 (4.2%) | 2 (3.1%) | 0.791 |
| D-/R+ | 26 (21.1%) | 3 (30.0%) | 10 (20.8%) | 13 (20.0%) | 0.769 |
| D-/R- | 0 | 0 | 0 | 0 | - |
| D?/R+ | 27 (22.0%) | 4 (40.0%) | 10 (20.8%) | 13 (20.0%) | 0.353 |
| Development of refractory CMV DNAemia (days) | 70 | 66.5 | 72 | 70 | 0.942 |
| CMV organ disease | |||||
| One | 39 (31.7%) | 4 (40.0%) | 12 (25.0%) | 23 (35.4%) | - |
| Two or more | 11 (8.9%) | 4 (40.0%) | 3 (6.3%) | 4 (6.2%) | - |
| No | 73 (59.3%) | 2 (20.0%) | 33 (68.8%) | 38 (58.5%) | 0.017 |
| Highest CMV viral load (IU/mL; range) | 593,178.4; 910–14,690,000 | 2281,671.8; 36,080–14,690,000 | 303,385.7; 3668–2,444,000 | 543,370.9; 910–10,378,623 | 0.015 * |
| Acute GVHD | |||||
| None to mild | 35 (28.5%) | 1 (10.0%) | 8 (16.7%) | 26 (40.0%) | 0.003 ** |
| Moderate to severe | 88 (71.5%) | 9 (90.0%) | 40 (83.3%) | 39 (60.0%) | - |
| One-year survival rate after HCT (%) | 52.9% | 40.0% | 43.8% | 61.5% | 0.044 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chae, S.; Kim, H.S.; Cho, S.-Y.; Nho, D.; Lee, R.; Lee, D.-G.; Kim, M.; Kim, Y. Genetic Variants Associated with Drug Resistance of Cytomegalovirus in Hematopoietic Cell Transplantation Recipients. Viruses 2023, 15, 1286. https://doi.org/10.3390/v15061286
Chae S, Kim HS, Cho S-Y, Nho D, Lee R, Lee D-G, Kim M, Kim Y. Genetic Variants Associated with Drug Resistance of Cytomegalovirus in Hematopoietic Cell Transplantation Recipients. Viruses. 2023; 15(6):1286. https://doi.org/10.3390/v15061286
Chicago/Turabian StyleChae, Seungwan, Hoon Seok Kim, Sung-Yeon Cho, Dukhee Nho, Raeseok Lee, Dong-Gun Lee, Myungshin Kim, and Yonggoo Kim. 2023. "Genetic Variants Associated with Drug Resistance of Cytomegalovirus in Hematopoietic Cell Transplantation Recipients" Viruses 15, no. 6: 1286. https://doi.org/10.3390/v15061286
APA StyleChae, S., Kim, H. S., Cho, S.-Y., Nho, D., Lee, R., Lee, D.-G., Kim, M., & Kim, Y. (2023). Genetic Variants Associated with Drug Resistance of Cytomegalovirus in Hematopoietic Cell Transplantation Recipients. Viruses, 15(6), 1286. https://doi.org/10.3390/v15061286