Abstract
Objectives: COVID-19 infection confers an increased risk of coagulation dysfunction (1) predisposing to thromboembolism in many anatomical sites including the gastrointestinal tract (GIT) (2). This study investigates the clinical presentation and outcome in patients presenting with concurrent COVID-19 infection and gastrointestinal tract ischaemia. Furthermore, differentiation and comparisons are drawn between those with arterial and venous aetiology for mesenteric ischaemia. Methods: A systematic search was undertaken on EMBASE, PubMed, and MEDLINE. Two independent reviewers screened titles, abstracts, and full-text articles according to the inclusion criteria and extracted relevant data. Data analyses were conducted using Excel®. Results: Forty-one studies were included in the data analyses, yielding 44 patients. Twenty-six patients had mesenteric arterial occlusion, sixteen patients had mesenteric venous occlusion, and two patients had both arterial and venous mesenteric occlusion. All patients had concurrent COVID-19 infection. The survival rate in patients with arterial aetiology was 38.5% in contrast to 68.8% in patients with venous aetiology. Twelve patients (29.3%) experienced respiratory symptoms in the community before the onset of gastrointestinal symptoms, and five (12.2%) developed gastrointestinal symptoms during their inpatient stay for COVID-19 pneumonitis. Conclusions: Acute mesenteric ischaemia presents a clinical challenge to diagnose due to its non-specific symptoms. Concurrent COVID-19 infection with its predominant respiratory symptoms adds a further challenge in recognising the non-specific symptoms of mesenteric ischaemia. Our study draws attention to the increased thromboembolic risk posed by COVID-19 infection and the need for a high index of suspicion to aid prompt diagnosis and management of acute mesenteric ischaemia, even in the post-pandemic era.
1. Introduction
The novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged in Wuhan, China in December. It quickly spread worldwide and was declared a pandemic by the World Health Organisation (WHO) in March. SARS-CoV-2 causes coronavirus disease 2019 (COVID-19), which predominantly affects the respiratory tract, but it can have a broad spectrum of presentations ranging from being asymptomatic to multi-organ dysfunction [1].
In patients with complicated COVID-19 infections needing acute hospital admission, it has been well-established that these patients are at an increased risk of thromboembolism [2,3,4]. Knight et al. refined the study of thromboembolism risk after COVID-19 infection into arterial and venous thrombosis [5]. It was found that the adjusted hazard ratios were higher in both groups when compared to their respective non-COVID-19 cohort [5]. Coagulation dysfunction in patients with COVID-19 is reflected through elevated markers of coagulability, such as high levels of D-dimer and prolonged prothrombin time [6]. The binding between SARS-CoV-2 and its host receptor, angiotensin-converting enzyme 2 (ACE2), upregulates the expression of tissue factors on cell surfaces. This activates the extrinsic coagulation pathway, sending the human body into a prothrombotic state [7,8]. In addition, it has been shown that there is an influx of proinflammatory cytokines and chemoattractants in circulation during COVID-19 infection, especially in the case of a severe infection [9,10]. This induced cytokine storm can cause extensive endothelial injury, thus activating the process of haemostasis [11]. An existing observational study has outlined the relationship between severe COVID-19 infection and the increased thrombosis risk [12].
Multiple studies have shown that the most common manifestations of thromboembolism in hospitalised COVID-19 patients are deep vein thrombosis and pulmonary embolism, and the risk increases further if the patient is admitted to an intensive care unit [3,4,13]. Although thromboembolism in mesenteric vessels is rare, it has been reported in COVID-19 patients in several case series [14,15,16]. Acute mesenteric ischaemia (AMI) is defined as a sudden disruption in circulation to the intestines necessitating urgent intervention in most cases to preserve the viability of the bowel [17]. The aetiology of AMI can be attributed to the occlusion of mesenteric arteries and mesenteric veins due to an embolus or a thrombus. In many cases, vasoconstriction of mesenteric vessels can interrupt blood supply without intraluminal occlusion, leading to non-occlusive AMI [17,18,19].
The current literature on COVID-19-induced AMI has looked into patient presentations and established a high mortality rate in these patients [20,21,22]. A further subset of studies investigated the radiological signs of AMI during COVID-19 and highlighted the importance of cross-sectional imaging to diagnose AMI promptly [16,23,24,25]. However, there is limited research on the effect different types of AMI have on patient outcomes during COVID. This study aims to conduct a scoping review of outcomes in patients with concurrent COVID-19 and AMI, considering the classifications of AMI.
2. Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) were followed [26]. The protocol for this study has been previously published [27].
2.1. Research Question
What is the impact of aetiological differences of AMI on the outcomes in COVID-19 patients?
2.2. Search Strategy
A systematic search was undertaken in EMBASE, PubMed, and Medline. The full search strategy was: (“Coronavirus disease” OR “coronavirus infections” OR “COVID-19” OR “2019-nCoV” OR “SARS-CoV-2”) AND clinical AND (“Intestinal isch*” OR “bowel isch*” OR “mesenteric isch*” OR “thromb*”) AND Imaging. This was adapted for each included database. There were exchangeable terms describing the location of acute mesenteric ischaemia, such as “bowel” and “intestinal”. Moreover, multiple terms describing the loss of blood supply to the bowel, such as “embolism”, “thrombosis”, “thromboembolism”, and “ischaemia” were collectively analysed. All included articles’ reference lists were screened for additional studies. Studies published in the English language from November 2019 to date were included.
2.3. Eligibility Criteria
Studies describing adult COVID-19 patients diagnosed with clinical manifestation and radiologically confirmed bowel ischaemia were included. Included studies also indicated the site of pathology from the radiological reports. Only studies published in the English language were included. Paediatric populations and patients with thromboembolic events in other organs, such as myocardial infarction, stroke, and pulmonary embolism, were excluded. Studies discussing other coronaviruses were excluded.
The study’s aim was to investigate the distribution of patient demographics and clinical symptoms of AMI with arterial, venous, and non-occlusive aetiology.
2.4. Study Selection Procedure
Extracted studies were uploaded to Rayyan for the organisation of the screening process [28]. Two independent reviewers (W.C. and Y.Z.) screened through the returned searches by evaluating the title and abstract according to the inclusion criteria. The selected studies were compared between the reviewers, any discrepancies were discussed, and a third reviewer (S.M.) was sought if agreement could not be reached. Full-text articles were accessed for studies that met the inclusion criteria. Upon studying full-text articles, only studies that specified the aetiology of AMI by obtaining cross-sectional imaging were included in the final study selection; our study aim necessitated this.
2.5. Data Extraction
Information on patient demographics was extracted from each study, including sex and age. The following clinical data were extracted: patient comorbidities, presenting complaints, imaging findings, and management plans. All data were collated and analysed in Microsoft Excel version 16.83® [29].
3. Results
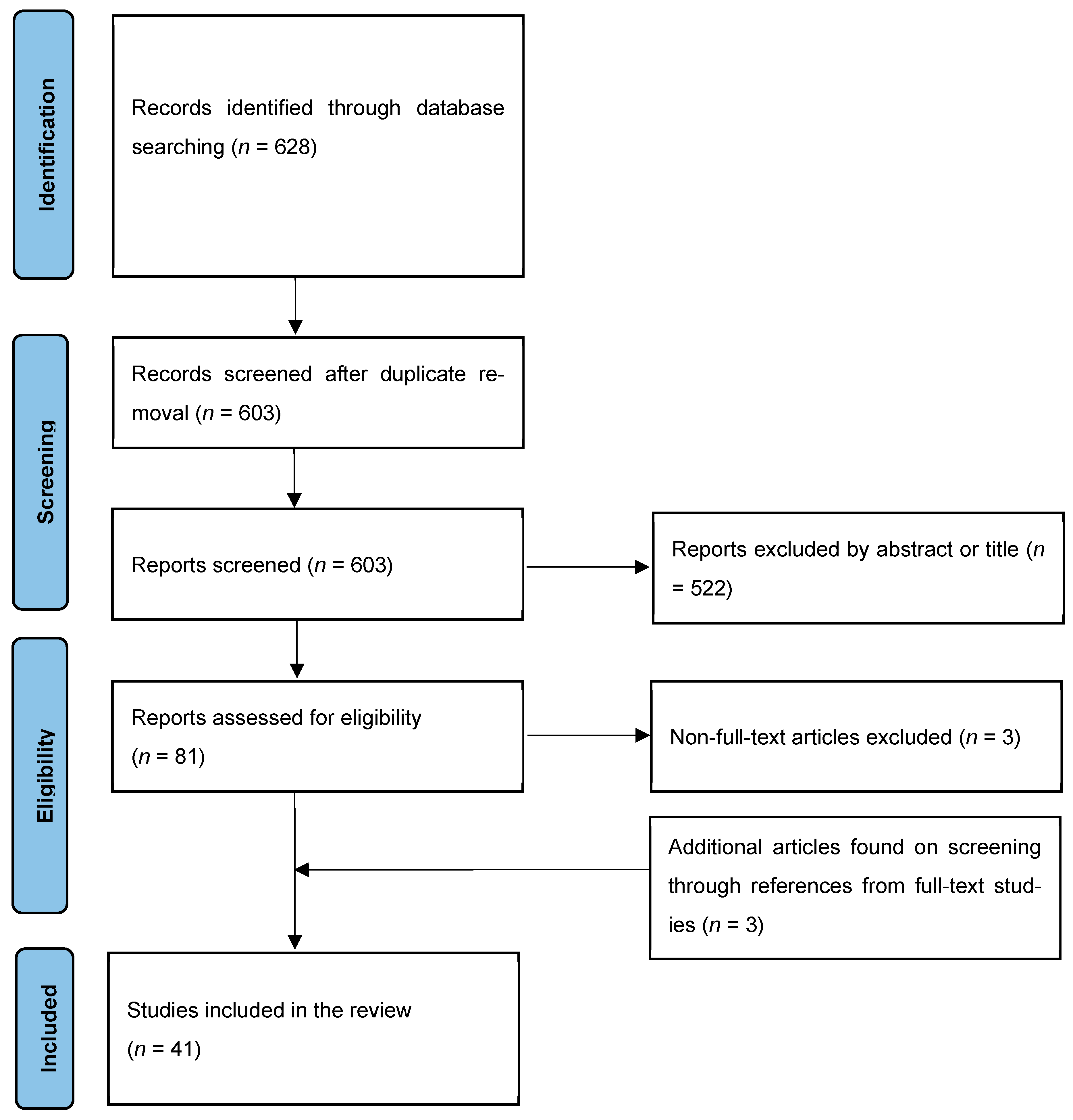
The database search yielded 628 articles. After removal of duplicates and screening of the title and abstract, 81 studies remained. These studies underwent full-text evaluation, and a further three studies were retrieved upon screening these studies’ references. Forty-one studies reporting on 44 patients were included in the final selection [14,16,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68]. Of these, 32 were case reports, and the remaining 9 were case series. Figure 1 demonstrates the PRISMA flow diagram of this study. Table 1 shows the summaries of the included studies.
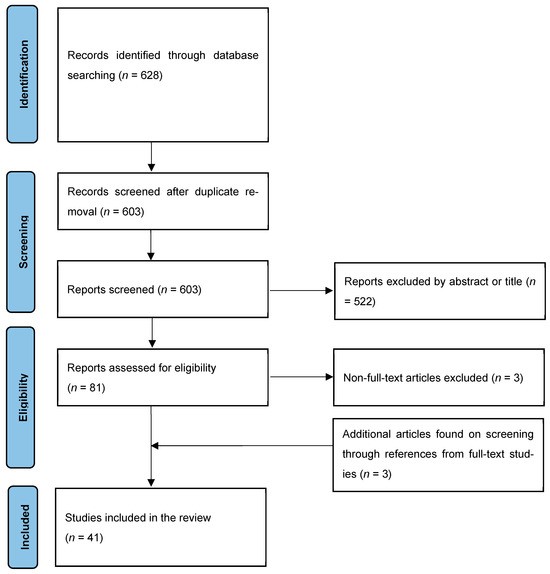
Figure 1.
PRISMA flow diagram of evidence acquisition. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis.

Table 1.
Summary of final selection of studies including first author, year of publication, number of patients, type of study, and aetiology of AMI.
The mean age of patients in the study selection was 55.6 (±16.9) years, and 26 out of 44 (59%) patients were male. Table 2 shows a summary of the studies and the patient demographics.
Table 2.
Patient characteristics of the included cases stratified by arterial, venous, and mixed aetiology.
The most common presenting complaints on admission were abdominal pain (77.3%) and vomiting (38.6%). Five patients presented with solely respiratory symptoms, and all developed abdominal pain later during their admission [43,53,54,65,66]. Thirteen patients who tested positive for COVID-19 made contact with healthcare services before presenting to the emergency department with gastrointestinal symptoms [16,30,31,32,35,37,38,40,41,45,48,54,63]. All patients had cross-sectional imaging to confirm the diagnosis of acute mesenteric ischaemia.
3.1. Arterial Mesenteric Ischaemia
Twenty-six patients (59.1%) had exclusively arterial mesenteric ischaemia. Twenty-three of them were found to have isolated superior mesenteric artery (SMA) occlusion, one patient had occlusion in both the coeliac trunk and the SMA, and the remaining two patients were found to have occlusion in the branches of the SMA. Twenty patients in this cohort underwent laparotomy, two underwent endovascular treatment, and one patient was deemed not a candidate for surgical treatment. The mean length of stay was 29.4 days amongst five reported cases. The survival rate for this group was 38.6%.
3.2. Venous Mesenteric Ischaemia
Sixteen patients (36.4%) had exclusively venous mesenteric ischaemia, eleven of them had isolated occlusion in the superior mesenteric vein (SMV), and the remainder had involvement of other mesenteric veins and the portal vein. Eight patients underwent laparotomy, and one patient was deemed unsuitable for surgical intervention. The survival rate for this group was 68.8%.
3.3. Mixed Arterial and Venous Mesenteric Ischaemia
Two patients were found to have mixed arterial and venous mesenteric ischaemia. Both underwent exploratory laparotomy, and one patient survived.
3.4. Anticoagulation Management
Eleven patients among twenty-six patients with arterial mesenteric ischemia received either anticoagulation treatment or a combination of anticoagulants and antiplatelets. Twelve patients among sixteen patients with venous mesenteric ischaemia received anticoagulation treatment. One patient out of two with mixed arterial and venous thrombosis received anticoagulation treatment. Fourteen patients out of twenty-four patients (58.3%) who received anticoagulation treatment survived. Five patients’ survival statuses after receiving anticoagulation were not reported.
4. Discussion
This study has investigated the presentations and outcomes in patients with COVID-19 and AMI. We found that the majority of patients had arterial mesenteric ischaemia provoked by COVID-19 infection, and the survival rate was better among patients in the venous mesenteric ischaemia group compared to those with arterial mesenteric ischaemia.
Gastrointestinal symptoms are widely prevalent in patients with COVID-19 [69,70]. It has been observed that diarrhoea is a common symptom during the early course of infection [71]. These findings contrast this study, where abdominal pain was the most typical gastrointestinal symptom. In addition, it has been postulated that gastrointestinal symptoms may indicate or predict a more severe case of COVID-19 [69,72].
This study highlights that respiratory symptoms and abdominal symptoms do not always present at the same time. Many patients had sought medical attention for respiratory symptoms days or weeks before the onset and subsequent severity of abdominal pain necessitated their emergency department visit. It may be common for clinicians to treat the two clusters of symptoms as separate disease entities, leading to delays in diagnosis.
Aetiology of AMI can be either due to an embolus or thrombosis. The clot leading to the occlusion of mesenteric vessels can be an embolus or worsening of existing thrombosis [17]. It has been estimated that half of AMI cases are due to SMA embolus [73,74]. This finding corresponds with this study, where more than half of the patients had an isolated SMA occlusion, but it is unknown if these occlusions were of embolic or thrombotic origin. Whilst patients with AMI secondary to an embolus in SMA typically present with worsening acute abdominal pain, in contrast, patients with AMI secondary to thrombosis of SMA typically have a background history suggestive of chronic mesenteric ischaemia; associated symptoms are postprandial abdominal pain and fear of eating [17].
Another way to classify AMI is to differentiate between arterial and venous pathology. Mesenteric venous ischaemia is less common than mesenteric arterial ischaemia [18]. Mesenteric venous ischaemia tends to affect a younger population, and any congenital hypercoagulable condition should be investigated and ruled out as a potential cause [18].
AMI can also be caused by nonocclusive aetiology. Non-occlusive mesenteric ischaemia is due to vasoconstriction of the mesenteric vessels without an intraluminal clot [75]. It accounts for approximately 20% of cases, and it has been observed in critically unwell patients in an intensive care setting [75].
Computed tomography angiography (CTA) of mesenteric vessels is essential in the timely diagnosis of AMI and in the differentiation between different types of AMI, primarily due to the lack of laboratory tests available to accurately diagnose mesenteric ischaemia as a differential diagnosis [17].
Anticoagulation is strongly recommended for all cases of AMI from the time of diagnosis. However, the indication is more robust in the case of venous mesenteric ischaemia than in the other types [17,18,76,77]. Extended anticoagulation through post-operative and post-discharge is crucial to reduce the incidence of future clots.
Once AMI is confirmed, open surgery should be performed promptly to assess bowel vitality [17]. The endovascular approach has become increasingly favourable when the facility allows for achieving revascularisation [78].
Mesenteric ischaemia has a mortality rate of more than 50% [79,80]. Delay in diagnosis is a significant factor contributing to the high mortality rate—only five studies reported the time lapse between patient presentation and diagnosis in this study.
Limitations
As COVID-19 is still a relatively new disease and AMI is a rare differential diagnosis of abdominal pain, studies with methodologies that occupy a higher level in the hierarchy of evidence are currently lacking in number. Thus, inferences cannot be drawn to the general population regarding prevalence, risks, and hazard ratios, and causal relationships cannot be established by looking at case studies. Furthermore, the information reported in each case report or case series differs widely, resulting in possible gaps in our data. Finally, other more common contributing factors of AMI other than COVID-19 infection, such as atrial fibrillation and other cardiac causes of embolism, have not been adequately investigated in the selected studies.
5. Conclusions
Acute mesenteric ischaemia is challenging to diagnose due to its low prevalence and non-specific symptoms. COVID-19’s predominant respiratory symptoms may drive the diagnostic focus away from considering AMI as a differential diagnosis. This study has shown poor survival outcomes in patients with concurrent COVID-19 infection and AMI. With emerging, new strains of COVID-19, the disease is ever-evolving, prompting a much higher index of suspicion, which aids in the prompt diagnosis and management of this life-threatening surgical emergency in the post-pandemic era.
Author Contributions
The authors’ contribution includes, but is not limited to, the following: Y.Z. and W.C. provided inputs to the methods, designed the search strategy, and drafted the manuscript. S.M. and Y.Z. created the study concept. S.M. provided inputs to the methods, provided supervision during the study, and critically revised the manuscript. W.C. is the guarantor of this work. All authors have read and agreed to the published version of the manuscript.
Funding
Imperial College London has kindly provided funding for the publication of this article.
Data Availability Statement
Raw data can be accessed upon personal request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Kollias, A.; Kyriakoulis, K.G.; Dimakakos, E.; Poulakou, G.; Stergiou, G.S.; Syrigos, K. Thromboembolic risk and anticoagulant therapy in COVID-19 patients: Emerging evidence and call for action. Br. J. Haematol. 2020, 189, 846–847. [Google Scholar] [CrossRef]
- Kollias, A.; Kyriakoulis, K.G.; Lagou, S.; Kontopantelis, E.; Stergiou, G.S.; Syrigos, K. Venous thromboembolism in COVID-19: A systematic review and meta-analysis. Vasc. Med. 2021, 26, 415–425. [Google Scholar] [CrossRef]
- Malas, M.B.; Naazie, I.N.; Elsayed, N.; Mathlouthi, A.; Marmor, R.; Clary, B. Thromboembolism risk of COVID-19 is high and associated with a higher risk of mortality: A systematic review and meta-analysis. EClinicalMedicine 2020, 29, 100639. [Google Scholar] [CrossRef]
- Knight, R.; Walker, V.; Ip, S.; Cooper, J.A.; Bolton, T.; Keene, S.; Denholm, R.; Akbari, A.; Abbasizanjani, H.; Torabi, F.; et al. Association of COVID-19 with Major Arterial and Venous Thrombotic Diseases: A Population-Wide Cohort Study of 48 Million Adults in England and Wales. Circulation 2022, 146, 892–906. [Google Scholar] [CrossRef]
- Zhang, Y.; Cao, W.; Jiang, W.; Xiao, M.; Li, Y.; Tang, N.; Liu, Z.; Yan, X.; Zhao, Y.; Li, T.; et al. Profile of natural anticoagulant, coagulant factor and anti-phospholipid antibody in critically ill COVID-19 patients. J. Thromb. Thrombolysis 2020, 50, 580–586. [Google Scholar] [CrossRef]
- Grover, S.P.; Mackman, N. Tissue Factor: An Essential Mediator of Hemostasis and Trigger of Thrombosis. Arter. Thromb. Vasc. Biol. 2018, 38, 709–725. [Google Scholar] [CrossRef]
- Sriram, K.; Insel, P.A. A hypothesis for pathobiology and treatment of COVID-19: The centrality of ACE1/ACE2 imbalance. Br. J. Pharmacol. 2020, 177, 4825–4844. [Google Scholar] [CrossRef]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.-C.; Uhl, S.; Hoagland, D.; Møller, R.; Albrecht, R.A. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 2020, 181, 1036–1045.e9. [Google Scholar] [CrossRef]
- Mulchandani, R.; Lyngdoh, T.; Kakkar, A.K. Deciphering the COVID-19 cytokine storm: Systematic review and meta-analysis. Eur. J. Clin. Investig. 2021, 51, e13429. [Google Scholar] [CrossRef]
- Perico, L.; Benigni, A.; Casiraghi, F.; Ng, L.F.P.; Renia, L.; Remuzzi, G. Immunity, endothelial injury and complement-induced coagulopathy in COVID-19. Nat. Rev. Nephrol. 2021, 17, 46–64. [Google Scholar] [CrossRef]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Katsoularis, I.; Fonseca-Rodríguez, O.; Farrington, P.; Jerndal, H.; Lundevaller, E.H.; Sund, M.; Lindmark, K.; Connolly, A.-M.F. Risks of deep vein thrombosis, pulmonary embolism, and bleeding after COVID-19: Nationwide self-controlled cases series and matched cohort study. BMJ 2022, 377, e069590. [Google Scholar] [CrossRef]
- Etkin, Y.; Conway, A.M.; Silpe, J.; Qato, K.; Carroccio, A.; Manvar-Singh, P.; Giangola, G.; Deitch, J.S.; Davila-Santini, L.; Schor, J.A.; et al. Acute Arterial Thromboembolism in Patients with COVID-19 in the New York City Area. Ann. Vasc. Surg. 2021, 70, 290–294. [Google Scholar] [CrossRef]
- O’Shea, A.; Parakh, A.; Hedgire, S.; Lee, S.I. Multisystem Assessment of the Imaging Manifestations of Coagulopathy in Hospitalized Patients with Coronavirus Disease (COVID-19). AJR Am. J. Roentgenol. 2021, 216, 1088–1098. [Google Scholar] [CrossRef]
- Khaleghi, M.; Aziz-Ahari, A.; Rezaeian, N.; Asadian, S.; Mounesi Sohi, A.; Motamedi, O.; Azhdeh, S. The Valuable Role of Imaging Modalities in the Diagnosis of the Uncommon Presentations of COVID-19: An Educative Case Series. Case Rep. Med. 2021, 2021, 7213627. [Google Scholar] [CrossRef]
- Bala, M.; Catena, F.; Kashuk, J.; De Simone, B.; Gomes, C.A.; Weber, D.; Sartelli, M.; Coccolini, F.; Kluger, Y.; Abu-Zidan, F.M.; et al. Acute mesenteric ischemia: Updated guidelines of the World Society of Emergency Surgery. World J. Emerg. Surg. 2022, 17, 54. [Google Scholar] [CrossRef]
- Tilsed, J.V.T.; Casamassima, A.; Kurihara, H.; Mariani, D.; Martinez, I.; Pereira, J.; Ponchietti, L.; Shamiyeh, A.; Al-Ayoubi, F.; Barco, L.A.B.; et al. ESTES guidelines: Acute mesenteric ischaemia. Eur. J. Trauma Emerg. Surg. 2016, 42, 253–270. [Google Scholar] [CrossRef]
- Björck, M.; Koelemay, M.; Acosta, S.; Goncalves, F.B.; Kölbel, T.; Kolkman, J.J.; ESVS Guidelines Committee. Editor’s Choice—Management of the Diseases of Mesenteric Arteries and Veins: Clinical Practice Guidelines of the European Society of Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2017, 53, 460–510. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.T.C.; Fonseca Neto OCLD. Acute mesenteric ischemia and COVID-19: An integrative review of the literature. Rev. Col. Bras. Cir. 2023, 50, e20233334. [Google Scholar] [CrossRef] [PubMed]
- Gebran, A.; El Moheb, M.; Argandykov, D.; Mashbari, H.; Gartland, R.M.; Hwabejire, J.O.; Velmahos, G.C.; Kaafarani, H.M. Mesenteric Ischemia in Patients with Coronavirus 2019: A Scoping Review. Surg. Infect. 2022, 23, 781–786. [Google Scholar] [CrossRef]
- Patel, S.; Parikh, C.; Verma, D.; Sundararajan, R.; Agrawal, U.; Bheemisetty, N.; Akku, R.; Sánchez-Velazco, D.; Waleed, M.S. Bowel ischemia in COVID-19: A systematic review. Int. J. Clin. Pract. 2021, 75, e14930. [Google Scholar] [CrossRef]
- Omar, S.F.; Habib, R.M.; Motawea, A.M. Radiological findings of COVID-19-related thromboembolic complications. Egypt. J. Radiol. Nucl. Med. 2021, 52, 99. [Google Scholar] [CrossRef]
- Olson, M.C.; Lubner, M.G.; Menias, C.O.; Mellnick, V.M.; Gettle, L.M.; Kim, D.H.; Pickhardt, P.J. RadioGraphics Update: Venous Thrombosis and Hypercoagulability in the Abdomen and Pelvis—Findings in COVID-19. Radiographics 2020, 40, E24–E28. [Google Scholar] [CrossRef]
- Abdelmohsen, M.A.; Alkandari, B.M.; Abdel Razek, A.A.K.; Tobar, A.M.; Gupta, V.K.; Elsebaie, N. Abdominal Computed Tomography Angiography and Venography in Evaluation of Hemorrhagic and Thrombotic lesions in Hospitalized COVID-19 patients. Clin. Imaging 2021, 79, 12–19. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Straus, S.E. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Zhao, Y.; Teh, J.J.; Kung, V.; Mallappa, S. Bowel ischaemia in COVID-19 infection: A scoping review protocol. BMJ Open 2022, 12, e060566. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Microsoft Excel Spreadsheet Software|Microsoft 365. Available online: https://www.microsoft.com/en-gb/microsoft-365/excel (accessed on 20 December 2023).
- Abeysekera, K.W.; Karteszi, H.; Clark, A.; Gordon, F.H. Spontaneous portomesenteric thrombosis in a non-cirrhotic patient with SARS-CoV-2 infection. BMJ Case Rep. 2020, 13, e238906. [Google Scholar] [CrossRef]
- Ahmed, A.O.E.; Mohamed, S.F.; Saleh, A.O.; Al-Shokri, S.D.; Ahmed, K.; Mohamed, M.F.H. Acute abdomen -like-presentation associated with SARS-CoV-2 infection. IDCases 2020, 21, e00895. [Google Scholar] [CrossRef]
- Alali, A.A.; Baqais, M.O.; Albishi, F.M.; Alkhamis, A.I.; Alshehri, Y.A.; Amri, K.F.; Al-Hawaj, F. Superior Mesenteric Artery Thrombosis Following Severe COVID-19 Pneumonia. Cureus 2021, 13, e19954. [Google Scholar] [CrossRef]
- Alemán, W.; Cevallos, L.C. Subacute mesenteric venous thrombosis secondary to COVID-19: A late thrombotic complication in a nonsevere patient. Radiol. Case Rep. 2021, 16, 899–902. [Google Scholar] [CrossRef]
- Amaravathi, U.; Balamurugan, N.; Muthu Pillai, V.; Ayyan, S.M. Superior Mesenteric Arterial and Venous Thrombosis in COVID-19. J. Emerg. Med. 2021, 60, e103–e107. [Google Scholar] [CrossRef]
- Aryal, S.; Bhattarai, V.; Sharma, S. SARS-CoV-2-related superior mesenteric artery thrombosis resulting in pneumatosis intestinalis complicated by pneumatosis portalis in a young male: A case report. Ann. Med. Surg. 2023, 85, 198–202. [Google Scholar] [CrossRef]
- Azouz, E.; Yang, S.; Monnier-Cholley, L.; Arrivé, L. Systemic arterial thrombosis and acute mesenteric ischemia in a patient with COVID-19. Intensive Care Med. 2020, 46, 1464–1465. [Google Scholar] [CrossRef]
- Bannazadeh, M.; Tassiopoulos, A.; Koullias, G. Acute superior mesenteric artery thrombosis seven days after discharge for novel coronavirus pneumonia. J. Vasc. Surg. Cases Innov. Tech. 2021, 7, 586–588. [Google Scholar] [CrossRef]
- Beccara, L.A.; Pacioni, C.; Ponton, S.; Francavilla, S.; Cuzzoli, A. Arterial Mesenteric Thrombosis as a Complication of SARS-CoV-2 Infection. Eur. J. Case Rep. Intern. Med. 2020, 7, 001690. [Google Scholar] [CrossRef]
- Calcagno, E.; Sogunro, O.; Nepal, P.; Assaker, R.; Sapire, J. COVID-19 induced mesenteric venous infarction. Radiol. Case Rep. 2021, 16, 1999–2002. [Google Scholar] [CrossRef]
- Cheung, S.; Quiwa, J.C.; Pillai, A.; Onwu, C.; Tharayil, Z.J.; Gupta, R. Superior Mesenteric Artery Thrombosis and Acute Intestinal Ischemia as a Consequence of COVID-19 Infection. Am. J. Case Rep. 2020, 21, e925753. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Nogueira, L.; Marques, S.; Torres, L.; Silva, A.F. An Improbable Thromboembolic Manifestation of COVID-19: A Case Report. Cureus 2022, 14, e23013. [Google Scholar] [CrossRef] [PubMed]
- de Barry, O.; Mekki, A.; Diffre, C.; Seror, M.; El Hajjam, M.; Carlier, R.-Y. Arterial and venous abdominal thrombosis in a 79-year-old woman with COVID-19 pneumonia. Radiol. Case Rep. 2020, 15, 1054–1057. [Google Scholar] [CrossRef]
- Dinoto, E.; Ferlito, F.; La Marca, M.A.; Mirabella, D.; Bajardi, G.; Pecoraro, F. Staged acute mesenteric and peripheral ischemia treatment in COVID-19 patient: Case report. Int. J. Surg. Case Rep. 2021, 84, 106105. [Google Scholar] [CrossRef]
- Fan, B.E.; Chang, C.C.R.; Teo, C.H.Y.; Yap, E.S. COVID-19 Coagulopathy with Superior Mesenteric Vein Thrombosis Complicated by an Ischaemic Bowel. Hamostaseologie 2020, 40, 592–593. [Google Scholar] [CrossRef] [PubMed]
- Carmo Filho, A.; Cunha, B.d.S. Inferior mesenteric vein thrombosis and COVID-19. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200412. [Google Scholar] [CrossRef] [PubMed]
- Fransvea, P.; Costa, G.; Pepe, G.; La Greca, A.; Magalini, S.; Puccioni, C.; D'Agostino, L.; Altieri, G.; Borello, A.; Cozza, V.; et al. Acute intestinal ischemia in patients with COVID-19: Single-centre experience and literature review. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1414–1429. [Google Scholar]
- Goodfellow, M.; Courtney, M.; Upadhyay, Y.; Marsh, R.; Mahawar, K. Mesenteric Venous Thrombosis Due to Coronavirus in a Post Roux-en-Y Gastric Bypass Patient: A Case Report. Obes. Surg. 2021, 31, 2308–2310. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Sharma, O.; Srikanth, K.; Mishra, R.; Tandon, A.; Rajput, D. Review of Mesenteric Ischemia in COVID-19 Patients. Indian. J. Surg. 2023, 85, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Del Hoyo, J.; López-Muñoz, P.; Fernández-de la Varga, M.; Garrido-Marín, A.; Valero-Pérez, E.; Prieto, M.; Aguilera, V. Hepatobiliary and Pancreatic: A fatal case of extensive splanchnic vein thrombosis in a patient with COVID-19. J. Gastroenterol. Hepatol. 2020, 35, 1853. [Google Scholar] [CrossRef] [PubMed]
- Hussein, M.H.; Alabdaljabar, M.S.; Alfagyh, N.; Badran, M.; Alamiri, K. Splanchnic venous thrombosis in a nephrotic patient following COVID-19 infection: A case report. BMC Nephrol. 2021, 22, 420. [Google Scholar] [CrossRef]
- Ignat, M.; Philouze, G.; Aussenac-Belle, L.; Faucher, V.; Collange, O.; Mutter, D.; Pessaux, P. Small bowel ischemia and SARS-CoV-2 infection: An underdiagnosed distinct clinical entity. Surgery 2020, 168, 14–16. [Google Scholar] [CrossRef]
- Jeilani, M.; Hill, R.; Riad, M.; Abdulaal, Y. Superior mesenteric vein and portal vein thrombosis in a patient with COVID-19: A rare case. BMJ Case Rep. 2021, 14, e244049. [Google Scholar] [CrossRef] [PubMed]
- Karna, S.T.; Panda, R.; Maurya, A.P.; Kumari, S. Superior Mesenteric Artery Thrombosis in COVID-19 Pneumonia: An Underestimated Diagnosis-First Case Report in Asia. Indian. J. Surg. 2020, 82, 1235–1237. [Google Scholar] [CrossRef] [PubMed]
- Krothapalli, N.; Jacob, J. A Rare Case of Acute Mesenteric Ischemia in the Setting of COVID-19 Infection. Cureus 2021, 13, e14174. [Google Scholar] [CrossRef] [PubMed]
- Lari, E.; Lari, A.; AlQinai, S.; Abdulrasoul, M.; AlSafran, S.; Ameer, A.; Al-Sabah, S. Severe ischemic complications in COVID-19—A case series. Int. J. Surg. Case Rep. 2020, 75, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Al Mahruqi, G.; Stephen, E.; Abdelhedy, I.; Al Wahaibi, K. Our early experience with mesenteric ischemia in COVID-19 positive patients. Ann. Vasc. Surg. 2021, 73, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.M.; Rakheja, D.; Gopal, P. SARS-CoV-2-related Hypercoagulable State Leading to Ischemic Enteritis Secondary to Superior Mesenteric Artery Thrombosis. Clin. Gastroenterol. Hepatol. 2021, 19, e111. [Google Scholar] [CrossRef] [PubMed]
- Nada, A.; Shabana, A.; Elsaadany, A.; Abdelrahman, A.; Gaballah, A.H. Superior mesenteric artery thrombosis and small bowel necrosis: An uncommon thromboembolic manifestation in COVID-19 pneumonia. Radiol. Case Rep. 2022, 17, 821–824. [Google Scholar] [CrossRef] [PubMed]
- Nasseh, S.; Trabelsi, M.M.; Oueslati, A.; Haloui, N.; Jerraya, H.; Nouira, R. COVID-19 and gastrointestinal symptoms: A case report of a Mesenteric Large vessel obstruction. Clin. Case Rep. 2021, 9, e04235. [Google Scholar] [CrossRef]
- Norsa, L.; Valle, C.; Morotti, D.; Bonaffini, P.A.; Indriolo, A.; Sonzogni, A. Intestinal ischemia in the COVID-19 era. Dig. Liver Dis. 2020, 52, 1090–1091. [Google Scholar] [CrossRef]
- Osilli, D.; Pavlovica, J.; Mane, R.; Ibrahim, M.; Bouhelal, A.; Jacob, S. Case reports: Mild COVID-19 infection and acute arterial thrombosis. J. Surg. Case Rep. 2020, 2020, rjaa343. [Google Scholar] [CrossRef]
- Pang, J.H.Q.; Tang, J.H.; Eugene-Fan, B.; Lee, C.L.; Low, J.K. A Peculiar Case of Small Bowel Stricture in a Coronavirus Disease 2019 Patient with Congenital Adhesion Band and Superior Mesenteric Vein Thrombosis. Ann. Vasc. Surg. 2021, 70, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Posada-Arango, A.M.; García-Madrigal, J.; Echeverri-Isaza, S.; Alberto-Castrillón, G.; Martínez, D.; Gómez, A.C.; Pinto, J.A.; Pinillos, L. Thrombosis in abdominal vessels associated with COVID-19 Infection: A report of three cases. Radiol. Case Rep. 2021, 16, 3044–3050. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Nakamura, R.M.; Gonzalez-Calatayud, M.; Martinez Martinez, A.R. Acute mesenteric thrombosis in two patients with COVID-Two cases report and literature review. Int. J. Surg. Case Rep. 2020, 76, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, M.; Nishiwada, S.; Terai, T.; Kuge, H.; Koyama, F.; Nakagawa, K.; Nagai, M.; Sho, M. Acute superior mesenteric artery occlusion associated with COVID-19 pneumonia: A case report. Surg. Case Rep. 2022, 8, 6. [Google Scholar] [CrossRef] [PubMed]
- Ucpinar, B.A.; Sahin, C. Superior Mesenteric Artery Thrombosis in a Patient with COVID-19: A Unique Presentation. J. Coll. Physicians Surg. Pak. 2020, 30, 112–114. [Google Scholar] [PubMed]
- Vidali, S.; Morosetti, D.; Granai, A.V.; Legramante, J.M.; Buonomo, O.C.; Argirò, R. Splenoportal-mesenteric axis thrombosis and splenic artery occlusion as initial presentations of COVID-19 disease. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1680–1683. [Google Scholar] [PubMed]
- Vulliamy, P.; Jacob, S.; Davenport, R.A. Acute aorto-iliac and mesenteric arterial thromboses as presenting features of COVID-19. Br. J. Haematol. 2020, 189, 1053–1054. [Google Scholar] [CrossRef]
- Zeng, W.; Qi, K.; Ye, M.; Zheng, L.; Liu, X.; Hu, S.; Zhang, W.; Tang, W.; Xu, J.; Yu, D.; et al. Gastrointestinal symptoms are associated with severity of coronavirus disease 2019: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2022, 34, 168. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C.; et al. Clinical Characteristics of COVID-19 Patients with Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. Am. J. Gastroenterol. 2020, 115, 766–773. [Google Scholar] [CrossRef]
- Cooney, J.; Appiahene, P.; Findlay, R.; Al-Hillawi, L.; Rafique, K.; Laband, W.; Shandro, B.; Poullis, A. COVID-19 infection causing residual gastrointestinal symptoms—A single UK centre case series. Clin. Med. 2022, 22, 181–183. [Google Scholar] [CrossRef]
- Hayashi, Y.; Wagatsuma, K.; Nojima, M.; Yamakawa, T.; Ichimiya, T.; Yokoyama, Y.; Nakase, H. The characteristics of gastrointestinal symptoms in patients with severe COVID-19: A systematic review and meta-analysis. J. Gastroenterol. 2021, 56, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Acosta, S. Mesenteric ischemia. Curr. Opin. Crit. Care 2015, 21, 171–178. [Google Scholar] [CrossRef]
- Clair, D.G.; Beach, J.M. Mesenteric Ischemia. N. Engl. J. Med. 2016, 374, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Liu, X.; Shou, C.; Yang, W.; Yu, J. Advances in the diagnosis of non-occlusive mesenteric ischemia and challenges in intra-abdominal sepsis patients: A narrative review. PeerJ 2023, 11, e15307. [Google Scholar] [CrossRef]
- Fuglseth, H.; Søreide, K.; Vetrhus, M. Acute mesenteric ischaemia. Br. J. Surg. 2023, 110, 1030–1034. [Google Scholar] [CrossRef] [PubMed]
- Moiz, B.; Muslim, Z.; Siddiqui, Z.F.; Zafar, H. Acute Mesenteric Thrombosis: A Hematologist Perspective. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620932999. [Google Scholar] [CrossRef] [PubMed]
- Ryer, E.J.; Kalra, M.; Oderich, G.S.; Duncan, A.A.; Gloviczki, P.; Cha, S.; Bower, T.C. Revascularization for acute mesenteric ischemia. J. Vasc. Surg. 2012, 55, 1682–1689. [Google Scholar] [CrossRef] [PubMed]
- Oldenburg, W.A.; Lau, L.L.; Rodenberg, T.J.; Edmonds, H.J.; Burger, C.D. Acute Mesenteric Ischemia: A Clinical Review. Arch. Intern. Med. 2004, 164, 1054–1062. [Google Scholar] [CrossRef]
- Tamme, K.; Blaser, A.R.; Laisaar, K.-T.; Mändul, M.; Kals, J.; Forbes, A.; Kiss, O.; Acosta, S.; Bjørck, M.; Starkopf, J. Incidence and outcomes of acute mesenteric ischaemia: A systematic review and meta-analysis. BMJ Open 2022, 12, e062846. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).