Abstract
Background: The involvement of the inferior vena cava in advanced abdominal tumors is a surgical challenge, given the high postoperative morbidity and poor long-term prognosis. Our goal was to analyze our experience, perioperative management, and results. Methods: We retrospectively evaluated short and long-term results of surgical resections of tumors with associated inferior vena cava resection performed in our facilities between 2012 and 2023. Results: A total of 25 patients were selected for our retrospective study: 3 with renal carcinoma, 5 with sarcoma, 12 with metastatic lesions, 2 with adrenal tumors, 1 pancreatic tumor, 1 extra-adrenal paraganglioma and 1 with hepatocellular carcinoma. Postoperative severe complications (Dindo-Clavien score ≥ IIIa) affected 36% of patients and the mortality rate was 8%. Partial resection with primary repair was performed in 13 patients (52%), with patch reconstruction in 6 (24%), and vascular reconstruction with prosthesis in 6 patients (24%). The mean disease-free survival was 7 months (IQR 2.5–11.5). Graft thrombosis occurred in 2 patients during follow-up. Conclusions: In selected patients, the resection of the inferior vena cava is a complex surgery with an assumable morbimortality and relative survival improvement.
1. Introduction
Clinical conditions requiring resection of the inferior vena cava are somewhat rare. The main indications for this procedure are traumatic or iatrogenic lesions, chronic membrane or post-thrombotic occlusion, and tumors [1,2]. Several series have reported on the safety and satisfactory oncological outcomes of resection for tumors that originate from or infiltrate the inferior vena cava (IVC) [2,3,4,5,6,7,8].
Tumors presenting with involvement of the IVC can either be primary, i.e., originating in the vena cava itself, like leiomyosarcoma, or secondary. The latter can infiltrate the vena cava from the outside or lead to neoplastic thrombosis, which may even reach the right atrium [4]. The main tumors with IVC involvement are renal cell carcinoma, Wilms tumors, leiomyosarcoma, adrenal tumors, hepatocellular tumors, and retroperitoneal lymphatic metastasis of testicular carcinoma [1,2].
Traditionally, the great vessels’ involvement has been considered a sign of advanced stage disease and a contraindication for abdominal tumor resection, given the high surgical risk and poor survival rate [2,9]. However, surgical in bloc resection of the IVC and retroperitoneal tumors with or without a major hepatectomy has been proposed in selected patients to achieve R0 resection [2,6,7]. The development of innovative surgical techniques, such as total hepatic vascular exclusion, veno-venous bypass and ex vivo hepatic resection, and liver transplant has led to a curative surgical approach to tumors involving the IVC [9,10].
The surgical approach to these lesions is a challenge and requires a preoperative evaluation of the patient’s operability, as well as of the tumor’s resectability [4,11]. The type of IVC reconstruction technique varies widely among surgeons and centers [12]. IVC reconstruction is not always required due to the gradual occlusion of the vena that allows for the formation of collateral veins [1,11]. However, in the absence of preoperative obstruction or when collateral pathways have to be sacrificed during tumor excision, IVC ligation may be not tolerated [11].
The objectives of this study were to record our experience in the resection of tumors with IVC involvement, evaluate the morbidity and mortality rates of the procedure, and analyze the types of reconstruction performed and the results obtained.
2. Materials and Methods
The work has been reported in line with the PROCESS criteria [13]. The study was approved by the Ethical Committee of our center (Number Id: 16102022).
2.1. Study Population
We retrospectively looked at patients who, from January 2012 to January 2023, underwent surgical procedures in our unit for IVC-specific tumors or for IVC resections due to secondary infiltrative tumors. In some cases, the IVC involvement was an intraoperative finding.
Patients with primary or secondary IVC involvement who underwent surgery were included in our study. Exclusion criteria were the presence of extrahepatic or peritoneal disease metastases found during surgical exploration in patients with colorectal metastases, or the presence of distant or peritoneal metastases in other patients.
In patients with known preoperative secondary IVC involvement, surgical intervention was considered for localized disease requiring limited vena cava resection to achieve complete resection of the disease. This option was not considered in cases with more extensive or circumferential involvement of >50% on diagnostic tests.
An additional analysis was made taking account two groups: primary IVC involvement and secondary disease (in our study, all patients had colorectal liver metastases).
2.2. Data Collection
Diagnostic management included establishment of a medical history, performance of clinical examination and imaging tests, including an abdominal ultrasound and computerized tomography (CT) scan to confirm the tumor origin and growth, as well as infiltration, if any, of adjacent structures. Positron emission tomography (PET) CT scan and abdominal magnetic resonance imaging (MRI) were additionally used for diagnosis. In cases with known IVC involvement preoperatively, an angio-CT and vascular reconstruction were performed to assess the level of involvement, as well as the extent and development of collateral circulation or not. These imaging tests also allowed us to rule out distant metastases, and to assess resectability and the option for vascular reconstruction (Figure 1). In some cases, the decision to resect the IVC was made during surgery, because IVC involvement was an intraoperative finding, which had remained unknown up to that point. Preoperative investigations included complete blood and liver function test as well as routine anesthetic and cardiorespiratory evaluation. In the preoperative planning phase, an electrocardiogram was conducted for all patients. In cases where inferior vena cava resection was already known to be necessary, a transthoracic echocardiogram was performed.
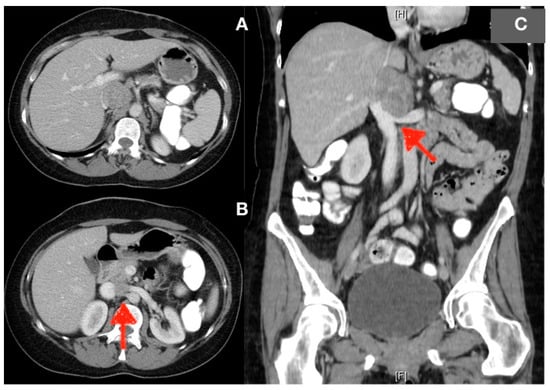
Figure 1.
(A) CT image showing a lesion within the inferior vena cava with displacement of the hepatic hilum. (B) Axial section: opening of the left renal vein into the inferior vena cava (red arrow) is interrupted. (C) Coronal section: showing broad contact (red arrow) of the mass with the left renal vein without interrupting flow. The images correspond to patient number 12. As can be observed in the image, the lesion is identified in the region below the supra-hepatic veins. In this patient, a circumferential resection of the inferior vena cava was performed with replacement with a Goretex prosthesis. The patient exhibited no postoperative complications.
In patients with a history of prior deep venous thrombosis or pulmonary embolism, a lower extremity venous duplex ultrasound examination was conducted. Patients were evaluated by a multidisciplinary team. According to the histologic type, specific neoadjuvant treatments were administered.
The variables taken into account were age, sex, BMI, the American Society of Anesthesiologists’ (ASA) classification, tumor type, preoperative chemotherapy and/or radiation therapy. In addition, another variable considered was whether the finding was intraoperative or preoperative. Perioperative clinical results, surgical approach, type of IVC resection and reconstruction, and intraoperative complications were recorded. Details of the postoperative course were collected. Some of the key short-term data recorded included length of hospital stay, complications’ ranking (according to the Dindo–Clavien classification [14], ‘severe complication’ is defined as greater or equal to IIIa), re-operation, re-admission and operative mortality (<90 days after operation). Some of the key long-term data recorded were patency of IVC or prosthesis (as determined by a CT scan), neoadjuvant and adjuvant chemotherapy, specific disease-free survival (DFS) and overall survival (OS).
2.3. Surgical Approach
Usually, we make a midline or oblique incision to expose the infrarenal and perirenal IVC. When the tumor extends laterally, a flank incision curves toward the midline. Management of IVC involvement was categorized in three groups, according to the surgical repair necessary: resection with primary repair, resection with autologous or prosthetic patch repair, and circumferential resection with graft replacement. Primary repair was defined as resection of a portion of the IVC with primary closure when <50% narrowing of the lumen would result. Patch closure was planned when a larger defect created by the resection required patch repair to avoid narrowing of the IVC. Circumferential resection or involvement > 50% of the circumference of IVC was managed with replacement using a prosthetic graft (Figure 2) [7]; the graft size chosen is usually smaller than the IVC (typically 12–16 mm) [1,15].
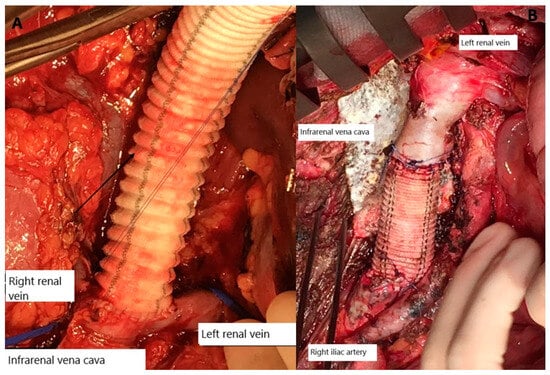
Figure 2.
(A) Intraoperative image corresponding to the case of Figure 1 showing the replacement of the inferior vena cava with synthetic prosthesis, including left renal vein opening. (B) Intraoperative image corresponding to patient no. 7. Infrarenal vena cava reconstruction with prosthesis.
For surgical planning, we used the classification according to Kulayat, which subdivides the IVC into three segments: upper portion (level 1)—extending from the opening of the hepatic veins up to the right atrium, middle portion (level 2)—extending from the renal veins to the hepatic veins, and lower portion (level 3)—extending from the junction of the iliac veins to the opening of the renal veins [16].
The approach to vena cava resection depended on the extent and location of tumor involvement. In tumors involving level 3, total vascular exclusion is performed. When the IVC involvement is below level 2, vascular control is performed below the hepatic veins. In patients with known IVC involvement preoperatively, veno-venous bypass is prepared, but only used if the patient presents hemodynamic instability during occlusion of the IVC. The decision was made on the basis of the extent and location of tumor involvement.
Intravenous heparin is not used during the clamping time of the IVC. Heparinized saline (2 units/mL of heparin sodium) is used, however, to flush out the prosthesis if used for reconstruction. A therapeutic heparin dose is used for 30 days after surgery, and patients with prosthesis receive oral blood thinners for at least six months.
2.4. Follow-Up
Patient follow-up included measuring tumor markers and performing a chest–abdominal CT scan every three months for the first two years, then twice a year, and then annually after five years. Local recurrence was defined as a return of a tumor within the surgical field, whereas systemic recurrence was defined as recurrent disease outside said field. The use of a contrast agent during CT scans allowed us to assess vascular or prosthetic permeability. Anticoagulation is maintained after six months in selected patients with a history of deep win thrombosis or evidence of partial caval thrombosis.
2.5. Statistical Analysis
Continuous variables were expressed as mean ± SD or median (interquartile range), and categorical variables were expressed by frequencies or percentage. The Kaplan–Meier method was used to evaluate the patient’s survival. The Statistical Package for the Social Sciences (SPSS, release 22.0 for Windows) was used for all analyses.
3. Results
Twenty-five IVC resection cases evaluated. The surgical technique of choice was thrombectomy + cavoplasty in 3 cases (12%), partial resection + primary closure in 11 cases (44%), partial resection + patch reconstruction in 5 cases (20%), and circular IVC resection and reconstruction with prosthesis in the remaining cases; specifically, 5 were made out of polyester (Hemagard®,- Intervascular SAS, La Ciotat Cedex, France) and the fifth was made out of polytetrafluoroethylene (PTFE, Gore-tex®- Gore & Associates, Inc., Newark, DE, USA). During surgery, 11 (44%) patients required extended resection, including other organs (radical nephrectomy was performed in 7 cases, pancreaticoduodenectomy in 3 cases and there was 1 total pancreatectomy). No patient required an external cardiovascular pump.
Out of 25 patients, 13 were male and 12 were female. The average age was 59.5 (±13.4 SD) years. Basal features of patients are recorded in Table 1.

Table 1.
Main patients’ characteristics.
Tumor classification per origin was as follows: 3 cases of renal cell carcinoma, 5 cases of sarcoma (2 were dedifferentiated retroperitoneal liposarcoma, 1 duodenal GIST, 1 renal leiomyosarcoma and the other a primary vena cava leiomyosarcoma), 9 cases of hepatic metastasis of colorectal tumors, 1 case of adrenal gland metastasis of hepatocellular carcinoma, 2 cases of adrenal carcinoma, 1 case of adrenal metastasis of lung cancer, 1 case of pancreatic metastasis of ovarian cancer, 1 case of extra-adrenal paraganglioma, 1 case of pancreatic tumor and 1 case of hepatocellular carcinoma.
Most of the patients did not have a previous history of narrowing or involvement of the venous return, with edema or ascites; only one patient presented with lower extremity edema.
Preoperative imaging tests of 18 of the patients (72%) showed IVC involvement either due to tumor infiltration or thrombosis. In the remaining patients, the need for IVC resection was determined during surgery to achieve complete resection of the tumor.
Eighteen (18) patients (72%) experienced postoperative complications. Nine (9) patients (36%) experienced major complications (Dindo–Clavien ≥ IIIa). Two (2) patients (8%) died during the immediate post-operation due to multiple organ failure, hemodynamic instability or acute re-thrombosis of the IVC. The average hospital stay was 10 days (IQR 7–17).
Thirteen (13) patients (52%) received neoadjuvant treatment. All of them were stable and/or their diseases responded to treatment before surgery.
Excluding those patients deceased during the immediate post-operation, the average follow-up was 26 (IQR 13–62) months. No patient was lost during follow-up. The 1-, 3- and 5-year OS rates were 95%, 66% and 45%, respectively, excluding postoperative mortality. The mean DFS was 10 months (range, 4.024–15.98). The 1-, 3- and 5-year DFS rates were 41%, 21% and 21%, respectively.
When we analyze subgroups, the 1-, 3- and 5-year OS rates were 91%, 68% and 41% in primary IVC involvement and 83%, 54% and 42% in secondary disease (p = 0.980). (Figure 3). The 1-year DFS rate was 33% in primary IVC involvement and the 1-, 3- and 5-year DFS rates were 50%, 38% and 38% in secondary disease (p = 0.09).
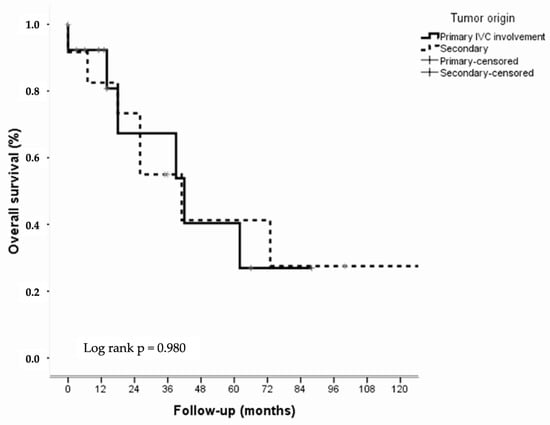
Figure 3.
Overall survival of the primary and secondary IVC involvement groups.
Two patients experienced thrombosis after surgery, one during the immediate post-op and the other during the follow-up phase, due to local recurrence. Twelve patients were prescribed follow-up anticoagulation.
4. Discussion
Tumors with IVC involvement may originate in the inferior vena cava itself or be secondary to other tumor invasion [4,8]. Liver tumors involving the IVC generally have poor oncological outcomes [17]. Among IVC primary tumors, the most common is the leiomyosarcoma, a rare tumor representing about 2% of soft tissue sarcomas [4]. Secondary tumors happen because of the growth, either outside or within the IVC, of retroperitoneal, soft-tissue tumors, or even hepatic tumors (hepatocellular carcinoma, cholangiocarcinoma, or liver metastases). Another possibility is the formation of a tumoral thrombus within the IVC, originating in the renal or pararenal veins due to a secondary tumor [4,18]. In our cohort, the most common origin was colorectal metastasis (36%). Classically, patients with CRLM involving the IVC were not considered as surgical candidates. Primary IVC leiomyosarcoma was uncommon, represented only by a single case (4%). These tumors involving the IVC have limited options for treatment with chemotherapy or interventional radiology. Despite advances in chemotherapy, resection of these advanced tumors remains the only potentially curative therapy, with studies reporting 5-year survival rates of up to 50%. Survival without surgery is typically less than 1 year [2,5,11].
Previously, IVC involvement was regarded as a contraindication for resection. However, significant advances, coupled with the development of existing liver transplantation surgical techniques, have broadened the technical scope for vascular exclusion procedures, safe resection and reconstruction.
As these procedural limitations are overcome, the pool of eligible patients has expanded, rendering liver resection in patients with IVC involvement an increasingly common surgical procedure [12].
Long-term survival is the most important parameter for assessing the oncological outcome of malignant tumors. Given that there is no effective alternative treatment for these patients and that the 5-year OS of palliative chemotherapy for CRLM is 2.2% [7,8], our results are acceptable.
Most tumors with IVC involvement are typically asymptomatic or present with unspecific symptoms, such as abdominal distension or palpable mass. Occlusion or thrombosis of the IVC secondary to tumor involvement is rare. In most instances, there is partial occlusion from a combination of tumor involvement and compression [3,7]. Patients presenting with lower extremity edema more often have deep venous thrombosis (DVT). Whether completely or partially occluded, lower extremity edema on presentation is seen in ≤30% of patients because the slow-growing nature of most of these malignancies enables the development of collateral venous drainage [3,7]. In our cohort, only one patient presented with a preoperative clinical history of lower extremity edema, abdominal distension, or ascites.
In recent years, the number of published reports has been increasing, but there are still many aspects of the surgery which require further discussion, since most published studies are isolated clinical cases or in small cohorts with a short follow-up interval [8].
The majority of studies encompass IVC resections for various tumor types and evaluate the outcomes collectively. Consequently, it is not feasible to derive reliable outcomes for the subgroup of patients with liver metastases from colorectal cancer.
Surgical resection of locally advanced tumors with IVC involvement is the only curative or palliative treatment available to treat the symptoms. Meticulous preoperative planning to include the degree of vascular resection required is essential, especially if a venous bypass is needed. The type of reconstruction to be performed also needs to be included in this planning. So far, the procedure is not performed frequently due to its inherent high risk and to the fact that most patients requiring it are at an advanced stage of the disease with distant metastases [8]. Surgical management of tumors with IVC involvement is a challenge and requires extensive expertise in vascular and retroperitoneal surgery, as well as proper perioperative management and postoperative support in the ICU [4]. The type of IVC resection performed will depend on the localization and extension of the lesion [3,6].
The hemodynamic repercussion of IVC clamping will depend on the extent of the procedure itself, and the amount and effectiveness of collaterals established through the azygos system [19].
When retro-hepatic cava resection is necessary, supra-hepatic IVC control and the Pringle maneuver allows for the resection and reconstruction of the retro-hepatic cava [7]. Complete vascular exclusion allows us to perform the upper anastomosis of the prosthesis near the supra-hepatic veins so that hepatic circulation can be reestablished quickly, thus reducing hepatic ischemia time [1]. For surgical management of tumors involving the adrenal segment of the IVC, veno-venous bypass with or without selective hypothermic hepatic perfusion is sometimes used instead of aortic cross-clamping by other groups to maintain hemodynamic stability [1,20,21]. High complication rates, as well as increased operative times and warm ischemia, have been associated with veno-venous bypass and the need for systematic heparinization, and especially patients with liver disease and coagulation disturbances may experience negative effects [12].
We have not performed this type of procedure because, when venous cross-clamping is performed beneath the supra0hepatic veins and without the Pringle maneuver, the decrease in venous return is well tolerated.
Reconstruction after IVC resection is controversial [2,22]. The slow tumor growth or progressive thrombosis of the IVC promotes the development of collaterals, making obstructive symptoms uncommon and allowing for IVC ligation under the renal veins. IVC ligation could cause lower limb edema in up to 50% of patients, although this is normally well tolerated [2,3,8]. There is still a paucity of literature analyzing the immediate and long-term consequences of patients requiring IVC ligation for the surgical management of various retroperitoneal tumors, which are encountered in surgical oncology practice [23]. Resection of large retroperitoneal tumors, including a segment of the IVC, as well as the performance of a retroperitoneal lymphadenectomy in indicated cases has the potential to alter the collateral venous flow [3].
Even in patients with IVC involvement over the renal veins, if the preoperative renal function is preserved, IVC ligation without reconstruction is a possibility. Although the right kidney is typically resected, the left kidney can more often be preserved, since part of its venous drainage happens through collateral vessels (gonadal, lumbar, and adrenal veins) [2,8,9]. Despite the aforementioned, the current trend leans towards reconstruction whenever possible, which is why we have not had any cases of IVC ligation without reconstruction. Long-term venous effects, such as kidney failure and severe lower limb edema, are impossible to predict based on preoperative venous signs, symptoms, and imaging tests [3,9,11]. Estimated incidence rates for lymphedema range from 2 to 16% for IVC-reconstruction and 14 to 60% for IVC ligation [23]. Interestingly, the reported need for postoperative dialysis after IVC ligation is approximately 3.5%, with several case series reporting no need for it [23].
Currently, multiple materials for reconstruction are available, including autologous materials, such as saphenous vein graft or peritoneum allografts, such as aortic homo-grafts, and xenografts, such as bovine pericardium [8,22]. However, in the last decade, graft synthetic mesh reconstruction (including Dacron and PTFE) has become a progressively better and more available option [8]. Only 2% of cases have reported graft-related complications, and the procedure has excellent patency [8].
Medical literature suggests having the prosthesis slightly narrower than the segment of IVC being replaced, in order to increase the flow rate. Some authors even recommend an arteriovenous fistula (AVF) to increase the flow rate and improve graft permeability [8,24]. Other authors, however, consider it unnecessary if the adrenal or supra-hepatic vena cava is reconstructed, given the high blood flow at that level [8]. Long-term complications secondary to the use of an AVF, such as congestive heart failure and edema, have been reported. These, however, are rare and typically occur only after a long period of time [8]. The fistula eliminates the need for long-term anticoagulation therapy [1]. At our center, we have never had to use this method, since the blood flow of all patients was considered sufficient.
Limited data are available on the use of biological grafts for the reconstruction of the IVC. It has lower risks of infection and thrombosis when compared with synthetic materials, and does not require long-term anticoagulation [22,25]. In our cohort, in six cases an autologous patch was used (all from falciform ligament, except one from parietal peritoneum) for IVC reconstruction. Primary autologous repair can be performed if <50% narrowing of the IVC lumen will result [7]. The peritoneal patch used for reconstruction could be harvested from three different sites: the falciform ligament, the pre-renal peritoneum or the right part of the diaphragm [15]. The type of prosthesis used was PTFE or Dracon. During vascular reconstruction, heparinized saline is used to fill the prosthesis and prevent local thrombosis during the procedure.
Intraoperative systemic anticoagulation is not used routinely and should be avoided, particularly for large tumor resections. No studies address this topic in the literature. The presence of thrombi (of non-tumoral origin), a history of lower extremity DVT or pulmonary embolism are considered indications to use systemic heparin during resection (intravenous) [7]. None of our patients had to receive this.
Reported postoperative mortality rate is 0–25% and morbidity ranges are around 18–50% [24]. At our center, we observed these rates to be similar to those reported by the literature, with the severe complication rate at 36% and the postoperative mortality rate at 8%. Although postoperative morbidity is high, which is similar to the figures reported in other series, this complication rate is to be expected, given the technical complexity of the surgery.
An aggressive approach to the management of these patients with advanced abdominal tumors may improve their long-term survival rate [2,26]. In the systematic review published by Serradilla et al. (2023), the 5-year overall survival is described as ranging from 0% to 51.9%, with a median of 16–34 months and a disease-free survival of 9–13 months [17].
The 5-year survival rate after curative resection exceeds 50% in renal cell carcinomas (RCC) with IVC involvement; and is also about 50% in primary leiomyosarcomas. However, the DFS is very low and is believed to be under 30% although, in studies with larger cohorts, it does not even reach 10% [27]. The report of Baldrich et al. had a cohort of 47 patients, who underwent resection due to a vena cava leiomyosarcoma with IVC reconstruction. The group’s 5-year survival rate was 45% ± 8.5% [7]. The mean OS rate in our cohort was 41 months (22.23–59.77), which is similar to that reported by other studies, but not directly comparable given the variety of tumors comprising most cohorts, including ours [3].
The subgroup analysis revealed that there was no statistical significance in overall survival rates between patients with primary or secondary tumors, and 1, 3 and 5-year OS rates were 91%, 68% and 41% in primary IVC involvement and 83%, 54% and 42% in secondary disease (p = 0.980).
In Table 2, data from some of the main studies published on IVC resection due to different abdominal tumors are recorded [2,4,8,10].
Table 2.
Data obtained from literature review and presentation of the results of our case series.
While, in the past, adjuvant therapy was considered ineffective, currently, adjuvant chemotherapy and/or radiation therapy are considered a key component of the comprehensive treatment of these patients [7]. New chemotherapeutic drugs have been introduced recently for these types of malignancies. New adjuvant treatments will allow us to better select patients that will benefit from this aggressive surgery and to potentially achieve R0 resection. It is also a powerful screening tool for selecting those patients who are truly going to benefit from this type of aggressive surgical resection [8]. In our cohort, all cases in which this surgery was recommended responded to treatment or achieved radiological stability.
Recent improvements in the imaging techniques, such as PET/CT and MRIs, allow us to better screen for patients who will benefit from this aggressive approach and to rule out those with distant metastases, which may be a contraindication for this type of surgery. Secondly, imaging tests, such as abdominal CT’s with vascular imaging, provide adequate information on vascular invasion and the potential presence of thrombosis and/or vascular abnormalities. These imaging tests are key in the planning of the correct surgical approach, given the complexity of this type of surgery [8], although, occasionally, they fail to identify IVC wall infiltration and the decision to resect is made during the surgery [3,18]. In 72% of our cases, vascular involvement was diagnosed preoperatively.
One of the more serious potential complications is graft infection, which is more frequent when the digestive tract is involved in the resection [22,24]. Therefore, the use of prosthetic materials should be avoided in cases of extensive contamination [24]. The interposition of the omentum between the graft and the resected organs may be beneficial [1,2,5]. The most common complication is graft obstruction, which has been described in 7–28% of cases in the literature [24]. In our cohort, no cases of postoperative infection were reported and two patients developed graft thrombosis in follow-up.
The medical literature also reports cases of permeability after prosthetic reconstructions, with or without anticoagulation, thus there is no clear consensus on its use [1]. There is no preestablished protocol on the use of postoperative anticoagulation in these patients [7,11]. Classically, it was used in those patients with a history of DVT, pulmonary embolism and, in some cases, limb edema due to tumor recurrence [7]. At our center, we prescribe oral anticoagulation to patients with prosthesis or postoperative embolism, initially with low-molecular-weight heparin at therapeutic doses, and then with oral blood thinners for at least six months.
In the series published, in the majority of cases where lymphoedema was present, it improved gradually and was treated conservatively with the use of compression stockings. Previous analyses have reported thromboembolism rates ranging from 0% to 25% for IVC reconstruction [22].
The main limitations of our study are its retrospective nature, the small size of the cohort and its heterogenicity, which does not allow us to reach a conclusion for each type of tumor in terms of survival benefits. In addition, the variety of surgical techniques employed and the lack of cases of simple vena cava ligation without reconstruction prevent us from being able to compare outcomes and reach consistent conclusions on when vascular reconstruction is the best option and what the best approach to it is. This said, we should also mention the study’s strengths: it is a case series with a higher number of patients than most published series, to our knowledge.
5. Conclusions
IVC resection, though a technically demanding procedure, can be safely performed to achieve complete tumor resection with relative survival improvement and acceptable mortality and morbidity rates in selected patients.
The use of prosthetic materials does not necessarily imply permanent anticoagulation.
A multidisciplinary team with oncologists, radiologists, pathologists and surgeons is needed to better define the treatment strategy for these patients.
Author Contributions
Conceptualization, I.J.-T., G.B.-F. and D.L.-G.; methodology, I.J.-T., G.B.-F. and D.L.-G.; formal analysis, I.J.-T., G.B.-F., D.L.-G. and A.R.-H.; investigation, I.J.-T., G.B.-F., A.R.-H. and A.E.G.-M.; resources, I.J.-T., G.B.-F. and D.L.-G.; data curation, I.J.-T., G.B.-F., D.L.-G. and A.R.-H.; writing—original draft preparation, I.J.-T., G.B.-F. and D.L.-G.; writing—review and editing, I.J.-T., G.B.-F., D.L.-G., A.R.-H. and A.E.G.-M.; visualization, I.J.-T., G.B.-F., D.L.-G., A.R.-H. and A.E.G.-M.; supervision, I.J.-T., G.B.-F., D.L.-G., A.R.-H. and A.E.G.-M.; project administration, G.B.-F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of the Hospital Universitario de Badajoz (Number Id: 16102022, approved date: 16 October 2022).
Informed Consent Statement
Patient consent was waived due to the fact that the study was retrospective and observational, and entailed no risk.
Data Availability Statement
All data generated or analysed during this study are included in this published article. The data obtainable by consulting the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Biswas, S.; Amin, A.; Chaudry, S.; Joseph, S. Leiomyosarcoma of the Inferior Vena Cava—Radical Resection, Vascular Reconstruction and Challenges: A Case Report and Review of Relevant Literature. World J. Oncol. 2013, 4, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Hardwigsen, J.; Baqué, P.; Crespy, B.; Moutardier, V.; Delpero, J.R.; Le Treut, Y.P. Resection of the inferior vena cava for neoplasms with or without prosthetic replacement: A 14-patient series. Ann. Surg. 2001, 233, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, D.; Andreani, P.; Maggi, U.; Salloum, C.; Perdigao, F.; Sebagh, M.; Lemoine, A.; Adam, R.; Castaing, D. Combined liver resection and reconstruction of the supra-renal vena cava: The Paul Brousse experience. Ann. Surg. 2006, 244, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Eder, F.; Halloul, Z.; Meyer, F.; Huth, C.; Lippert, H. Surgery of inferior vena cava associated malignant tumor lesions. VASA Z. Gefasskrankh. 2008, 37, 68–80. [Google Scholar] [CrossRef]
- Hemming, A.W.; Mekeel, K.L.; Zendejas, I.; Kim, R.D.; Sicklick, J.K.; Reed, A.I. Resection of the liver and inferior vena cava for hepatic malignancy. J. Am. Coll. Surg. 2013, 217, 115. [Google Scholar] [CrossRef]
- Nuzzo, G.; Giordano, M.; Giuliante, F.; Lopez-Ben, S.; Albiol, M.; Figueras, J. Complex liver resection for hepatic tumours involving the inferior vena cava. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2011, 37, 921–927. [Google Scholar] [CrossRef]
- Quinones-Baldrich, W.J.; Farley, S. Techniques for inferior vena cava resection and reconstruction for retroperitoneal tumor excision. J. Vasc. Surg. Venous Lymphat. Disord. 2013, 1, 84–89. [Google Scholar] [CrossRef]
- Vicente, E.; Quijano, Y.; Ielpo, B.; Duran, H.; Diaz, E.; Fabra, I.; Malave, L.; Ferri, V.; Ferronetti, A.; Caruso, R. Surgical Resection of Malignancies Invading Inferior Vena Cava Level I and II. Issues Still Need to Be Discussed. Anticancer. Res. 2017, 37, 2523–2528. [Google Scholar] [CrossRef][Green Version]
- Vladov, N.N.; Mihaylov, V.I.; Belev, N.V.; Mutafchiiski, V.M.; Takorov, I.R.; Sergeev, S.K.; Odisseeva, E.H. Resection and reconstruction of the inferior vena cava for neoplasms. World J. Gastrointest. Surg. 2012, 4, 96–101. [Google Scholar] [CrossRef]
- Vladov, N.; Kostadinov, R.; Mihaylov, V.; Takorov, I.; Lukanova, T.; Yakova, M.; Trichkov, T.; Odisseeva, E.; Mutafchiyski, V. Single-Centre Experience of Supra-Renal Vena Cava Resection and Reconstruction. World J. Surg. 2021, 45, 2270–2279. [Google Scholar] [CrossRef]
- Papamichail, M.; Marmagkiolis, K.; Pizanias, M.; Koutserimpas, C.; Heaton, N. Safety and Efficacy of Inferior Vena Cava Reconstruction during Hepatic Resection. Scand. J. Surg. SJS Off. Organ Finn. Surg. Soc. Scand. Surg. Soc. 2019, 108, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Baimas-George, M.; Tschuor, C.; Watson, M.; Sulzer, J.; Salibi, P.; Iannitti, D.; Martinie, J.B.; Baker, E.; Clavien, P.A.; Vrochides, D. Current trends in vena cava reconstructive techniques with major liver resection: A systematic review. Langenbeck’s Arch. Surg. 2021, 406, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Agha, R.A.; Borrelli, M.R.; Farwana, R.; Koshy, K.; Fowler, A.J.; Orgill, D.P.; Zhu, H.; Alsawadi, A.; Noureldin, A.; Rao, A.; et al. The PROCESS 2018 statement: Updating Consensus Preferred Reporting of CasE Series in Surgery (PROCESS) guidelines. Int. J. Surg. 2018, 60, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Hobeika, C.; Cauchy, F.; Soubrane, O. Case series of extended liver resection associated with inferior vena cava reconstruction using peritoneal patch. Int. J. Surg. 2020, 80, 6–11. [Google Scholar] [CrossRef]
- Kulaylat, M.N.; Karakousis, C.P.; Doerr, R.J.; Karamanoukian, H.L.; O’Brien, J.; Peer, R. Leiomyosarcoma of the inferior vena cava: A clinicopathologic review and report of three cases. J. Surg. Oncol. 1997, 65, 205–217. [Google Scholar] [CrossRef]
- Serradilla-Martín, M.; Oliver-Guillén, J.R.; Ruíz-Quijano, P.; Palomares-Cano, A.; de la Plaza-llamas, R.; Ramia, J.M. Surgery of Colorectal Liver Metastases Involving the Inferior Vena Cava: A Systematic Review. Cancers 2023, 15, 2965. [Google Scholar] [CrossRef]
- Arii, S.; Teramoto, K.; Kawamura, T.; Takamatsu, S.; Sato, E.; Nakamura, N.; Iwai, T.; Mori, A.; Tanaka, J.; Imamura, M. Significance of hepatic resection combined with inferior vena cava resection and its reconstruction with expanded polytetrafluoroethylene for treatment of liver tumors. J. Am. Coll. Surg. 2003, 196, 243–249. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Koch, M.; Zimmermann, J.B.; Elbers, H.; Bruckner, T.; Contin, P.; Reissfelder, C.; Schmidt, T.; Weigand, M.A.; Martin, E.; et al. Infrahepatic inferior vena cava clamping for reduction of central venous pressure and blood loss during hepatic resection: A randomized controlled trial. Ann. Surg. 2011, 253, 1102–1110. [Google Scholar] [CrossRef]
- Jibiki, M.; Inoue, Y.; Kudo, T.; Toyofuku, T.; Saito, K.; Kihara, K.; Kudo, A.; Ban, D.; Arii, S. Combined resection of a tumor and the inferior vena cava: Report of two cases. Surg. Today 2014, 44, 166–170. [Google Scholar] [CrossRef]
- Oldhafer, K.J.; Stavrou, G.A.; Wagner, K.C.; Fard-Aghaie, M.H. Liver Resection with In Situ Hypothermic Perfusion: An Old but Effective Method. Ann. Surg. Oncol. 2019, 26, 1859. [Google Scholar] [CrossRef] [PubMed]
- Pulitanó, C.; Crawford, M.; Ho, P.; Gallagher, J.; Joseph, D.; Stephen, M.; Sandroussi, C. The use of biological grafts for reconstruction of the inferior vena cava is a safe and valid alternative: Results in 32 patients in a single institution. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2013, 15, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Palacios, A.R.; Schmeusser, B.N.; Midenberg, E.; Patil, D.; Xie, L.; Nabavizadeh, R.; Ogan, K.; Cardona, K.; Maithel, S.K.; Master, V.A. Resection of retroperitoneal tumors with inferior vena cava involvement without caval reconstruction. J. Surg. Oncol. 2022, 126, 1306–1315. [Google Scholar] [CrossRef]
- Fiore, M.; Colombo, C.; Locati, P.; Berselli, M.; Radaelli, S.; Morosi, C.; Casali, P.G.; Gronchi, A. Surgical technique, morbidity, and outcome of primary retroperitoneal sarcoma involving inferior vena cava. Ann. Surg. Oncol. 2012, 19, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Balzan, S.M.P.; Gava, V.G.; Magalhaes, M.A.; Rieger, A.; Roman, L.I.; Dos Santos, C.; Marins, M.P.; Rabaioli, B.; Raupp, I.T.; Kunzler, V.B. Complete and partial replacement of the inferior vena cava with autologous peritoneum in cancer surgery. J. Surg. Oncol. 2021, 124, 665–668. [Google Scholar] [CrossRef]
- Orbach, L.; Nachmany, I.; Goykhman, Y.; Lahat, G.; Yossepowitch, O.; Beri, A.; Ben-Gal, Y.; Klausner, J.M.; Lubezky, N. Surgical approach to abdominal tumors involving the inferior vena cava. Isr. Med. Assoc. J. 2020, 22, 364–368. [Google Scholar]
- Wachtel, H.; Gupta, M.; Bartlett, E.K.; Jackson, B.M.; Kelz, R.R.; Karakousis, G.C.; Fraker, D.L.; Roses, R.E. Outcomes after resection of leiomyosarcomas of the inferior vena cava: A pooled data analysis of 377 cases. Surg. Oncol. 2015, 24, 21–27. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).