
Interventional Treatment of Malignant Biliary Obstruction: Is It Time to Change the Paradigm?

 , ,
, ,  , , ,
, , ,  ,
,
Abstract
1. Introduction
- Endoscopic retrograde cholangiopancreatography (ERCP). Since the initial description of the technique by McCune et al. in 1968, ERCP has gradually evolved and been established as the first-line treatment of obstructive jaundice, particularly in benign indications or in the setting of unresectable malignancy [8]. Achieving high success (90–95%) and low adverse event (AE) (5.18–9.8%) rates, while preserving the anatomy and physiology of the gastrointestinal tract, its value in the management of a broad spectrum of biliary disorders is enormous [9]. Even in expert hands, however, in about 3–10% of the patients, drainage through ERCP is impossible due to a number of factors, including an inaccessible or grossly infiltrated papilla, failure to cannulate, altered anatomy, etc. Additionally, post-ERCP pancreatitis (PEP) remains a source of grave concern. Despite the introduction of various techniques to reduce its incidence (guidewire cannulation, rectal nonsteroid anti-inflammatory drugs, prophylactic pancreatic stenting), PEP occurs in about 10% of all procedures and in up to 30% in high-risk patients [10].
- Percutaneous transhepatic biliary drainage (PTBD). The development of PTBD techniques is largely parallel to the development of ERCP. Its adoption has been slightly slower compared to ERCP (first ultrasound-guided percutaneous cholangiography performed by Makuuchi in 1977 [11]). However, for decades, PTBD was considered the only viable alternative to ERCP and even a first-choice modality in the setting of complex hilar obstruction. While being acceptably effective in terms of technical and clinical success, of 90–100% and 77–98%, respectively, percutaneous biliary intervention’s main disadvantage is the potential for AEs ranging between 8–30% in most studies, but up to 62% according to more recent large observational studies [12,13]. There is an uptrend in the incidence of AEs associated with PTBD, which probably reflects certain aspects of the patient selection process. Other factors that are worth considering include the persistent need for external drainage catheters, which worsen patients’ quality of life, impair normal intestinal absorption and integrity, and lead to loss of fluid and electrolytes.
- Endoscopic ultrasound-guided biliary drainage (EUS-BD). Initially described by Giovannini et al. in the form of endoscopic ultrasound-guided choledochoduodenostomy (EUS-CDS) in 2001 and hepaticogastrostomy (HGS) in 2003, EUS-BD emerged as a viable alternative to conventional endoscopic and percutaneous drainage procedures [14,15]. While initially performed only in high-volume expert centers, the gradual increase in expertise and development of new devices and stents led to broader adoption of the technique. In 2022 and 2023 European Society of Gastrointestinal Endoscopy (ESGE) and Society of Gastrointestinal endoscopy of India (SGEI) published guidelines on the application of EUS for biliopancreatic drainage [16,17]. These guidelines outline EUS-BD as a first-choice alternative to ERCP, mainly in the setting of malignant biliary obstruction. Multiple studies, however, comparing the clinical outcomes of primary EUS-BD to ERCP state that EUS-BD has noninferior clinical and technical success rate and fewer AEs (PEP in particular) [18,19,20]. Additionally, EUS-BD has certain theoretical advantages over ERCP in terms of lower stent occlusion rate [18]. Those results raise the question of whether EUS-BD could be regarded as primary therapeutic modality at least in selected patients with anticipated difficult transpapillary biliary access.
2. Aim
3. Ethics
4. Materials and Methods
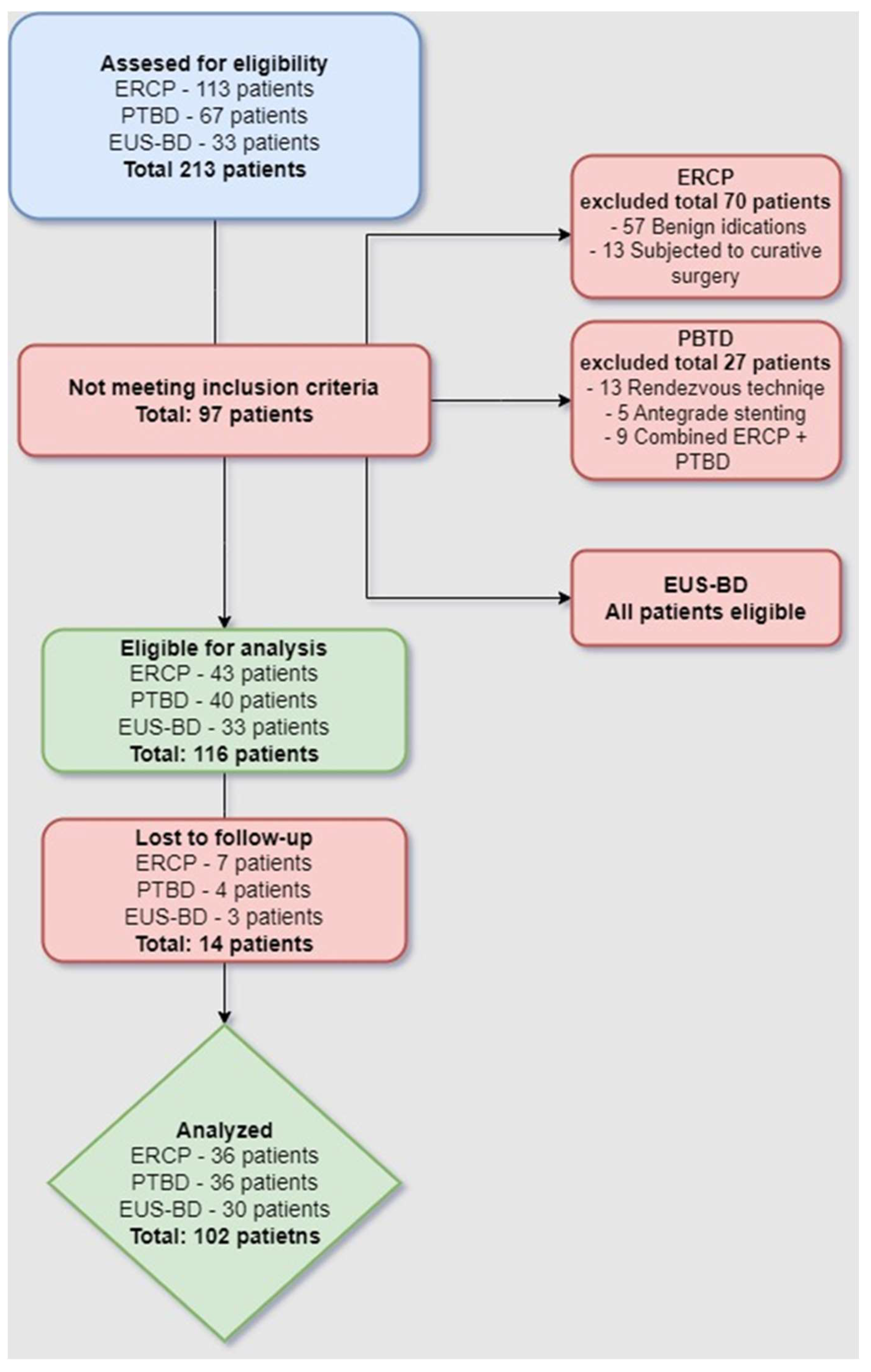
4.1. Patient Selection
- Inclusion criteria.
- -
- Age ≥ 18 years
- -
- Histologically confirmed biliopancreatic malignancy inducing obstructive jaundice.
- -
- Imaging data (computer tomography (CT), magnetic resonance cholangiopancreatography (MRCP), or EUS) suggestive of nonresectability (locally advanced or metastatic disease) or poor general condition precluding major surgery.
- -
- Interventional treatment by means of ERCP, EUS-BD, or PTBD was considered the chief inclusion criteria.
- -
- Follow-up of at least 6 months post-procedure or until death.
- -
- Competence to give informed consent.
- Exclusion criteria.
- -
- Benign etiology of biliary obstruction.
- -
- Patients subjected to subsequent surgery with curative intent.
- -
- Modifications of the percutaneous biliary interventions including antegrade stenting, rendezvous technique, hybrid techniques (ERCP + PTBD), etc.
- -
- Patients lost to follow-up.
- -
- Refusal to participate in the study.
4.2. Methods
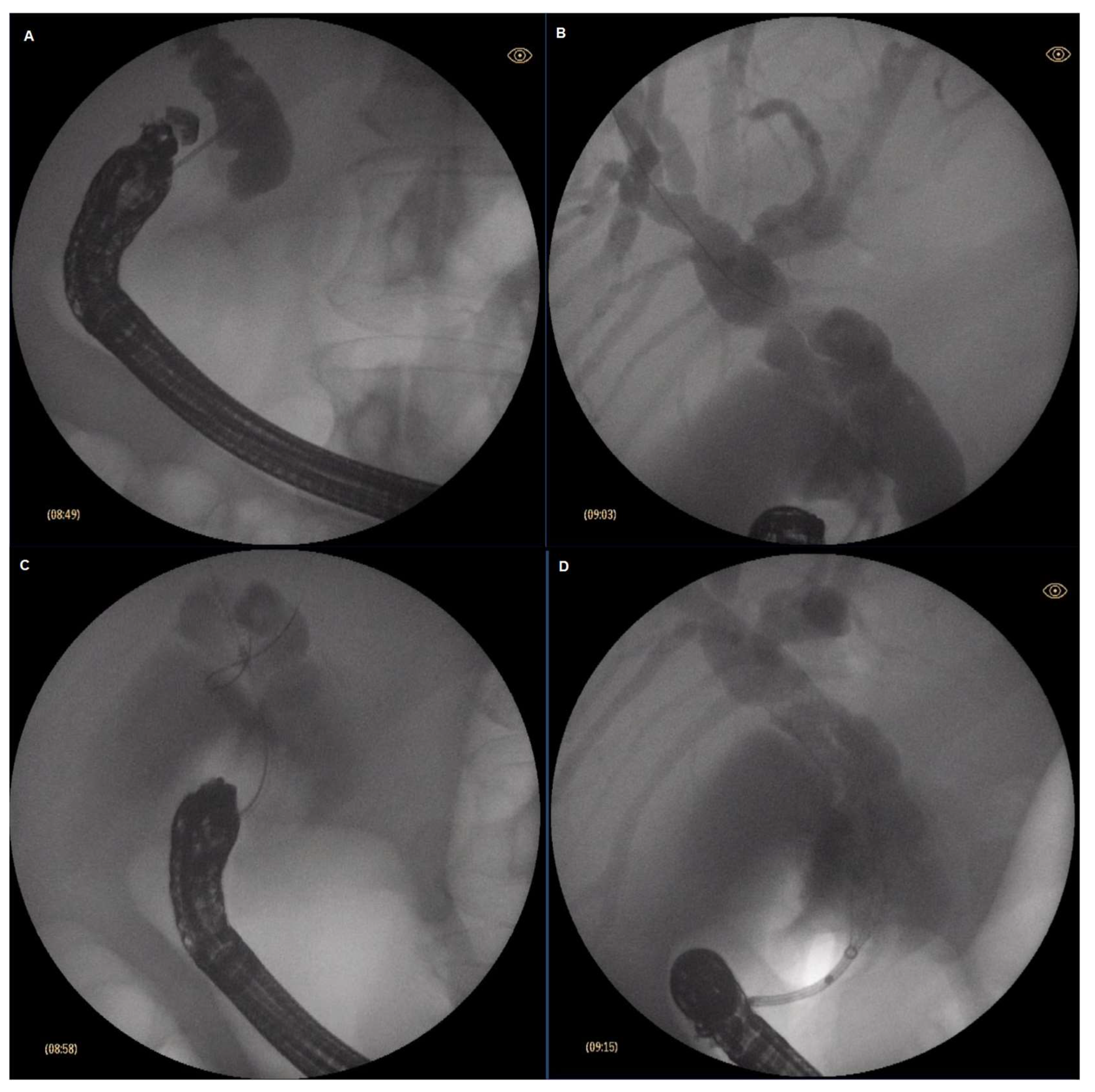
4.2.1. ERCP
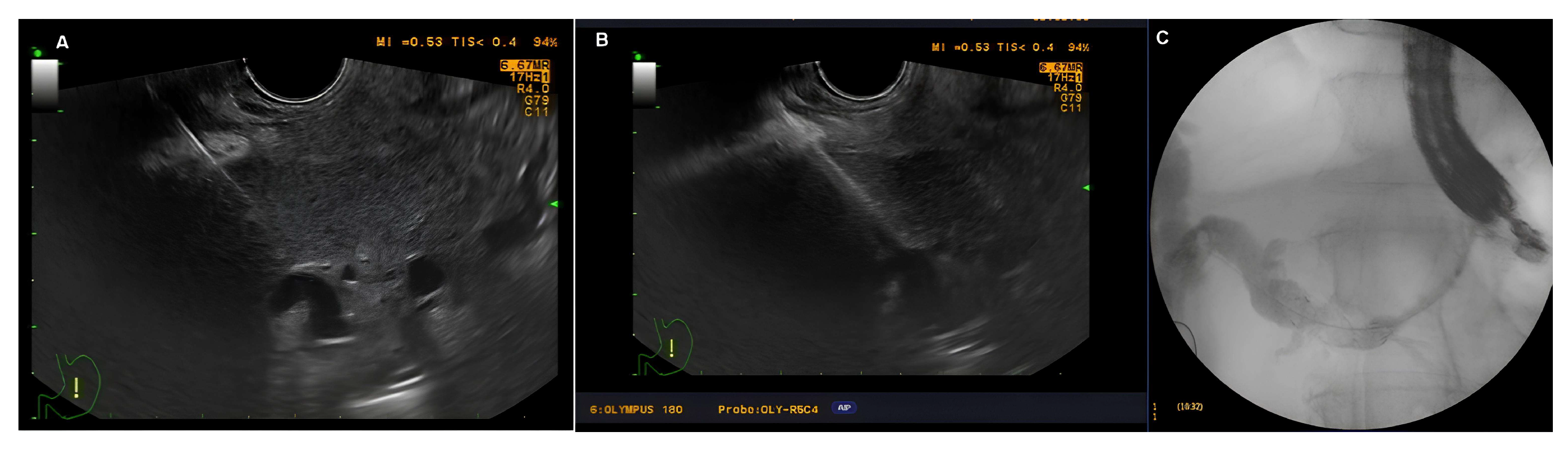
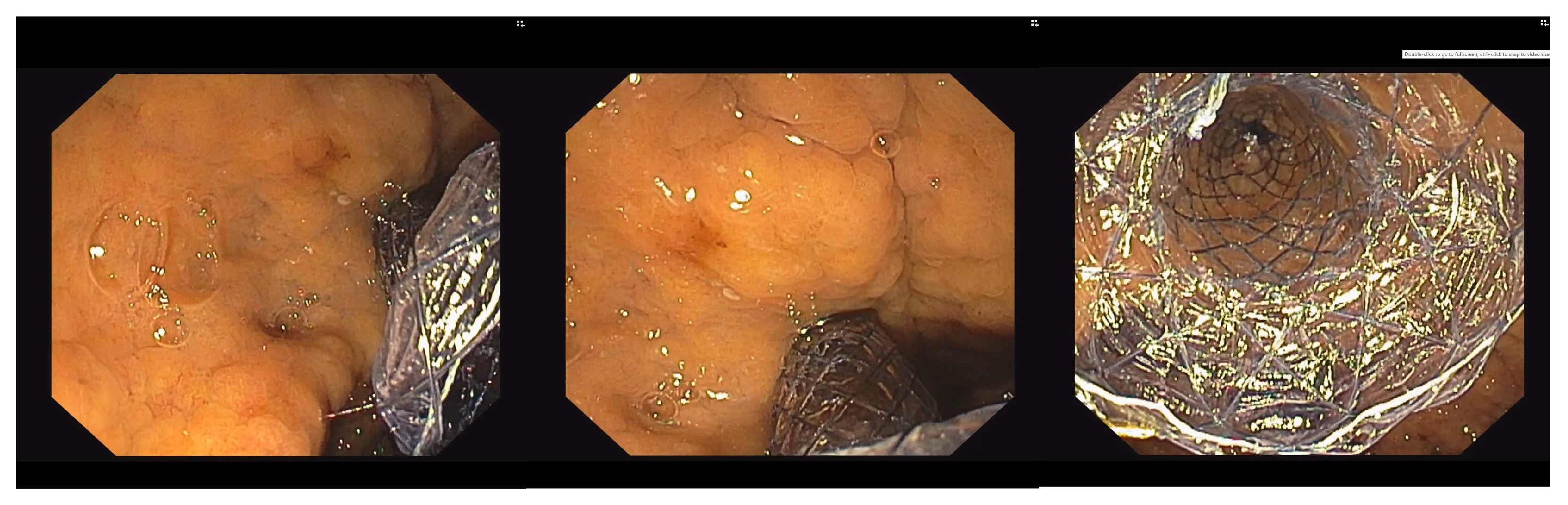
4.2.2. EUS-BD
4.2.3. EUS-CDS
4.2.4. EUS-HGS
4.2.5. PTBD
4.3. Statistical Methods
5. Results
5.1. Background and Clinical Data
5.2. Technical and Clinical Success Rate
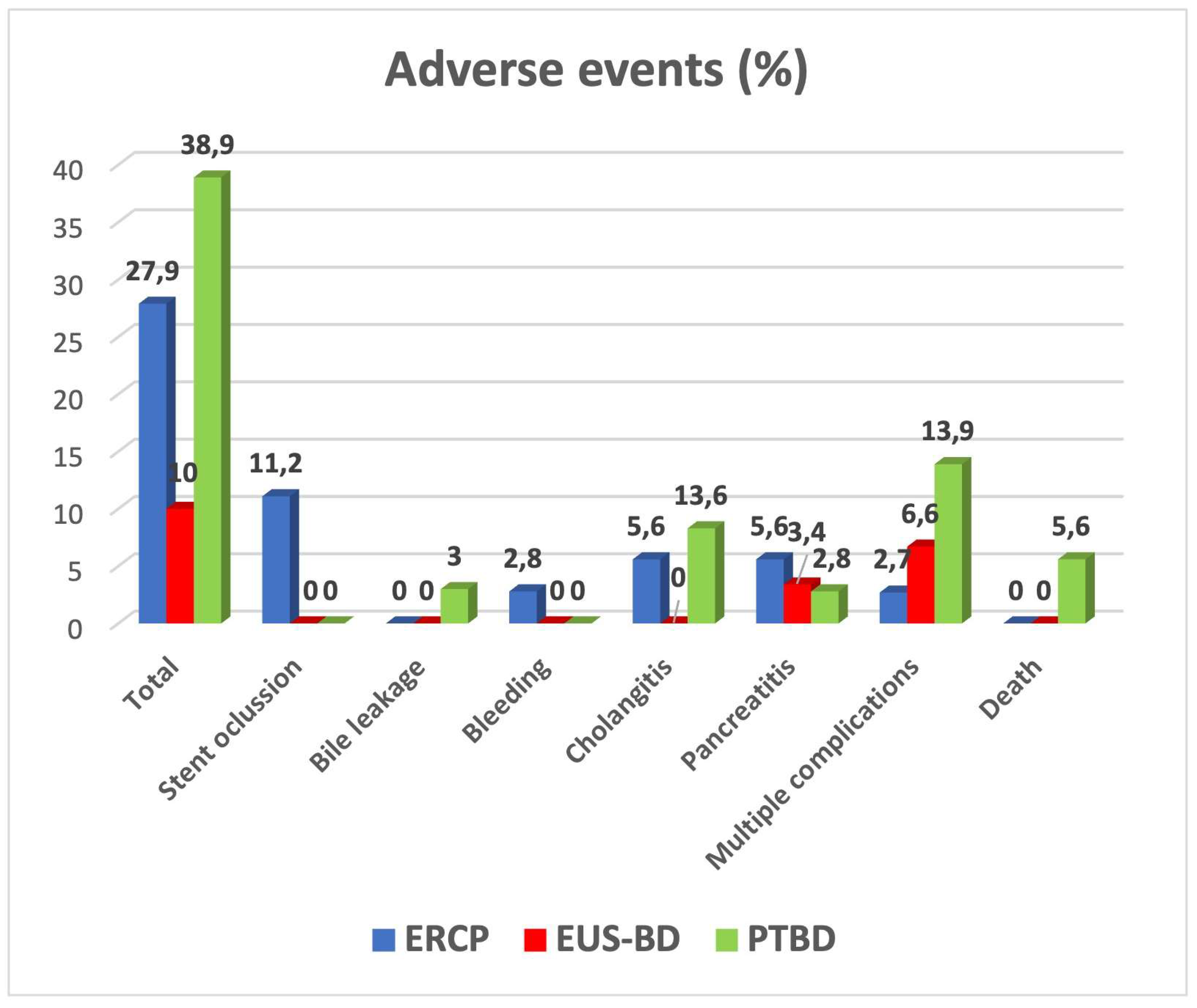
5.3. Adverse Events
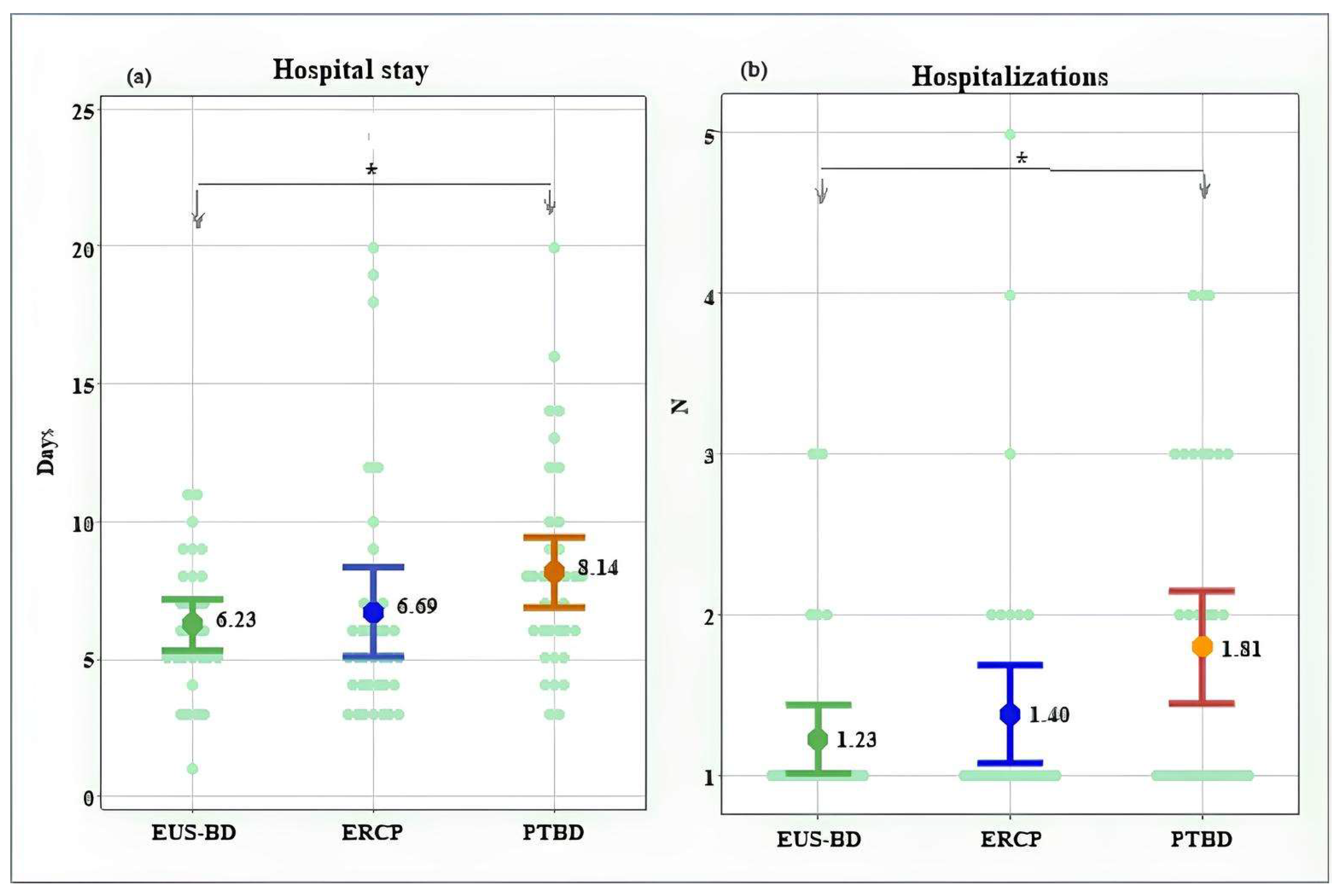
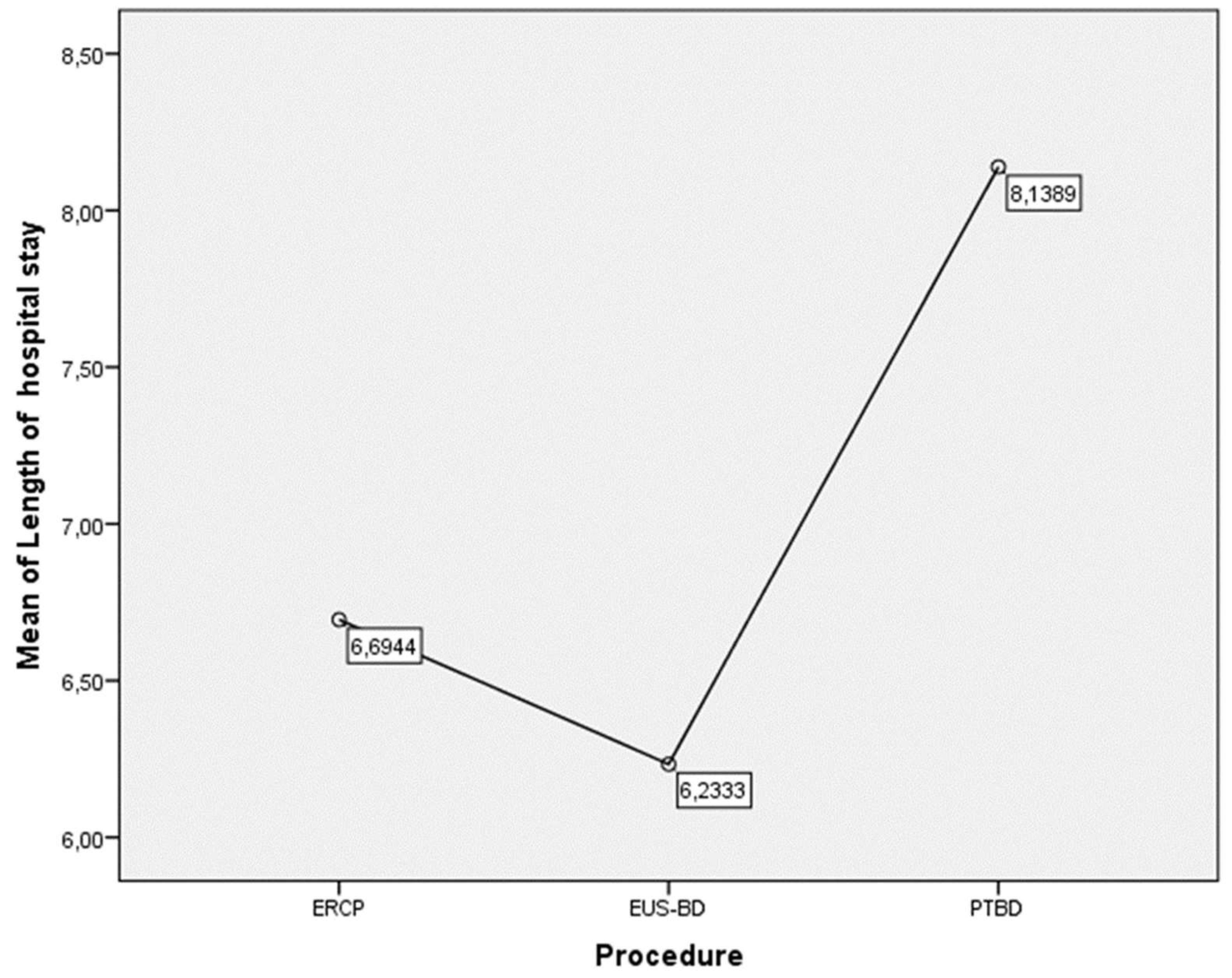
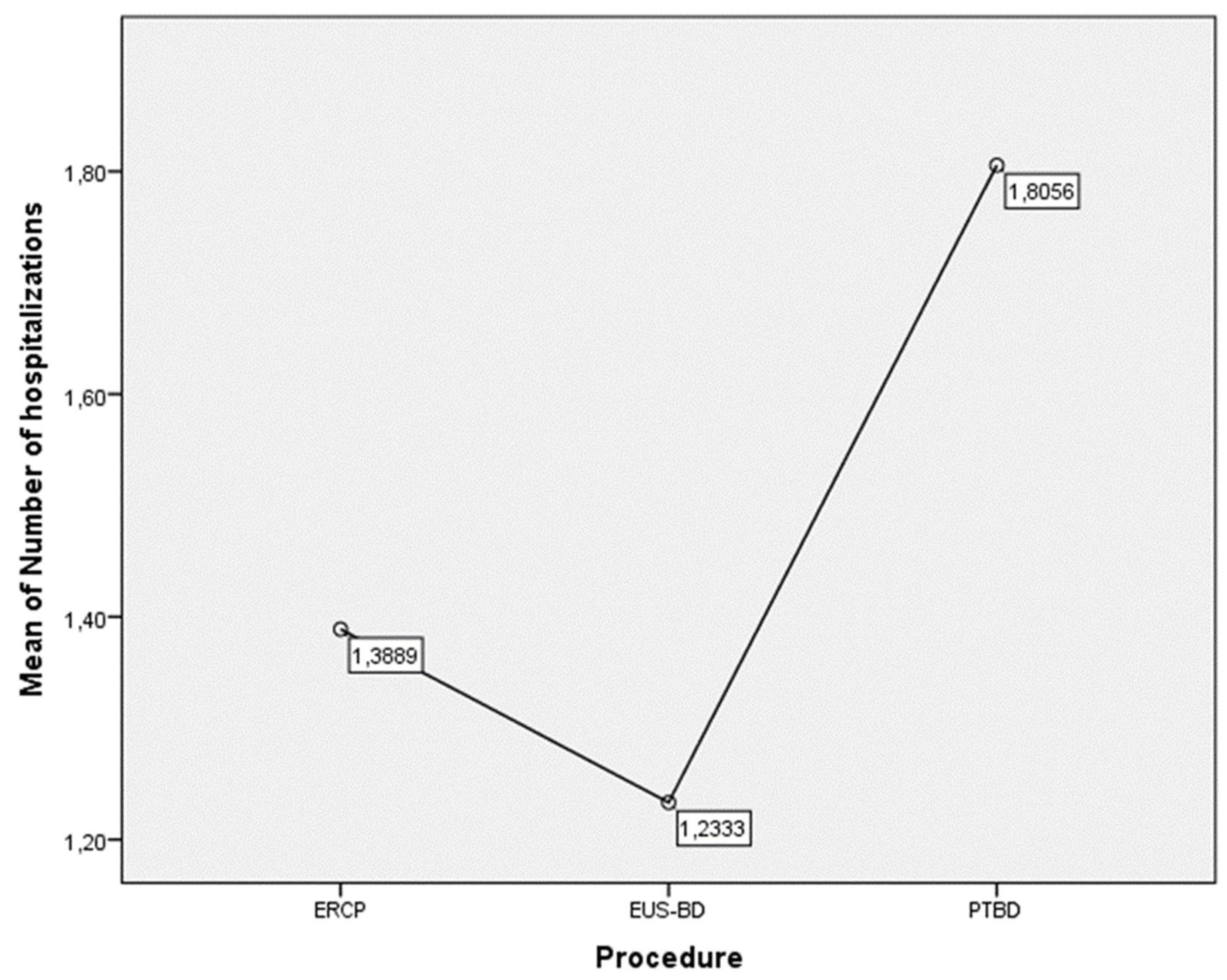
5.4. Length of Hospital Stay and Number of Hospitalizations
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AE | Adverse event |
| ASGE | American Society of Gastrointestinal Endoscopy |
| CT | Computer tomography |
| CECT | Contrast-enhanced computer tomography |
| ECOG | Eastern Cooperative Oncology Group |
| ERCP | Endoscopic retrograde cholangiopancreatography |
| ESGE | European Society of Gastrointestinal Endoscopy |
| EUS | Endoscopic ultrasonography |
| EUS-BD | Endoscopic ultrasound-guided biliary drainage |
| EUS-CDS | Endoscopic ultrasound-guided choledochoduodenostomy |
| EUS-HGS | Endoscopic ultrasound-guided hepaticogastrostomy |
| FC-SEMS | Fully covered self-expandable metal stent |
| FNA | Fine needle aspiration |
| HGS-SEMS | Hepatico-gastrostomy SEMS |
| ICU | Intensive care unit |
| MBO | Malignant biliary obstruction |
| MRCP | Magnetic resonance cholangiopancreatography |
| PBI | Percutaneous biliary interventions |
| PEP | Post-ERCP pancreatitis |
| PS | Performance status |
| PTBD | Percutaneous transhepatic biliary drainage |
| SEMS | Self-expandable metal stent |
| SGEI | Society of Gastrointestinal Endoscopy of India |
| US | Ultrasound |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | ECOG Performance Status |
|---|---|
| 0 | Fully active, able to carry on all predisease performance without restriction. |
| 1 | Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, e.g., light house work, office work. |
| 2 | Ambulatory and capable of all selfcare but unable to carry out any work activities; up and about more than 50% of waking hours. |
| 3 | Capable of only limited selfcare; confined to bed or chair more than 50% of waking hours. |
| 4 | Completely disabled; cannot carry on any selfcare; totally confined to bed or chair. |
| 5 | Dead. |
| Grade | Definition of Grades | Modes of Therapy |
|---|---|---|
| Grade I | Any deviation from the normal postoperative course. | No pharmacological or surgical treatment, endoscopic, or radiological interventions were required. Acceptable therapeutic regimens are drugs such as antiemetics, antipyretics, analgesics, diuretics, electrolytes, and physiotherapy. Wound infections or small abscess requiring incision at bedside are within this category. |
| Grade II | Normal course altered. | Pharmacological management other than Grade I. Blood transfusions and total parenteral nutrition are also included. |
| Grade III | Complications that require intervention of various degrees. | Grade IIIa—complications that require an intervention performed under local anesthesia. |
| Grade IIIb—interventions that require general or epidural anesthesia. | ||
| Grade IV | Complications threatening life of patients (including CNS complications), requiring ICU support. | Grade IVa—single organ dysfunction (including dialysis). |
| Grade IVb—multiorgan dysfunction. | ||
| Grade V | Death of patient. |
| Type I | Tumor involves the common hepatic duct below the confluence of the left and right hepatic ducts. |
| Type II | Tumor involves the confluence of the left and right hepatic ducts. |
| Type IIIa | Tumor involves the confluence and right hepatic duct. |
| Type IIIb | Tumor involves the confluence and left hepatic duct. |
| Type IVa | Tumor involves the confluence and both left and right hepatic duct. |
| Type IVb | Multicentric tumors. |
| 1 |
|
| 2 |
|
| 3 |
|
| 4 |
|
References
- Björnsson, E.; Gustafsson, J.; Borkman, J.; Kilander, A. Fate of patients with obstructive jaundice. J. Hosp. Med. 2008, 3, 117–123. [Google Scholar] [CrossRef]
- Carriaga, M.T.; Henson, D.E. Liver, gallbladder, extrahepatic bile ducts, and pancreas. Cancer 1995, 75, 171–190. [Google Scholar] [CrossRef]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef]
- Parasher, G.; Lee, J.G. The role of ERCP in pancreato-biliary malignancies. Adv. Dig. Endosc. ERCP 2006, 6, 120–141. [Google Scholar]
- Ho, C.S.; E Warkentin, A. Evidence-Based Decompression in Malignant Biliary Obstruction. Korean J. Radiol. 2012, 13 (Suppl. 1), S56–S61. [Google Scholar] [CrossRef]
- Distler, M.; Kersting, S.; Rückert, F.; Dobrowolski, F.; Miehlke, S.; Grützmann, R.; Saeger, H.-D. Palliative treatment of obstructive jaundice in patients with carcinoma of the pancreatic head or distal biliary tree. Endoscopic stent placement vs. hepaticojejunostomy. J. Pancreas 2010, 11, 568–574. [Google Scholar] [CrossRef]
- Soares, K.C.; Kamel, I.; Cosgrove, D.P.; Herman, J.M.; Pawlik, T.M. Hilar cholangiocarcinoma: Diagnosis, treatment options, and management. Hepatobiliary Surg. Nutr. 2014, 3, 18–34. [Google Scholar]
- McCune, W.S. ERCP at thirty years: An interview with Dr. William S. McCune (1909–1998). Gastrointest. Endosc. 1998, 48, 643–644. [Google Scholar] [CrossRef]
- Szary, N.M.; Al-Kawas, F.H. Complications of endoscopic retrograde cholangiopancreatography: How to avoid and manage them. Gastroenterol. Hepatol. 2013, 9, 496–504. [Google Scholar]
- Ribeiro, I.B.; Junior, E.S.D.M.; Neto, A.A.M.; Proença, I.M.; de Moura, D.T.H.; Minata, M.K.; Ide, E.; dos Santos, M.E.L.; Luz, G.d.O.; Matuguma, S.E.; et al. Pancreatitis after endoscopic retrograde cholangiopancreatography: A narrative review. World J. Gastroenterol. 2021, 27, 2495–2506. [Google Scholar] [CrossRef]
- Makuuchi, M.; Beppu, T.; Kamiya, K.; Futagawa, S.; Sugiura, M.; Wada, T.; Muroi, T. Echo guide percutaneous transhepatic cholangiography. Jpn. J. Surg. 1977, 8, 165–175. [Google Scholar] [CrossRef]
- Van Delden, O.M.; Laméris, J.S. Percutaneous drainage and stenting for palliation of malignant bile duct obstruction. Eur. Radiol. 2007, 18, 448–456. [Google Scholar] [CrossRef]
- Turan, A.S.; Jenniskens, S.; Martens, J.M.; Rutten, M.J.C.M.; Yo, L.S.F.; van Strijen, M.J.L.; Drenth, J.P.H.; Siersema, P.D.; van Geenen, E.J.M. Complications of percutaneous transhepatic cholangiography and biliary drainage, a multicenter observational study. Abdom. Radiol. 2022, 47, 3338–3344. [Google Scholar] [CrossRef]
- Giovannini, M.; Moutardier, V.; Pesenti, C.; Bories, E.; Lelong, B.; Delpero, J. Endoscopic Ultrasound-Guided Bilioduodenal Anastomosis: A New Technique for Biliary Drainage. Endoscopy 2001, 33, 898–900. [Google Scholar] [CrossRef]
- Giovannini, M.; Dotti, M.; Bories, E.; Moutardier, V.; Pesenti, C.; Danisi, C.; Delpero, J. Hepaticogastrostomy by Echo-Endoscopy as a Palliative Treatment in a Patient with Metastatic Biliary Obstruction. Endoscopy 2003, 35, 1076–1078. [Google Scholar] [CrossRef]
- van der Merwe, S.W.; van Wanrooij, R.L.J.; Bronswijk, M.; Everett, S.; Lakhtakia, S.; Rimbas, M.; Hucl, T.; Kunda, R. Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2022, 54, 185–205. [Google Scholar] [CrossRef]
- Rai, P.; Udawat, P.; Chowdhary, S.D.; Gunjan, D.; Samanta, J.; Bhatia, V.; Club, I.E. Society of Gastrointestinal Endoscopy of India Consensus Guidelines on Endoscopic Ultrasound-Guided Biliary Drainage: Part I (Indications, Outcomes, Comparative Evaluations, Training). J. Digest. Endosc. 2023, 14, 30–40. [Google Scholar] [CrossRef]
- Tanikawa, T.; Ishii, K.; Katsumata, R.; Urata, N.; Nishino, K.; Suehiro, M.; Kawanaka, M.; Haruma, K.; Kawamoto, H. Efficacy of primary drainage by endoscopic ultrasound-guided biliary drainage for unresectable pancreatic adenocarcinoma. JGH Open 2022, 6, 251–256. [Google Scholar] [CrossRef]
- Paik, W.H.; Lee, T.H.; Park, D.H.; Choi, J.-H.; Kim, S.-O.; Jang, S.; Kim, D.U. EUS-Guided Biliary Drainage Versus ERCP for the Primary Palliation of Malignant Biliary Obstruction: A Multicenter Randomized Clinical Trial. Am. J. Gastroenterol. 2018, 113, 987–997, Erratum in Am. J. Gastroenterol. 2018, 113, 1566. [Google Scholar] [CrossRef]
- Han, S.Y.; Kim, S.-O.; So, H.; Shin, E.; Kim, D.U.; Park, D.H. EUS-guided biliary drainage versus ERCP for first-line palliation of malignant distal biliary obstruction: A systematic review and meta-analysis. Sci. Rep. 2019, 9, 16551. [Google Scholar] [CrossRef]
- Dumonceau, J.M.; Tringali, A.; Papanikolaou, I.S.; Blero, D.; Mangiavillano, B.; Schmidt, A.; van Hooft, J.E. Endoscopic biliary Stenting: Indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline—Updated October 2017. Endoscopy 2018, 50, 910–930. [Google Scholar] [CrossRef]
- Demir, T.; Ustaoglu, M. Evaluation of the success and complication rates of endoscopic retrograde cholangiography according to the difficulty of the procedure. Precis. Med. Sci. 2023, 12, 4–9. [Google Scholar] [CrossRef]
- Wang, K.; Zhu, J.; Xing, L.; Wang, Y.; Jin, Z.; Li, Z. Assessment of efficacy and safety of EUS-guided biliary drainage: A systematic review. Gastrointest. Endosc. 2016, 83, 1218–1227. [Google Scholar] [CrossRef]
- Zerem, E.; Imširović, B.; Kunosić, S.; Zerem, D.; Zerem, O. Percutaneous biliary drainage for obstructive jaundice in patients with inoperable, malignant biliary obstruction. Clin. Exp. Hepatol. 2022, 8, 70–77. [Google Scholar] [CrossRef]
- Anderloni, A.; Fugazza, A.; Troncone, E.; Auriemma, F.; Carrara, S.; Semeraro, R.; Maselli, R.; Di Leo, M.; D’Amico, F.; Sethi, A.; et al. Single-stage EUS-guided choledochoduodenostomy using a lumen-apposing metal stent for malignant distal biliary obstruction. Gastrointest. Endosc. 2018, 89, 69–76. [Google Scholar] [CrossRef]
- Cotton, P.B.; Eisen, G.; Romagnuolo, J.; Vargo, J.; Baron, T.; Tarnasky, P.; Petersen, B. Grading the complexity of endoscopic procedures: Results of an ASGE working party. Gastrointest. Endosc. 2011, 73, 868–874. [Google Scholar] [CrossRef]












| Variables | ERCP (n = 36) | PTBD (n = 36) | EUS-BD (n = 30) | p-Value |
|---|---|---|---|---|
| Age (years) | ||||
| 65.58 10.04 33–82 | 64.94 12.31 46–86 | 67.83 11.18 46–87 | 0.577 A |
| Sex N (%) | ||||
| 20 (55.60%) a 16 (44.40%) | 29 (80.60%) b 7 (19.40%) | 17 (56.70%) a 13(43.30%) | 0.047 χ2 |
| Prior interventions N (%) | ||||
| 1 (2.80%) a 35 (97.20%) | 23 (63.90%) b 13 (36.10%) | 15 (50.00%) b 15 (50.00%) | <0.001 χ2 |
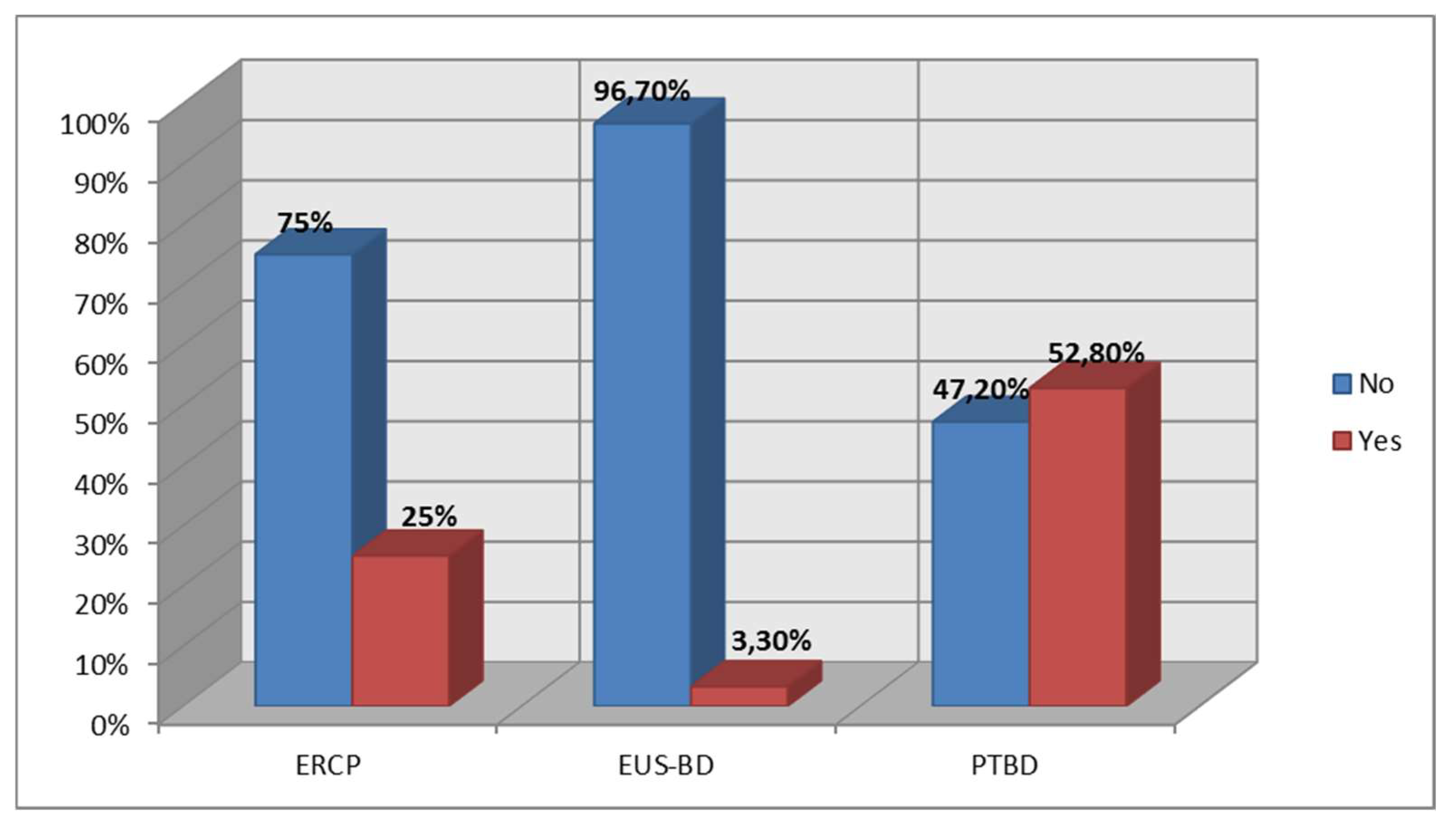
| Reinterventions N (%) | ||||
| 10 (27.80%) a 26 (72.20%) | 19 (52.80%) b 17(47.20%) | 1 (3.30%) c 29 (96.70%) | <0.001 χ2 |
| Etiology N (%) | ||||
| 19 (52.80%) a 5 (13.90%) a 4 (11.10%) 2 (5.60%) 5 (13.90%) 1 (2.80%) | 8 (22.20%) b 15 (41.70%) b 4 (11.10%) 1 (2.80%) 7 (19.40%) 1 (2.80%) | 13 (43.30%) a,b 7 (23.30%) a,b 6 (20.00%) 0 (0.00%) 3 (10.00%) 1 (3.40% | 0.014 f 0.017 f n.s. n.s. n.s. n.s. |
| Level of stenosis N (%) | ||||
| 7 (19.40%) 2 (5.60%) 0 (0.00%) a 3 (8.30%) 24 (66.70) a | 10 (27.80%) 6 (16.70%) 7 (19.40%) b 4 (11.10%) 9 (25.00%) b | 7 (23.30%) 1 (3.30%) 2 (6.70%) a,b 5 (16.70%) 15 (50.00%) a | n.s. n.s. 0.010 f n.s. 0.010 χ2 |
| Performance status N (%) | ||||
| 1 (2.80%) a 14 (38.90%) a 16 (44.40%) a 5 (13.90%) a | 1 (2.80%) a 11 (30.60%) a 8 (50.00%) a 6 (16.70%) a | 8 (26.70%) b 5 (16.70%) b 20 (43.30%) a 4 (13.30%) a | 0.017 χ2 |
| Type of stent N (%) | ||||
| 2 (5.60%) a 12 (33.30%) a 22 (61.10%) a 0 (0.00%) a 0 (0.00%) a 0 (0.00%) a | 0 (0.00%) b 0 (0.00%) b 0 (0.00%) a 0 (0.00%) a 35(97.20%) b 1(2.80%) a | 0 (0.00%) b 0 (0.00%) b 9 (30.00%) b 18(60.00%) b 0 (0.00%) a 3 (10.00%) a | <0.00 χ2 |
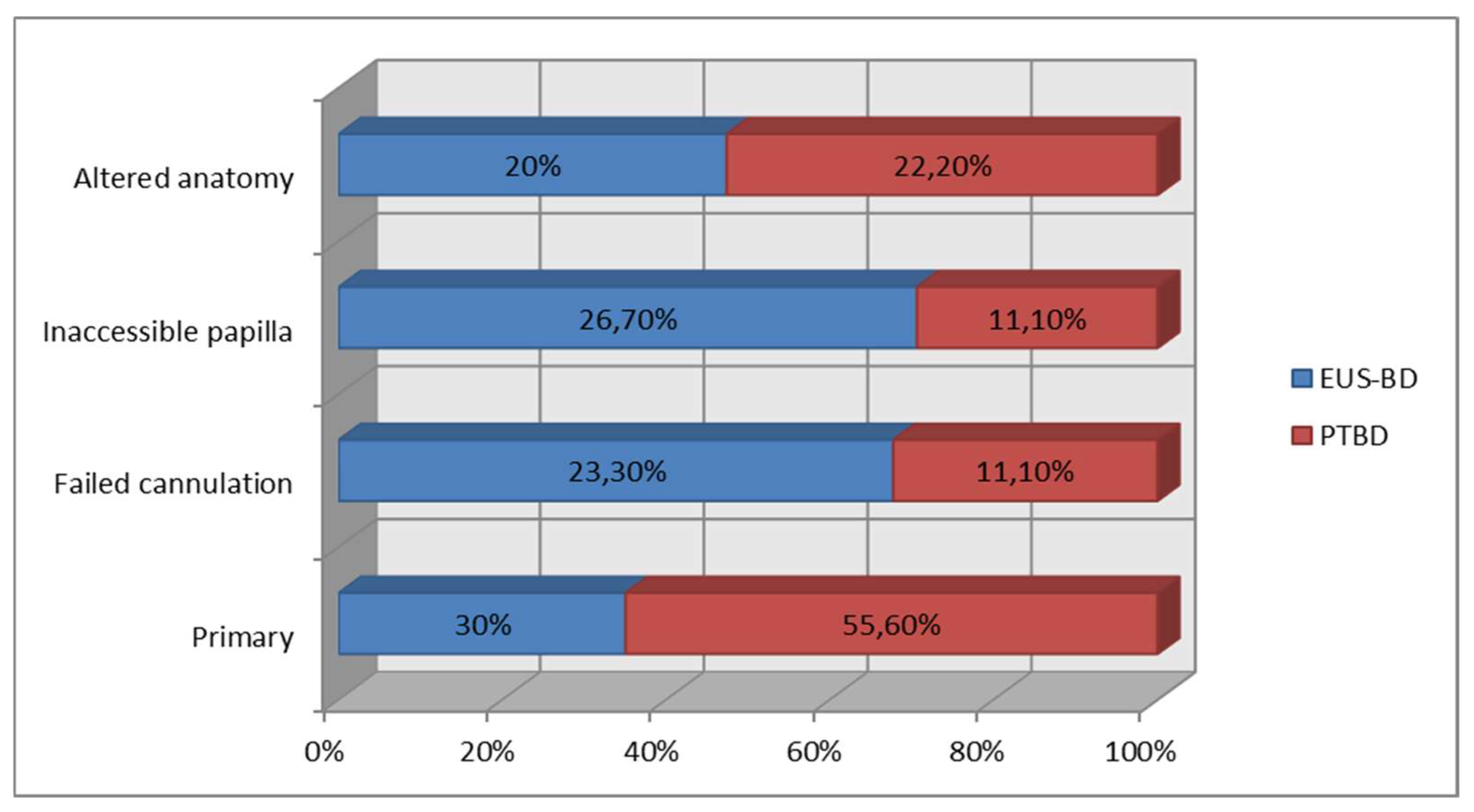
| Decision for PTBD/EUS-BD N (%) | ||||
| na | 4 (11.10%) 4 (11.10%) 20 (55.60%) a 8 (22.20%) | 7 (23.30%) 8 (26.70%) 9 (30.00%) b 6 (20.00%) | n.s. n.s. 0.048 f n.s. |
| Grade | Total No/% of All AEs | ERCP No/% of All AEs | PTBD No/% of All AEs | EUS-BD No/% of All AEs |
|---|---|---|---|---|
| 1 | 0/0% | 0/0% | 0/0% | 0/0% |
| 2 | 1/4.2% | 0/0% | 0/0% | 1/33.3% |
| 3 | 18/75% | 7/87.5% | 10/76.9% | 1/33.3% |
| 4 | 3/12.5% | 1/12.5% | 1/7.7% | 1/33.3% |
| 5 | 2/8.3% | 0/0% | 2/15.40% | 0/0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hristov, B.; Doykov, D.; Andonov, V.; Doykov, M.; Kraev, K.; Uchikov, P.; Dimov, R.; Kostov, G.; Valova, S.; Doykova, K.; et al. Interventional Treatment of Malignant Biliary Obstruction: Is It Time to Change the Paradigm? Gastroenterol. Insights 2024, 15, 266-284. https://doi.org/10.3390/gastroent15020020
Hristov B, Doykov D, Andonov V, Doykov M, Kraev K, Uchikov P, Dimov R, Kostov G, Valova S, Doykova K, et al. Interventional Treatment of Malignant Biliary Obstruction: Is It Time to Change the Paradigm? Gastroenterology Insights. 2024; 15(2):266-284. https://doi.org/10.3390/gastroent15020020
Chicago/Turabian StyleHristov, Bozhidar, Daniel Doykov, Vladimir Andonov, Mladen Doykov, Krasimir Kraev, Petar Uchikov, Rosen Dimov, Gancho Kostov, Siyana Valova, Katya Doykova, and et al. 2024. "Interventional Treatment of Malignant Biliary Obstruction: Is It Time to Change the Paradigm?" Gastroenterology Insights 15, no. 2: 266-284. https://doi.org/10.3390/gastroent15020020
APA StyleHristov, B., Doykov, D., Andonov, V., Doykov, M., Kraev, K., Uchikov, P., Dimov, R., Kostov, G., Valova, S., Doykova, K., Chakarov, D., & Sandeva, M. (2024). Interventional Treatment of Malignant Biliary Obstruction: Is It Time to Change the Paradigm? Gastroenterology Insights, 15(2), 266-284. https://doi.org/10.3390/gastroent15020020