
Sex Modifies the Effect of COVID-19 on Arterial Elasticity

 ,
,
Abstract
1. Introduction
2. Materials and Methods
Statistical Methods
3. Results
3.1. Characteristics
3.1.1. Associations with Female Sex
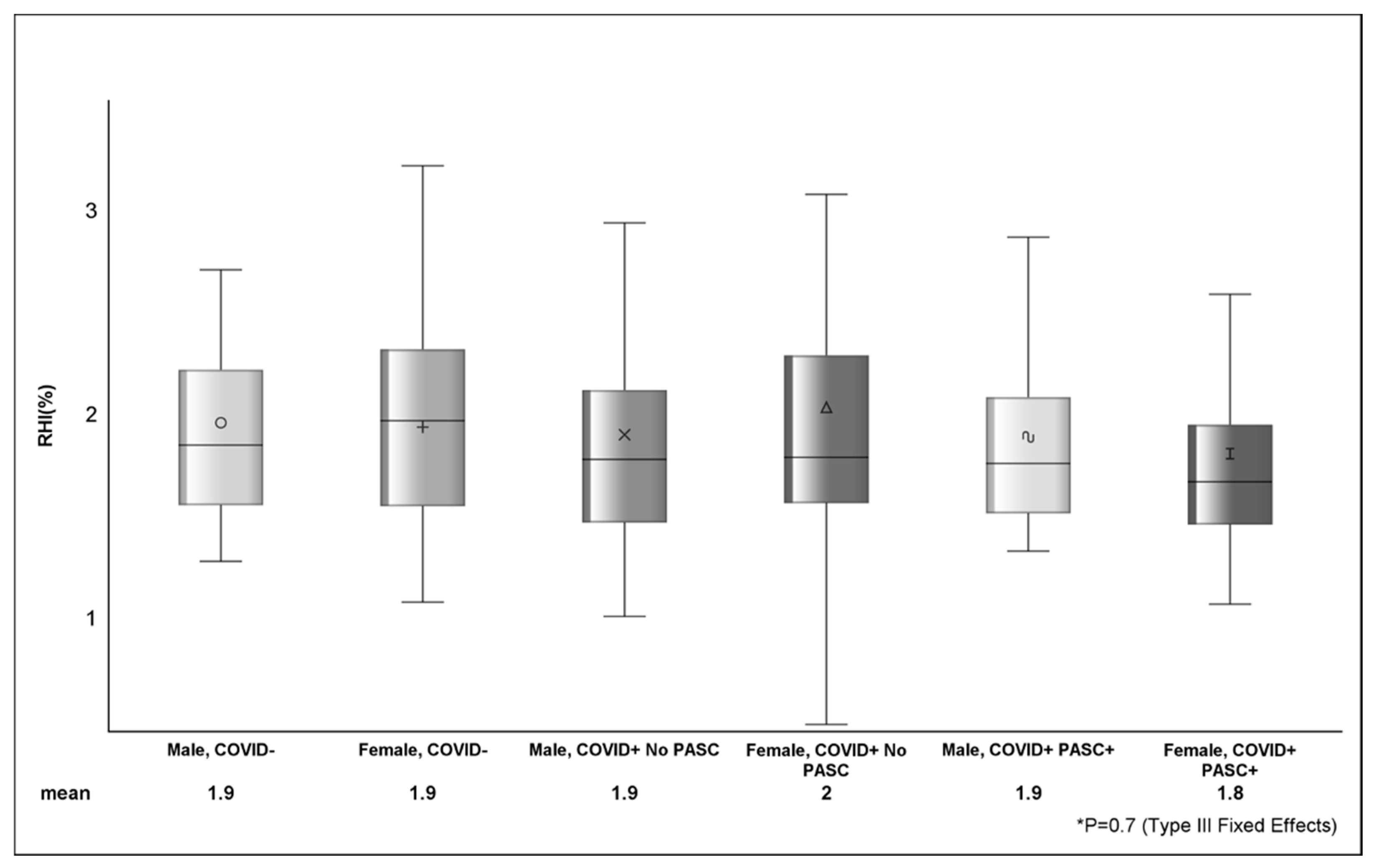
3.1.2. Endothelial Assessment by COVID-19 Status and Sex
3.1.3. Associations with Arterial Elasticity as Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- World Health Organization. R and D Blueprint and COVID-19. Available online: https://www.who.int/teams/blueprint/covid-19 (accessed on 2 March 2024).
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Cao, P.; Chong, M.K.; Gao, D.; Lou, Y.; Ran, J.; Wang, K.; Wang, W.; Yang, L.; He, D.; et al. COVID-19 and gender-specific difference: Analysis of public surveillance data in Hong Kong and Shenzhen, China, from January 10 to February 15, 2020. Infect. Control Hosp. Epidemiol. 2020, 41, 750–751. [Google Scholar] [CrossRef] [PubMed]
- Scully, E.P.; Haverfield, J.; Ursin, R.L.; Tannenbaum, C.; Klein, S.L. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat. Rev. Immunol. 2020, 20, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female gender is associated with long COVID syndrome: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, e9–e611. [Google Scholar] [CrossRef] [PubMed]
- Saeed, S.; Tadic, M.; Larsen, T.H.; Grassi, G.; Mancia, G. Coronavirus disease 2019 and cardiovascular complications: Focused clinical review. J. Hypertens. 2021, 39, 1282–1292. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Long, B.; Brady, W.J.; Koyfman, A.; Gottlieb, M. Cardiovascular complications in COVID-19. Am. J. Emerg. Med. 2020, 38, 1504–1507. [Google Scholar] [CrossRef] [PubMed]
- Zanoli, L.; Briet, M.; Empana, J.P.; Cunha, P.G.; Mäki-Petäjä, K.M.; Protogerou, A.D.; Tedgui, A.; Touyz, R.M.; Schiffrin, E.L.; Spronck, B.; et al. Vascular consequences of inflammation: A position statement from the ESH Working Group on Vascular Structure and Function and the ARTERY Society. J. Hypertens. 2020, 38, 1682–1698. [Google Scholar] [CrossRef]
- Teuwen, L.-A.; Geldhof, V.; Pasut, A.; Carmeliet, P. COVID-19: The vasculature unleashed. Nat. Rev. Immunol. 2020, 20, 389–391. [Google Scholar] [CrossRef]
- Mitchell, G.F. Arterial Stiffness and Wave Reflection: Biomarkers of Cardiovascular Risk. Artery Res. 2009, 3, 56–64. [Google Scholar] [CrossRef]
- Mitchell, G.F. Arterial stiffness and hypertension: Chicken or egg? Hypertension 2014, 64, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Beale, A.L.; Meyer, P.; Marwick, T.H.; Lam, C.S.; Kaye, D.M. Sex Differences in Cardiovascular Pathophysiology: Why Women Are Overrepresented in Heart Failure with Preserved Ejection Fraction. Circulation 2018, 138, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Zisis, S.; Durieux, J.; Mouchati, C.; Funderburg, N.; Ailstock, K.; Chong, M.; Labbato, D.; McComsey, G. Arterial Stiffness and Oxidized LDL Independently Associated with Post-Acute Sequalae of SARS-CoV-2. Pathog. Immun. 2023, 8, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Mouchati, C.; Durieux, J.C.; Zisis, S.N.; Labbato, D.; Rodgers, M.A.; Ailstock, K.; Reinert, B.L.; Funderburg, N.T.; McComsey, G.A. Increase in gut permeability and oxidized ldl is associated with post-acute sequelae of SARS-CoV-2. Front. Immunol. 2023, 14, 1182544. [Google Scholar] [CrossRef]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Yoon, K.; Kim, N. Roles of Sex Hormones and Gender in the Gut Microbiota. J. Neurogastroenterol. Motil. 2021, 27, 314–325. [Google Scholar] [CrossRef]
- Chen, K.L.; Madak-Erdogan, Z. Estrogen and Microbiota Crosstalk: Should We Pay Attention? Trends Endocrinol. Metab. 2016, 27, 752–755. [Google Scholar] [CrossRef]
- Menon, R.; Watson, S.E.; Thomas, L.N.; Allred, C.D.; Dabney, A.; Azcarate-Peril, M.A.; Sturino, J.M. Diet complexity and estrogen receptor β status affect the composition of the murine intestinal microbiota. Appl. Environ. Microbiol. 2013, 79, 5763–5773. [Google Scholar] [CrossRef]
- Santos-Marcos, J.A.; Mora-Ortiz, M.; Tena-Sempere, M.; Lopez-Miranda, J.; Camargo, A. Interaction between gut microbiota and sex hormones and their relation to sexual dimorphism in metabolic diseases. Biol. Sex Differ. 2023, 14, 4. [Google Scholar] [CrossRef]
- Takahashi, T.; Iwasaki, A. Sex differences in immune responses. Science 2021, 371, 347–348. [Google Scholar] [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Chen, Y.; Yuan, J.; Yi, P.; Ding, C.; Wu, W.; Li, Y.; Ni, Q.; Zou, R.; Li, X.; et al. Factors Associated with Prolonged Viral RNA Shedding in Patients with Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2020, 71, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Sharma, G.; Volgman, A.S.; Michos, E.D. Sex Differences in Mortality from COVID-19 Pandemic: Are Men Vulnerable and Women Protected? JACC Case Rep. 2020, 2, 1407–1410. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Swank, Z.; Senussi, Y.; Manickas-Hill, Z.; Yu, X.G.; Li, J.Z.; Alter, G.; Walt, D.R. Persistent Circulating Severe Acute Respiratory Syndrome Coronavirus 2 Spike Is Associated with Post-acute Coronavirus Disease 2019 Sequelae. Clin. Infect. Dis. 2022, 76, e487–e490. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Newson, L.; Briggs, T.A.; Grammatopoulos, D.; Young, L.; Gill, P. Long COVID risk—A signal to address sex hormones and women’s health. Lancet Reg. Health Eur. 2021, 11, 100242. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, I.G.; Hussain, I.I.; Almalki, S.S.; Alghamdi, M.S.; Alghamdi, M.M.; El-Sheemy, M.A. The pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia: A descriptive epidemiological analysis of data from the Saudi Ministry of Health. Int. J. Gen. Med. 2014, 7, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Karlberg, J.; Chong, D.S.Y.; Lai, W.Y. Do men have a higher case fatality rate of severe acute respiratory syndrome than women do? Am. J. Epidemiol. 2004, 159, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Leung, G.M.; Hedley, A.J.; Ho, L.-M.; Chau, P.; Wong, I.O.; Thach, T.Q.; Ghani, A.C.; Donnelly, C.A.; Fraser, C.; Riley, S.; et al. The epidemiology of severe acute respiratory syndrome in the 2003 Hong Kong epidemic: An analysis of all 1755 patients. Ann. Intern. Med. 2004, 141, 662–673. [Google Scholar] [CrossRef]
- Ratchford, S.M.; Stickford, J.L.; Province, V.M.; Stute, N.; Augenreich, M.A.; Koontz, L.K.; Bobo, L.K.; Stickford, A.S. Vascular alterations among young adults with SARS-CoV-2. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H404–H410. [Google Scholar] [CrossRef]
- Szeghy, R.E.; Stute, N.L.; Province, V.M.; Augenreich, M.A.; Stickford, J.L.; Stickford, A.S.L.; Ratchford, S.M. Six-month longitudinal tracking of arterial stiffness and blood pressure in young adults following SARS-CoV-2 infection. J. Appl. Physiol. 2022, 132, 1297–1309. [Google Scholar] [CrossRef] [PubMed]
- Rodilla, E.; Lopez-Carmona, M.D.; Cortes, X.; Cobos-Palacios, L.; Canales, S.; Saez, M.C.; Escudero, S.C.; Rubio-Rivas, M.; Manglano, J.D.; Castro, S.J.F.; et al. Impact of Arterial Stiffness on All-Cause Mortality in Patients Hospitalized with COVID-19 in Spain. Hypertension 2021, 77, 856–867. [Google Scholar] [CrossRef] [PubMed]
- Schnaubelt, S.; Oppenauer, J.; Tihanyi, D.; Mueller, M.; Maldonado-Gonzalez, E.; Zejnilovic, S.; Haslacher, H.; Perkmann, T.; Strassl, R.; Anders, S.; et al. Arterial stiffness in acute COVID-19 and potential associations with clinical outcome. J. Intern. Med. 2021, 290, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Szoltysek-Boldys, I.; Zielinska-Danch, W.; Loboda, D.; Wilczek, J.; Gibinski, M.; Paradowska-Nowakowska, E.; Golba, K.S.; Sarecka-Hujar, B. Photoplethysmographic Measurement of Arterial Stiffness in Polish Patients with Long-COVID-19 Syndrome-The Results of a Cross-Sectional Study. Diagnostics 2022, 12, 3189. [Google Scholar] [CrossRef] [PubMed]
- Tudoran, C.; Bende, F.; Bende, R.; Giurgi-Oncu, C.; Dumache, R.; Tudoran, M. Correspondence between Aortic and Arterial Stiffness, and Diastolic Dysfunction in Apparently Healthy Female Patients with Post-Acute COVID-19 Syndrome. Biomedicines 2023, 11, 492. [Google Scholar] [CrossRef] [PubMed]
- Pettersson-Pablo, P.; Cao, Y.; Breimer, L.H.; Nilsson, T.K.; Hurtig-Wennlöf, A. Pulse wave velocity, augmentation index, and carotid intima-media thickness are each associated with different inflammatory protein signatures in young healthy adults: The lifestyle, biomarkers and atherosclerosis study. Atherosclerosis 2020, 313, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Tap, L.; Dommershuijsen, L.J.; Corsonello, A.; Lattanzio, F.; Bustacchini, S.; Ziere, G.; van Saase, J.L.; Mattace-Raso, F.U. The Possible Impact of Aortic Stiffness on Quality of Late Life: An Exploratory Study. Clin. Interv. Aging 2020, 15, 133–140. [Google Scholar] [CrossRef]
- Mohan, V.; Poongothai, S.; Pradeepa, R.; Indulekha, K.; Surendar, J. Association of depression with common carotid artery intima media thickness and augmentation index in a large Urban South Indian population—The Chennai Urban Rural Epidemiology Study (CURES—138). Indian J. Endocrinol. Metab. 2015, 19, 136–142. [Google Scholar] [CrossRef]
- Szucs, B.; Petrekanits, M.; Varga, J. Effectiveness of a 4-week rehabilitation program on endothelial function, blood vessel elasticity in patients with chronic obstructive pulmonary disease. J. Thorac. Dis. 2018, 10, 6482–6490. [Google Scholar] [CrossRef]
- Vanfleteren, L.E.; Spruit, M.A.; Groenen, M.T.; Bruijnzeel, P.L.; Taib, Z.; Rutten, E.P.; Op ‘t Roodt, J.; Akkermans, M.A.; Wouters, E.F.; Franssen, F.M. Arterial stiffness in patients with COPD: The role of systemic inflammation and the effects of pulmonary rehabilitation. Eur. Respir. J. 2014, 43, 1306–1315. [Google Scholar] [CrossRef]
- Ambrosino, P.; Molino, A.; Calcaterra, I.; Formisano, R.; Stufano, S.; Spedicato, G.A.; Motta, A.; Papa, A.; Di Minno, M.N.D.; Maniscalco, M. Clinical Assessment of Endothelial Function in Convalescent COVID-19 Patients Undergoing Multidisciplinary Pulmonary Rehabilitation. Biomedicines 2021, 9, 614. [Google Scholar] [CrossRef] [PubMed]
- Rubinshtein, R.; Kuvin, J.T.; Soffler, M.; Lennon, R.J.; Lavi, S.; Nelson, R.E.; Pumper, G.M.; Lerman, L.O.; Lerman, A. Assessment of endothelial function by non-invasive peripheral arterial tonometry predicts late cardiovascular adverse events. Eur. Heart J. 2010, 31, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Axtell, A.L.; Gomari, F.A.; Cooke, J.P. Assessing endothelial vasodilator function with the Endo-PAT 2000. J. Vis. Exp. 2010, 44, e2167. [Google Scholar]
- Wilkinson, I.B.; MacCallum, H.; Flint, L.; Cockcroft, J.R.; Newby, D.E.; Webb, D.J. The influence of heart rate on augmentation index and central arterial pressure in humans. J. Physiol. 2000, 525 Pt 1, 263–270. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| COVID+ (n = 151) | COVID− (n = 94) | p-Value | |||||
|---|---|---|---|---|---|---|---|
| n (%) or Median (IQR)/Mean ± Std | |||||||
| Demographics | |||||||
| Age (years) | 45.9 ± 13.4 | 40.9 ± 14.2 | 0.01 | ||||
| Sex (Female) | 86 (56.9) | 47 (50.0) | 0.3 | ||||
| Non-white Race * | 46 (30.5) | 36 (38.3) | 0.2 | ||||
| BMI (kg/m2) | 29.9 ± 6.4 | 29.3 ± 5.6 | 0.6 | ||||
| Current Smoker (Yes) | 26 (17.2) | 28 (29.8) | 0.02 | ||||
| Hypertension at Baseline (Yes) | 33 (21.9) | 13 (13.8) | 0.1 | ||||
| Diabetes at Baseline (yes) | 8 (5.3) | 4 (4.3) | 0.7 | ||||
| Number of days since COVID-19 Diagnosis | 249.0 (139.0, 510.0) | -- | -- | ||||
| Total Number of self-reported PASC Symptoms ** | |||||||
| 1 to 6 | 47 (31.1) | -- | -- | ||||
| ≥7 | 53 (35.1) | -- | -- | ||||
| Current Medications | |||||||
| ACE or ARB (Yes) *** | 13 (8.6) | 7 (2.9) | 0.7 | ||||
| Beta Blocker (Yes) | 6 (3.9) | 0 | 0.08 | ||||
| Statin (Yes) | 8 (5.3) | 9 (9.6) | 0.2 | ||||
| Laboratory Data | |||||||
| Cholesterol (mg/dL) | 180.8 ± 33.9 | 176.2 ± 33.8 | 0.3 | ||||
| non-HDL (mg/dL) **** | 127.8 ± 36.2 | 126.5 ± 39.5 | 0.5 | ||||
| Triglycerides (mg/dL) | 119.3 ± 70.8 | 126.3 ± 129.9 | 0.7 | ||||
| Biomarkers | |||||||
| Coagulation; D-dimer (ng/mL) | 415.6 (257.3, 617.1) | 358.3 (204.0, 584.5) | 0.2 | ||||
| OxLDL ***** | 76.6 ± 32.1 | 53.9 ± 24.9 | <.0001 | ||||
| Inflammation; hs-CRP (ng/mL) | 2792.9 (1193.2, 7241.8) | 2595.6 (818.5, 7525.1) | 0.3 | ||||
| Gut permeability; Zonulin (mg/mL) | 4282.9 (2462.8, 6506.5) | 3053.9 (1947.9, 5165.0) | 0.01 | ||||
| uOR (95% CI); p-Value ** | aOR (95% CI); p-Value *** | ||
|---|---|---|---|
| COVID-19 Status (+ vs. −) | 1.32 (0.79, 2.22); p = 0.3 | 1.2 (0.68, 2.12); p = 0.5 | |
| BMI (kg/m2) | 1.05 (1.01, 1.11); p = 0.03 | 1.06 (1.01, 1.11); p = 0.04 | |
| non-HDL (mg/dL) | 3.18 (1.29, 7.81); p = 0.01 | 2.49 (0.91, 6.83); p = 0.08 | |
| OX-LDL | 2.01 (1.1, 3.67); p = 0.02 | 1.7 (0.85, 3.55); p = 0.1 | |
| Ddimer (ng/mL) | 1.57 (1.1, 2.24); p = 0.01 | 1.93 (1.23, 3.05); p = 0.01 | |
| Zonulin (mg/mL) | 1.86 (1.27, 2.73); p = 0.001 | 1.89 (1.25, 2.84); p = 0.002 | |
| COVID+ | COVID− | p-Value ** | ||||
|---|---|---|---|---|---|---|
| Mean ± Std/n(%) | ||||||
| Augmentation Index @75 bpm | ||||||
| Overall | 8.44 ± 15.73 | 0.88 ± 17.15 | 0.001 | |||
| Female | 13.83 ± 16.27 | 7.64 ± 16.38 | ||||
| Male | 1.31 ± 11.73 | −5.87 ± 15.27 | ||||
| Reactive Hyperemia Index (%) | ||||||
| Overall | 1.87 ± 0.63 | 1.89 ± 0.59 | 0.9 | |||
| Female | 1.86 ± 0.56 | 1.87 ± 0.5 | ||||
| Male | 1.88 ± 0.69 | 1.9 ± 0.67 | ||||
| Reactive Hyperemia Index (≤1.67) | ||||||
| Overall | 66 (43.7) | 40 (42.6) | 0.8 | |||
| Female | 41 (47.67) | 19 (40.43) | ||||
| Male | 25 (38.46) | 21 (44.68) | ||||
| Unadjusted | p-Value | Adjusted ** | p-Value *** | ||
|---|---|---|---|---|---|
| Estimate ± s.e. | Estimate ± s.e. | ||||
| COVID-19 and PASC STATUS | 0.001 | 0.002 | |||
| COVID+ PASC+ | 9.06 ± 1.99 | 11.84 ± 2.4 | |||
| COVID+ No PASC | 0.92 ± 2.64 | 5.53 ± 2.72 | |||
| COVID- | −0.17 ± 1.59 | 5.47 ± 2.25 | |||
| SEX (F vs. M) | 9.26 ± 2.23 | <0.0001 | 14.86 ± 1.81 | <0.0001 | |
| OxLDL | 0.07 ± 0.04 | 0.1 | 0.03 ± 0.04 | 0.4 | |
| D-dimer | 5.22 ± 1.39 | 0.0002 | −1.85 ± 1.12 | 0.1 | |
| Zonulin | 3.52 ± 1.45 | 0.02 | −0.8 ± 1.21 | 0.4 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durieux, J.C.; Zisis, S.N.; Mouchati, C.; Labbato, D.; Abboud, M.; McComsey, G.A. Sex Modifies the Effect of COVID-19 on Arterial Elasticity. Viruses 2024, 16, 1089. https://doi.org/10.3390/v16071089
Durieux JC, Zisis SN, Mouchati C, Labbato D, Abboud M, McComsey GA. Sex Modifies the Effect of COVID-19 on Arterial Elasticity. Viruses. 2024; 16(7):1089. https://doi.org/10.3390/v16071089
Chicago/Turabian StyleDurieux, Jared C., Sokratis N. Zisis, Christian Mouchati, Danielle Labbato, Marc Abboud, and Grace A. McComsey. 2024. "Sex Modifies the Effect of COVID-19 on Arterial Elasticity" Viruses 16, no. 7: 1089. https://doi.org/10.3390/v16071089
APA StyleDurieux, J. C., Zisis, S. N., Mouchati, C., Labbato, D., Abboud, M., & McComsey, G. A. (2024). Sex Modifies the Effect of COVID-19 on Arterial Elasticity. Viruses, 16(7), 1089. https://doi.org/10.3390/v16071089