
Risk of Cardiovascular Events in People with HIV (PWH) Treated with Integrase Strand-Transfer Inhibitors: The Debate Is Not Over; Results of the SCOLTA Study
 , , ,
, , ,  , ,
, ,  ,
,  ,
,  , ,
, ,  , , ,
, , ,  , , add
Show full author list
, , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joint United Nations Programme on HIV/AIDS (UNAIDS) 2022. In Danger: UNAIDS Global AIDS Update 2022; 2022, 2022, 1–22. Available online: https://www.unaids.org/en/resources/documents/2022/in-danger-global-aids-update (accessed on 11 April 2024).
- World Health Organization. Global Health Sector Strategies on, Respectively, HIV, Viral Hepatitis and Sexually Transmitted in-Fections for the Period 2022–2030; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Ntsekhe, M.; Baker, J.V. Cardiovascular Disease Among Persons Living with HIV: New Insights into Pathogenesis and Clinical Manifestations in a Global Context. Circulation 2023, 147, 83–100. [Google Scholar] [CrossRef] [PubMed]
- Freiberg, M.S.; Chang, C.C.H.; Kuller, L.H.; Skanderson, M.; Lowy, E.; Kraemer, K.L.; Butt, A.A.; Goetz, M.B.; Leaf, D.; Oursler, K.A.; et al. HIV infection and the risk of acute myocardial infarction. JAMA Intern. Med. 2013, 173, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Chow, F.C.; Regan, S.; Feske, S.; Meigs, J.B.; Grinspoon, S.K.; Triant, V.A. Comparison of ischemic stroke incidence in HIV-infected and non–HIV-infected patients in a US health care system. J. Acquir. Immune Defic. Syndr. 2012, 60, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Triant, V.A.; Lee, H.; Hadigan, C.; Grinspoon, S.K. Increased acute myocardial infarction rates and cardiovascular risk factors among patients with human immunodeficiency virus disease. J. Clin. Endocrinol. Metab. 2007, 92, 2506–2512. [Google Scholar] [CrossRef] [PubMed]
- Hsue, P.Y.; Waters, D.D. HIV infection and coronary heart disease: Mechanisms and management. Nat. Rev. Cardiol. 2019, 16, 745–759. [Google Scholar] [CrossRef]
- Society EAC. European AIDS Clinical Society—Version 12.0, October 2023. Available online: https://www.eacsociety.org/media/guidelines-12.0.pdf (accessed on 11 April 2024).
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Department of Health and Human Services. Available online: https://clinicalinfo.hiv.gov/ (accessed on 11 April 2024).
- Deeks, S.G.; Lewin, S.R.; Havlir, D.V. The end of AIDS: HIV infection as a chronic disease. Lancet 2013, 382, 1525–1533. [Google Scholar] [CrossRef] [PubMed]
- Marcus, J.L.; Chao, C.R.; Leyden, W.A.; Xu, L.; Quesenberry, C.P.; Klein, D.B.; Towner, W.J.; Horberg, M.A.; Silverberg, M.J. Narrowing the gapo in life expectancy between HIV-infected and HIV-uninfected individuals with access to care. J. Acquir. Immune Defic. Syndr. 2017, 73, 39–46. [Google Scholar] [CrossRef] [PubMed]
- El-Sadr, W.M.; The Strategies for Management of Antiretroviral Therapy (SMART) Study Group. CD4+ Count–Guided Interruption of Antiretroviral Treatment. N. Engl. J. Med. 2006, 365, 687–696. [Google Scholar] [CrossRef]
- Hsue, P.Y.; Squires, K.; Bolger, A.F.; Capili, B.; Mensah, G.A.; Temesgen, Z.; Wanke, C.A.; Wohl, D.A. Screening and assessment of coronary heart disease in HIV-infected patients. Circulation 2008, 118, e41–e47. [Google Scholar] [CrossRef]
- Grinspoon, S.K.; Fitch, K.V.; Zanni, M.V.; Fichtenbaum, C.J.; Umbleja, T.; Aberg, J.A.; Overton, E.T.; Malvestutto, C.D.; Bloomfield, G.S.; Currier, J.S.; et al. Pitavastatin to Prevent Cardiovascular Disease in HIV Infection. N. Engl. J. Med. 2023, 389, 687–699. [Google Scholar] [CrossRef] [PubMed]
- Friismoller, N.; Sabin, C.A.; Weber, R.S.; Monforte, A.D.; Elsadr, W.; Reiss, P.; Thiebaut, R.; Morfeldt, L.; De Wit, S.; Pradier, C.; et al. Combination Antiretroviral Therapy and the Risk of Myocardial Infarction. N. Engl. J. Med. 2003, 349, 1993–2003. [Google Scholar] [CrossRef]
- Bozzette, S.A.; Ake, C.F.; Tam, H.K.; Chang, S.W.; Louis, T.A. Cardiovascular and Cerebrovascular Events in Patients Treated for Human Immunodeficiency Virus Infection. N. Engl. J. Med. 2003, 348, 702–710. [Google Scholar] [CrossRef]
- Holmes, C.B.; Rabkin, M.; Ford, N.; Preko, P.; Rosen, S.; Ellman, T.; Ehrenkranz, P. Tailored HIV programmes and universal health coverage. Bull. World Health Organ. 2020, 98, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Burgos, J.; Ribera, E.; Falcó, V. Antiretroviral Therapy in Advanced HIV Disease: Which is the Best Regimen? AIDS Rev. 2018, 20, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Group, D.A.D.S.; Sabin, C.A.; Worm, S.W.; Weber, R.; Reiss, P.; El-Sadr, W.; Dabis, F.; De Wit, S.; Law, M.; D’Arminio Monforte, A.; et al. Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the D:A:D study: A multi-cohort collaboration. Lancet 2008, 371, 1417–1426. [Google Scholar] [CrossRef]
- Tanuma, J.; Ishizaki, A.; Gatanaga, H.; Kikuchi, Y.; Kimura, S.; Hiroe, M.; Oka, S. Dilated cardiomyopathy in an adult human immunodeficiency virus type 1-positive patient treated with a zidovudine-containing antiretroviral regime. Clin. Infect. Dis. 2003, 37, e109–e111. [Google Scholar] [CrossRef]
- Ryom, L.; Lungdren, J.D.; El-Sadr, W.; Reiss, P.; Kirk, O.; Law, M.; Phillips, A.; Weber, R.; Fontas, E.; d’Arminio Monforte, A.; et al. Cardiovascular Disease and Use of Contemporary Protease Inhibitors: The D:A:D international prospective cohort Study. Lancet HIV 2018, 5, e291–e300. [Google Scholar] [CrossRef]
- Milic, J.; Renzetti, S.; Ferrari, D.; Barbieri, S.; Menozzi, M.; Carli, F.; Dolci, G.; Ciusa, G.; Mussini, C.; Calza, S.; et al. Relationship between weight gain and insulin resistance in people living with HIV switching to integrase strand transfer inhibitors-based regimens. AIDS 2022, 36, 1643–1653. [Google Scholar] [CrossRef] [PubMed]
- McCann, K.; Shah, S.; Hindley, L.; Hill, A.; Qavi, A.; Simmons, B.; Serenata, C.; Sokhela, S.; Venter, W.F. Implications of weight gain with newer anti-retrovirals: 10-year predictions of cardiovascular disease and diabetes. AIDS 2021, 35, 1657–1665. [Google Scholar] [CrossRef]
- Venter, W.D.F.; Sokhela, S.; Simmons, B.; Moorhouse, M.; Fairlie, L.; Mashabane, N.; Serenata, C.; Akpomiemie, G.; Masenya, M.; Qavi, A.; et al. Dolutegravir with emtricitabine and tenofovir alafenamide or tenofovir disoproxil fumarate versus efavirenz, emtricitabine, and tenofovir disoproxil fumarate for initial treatment of HIV-1 infection (ADVANCE): Week 96 results from a randomised, phase 3, non-inferiority trial. Lancet HIV 2020, 7, e666–e676. [Google Scholar] [CrossRef] [PubMed]
- Neesgaard, B.; Greenberg, L.; Miró, J.M.; Grabmeier-Pfistershammer, K.; Wandeler, G.; Smith, C.; De Wit, S.; Wit, F.; Pelchen-Matthews, A.; Mussini, C.; et al. Association between Integrase Strand Transfer Inhibitors and Cardiovascular Disease in People Living with HIV: A multicentered Prospective Study from the RESPOND Cohort Consortium. Lancet HIV 2022, 9, e474–e485. [Google Scholar] [CrossRef]
- Eckard, A.R.; McComsey, G.A. Weight gain and integrase inhibitors. Curr. Opin. Infect. Dis. 2020, 33, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Rein, S.M.; Lodi, S.; Logan, R.W.; Touloumi, G.; Antoniadou, A.; Wittkop, L.; Bonnet, F.; van Sighem, A.; van der Valk, M.; Reiss, P.; et al. Integrase strand-transfer inhibitor use and cardiovascular events in adults with HIV: An emulation of target trials in the HIV-CAUSAL Collaboration and the Antiretroviral Therapy Cohort Collaboration. Lancet HIV 2023, 10, e723–e732. [Google Scholar] [CrossRef]
- Byonanebye, D.M.; Polizzotto, M.N.; Neesgaard, B.; Sarcletti, M.; Matulionyte, R.; Braun, D.L.; Castagna, A.; de Wit, S.; Wit, F.; Fontas, E.; et al. Incidence of hypertension in people with HIV who are treated with integrase inhibitors versus other antiretroviral regimens in the RESPOND cohort consortium. HIV Med. 2022, 23, 895–910. [Google Scholar] [CrossRef]
- Guaraldi, G.; Milic, J. Comparing implications of cardiovascular risk of abacavir and integrase inhibitors: Why scientific community is confused and timid? AIDS 2023, 37, 1005–1008. [Google Scholar] [CrossRef]
- Bonfanti, P.; Martinelli, C.; Ricci, E.; Carradori, S.; Parruti, G.; Armignacco, O.; Magnani, C.; Quirino, T. An Italian approach to postmarketing monitoring: Preliminary results from the SCOLTA (Surveillance Cohort Long-Term Toxicity Antiretrovirals) project on the safety of lopinavir/ritonavir. J. Acquir. Immune Defic. Syndr. 2005, 39, 317–320. [Google Scholar] [CrossRef]
- American Diabetes Association. Classification and diagnosis of diabetes. Diabetes Care 2016, 39 (Suppl. S1), S13–S22. [Google Scholar] [CrossRef]
- U.S. Department of Health; Human Services. Common Terminology Criteria for Adverse Events (CTCAE). Version 5. 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 9 April 2024).
- Surial, B.; Chammartin, F.; Damas, J.; Calmy, A.; Haerry, D.; Stöckle, M.; Schmid, P.; Bernasconi, E.; Fux, C.A.; Tarr, P.E.; et al. Impact of Integrase Inhibitors on Cardiovascular Disease Events in People with Human Immunodeficiency Virus Starting Antiretroviral Therapy. Clin. Infect. Dis. 2023, 77, 729–737. [Google Scholar] [CrossRef]
- Visseren, F.L.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Rev. Esp. Cardiol. 2022, 75, 429. [Google Scholar] [CrossRef]
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef] [PubMed]
- Bansilal, S.; Castellano, J.M.; Fuster, V. Global burden of CVD: Focus on secondary prevention of cardiovascular disease. Int. J. Cardiol. 2015, 201, S1–S7. [Google Scholar] [CrossRef]
- La Vecchia, C.; Chatenoud, L.; Altieri, A.; Tavani, A. Nutrition and health: Epidemiology of diet, cancer and cardiovascular disease in Italy. Nutr. Metab. Cardiovasc. Dis. 2001, 11 (Suppl. S4), 10–15. [Google Scholar] [PubMed]
- Volpe, M.; the Writing Committee; Battistoni, A.; Gallo, G.; Rubattu, S.; Tocci, G.; Societies, O.B.O.T.S. Executive Summary of the 2018 Joint Consensus Document on Cardiovascular Disease Prevention in Italy. High Blood Press. Cardiovasc. Prev. 2018, 25, 327–341. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef] [PubMed]
- Goldsborough, E.; Osuji, N.; Blaha, M.J. Assessment of Cardiovascular Disease Risk. Endocrinol. Metab. Clin. N. Am. 2022, 51, 483–509. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, S.S.; Levy, D.; Vasan, R.S.; Wang, T.J. The Framingham Heart Study and the epidemiology of cardiovascular disease: A historical perspective. Lancet 2014, 383, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Townsend, N.; Kazakiewicz, D.; Wright, F.L.; Timmis, A.; Huculeci, R.; Torbica, A.; Gale, C.P.; Achenbach, S.; Weidinger, F.; Vardas, P. Epidemiology of cardiovascular disease in Europe. Nat. Rev. Cardiol. 2021, 19, 133–143. [Google Scholar] [CrossRef]
- Stockdale, A.J.; Khoo, S. Doravirine: Its role in HIV treatment. Curr. Opin. HIV AIDS 2022, 17, 4–14. [Google Scholar] [CrossRef]



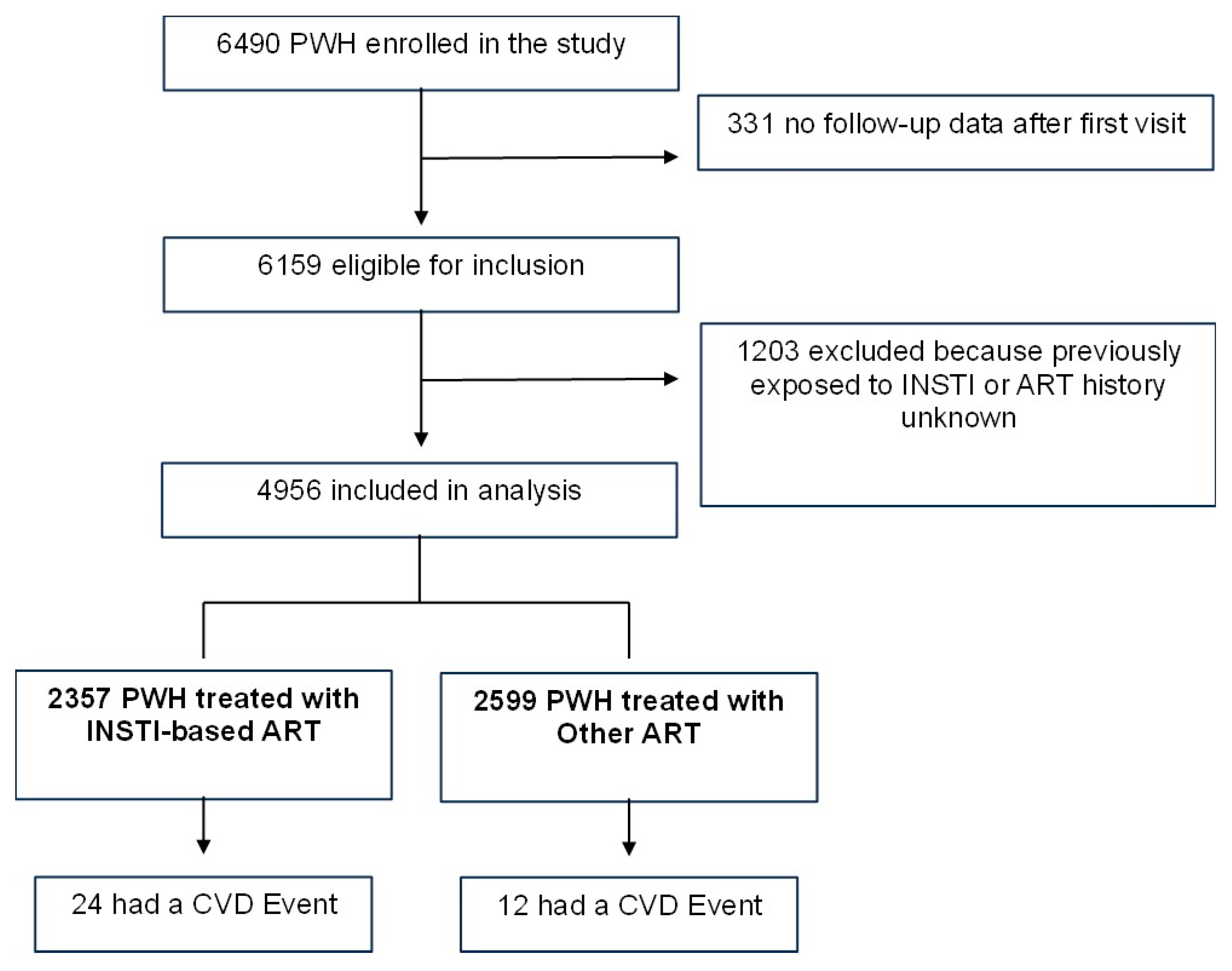{kind=link}
{kind=link}
| Characteristics | INSTI N = 2357 (47.6%) | Non INSTI N = 2599 (52.4%) | Total N = 4956 | p-Value * |
|---|---|---|---|---|
| Male sex, n (%) | 1750 (74.2) | 1862 (71.6) | 3612 (72.9) | 0.04 |
| Age, years (median, IQR) | 47.0 (40.0–54.0) | 42.0 (37.0–48.0) | 44.0 (38.0–51.0) | <0.0001 |
| Caucasian ethnicity, n (%) | 2140 (90.8) | 2405 (92.5) | 4545 (91.7) | 0.03 |
| BMI > 30.0 kg/m2, n (%) | 161 (6.8) | 62 (2.4) | 223 (4.5) | 0.49 |
| missing | 301 (12.8) | 1725 (66.4) | 2026 (40.9) | |
| Intravenous drug use, n (%) | 501 (21.3) | 879 (33.8) | 1380 (27.8) | <0.0001 |
| CDC stage C, n (%) | 624 (26.5) | 812 (31.2) | 1436 (29.0) | 0.0003 |
| CD4 cells/mm3 < 200, n (%) | 507 (21.5) | 704 (27.1) | 1211 (24.4) | <0.0001 |
| Naïve, n (%) | 636 (27.0) | 384 (14.8) | 1020 (20.6) | <0.0001 |
| Hypertension, n (%) | 379 (16.1) | 211 (8.1) | 590 (11.9) | <0.0001 |
| Diabetes, n (%) | 106 (4.5) | 67 (2.6) | 173 (3.5) | 0.0002 |
| Dyslipidaemia, n (%) | 326 (13.8) | 170 (6.5) | 496 (10.0) | <0.0001 |
| Chronic kidney disease, n (%) | 32 (1.4) | 15 (0.6) | 47 (0.9) | 0.005 |
| Previous cardiovascular event, n (%) | 54 (2.3) | 24 (0.9) | 78 (1.6) | 0.0001 |
| Ever smoker, n (%) | 1147 (48.7) | 943 (36.3) | 2090 (42.2) | <0.0001 |
| Never smoker, n (%) | 740 (31.4) | 415 (16.0) | 1155 (23.3) | |
| ND, n (%) | 470 (19.9) | 1241 (47.7) | 1711 (34.5) |
| N | Events | PYFU | Crude IR/1000 PYFU (95% CI) | Crude RR (95% CI) | Adjusted * IR/1000 PYFU (95% CI) | Adjusted * RR (95% CI) | |
|---|---|---|---|---|---|---|---|
| 2-year follow-up | |||||||
| Total | 4984 | 28 | 7321.37 | 3.8 (2.6–5.5) | 6.7 (3.6–12.2) | ||
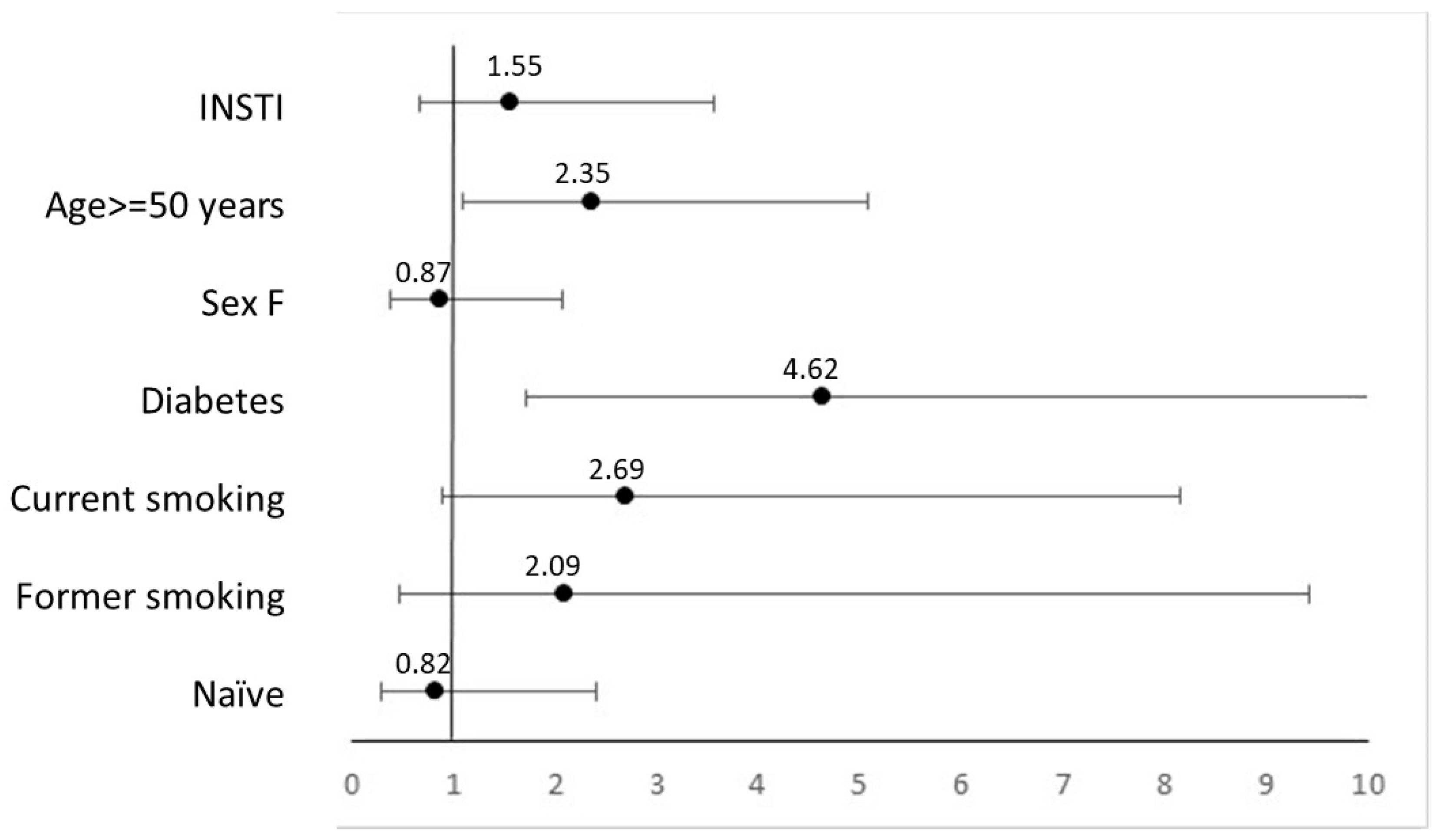
| INSTI | 2192 | 19 | 3736.59 | 5.1 (3.2–8.0) | 2.02 (0.91–4.46) | 8.7 (4.5–16.7) | 1.55 (0.67–3.56) |
| Non INSTI | 2792 | 9 | 3574.54 | 2.5 (1.3–4.8) | 5.6 (2.4–12.8) | ||
| Naïve | 1020 | 4 | 1459.94 | 2.7 (1.0–7.3) | 0.67 (0.23–1.93) | 6.2 (2.0–19.0) | 0.82 (0.28–2.39) |
| Experienced | 3964 | 24 | 5851.18 | 4.1 (2.7–6.1) | 7.6 (4.1–14.0) | ||
| Complete follow-up | |||||||
| Total | 4984 | 36 | 11,688.51 | 3.1 (2.2–4.3) | 7.4 (4.1–14.5) | ||
| INSTI | 2356 | 24 | 6770.75 | 3.5 (2.4–5.3) | 1.45 (0.72–2.90) | 5.4 (2.9–10.0) | 1.10 (0.53–2.29) |
| Non INSTI | 2598 | 12 | 4907.51 | 2.4 (1.4–4.3) | 4.9 (2.3–10.5) | ||
| Naïve | 1020 | 5 | 2149.58 | 2.3 (1.0–5.6) | 0.72 (0.28–1.84) | 4.8 (1.7–13.3) | 0.91 (0.35–2.36) |
| Experienced | 3934 | 31 | 9528.67 | 3.2 (2.3–4.6) | 5.3 (3.0–9.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corti, N.; Menzaghi, B.; Orofino, G.; Guastavigna, M.; Lagi, F.; Di Biagio, A.; Taramasso, L.; De Socio, G.V.; Molteni, C.; Madeddu, G.; et al. Risk of Cardiovascular Events in People with HIV (PWH) Treated with Integrase Strand-Transfer Inhibitors: The Debate Is Not Over; Results of the SCOLTA Study. Viruses 2024, 16, 613. https://doi.org/10.3390/v16040613
Corti N, Menzaghi B, Orofino G, Guastavigna M, Lagi F, Di Biagio A, Taramasso L, De Socio GV, Molteni C, Madeddu G, et al. Risk of Cardiovascular Events in People with HIV (PWH) Treated with Integrase Strand-Transfer Inhibitors: The Debate Is Not Over; Results of the SCOLTA Study. Viruses. 2024; 16(4):613. https://doi.org/10.3390/v16040613
Chicago/Turabian StyleCorti, Nicolò, Barbara Menzaghi, Giancarlo Orofino, Marta Guastavigna, Filippo Lagi, Antonio Di Biagio, Lucia Taramasso, Giuseppe Vittorio De Socio, Chiara Molteni, Giordano Madeddu, and et al. 2024. "Risk of Cardiovascular Events in People with HIV (PWH) Treated with Integrase Strand-Transfer Inhibitors: The Debate Is Not Over; Results of the SCOLTA Study" Viruses 16, no. 4: 613. https://doi.org/10.3390/v16040613
APA StyleCorti, N., Menzaghi, B., Orofino, G., Guastavigna, M., Lagi, F., Di Biagio, A., Taramasso, L., De Socio, G. V., Molteni, C., Madeddu, G., Salomoni, E., Pellicanò, G. F., Pontali, E., Bellagamba, R., Celesia, B. M., Cascio, A., Sarchi, E., Gulminetti, R., Calza, L., ... Bonfanti, P. (2024). Risk of Cardiovascular Events in People with HIV (PWH) Treated with Integrase Strand-Transfer Inhibitors: The Debate Is Not Over; Results of the SCOLTA Study. Viruses, 16(4), 613. https://doi.org/10.3390/v16040613