Two Distinct Clinical Courses of Human Cowpox, Germany, 2015


Abstract
:1. Introduction
2. Case Reports
2.1. Case 1
2.2. Case 2
3. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Essbauer, S.; Pfeffer, M.; Meyer, H. Zoonotic poxviruses. Vet. Microbiol. 2010, 140, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Fassbender, P.; Zange, S.; Ibrahim, S.; Zoeller, G.; Herbstreit, F.; Meyer, H. Generalized Cowpox Virus Infection in a Patient with HIV, Germany, 2012. Emerg. Infect. Dis. 2016, 22, 553–555. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, A.; Pauli, G. Sporadic human cases of cowpox in Germany. Eurosurveillance 2007, 12, E070419. [Google Scholar] [CrossRef] [PubMed]
- Coras, B.; Eßbauer, S.; Pfeffer, M.; Meyer, H.; Schröder, J.; Stolz, W.; Landthaler, M.; Vogt, T. Cowpox and a cat. Lancet 2005, 365, 446. [Google Scholar] [CrossRef]
- Campe, H.; Zimmermann, P.; Glos, K.; Bayer, M.; Bergemann, H.; Dreweck, C.; Graf, P.; Weber, B.K.; Meyer, H.; Büttner, M.; et al. Cowpox virus transmission from pet rats to humans, Germany. Emerg. Infect. Dis. 2009, 15, 777–780. [Google Scholar] [CrossRef] [PubMed]
- Eis-Hubinger, A.M.; Gerritzen, A.; Schneweis, K.E.; Pfeiff, B.; Pullmann, H.; Mayr, A.; Czerny, C.P. Fatal cowpox-like virus infection transmitted by cat. Lancet 1990, 336, 880. [Google Scholar] [CrossRef]
- Miernik, B.; Casetti, F.; Panning, M.; Huzly, D.; Meyer, H.; Technau-Hafsi, K. Multilocular facial necrosis in a young boy: A quiz. Acta Derm. Venereol. 2017, 97, 299–301. [Google Scholar] [CrossRef] [PubMed]
- Olson, V.A.; Laue, T.; Laker, M.T.; Babkin, I.V.; Drosten, C.; Shchelkunov, S.N.; Niedrig, M.; Damon, I.K.; Meyer, H. Real-time PCR system for detection of orthopoxviruses and simultaneous identification of smallpox virus. J. Clin. Microbiol. 2004, 42, 1940–1946. [Google Scholar] [CrossRef] [PubMed]
- Franke, A.; Pfaff, F.; Jenckel, M.; Hoffmann, B.; Höper, D.; Antwerpen, M.; Meyer, H.; Beer, M.; Hoffmann, D. Classification of Cowpox Viruses into Several Distinct Clades and Identification of a Novel Lineage. Viruses 2017, 9, 142. [Google Scholar] [CrossRef] [PubMed]
- Ninove, L.; Domart, Y.; Vervel, C.; Voinot, C.; Salez, N.; Raoult, D.; Meyer, H.; Capek, I.; Zandotti, C.; Charrel, R.N. Cowpox virus transmission from pet rats to humans. Emerg. Infect. Dis. 2009, 15, 871–874. [Google Scholar] [CrossRef] [PubMed]
- Haase, O.; Moser, A.; Rose, C.; Kurth, A.; Zillikens, D.; Schmidt, E. Generalized cowpox infection in a patient with Darier disease. Br. J. Dermatol. 2011, 164, 1116–1118. [Google Scholar] [CrossRef] [PubMed]
- Blackford, S.; Roberts, D.L.; Thomas, P.D. Cowpox infection causing a generalized eruption in a patient with atopic dermatitis. Br. J. Dermatol. 1993, 129, 628–629. [Google Scholar] [CrossRef] [PubMed]
- Pelkonen, P.M.; Tarvainen, K.; Hynninen, A.; Kallio, E.R.; Henttonen, H.; Palva, A.; Vaheri, A.; Vapalahti, O. Cowpox with severe generalized eruption, Finland. Emerg. Infect. Dis. 2003, 9, 1458–1461. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Day | Figure | Clinic, Diagnostic Findings |
|---|---|---|
| Day 0 | Small pustule retroauricular on the right side | |
| Day 6 | Pustule, lymphadenitis, local application of cortisone | |
| Day 10 | Figure 1a | Round ulceration with sharp margin (ca. 10 × 10 mm) and surrounding erythema and edema, painful swelling, lymphadenitis, abscess suspected, hospitalization |
| Day 11 | Skin swab: Growth of normal bacterial skin flora | |
| Day 12 | Skin swab: Positive for Orthopoxvirus (OPV) DNA, anti-OPV-titer 80, virus isolation positive | |
| Day 13 | Figure 1b | Round to ovoid ulceration with central necrosis and surrounding erythema and edema |
| Day 20 | Figure 1c | Ulceration turns into an eschar with still inflamed surrounding skin (ca. 50 × 35 mm) |
| Day 21 | Discharge from hospital | |
| Day 30 | Figure 1d | Eschar at its maximum extend measuring ca. 60 × 40 mm with deep necrosis and prominent swelling of the margin of the wound |
| Day 37 | Anti-OPV-titer 640 | |
| Day 47 | Figure 1e | Eschar remodels into hyperkeratotic necrotic tissue and starts to flake off, surrounding erythema is progressive, anti-OPV-titer 320 |
| Day 77 | Anti-OPV-titer 320 | |
| Day 83 | Eschar falls off, biopsy of eschar: OPV-PCR-positive, virus isolation negative | |
| Day 84 | Figure 1f | After flaking of the eschar a ca. 50 × 35 mm necrosis remains with incipient granulation of the wound and fibrin coating |
| Day 89 | Figure 1g | Secondary wound healing with advanced granulation and fibrin coating, skin swab OPV-PCR-positive |
| Day 106 | Anti-OPV-titer 320 | |
| Day 110 | Ending of sick leave | |
| Day 210 | Figure 1h | Scar formation, remaining hyperpigmentation of the formerly inflamed surrounding tissue, anti-OPV-titer 160 |
| Day 326 | Figure 1i | A 60 mm long cicatrix remains |
| Day | Figure | Clinic, Diagnostic Findings |
|---|---|---|
| Day 0 | Pustule on the forehead | |
| Day 6 | Painful swelling, lymphadenitis | |
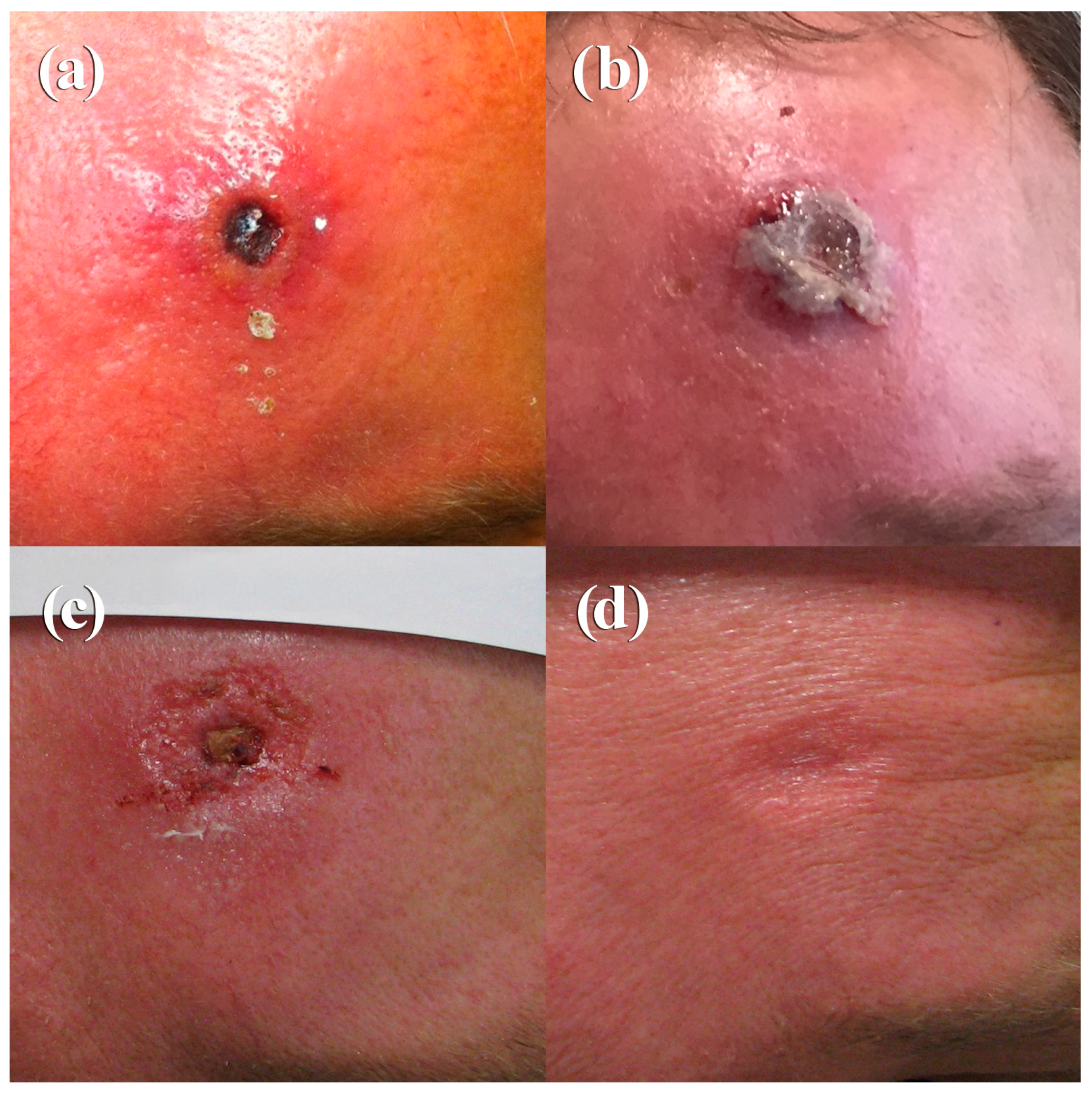
| Day 10 | Figure 2a | Circular ulcerated wound with sharp margins and deep-seated eschar (ca. 10 × 10 mm) surrounded by erythema and edema Skin swab: Growth of normal bacterial skin flora Skin swab: Positive for OPV DNA, virus isolation positive Anti-OPV-titer 1280 |
| Day 12 | Figure 2b | ca. 12 × 12 mm eschar on still inflamed surrounding skin |
| Day 32 | Figure 2c | Regressive redness and swelling of the skin, flaking of the eschar, still incrusted wound base with granulation in the surrounding tissue, Anti-OPV-titer 2560 |
| Day 41 | Figure 2d | Wound covered with epithelial tissue after secondary wound healing |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eder, I.; Vollmar, P.; Pfeffer, M.; Naether, P.; Rodloff, A.C.; Meyer, H. Two Distinct Clinical Courses of Human Cowpox, Germany, 2015. Viruses 2017, 9, 375. https://doi.org/10.3390/v9120375
Eder I, Vollmar P, Pfeffer M, Naether P, Rodloff AC, Meyer H. Two Distinct Clinical Courses of Human Cowpox, Germany, 2015. Viruses. 2017; 9(12):375. https://doi.org/10.3390/v9120375
Chicago/Turabian StyleEder, Ines, Patrick Vollmar, Martin Pfeffer, Philipp Naether, Arne Christian Rodloff, and Hermann Meyer. 2017. "Two Distinct Clinical Courses of Human Cowpox, Germany, 2015" Viruses 9, no. 12: 375. https://doi.org/10.3390/v9120375
APA StyleEder, I., Vollmar, P., Pfeffer, M., Naether, P., Rodloff, A. C., & Meyer, H. (2017). Two Distinct Clinical Courses of Human Cowpox, Germany, 2015. Viruses, 9(12), 375. https://doi.org/10.3390/v9120375