
Development and Validation of Three Triplex Real-Time RT-PCR Assays for Typing African Horse Sickness Virus: Utility for Disease Control and Other Laboratory Applications
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Samples and Virus Isolates
2.2. Virus Cloning by End Point Dilution of AHSV Suspensions Containing More than One AHSV Serotype (Polyvalent Commercial LAV and Original AHSV Reference Strains)
2.3. Nucleid Acid Extraction
2.4. Primers and Probes Design
2.5. Optimisation of rRT-PCRs in Triplex
2.6. Validation Parameters Evaluated
2.7. Ethical Statement
3. Results
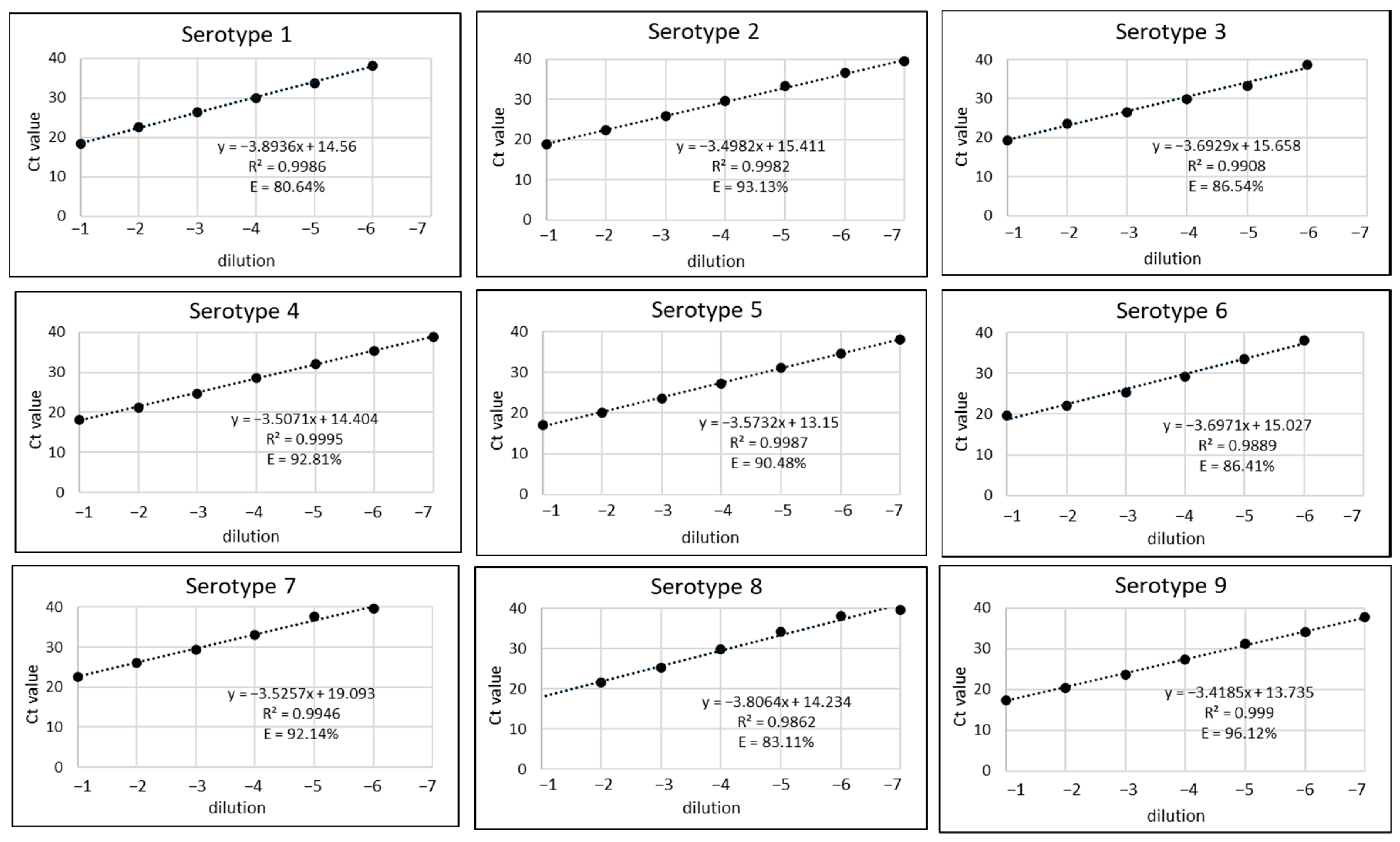
3.1. Analytical Sensitivity
3.2. Analytical Specificity
- Exclusivity
- Exclusivity among serotypes
3.3. Diagnostic Sensitivity
3.4. Diagnostic Specificity
3.5. Intra-Assay and Intra-Laboratory Repeatability
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coetzer, J.A.W.; Guthrie, A.J. African Horse Sickness. In Infectious Diseases of Livestock; Coetzer, J.A.W., Tustin, R.C., Eds.; Oxford University Press: Oxford, UK, 2004; Volume 2, pp. 1231–1264. [Google Scholar]
- Mellor, P.S.; Hamblin, C. African Horse Sickness. Vet. Res. 2004, 35, 445–466. [Google Scholar] [CrossRef] [PubMed]
- Zientara, S.; Weyer, C.T.; Lecollinet, S. African horse sickness. Rev. Sci. Tech. 2015, 34, 315–327. [Google Scholar] [CrossRef] [PubMed]
- King, S.; Rajko-Nenow, P.; Ashby, M.; Frost, L.; Carpenter, S.; Batten, C. Outbreak of African horse sickness in Thailand, 2020. Transbound. Emerg. Dis. 2020, 67, 1764–1767. [Google Scholar] [CrossRef] [PubMed]
- Lu, G.; Pan, J.; Ou, J.; Shao, R.; Hu, X.; Wang, C.; Li, S. African horse sickness: Its emergence in Thailand and potential threat to other Asian countries. Transbound. Emerg. Dis. 2020, 67, 1751–1753. [Google Scholar] [CrossRef] [PubMed]
- WOAH. The Official #2022-2. May 2022. Available online: https://bulletin.woah.org/?officiel=11-1-1-2020-2_mys-ahs-suspension (accessed on 12 January 2024).
- WOAH. Animal Diseases. January 2024. Available online: https://www.woah.org/en/what-we-do/animal-health-and-welfare/animal-diseases/ (accessed on 21 January 2024).
- WOAH. Official Disease Status. January 2024. Available online: https://www.woah.org/en/what-we-do/animal-health-and-welfare/official-disease-status/ (accessed on 21 January 2024).
- European Union. Regulation (EU) 2016/429 of the European Parliament and of the Council of 9 March 2016 on Transmissible Animal Diseases and Amending and Repealing Certain Acts in the Area of Animal Health (“Animal Health Law”). Official Journal of the European Union-L84.31.3.2016. 1 November 2016. Available online: http://data.europa.eu/eli/reg/2016/429/oj (accessed on 21 January 2024).
- WOAH. Infection with African Horse Sickness Virus. In Terrestrial Animal Health Code; January 2024; Chapter 12.1; Available online: https://www.woah.org/en/what-we-do/standards/codes-and-manuals/terrestrial-code-online-access/?id=169&L=1&htmfile=chapitre_ahs.htm (accessed on 21 January 2024).
- Von Teichman, B.F.; Dungu, B.; Smit, T.K. In vivo cross-protection to African horse sickness Serotypes 5 and 9 after vaccination with Serotypes 8 and 6. Vaccine 2010, 28, 6505–6517. [Google Scholar] [CrossRef] [PubMed]
- Weyer, C.T.; Grewar, J.D.; Burger, P.; Joone, C.; Lourens, C.; MacLachlan, N.J.; Guthrie, A.J. Dynamics of African horse sickness virus nucleic acid and antibody in horses following immunization with a commercial polyvalent live attenuated vaccine. Vaccine 2017, 35, 2504–2510. [Google Scholar] [CrossRef] [PubMed]
- Roy, P. Orbivirus Structure and Assembly. Virology 1996, 216, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Weyer, C.T.; Grewar, J.D.; Burger, P.; Rossouw, E.; Lourens, C.; Joone, C.; Le Grange, M.; Coetzee, P.; Venter, E.; Martin, D.P.; et al. African Horse Sickness Caused by Genome Reassortment and Reversion to Virulence of Live, Attenuated Vaccine Viruses, South Africa, 2004–2014. Emerg. Infect. Dis. 2016, 22, 2087–2096. [Google Scholar] [CrossRef]
- WOAH. Reference Experts and Laboratories. 2024. Available online: https://www.woah.org/en/what-we-offer/expertise-network/reference-laboratories/#ui-id-3 (accessed on 21 January 2024).
- European Union Reference Laboratories. Available online: https://food.ec.europa.eu/horizontal-topics/european-union-reference-laboratories_en (accessed on 21 January 2024).
- WOAH. African Horse Sickness (Infection with African Horse Sickness Virus). In Manual of Diagnostic Tests and Vaccines for Terrestrial Animals; 2019; Chapter 3.6.1; Available online: https://www.woah.org/fileadmin/Home/eng/Health_standards/tahm/3.06.01_AHS.pdf (accessed on 21 January 2024).
- European Union Reference Laboratory for African Horse Sickness and Bluetongue. Diagnosis. Available online: https://www.mapa.gob.es/en/ganaderia/temas/laboratorios-sanidad-genetica/referencia-ue/diagnostico/ (accessed on 21 January 2024).
- Koekemoer, J.J.O.; Potgieter, A.C.; Paweska, J.T.; van Dijk, A.A. Development of probes for typing African horse sickness virus isolates using a complete set of cloned VP2-genes. J. Virol. Methods 2000, 88, 135–144. [Google Scholar] [CrossRef]
- Koekemoer, J.J.O.; van Dijk, A.A. African horse sickness virus serotyping and identification of multiple co-infecting serotypes with a single genome segment 2 RT-PCR amplification and reverse line blot hybridization. J. Virol. Methods 2004, 122, 49–56. [Google Scholar] [CrossRef]
- Sailleau, C.; Hamblin, C.; Paweska, J.; Zientara, S. Identification and differentiation of the nine African horse sickness virus serotypes by RT-PCR amplification of the serotype-specific genome segment 2. J. Gen. Virol. 2000, 81, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Maan, N.S.; Maan, S.; Nomikou, K.; Belaganahalli, M.N.; Bachanek-Bankowska, K.; Mertens, P.P. Serotype Specific Primers and Gel-Based RT-PCR Assays for ‘Typing’ African Horse Sickness Virus: Identification of Strains from Africa. PLoS ONE 2011, 6, e25686. [Google Scholar] [CrossRef] [PubMed]
- Koekemoer, J.J. Serotype-specific detection of African horse sickness virus by real-time PCR and the influence of genetic variations. J. Virol. Methods 2008, 154, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Bachanek-Bankowska, K.; Maan, S.; Castillo-Olivares, J.; Manning, N.M.; Maan, N.S.; Potgieter, A.C.; Di Nardo, A.; Sutton, G.; Batten, C.; Mertens, P.P.C. Real time RT-PCR assays for detection and typing of African horse sickness virus. PLoS ONE 2014, 9, e93758. [Google Scholar] [CrossRef] [PubMed]
- Weyer, C.T.; Joone, C.; Lourens, C.W.; Monyai, M.S.; Koekemoer, O.; Grewar, J.D.; van Schalkwyk, A.; Majiwa, P.O.; MacLachlan, N.J.; Guthrie, A.J. Development of three triplex real-time reverse transcription PCR assays for the qualitative molecular typing of the nine serotypes of African horse sickness virus. J. Virol. Methods 2015, 223, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, S.J.; McHolland, L.E. Susceptibilities of 14 cell lines to bluetongue virus infection. J. Clin. Microbiol. 1988, 26, 2324–2327. [Google Scholar] [CrossRef] [PubMed]
- WOAH. The Official #2016-1. Validation of Real-Time RT-PCR for the Detection of African Horse Sickness Virus Genome. 2016. Available online: https://www.woah.org/fileadmin/Home/eng/Publications_%26_Documentation/docs/pdf/bulletin/Bull_2016-1-ENG.pdf (accessed on 12 January 2024).
- Durán-Ferrer, M.; Villalba, R.; Fernández-Pacheco, P.; Tena-Tomás, C.; Jiménez-Clavero, M.Á.; Bouzada, J.A.; Ruano, M.J.; Fernández-Pinero, J.; Arias, M.; Castillo-Olivares, J.; et al. Clinical, Virological and Immunological Responses after Experimental Infection with African Horse Sickness Virus Serotype 9 in Immunologically Naïve and Vaccinated Horses. Viruses 2022, 14, 1545. [Google Scholar] [CrossRef] [PubMed]
- Agüero, M.; Gómez-Tejedor, C.; Angeles Cubillo, M.; Rubio, C.; Romero, E.; Jiménez-Clavero, A. Real-time fluorogenic reverse transcription polymerase chain reaction assay for detection of African horse sickness virus. J. Vet. Diagn. Investig. 2008, 20, 325–328. [Google Scholar] [CrossRef]
- EURL, GL-LCV-07. Rev. 02. 22/06/2021 Standard Operating Procedure: RRT-PCR for African Horse Sickness Detection Method (Agüero et al., 2008). European Union Reference Laboratory for African Horse Sickness and Bluetongue Website. Available online: https://www.mapa.gob.es/en/ganaderia/temas/laboratorios-sanidad-genetica/gl-lcv-07ed2jun2021rrt-pcrforahsdetectionmethodaguero2008_tcm38-576039.pdf (accessed on 21 January 2024).
- Potgieter, A.C.; Cloete, M.; Pretorius, P.J.; van Dijk, A.A. A first full outer capsid protein sequence data-set in the Orbivirus genus (family Reoviridae): Cloning, sequencing, expression and analysis of a complete set of full-length outer capsid VP2 genes of the nine African horse sickness virus serotypes. J. Gen. Virol. 2003, 84, 1317–1326. [Google Scholar] [CrossRef]
- Maan, S.; Maan, N.S.; Belaganahalli, M.N.; Potgieter, A.C.; Kumar, V.; Batra, K.; Wright, I.M.; Kirkland, P.D.; Mertens, P.P. Development and Evaluation of Real Time RT-PCR Assays for Detection and Typing of Bluetongue Virus. PLoS ONE 2016, 11, e0163014. [Google Scholar] [CrossRef]
- Maan, N.S.; Maan, S.; Belaganahalli, M.N.; Ostlund, E.N.; Johnson, D.J.; Nomikou, K.; Mertens, P.P.C. Identification and differentiation of the twenty-six bluetongue virus serotypes by RT-PCR amplification of the serotype specific genome segment 2. PLoS ONE 2012, 7, e32601. [Google Scholar] [CrossRef] [PubMed]
- Mertens, P.P.; Maan, N.S.; Prasad, G.; Samuel, A.R.; Shaw, A.E.; Potgieter, A.C.; Anthony, S.J.; Maan, S. Design of primers and use of RT-PCR assays for typing European bluetongue virus isolates: Differentiation of field and vaccine strains. J. Gen. Virol. 2007, 88 Pt 10, 2811–2823. [Google Scholar] [CrossRef]
- Squire, K.R.; Chuang, R.Y.; Chuang, L.F.; Doi, R.H.; Osburn, B.I. Detecting bluetongue virus RNA in cell culture by dot hybridization with a cloned genetic probe. J. Virol. Methods 1985, 10, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Viarouge, C.; Breard, E.; Zientara, S.; Vitour, D.; Sailleau, C. Duplex Real-Time RT-PCR Assays for the Detection and Typing of Epizootic Haemorrhagic Disease Virus. PLoS ONE 2015, 10, e0132540. [Google Scholar] [CrossRef] [PubMed]
- Maan, N.S.; Maan, S.; Potgieter, A.C.; Wright, I.M.; Belaganahalli, M.; Mertens, P.P.C. Development of Real-Time RT-PCR Assays for Detection and Typing of Epizootic Haemorrhagic Disease Virus. Transbound. Emerg. Dis. 2017, 64, 1120–1132. [Google Scholar] [CrossRef] [PubMed]
- The RNAs and Proteins of dsRNA Viruses. Edited by Peter. P. C. Mertens, Houssam Attoui and Dennis H. Bamford. Available online: https://www.reoviridae.org/dsRNA_virus_proteins/ReoID/AHSV-Nos.htm (accessed on 21 January 2024).
- Rodriguez, M.; Hooghuis, H.; Castaño, M. African horse sickness in Spain. Vet. Microbiol. 1992, 33, 129–142. [Google Scholar] [CrossRef] [PubMed]
- WOAH. WAHIS. EVENT 3159. Thailand—African Horse Sickness Virus (Inf. with). Historical Reports. Available online: https://wahis.woah.org/#/in-event/3159/dashboard (accessed on 22 January 2024).
- WOAH. WAHIS. EVENT 4785. Nigeria—African Horse Sickness Virus (Inf. with). Historical Reports. Available online: https://wahis.woah.org/#/in-event/4785/dashboard (accessed on 22 January 2024).
- Adesola, R.O.; Bakre, A.A.; Gulumbe, B.H. Addressing the recent outbreak of African horse sickness in Lagos, Nigeria. Front. Vet. Sci. 2023, 10, 1160856. [Google Scholar] [CrossRef]


{kind=link}
| AHSV | Primers (F/R) and Probe | Sequence 5′-3′ |
|---|---|---|
| Serotype 1 | AHS-1F | GCAAGCGCTGGCACTTG |
| AHS-1R | TTCGAACTCATTCCTTACATCAACA | |
| AHS1P | FAM-AATGTCTTAGATCGTCAACT-MGB | |
| Serotype 2 | AHS-2F | CGGAAACTYTGTATTGCCAAA |
| AHS-2R | TTGTCRTCCTGATCAACCCTAA | |
| AHS-2P | Cy5-TGAAGGTGCTTACCCGATCTTTCCACA-BBQ | |
| Serotype 3 | AHS-3F | AATTATTACAGCGGAGAATGCAGTT |
| AHS-3R | GGTTATGAGTGGGGTGCGA | |
| AHS-3P | FAM-AGAGTTGAGGTTGCGGGA-MGB | |
| Serotype 4 | AHS-4F | TGAGGTGGAACACGAYATGTC |
| AHS-4R | GATATGCCCCCTCACAYCTGA | |
| AHS-4P | VIC-TATCGGRATTTATGTACAATGAG-MGB | |
| Serotype 5 | AHS-5F | GAAGAGACAGGCGATTCAAATGA |
| AHS-5R | AAAGCCACCCTTTTTGGTACAAA | |
| AHS-5P | NED-TGTTGARATGCTGAGGC-MGB | |
| Serotype 6 | AHS-6F | AGCCAGGGCTTCTTTGCA |
| AHS-6R | CTCATGTTCAACCCACTGTACATTAA | |
| AHS-6P | VIC-GTCATCACCGTAAGCG-MGB | |
| Serotype 7 | AHS-7F | AGCCAGGGCTTCTTTGCA |
| AHS-7R | CTCATGTTCAACCCACTGTACATTAA | |
| AHS-7P | VIC-GTCATCACCGTAAGCG-MGB | |
| Serotype 8 | AHS-8F | GAAATTATCAGCGGACTGACTAAGAA |
| AHS-8R | AAACATCTACCTTTTGCGAATCTTG | |
| AHS-8P | NED-ACGTGATTCTTTTCCC-MGB | |
| Serotype 9 | AHS-9F | TACTGTGTCGGTGAGGGATTTT |
| AHS-9R | GCCACGACCGGATATGA | |
| AHS-9P | FAM-AAACAAACGAAATGTGAA-MGB |
| Strain | Positive Serotypes in Triplex TS-rRT-PCRs Assays (Ct Value) * | Specific Antisera Used in the Cloning Process | |
|---|---|---|---|
| Before Cloning | After Cloning | ||
| AHSV1 29/62 reference strain | 1 (14.7) and 4 (26.4) | 1 (18.3) | without antiserum |
| AHSV2 82/61 reference strain | 2 (15.2) | 2 (18.9) | without antiserum |
| AHSV3 13/63 reference strain | 1 (24.8) and 3 (15.0) | 3 (19.4) | without antiserum |
| AHSV4 32/62 reference strain | 4 (13.5) | 4 (18.1) | without antiserum |
| AHSV5 30–62 reference strain | 3 (15.6) and 5 (18.9) | 5 (17.2) | without antiserum |
| AHSV6 39/62 reference strain | 6 (19.8) and 7 (21.3) | 6 (19.7) | without antiserum |
| AHSV7 62/31 reference strain | 3 (15.5) and 7 (18.3) | 7 (22.7) | without antiserum |
| AHSV8 62/10 reference strain | 5 (28.2) and 8 (15.5) | 8 (22.1) | without antiserum |
| AHSV9 90/61 reference strain | 9 (15.0) | 9 (17.4) | without antiserum |
| AHSV commercial vaccine OBP vial 1 (serotypes 1, 3 and 4) | 1 (17.2), 3 (15.5) and 4 (17.9) | 1 (14.0) | serotypes 3 and 4 |
| 3 (13.9) | serotypes 1 and 4 | ||
| 4 (14.7) | serotypes 1 and 3 | ||
| AHSV commercial vaccine OBP vial 2 (serotypes 2, 6, 7 and 8) | 2 (22.0), 6 (21.8), 7 (23.9) and 8 (21.7) | 2 (17.4) | serotypes 6, 7 and 8 |
| 6 (18.4) | serotypes 2, 7 and 8 | ||
| 7 (17.7) | serotypes 2, 6 and 8 | ||
| 8 (13.6) | serotypes 2, 6 and 7 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villalba, R.; Tena-Tomás, C.; Ruano, M.J.; Valero-Lorenzo, M.; López-Herranz, A.; Cano-Gómez, C.; Agüero, M. Development and Validation of Three Triplex Real-Time RT-PCR Assays for Typing African Horse Sickness Virus: Utility for Disease Control and Other Laboratory Applications. Viruses 2024, 16, 470. https://doi.org/10.3390/v16030470
Villalba R, Tena-Tomás C, Ruano MJ, Valero-Lorenzo M, López-Herranz A, Cano-Gómez C, Agüero M. Development and Validation of Three Triplex Real-Time RT-PCR Assays for Typing African Horse Sickness Virus: Utility for Disease Control and Other Laboratory Applications. Viruses. 2024; 16(3):470. https://doi.org/10.3390/v16030470
Chicago/Turabian StyleVillalba, Rubén, Cristina Tena-Tomás, María José Ruano, Marta Valero-Lorenzo, Ana López-Herranz, Cristina Cano-Gómez, and Montserrat Agüero. 2024. "Development and Validation of Three Triplex Real-Time RT-PCR Assays for Typing African Horse Sickness Virus: Utility for Disease Control and Other Laboratory Applications" Viruses 16, no. 3: 470. https://doi.org/10.3390/v16030470