
Elevated Serum Presepsin Identifies Herpes Simplex Virus-1 Reactivation in COVID-19 Patients
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Measurement of Serum Presepsin Levels
2.3. Microbiological Tests and Bronchoalveolar Lavage
2.4. Routine Laboratory Testing
2.5. Statistical Analysis
3. Results
3.1. Serum Presepsin Levels of Healthy Controls and Patients with COVID-19
3.2. Effect of Vasopressor Therapy and Dialysis on Serum Presepsin
3.3. Correlation of Serum Presepsin Levels with Inflammation
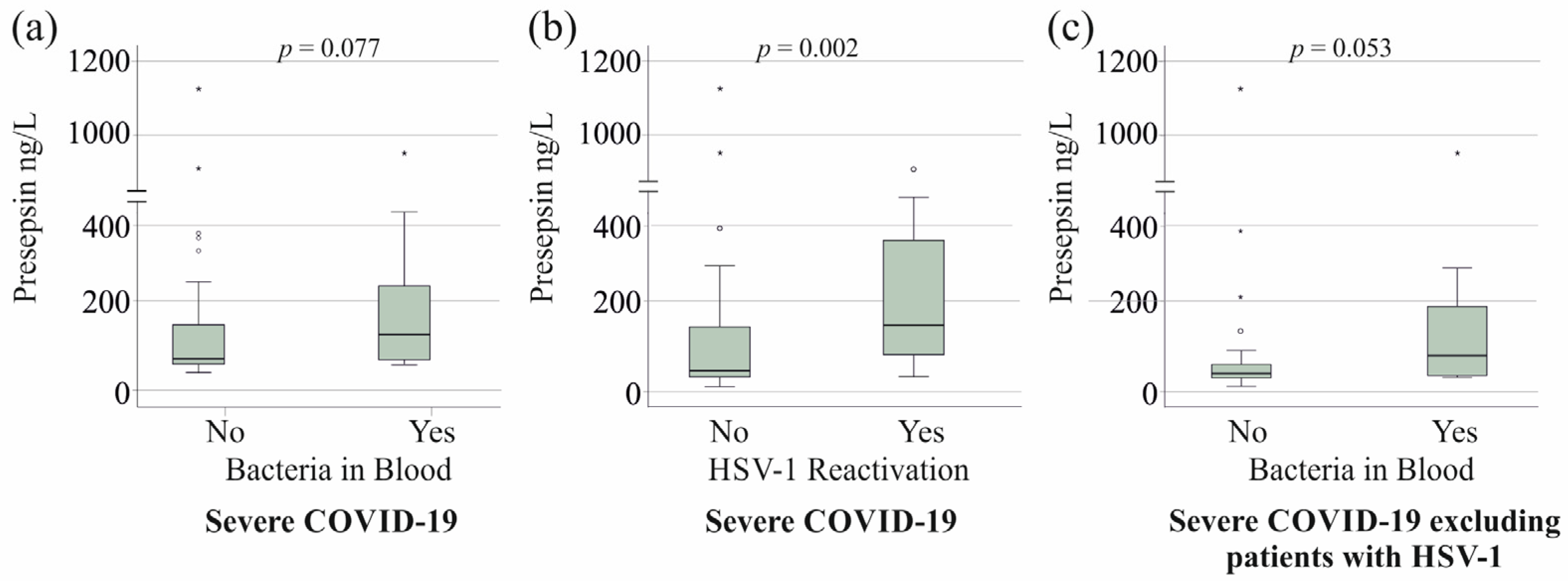
3.4. Serum Presepsin Levels of Patients with Superinfections and HSV-1 Reactivation
3.5. Serum Presepsin Levels and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ruscica, M.; Macchi, C.; Iodice, S.; Tersalvi, G.; Rota, I.; Ghidini, S.; Terranova, L.; Valenti, L.; Amati, F.; Aliberti, S.; et al. Prognostic parameters of in-hospital mortality in COVID-19 patients-An Italian experience. Eur. J. Clin. Investig. 2021, 51, e13629. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.D.; Sumeh, A.S.; Sheraz, M.; Kavitha, M.S.; Venmathi Maran, B.A.; Rodrigues, K.F. A mini-review on the impact of COVID-19 on vital organs. Biomed. Pharmacother. 2021, 143, 112158. [Google Scholar] [CrossRef] [PubMed]
- Grewal, T.; Buechler, C. Adipokines as Diagnostic and Prognostic Markers for the Severity of COVID-19. Biomedicines 2023, 11, 1302. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Jafri, L.; Hoodbhoy, Z.; Siddiqui, I. Prognostic Value of Serum Procalcitonin in COVID-19 Patients: A Systematic Review. Indian. J. Crit. Care Med. 2021, 25, 77–84. [Google Scholar] [CrossRef]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in COVID-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef]
- Semiz, S. COVID19 biomarkers: What did we learn from systematic reviews? Front. Cell Infect. Microbiol. 2022, 12, 1038908. [Google Scholar] [CrossRef]
- Guarino, M.; Perna, B.; Maritati, M.; Remelli, F.; Trevisan, C.; Spampinato, M.D.; Costanzini, A.; Volpato, S.; Contini, C.; De Giorgio, R. Presepsin levels and COVID-19 severity: A systematic review and meta-analysis. Clin. Exp. Med. 2023, 23, 993–1002. [Google Scholar] [CrossRef]
- Wu, Z.; Geng, N.; Liu, Z.; Pan, W.; Zhu, Y.; Shan, J.; Shi, H.; Han, Y.; Ma, Y.; Liu, B. Presepsin as a prognostic biomarker in COVID-19 patients: Combining clinical scoring systems and laboratory inflammatory markers for outcome prediction. Virol. J. 2024, 21, 96. [Google Scholar] [CrossRef]
- Yamazaki, A.; Nukui, Y.; Kameda, T.; Saito, R.; Koda, Y.; Ichimura, N.; Tohda, S.; Ohkawa, R. Variation in presepsin and thrombomodulin levels for predicting COVID-19 mortality. Sci. Rep. 2023, 13, 21493. [Google Scholar] [CrossRef]
- Chenevier-Gobeaux, C.; Borderie, D.; Weiss, N.; Mallet-Coste, T.; Claessens, Y.E. Presepsin (sCD14-ST), an innate immune response marker in sepsis. Clin. Chim. Acta 2015, 450, 97–103. [Google Scholar] [CrossRef]
- Arai, Y.; Mizugishi, K.; Nonomura, K.; Naitoh, K.; Takaori-Kondo, A.; Yamashita, K. Phagocytosis by human monocytes is required for the secretion of presepsin. J. Infect. Chemother. 2015, 21, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Juan, T.S.; Kelley, M.J.; Johnson, D.A.; Busse, L.A.; Hailman, E.; Wright, S.D.; Lichenstein, H.S. Soluble CD14 truncated at amino acid 152 binds lipopolysaccharide (LPS) and enables cellular response to LPS. J. Biol. Chem. 1995, 270, 1382–1387. [Google Scholar] [CrossRef] [PubMed]
- Ferrarese, A.; Frigo, A.C.; Mion, M.M.; Plebani, M.; Russo, F.P.; Germani, G.; Gambato, M.; Cillo, U.; Cattelan, A.; Burra, P.; et al. Diagnostic and prognostic role of presepsin in patients with cirrhosis and bacterial infection. Clin. Chem. Lab. Med. 2021, 59, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Tanimura, S.; Fujieda, Y.; Kono, M.; Shibata, Y.; Hisada, R.; Sugawara, E.; Nakamura, H.; Ohmura, K.; Shimamura, S.; Mitani, A.; et al. Clinical significance of plasma presepsin levels in patients with systemic lupus erythematosus. Mod. Rheumatol. 2018, 28, 865–871. [Google Scholar] [CrossRef]
- Formenti, P.; Gotti, M.; Palmieri, F.; Pastori, S.; Roccaforte, V.; Menozzi, A.; Galimberti, A.; Umbrello, M.; Sabbatini, G.; Pezzi, A. Presepsin in Critical Illness: Current Knowledge and Future Perspectives. Diagnostics 2024, 14, 1311. [Google Scholar] [CrossRef]
- Ikegame, A.; Kondo, A.; Kitaguchi, K.; Sasa, K.; Miyoshi, M. Presepsin production in monocyte/macrophage-mediated phagocytosis of neutrophil extracellular traps. Sci. Rep. 2022, 12, 5978. [Google Scholar] [CrossRef]
- Pluta, M.P.; Czempik, P.F.; Kwiatkowska, M.; Marczyk-Belbot, K.; Maslanka, S.; Mika, J.; Krzych, L.J. Presepsin Does Not Predict Risk of Death in Sepsis Patients Admitted to the Intensive Care Unit: A Prospective Single-Center Study. Biomedicines 2024, 12, 2313. [Google Scholar] [CrossRef]
- Endo, S.; Suzuki, Y.; Takahashi, G.; Shozushima, T.; Ishikura, H.; Murai, A.; Nishida, T.; Irie, Y.; Miura, M.; Iguchi, H.; et al. Usefulness of presepsin in the diagnosis of sepsis in a multicenter prospective study. J. Infect. Chemother. 2012, 18, 891–897. [Google Scholar] [CrossRef]
- Bergmann, F.; Gabler, C.; Nussbaumer-Proll, A.; Wolfl-Duchek, M.; Blaschke, A.; Radtke, C.; Zeitlinger, M.; Jorda, A. Early Bacterial Coinfections in Patients Admitted to the ICU With COVID-19 or Influenza: A Retrospective Cohort Study. Crit. Care Explor. 2023, 5, e0895. [Google Scholar] [CrossRef]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaelo, M.; Longuet Flandre, P.; Dubert, M.; Cally, R.; Logre, E.; Fraisse, M.; Mentec, H.; et al. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann. Intensive Care 2020, 10, 119. [Google Scholar] [CrossRef]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and outcomes of co-infection and superinfection with SARS-CoV-2 and other pathogens: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.; Yue, S.; Xue, W. Herpes simplex and herpes zoster viruses in COVID-19 patients. Ir. J. Med. Sci. 2022, 191, 1093–1097. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Di Bella, S.; Dettori, S.; Brucci, G.; Zerbato, V.; Pol, R.; Segat, L.; D’Agaro, P.; Roman-Pognuz, E.; Friso, F.; et al. Reactivation of Herpes Simplex Virus Type 1 (HSV-1-1) Detected on Bronchoalveolar Lavage Fluid (BALF) Samples in Critically Ill COVID-19 Patients Undergoing Invasive Mechanical Ventilation: Preliminary Results from Two Italian Centers. Microorganisms 2022, 10, 362. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-Garcia, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Bazaid, A.S.; Barnawi, H.; Qanash, H.; Alsaif, G.; Aldarhami, A.; Gattan, H.; Alharbi, B.; Alrashidi, A.; Al-Soud, W.A.; Moussa, S.; et al. Bacterial Coinfection and Antibiotic Resistance Profiles among Hospitalised COVID-19 Patients. Microorganisms 2022, 10, 495. [Google Scholar] [CrossRef]
- Zsichla, L.; Muller, V. Risk Factors of Severe COVID-19: A Review of Host, Viral and Environmental Factors. Viruses 2023, 15, 175. [Google Scholar] [CrossRef]
- Kluge, S.; Janssens, U.; Spinner, C.D.; Pfeifer, M.; Marx, G.; Karagiannidis, C. Clinical Practice Guideline: Recommendations on Inpatient Treatment of Patients with COVID-19. Dtsch. Arztebl. Int. 2021, 118, 375. [Google Scholar] [CrossRef]
- Bone, R.C. Sepsis, sepsis syndrome, and the systemic inflammatory response syndrome (SIRS). Gulliver in Laputa. JAMA 1995, 273, 155–156. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines. Available online: https://wayback.archive-it.org/4887/20240626155208/https://www.covid19treatmentguidelines.nih.gov (accessed on 21 February 2025).
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 49, e1063–e1143. [Google Scholar] [CrossRef]
- Karakike, E.; Giamarellos-Bourboulis, E.J.; Kyprianou, M.; Fleischmann-Struzek, C.; Pletz, M.W.; Netea, M.G.; Reinhart, K.; Kyriazopoulou, E. Coronavirus Disease 2019 as Cause of Viral Sepsis: A Systematic Review and Meta-Analysis. Crit. Care Med. 2021, 49, 2042–2057. [Google Scholar] [CrossRef] [PubMed]
- Botondi, V.; D’Adamo, E.; Trubiani, O.; Gazzolo, D. Effects of temperature on presepsin assessment in biological fluids. Ital. J. Anat. Embryol. 2023, 127, 69–72. [Google Scholar] [CrossRef]
- Zhang, J.; Hu, Z.-D.; Song, J.H.; Shao, J. Diagnostic Value of Presepsin for Sepsis. Medicine 2015, 94, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Idelevich, E.A.; Reischl, U.; Becker, K. New Microbiological Techniques in the Diagnosis of Bloodstream Infections. Dtsch. Arztebl. Int. 2018, 115, 822–832. [Google Scholar] [CrossRef]
- Schwertner, B.; Lindner, G.; Toledo Stauner, C.; Klapproth, E.; Magnus, C.; Rohrhofer, A.; Gross, S.; Schuler-Thurner, B.; Ottl, V.; Feichtgruber, N.; et al. Nectin-1 Expression Correlates with the Susceptibility of Malignant Melanoma to Oncolytic Herpes Simplex Virus In Vitro and In Vivo. Cancers 2021, 13, 3058. [Google Scholar] [CrossRef]
- Miyoshi, M.; Inoue, Y.; Nishioka, M.; Ikegame, A.; Nakao, T.; Kishi, S.; Doi, T.; Nagai, K. Clinical evaluation of presepsin considering renal function. PLoS ONE 2019, 14, e0215791. [Google Scholar] [CrossRef]
- Nagata, T.; Yasuda, Y.; Ando, M.; Abe, T.; Katsuno, T.; Kato, S.; Tsuboi, N.; Matsuo, S.; Maruyama, S. Clinical impact of kidney function on presepsin levels. PLoS ONE 2015, 10, e0129159. [Google Scholar] [CrossRef]
- Kocyigit, A.; Sogut, O.; Durmus, E.; Kanimdan, E.; Guler, E.M.; Kaplan, O.; Yenigun, V.B.; Eren, C.; Ozman, Z.; Yasar, O. Circulating furin, IL-6, and presepsin levels and disease severity in SARS-CoV-2-infected patients. Sci. Prog. 2021, 104, 368504211026119. [Google Scholar] [CrossRef]
- Assal, H.H.; Abdelrahman, S.M.; Abdelbasset, M.A.; Abdelaziz, M.; Sabry, I.M.; Shaban, M.M. Presepsin as a Novel Biomarker in predicting In-hospital Mortality in Patients With COVID-19 Pneumonia. Int. J. Infect. Dis. 2022, 118, 155–163. [Google Scholar] [CrossRef]
- Simon, L.; Gauvin, F.; Amre, D.K.; Saint-Louis, P.; Lacroix, J. Serum procalcitonin and C-reactive protein levels as markers of bacterial infection: A systematic review and meta-analysis. Clin. Infect. Dis. 2004, 39, 206–217. [Google Scholar] [CrossRef]
- Kim, J.H. Clinical Utility of Procalcitonin on Antibiotic Stewardship: A Narrative Review. Infect. Chemother. 2022, 54, 610–620. [Google Scholar] [CrossRef] [PubMed]
- Lai, L.; Lai, Y.; Wang, H.; Peng, L.; Zhou, N.; Tian, Y.; Jiang, Y.; Gong, G. Diagnostic Accuracy of Procalcitonin Compared to C-Reactive Protein and Interleukin 6 in Recognizing Gram-Negative Bloodstream Infection: A Meta-Analytic Study. Dis. Markers 2020, 2020, 4873074. [Google Scholar] [CrossRef] [PubMed]
- Nargis, W.; Ibrahim, M.; Ahamed, B.U. Procalcitonin versus C-reactive protein: Usefulness as biomarker of sepsis in ICU patient. Int. J. Crit. Illn. Inj. Sci. 2014, 4, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Pink, I.; Raupach, D.; Fuge, J.; Vonberg, R.P.; Hoeper, M.M.; Welte, T.; Rademacher, J. C-reactive protein and procalcitonin for antimicrobial stewardship in COVID-19. Infection 2021, 49, 935–943. [Google Scholar] [CrossRef]
- Park, W.B.; Lee, K.D.; Lee, C.S.; Jang, H.C.; Kim, H.B.; Lee, H.S.; Oh, M.D.; Choe, K.W. Production of C-reactive protein in Escherichia coli-infected patients with liver dysfunction due to liver cirrhosis. Diagn. Microbiol. Infect. Dis. 2005, 51, 227–230. [Google Scholar] [CrossRef]
- Pieri, G.; Agarwal, B.; Burroughs, A.K. C-reactive protein and bacterial infection in cirrhosis. Ann. Gastroenterol. 2014, 27, 113–120. [Google Scholar]
- Ng, K.J.; Yu, H.C.; Huang Tseng, H.Y.; Hsu, C.W.; Lu, M.C. Modestly Elevated Serum Procalcitonin Levels in Patients with Rheumatoid Arthritis Free of Active Infection. Medicina 2020, 56, 545. [Google Scholar] [CrossRef] [PubMed]
- Stogbauer, F.; Neumeier, M.; Weigert, J.; Wanninger, J.; Grandl, M.; Lehle, K.; Schmitz, G.; Aslanidis, C.; Schaffler, A.; Scholmerich, J.; et al. Highly efficient and low-cost method to isolate human blood monocytes with high purity. J. Immunol. Methods 2008, 337, 78–80. [Google Scholar] [CrossRef]
- Cormican, S.; Griffin, M.D. Human Monocyte Subset Distinctions and Function: Insights From Gene Expression Analysis. Front. Immunol. 2020, 11, 1070. [Google Scholar] [CrossRef]
- Lee, K.R.; Hong, D.Y.; Paik, J.H.; Jung, H.M. Prognostic Value of Plasma Presepsin and Pneumonia Severity Index in Patients with Community-Acquired Pneumonia in the Emergency Department. Medicina 2022, 58, 1504. [Google Scholar] [CrossRef]
- Çağlar, F.N.; Yildiz, C.; Korkusuz, R.; Yasar, K.K.; Isıksacan, N. Serum presepsin levels among patients with COVID-19. Indian. J. Med. Spec. 2022, 13, 17–22. [Google Scholar] [CrossRef]
- Forbes, H.; Warne, B.; Doelken, L.; Brenner, N.; Waterboer, T.; Luben, R.; Wareham, N.J.; Warren-Gash, C.; Gkrania-Klotsas, E. Risk factors for herpes simplex virus type-1 infection and reactivation: Cross-sectional studies among EPIC-Norfolk participants. PLoS ONE 2019, 14, e0215553. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.; Buetti, N.; Houhou-Fidouh, N.; Patrier, J.; Abdel-Nabey, M.; Jaquet, P.; Presente, S.; Girard, T.; Sayagh, F.; Ruckly, S.; et al. HSV-1-1 reactivation is associated with an increased risk of mortality and pneumonia in critically ill COVID-19 patients. Crit. Care 2021, 25, 417. [Google Scholar] [CrossRef]
- Talukder, S.; Deb, P.; Parveen, M.; Zannat, K.E.; Bhuiyan, A.H.; Yeasmin, M.; Molla, M.M.A.; Saif-Ur-Rahman, K.M. Clinical features and outcomes of COVID-19 patients with concomitant herpesvirus co-infection or reactivation: A systematic review. New Microbes New Infect. 2024, 58, 101233. [Google Scholar] [CrossRef] [PubMed]
- Chiesa, A.F.; Pallanza, M.; Martinetti, G.; Lanzi, F.; Previsdomini, M.; Pagnamenta, A.; Elzi, L. Herpes simplex virus reactivation in patients with COVID-19 and acute respiratory distress syndrome: A prospective cohort study. Antivir. Ther. 2022, 27, 13596535211068613. [Google Scholar] [CrossRef]
- Aliu-Bejta, A.; Atelj, A.; Kurshumliu, M.; Dreshaj, S.; Barsic, B. Presepsin values as markers of severity of sepsis. Int. J. Infect. Dis. 2020, 95, 1–7. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Moderate COVID-19 | Severe COVID-19 |
|---|---|---|
| Males/Females | 34/29 | 42/18 |
| Age (years) | 60 (22–83) | 57 (31–83) |
| BMI (kg/m2) | 26.3 (18.4–42.6) 32 | 29.4 (19.2–66.7) 56; p = 0.008 |
| C-reactive protein (mg/L) | 26 (0–222) | 74 (1–367) p < 0.001 |
| Procalcitonin (ng/L) | 90 (0–24,900) | 240 (60–25,000) p < 0.001 |
| LDH (U/L) | 224 (127–929) 39 | 378 (162–1534) p < 0.001 |
| AP (U/L) | 96 (38–372) 29 | 99 (37–743) |
| Ferritin (ng/mL) | 573 (32–4826) 45 | 1088 (77–21,976) 60; p < 0.001 |
| Interleukin-6 (ng/L) | 19 (4–265) 37 | 36 (3–1175) |
| Neutrophils (n × 109/L) | 4.05 (0.13–23.10) | 8.18 (0.90–24.91) p < 0.001 |
| Basophils (n × 109/L) | 0.03 (0–0.21) | 0.05 (0.01–0.17) p < 0.001 |
| Eosinophils (n × 109/L) | 0.08 (0–1.19) | 0.04 (0–1.07) |
| Monocytes (n × 109/L) | 0.57 (0.07–2.52) | 0.71 (0.03–2.21) p = 0.037 |
| Lymphocytes (n × 109/L) | 1.11 (0.09–57.83) | 1.20 (0–75.95) |
| Immature granulocytes (n × 109/L) | 0.03 (0–1.38) | 0.25 (0.04–2.92) p < 0.001 |
| Intervention/Drug | No | Yes | p-Value |
|---|---|---|---|
| Moderate COVID-19 | |||
| Dialysis (6 patients) | 50 (0–310) | 80 (11–238) | 0.274 |
| Severe COVID-19 | |||
| Dialysis (7 patients) | 61 (11–1127) | 246 (33–907) | 0.039 |
| Catecholamine (41 patients) | 44 (11–360) | 99 (21–1127) | 0.016 |
| Inflammation Marker | Moderate COVID-19 | Severe COVID-19 |
|---|---|---|
| C-reactive protein | 0.241 | 0.357 p = 0.005 |
| Procalcitonin | 0.519 p < 0.001 | 0.434 p = 0.001 |
| Interleukin-6 | 0.164 | 0.294 p = 0.023 |
| Ferritin | 0.107 | 0.246 |
| Neutrophils | 0.187 | 0.035 |
| Basophils | 0.161 | 0.186 |
| Eosinophils | 0.139 | 0.310 p = 0.016 |
| Monocytes | 0.092 | −0.002 |
| Lymphocytes | 0.006 | 0.074 |
| Immature granulocytes | 0.305 p = 0.015 | −0.041 |
| Inflammation Marker | Severe COVID-19 |
|---|---|
| C-reactive protein | 0.399 p = 0.011 |
| Procalcitonin | 0.361 p = 0.022 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mester, P.; Keller, D.; Kunst, C.; Schmid, S.; Krautbauer, S.; Müller, M.; Buechler, C.; Pavel, V. Elevated Serum Presepsin Identifies Herpes Simplex Virus-1 Reactivation in COVID-19 Patients. Viruses 2025, 17, 357. https://doi.org/10.3390/v17030357
Mester P, Keller D, Kunst C, Schmid S, Krautbauer S, Müller M, Buechler C, Pavel V. Elevated Serum Presepsin Identifies Herpes Simplex Virus-1 Reactivation in COVID-19 Patients. Viruses. 2025; 17(3):357. https://doi.org/10.3390/v17030357
Chicago/Turabian StyleMester, Patricia, Dennis Keller, Claudia Kunst, Stephan Schmid, Sabrina Krautbauer, Martina Müller, Christa Buechler, and Vlad Pavel. 2025. "Elevated Serum Presepsin Identifies Herpes Simplex Virus-1 Reactivation in COVID-19 Patients" Viruses 17, no. 3: 357. https://doi.org/10.3390/v17030357
APA StyleMester, P., Keller, D., Kunst, C., Schmid, S., Krautbauer, S., Müller, M., Buechler, C., & Pavel, V. (2025). Elevated Serum Presepsin Identifies Herpes Simplex Virus-1 Reactivation in COVID-19 Patients. Viruses, 17(3), 357. https://doi.org/10.3390/v17030357