Abstract
Background/Objective: Inflammatory bowel disease (IBD) diagnosis in the elderly falls under two categories: those diagnosed at a younger age and transitioning to the elderly group (>60 years) and those diagnosed at ≥60 years of age. Although it is difficult to calculate the incidence of IBD among elderly adults precisely, it is estimated that around 10–15% of IBD in the US are diagnosed after 60 years, and approximately 13% of IBD cases are diagnosed after the age of 65 globally. The objective of this systematic review is to assess the therapeutic needs of elderly adults with IBD, focusing on quality of life (QOL), symptom presentation, mental health management, IBD medication utilization patterns, surgical outcomes, and healthcare utilization to identify gaps in IBD management. Methods: We identified 42 published articles through a database search using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses from October 2023 to June 2024. We conducted the quality appraisal of the selected studies using the Joanna Briggs Institute (JBI) critical appraisal tools. Results: Our findings indicate decreased health-related QOL, more colonic and less penetrating disease in elderly Crohn’s disease patients, and comparable symptoms between elderly and younger ulcerative colitis patients. Despite an increased trend in prescribing biologics, the elderly show decreased response rates and poor remission. Higher healthcare utilization is noted among elderly IBD patients, alongside insufficient attention to their mental health concerns. Conclusions: The findings from this systematic review offer a comprehensive synthesis of the management of elderly adults with IBD and highlight several unmet needs that warrant attention in future research and clinical practice considerations.
1. Introduction
Inflammatory bowel disease (IBD) is an incurable illness affecting the gastrointestinal (GI) tract characterized by diarrhea, abdominal cramps, weight loss, rectal bleeding, and other extra-intestinal manifestations [1]. Crohn’s disease (CD) and ulcerative colitis (UC) represent the primary forms of IBD. According to recent data, approximately 3.1 million adults in the United States are affected by IBD [1]. The prevalence of IBD is increasing by 5.2% annually among elderly adults [2]. IBD diagnosis among elderly adults can be categorized into two groups: 1) those diagnosed with IBD at a younger age and then transitioned to the elderly group (>60 years of age) and adults diagnosed with IBD at 60 years of age or older [3]. Based on a 2019 global study, there has been a significant rise in the incidence rate of IBD among older adults worldwide, with the highest rates observed in the Western Pacific area and the greatest burden found in the US [4]. Although it is difficult to calculate the incidence of IBD among elderly adults precisely, it is estimated that around 10–15% of IBD in the US are diagnosed after 60 years, and approximately 13% of IBD cases are diagnosed after the age of 65 globally [4,5].
The dysbiosis of intestinal microbial flora is a major contributing factor to the diagnosis of IBD among elderly adults. The intestinal microbiota is altered in the elderly due to several reasons. Physiological changes associated with normal aging, such as decreased intestinal motility, fecal retention, altered nutrition due to decreased taste and smell, and decreased resistance to stressors, may disrupt the balance of gut bacteria in elderly adults and increase their risk for IBD [3]. In addition to the unique pathophysiology of IBD among elderly adults, elderly patients face multiple challenges associated with its treatment. Elderly adults with IBD are often excluded from clinical trials due to factors such as age, multiple comorbid conditions, and a history of dysplasia or cancer [5,6]. As a result, determining the best drug therapy for this population to manage their IBD-related symptoms remains difficult. To address these challenges, the American Gastroenterology Association (AGA) updated its clinical practice guidelines on the management of IBD in elderly patients [2]. However, these recommendations heavily focused on diagnosis and medical management, with little or no attention to the management of mental health, symptom management, evaluation of the cost of illness, and other unmet needs of elderly adults with IBD [2].
Any chronic illness significantly affects the quality of life (QOL) of the affected population. This is also true for IBD, which impairs the QOL of elderly adults [7]. Moreover, little is known about the other unmet needs and burdens perceived by elderly adults with IBD. These individuals are at risk for mental health concerns due to both disease-related and treatment-related factors [8]. Older adults with IBD tend to have a higher geriatric deficit [9] and experience negative health outcomes due to frailty [10]. IBD patients generally face many unplanned healthcare utilization needs [11]; however, the situation varies greatly among elderly adults with IBD due to aging and related co-morbid conditions. Therefore, the purpose of this systematic review is to assess the therapeutic needs of elderly adults with IBD, with a specific focus on their QOL, symptom presentation, mental health management, IBD medication utilization patterns, surgical outcomes, and healthcare utilization, to identify the gaps in their IBD management.
2. Methods
We utilized a systematic review methodology to achieve the purpose of this study, conducting a literature review from October 2023 to June 2024 to select published manuscripts focused on the management of elderly adults with IBD. We adhered to the Joanna Briggs Institute (JBI) guidelines for systematic reviews to guide our study [12].
2.1. Search Method
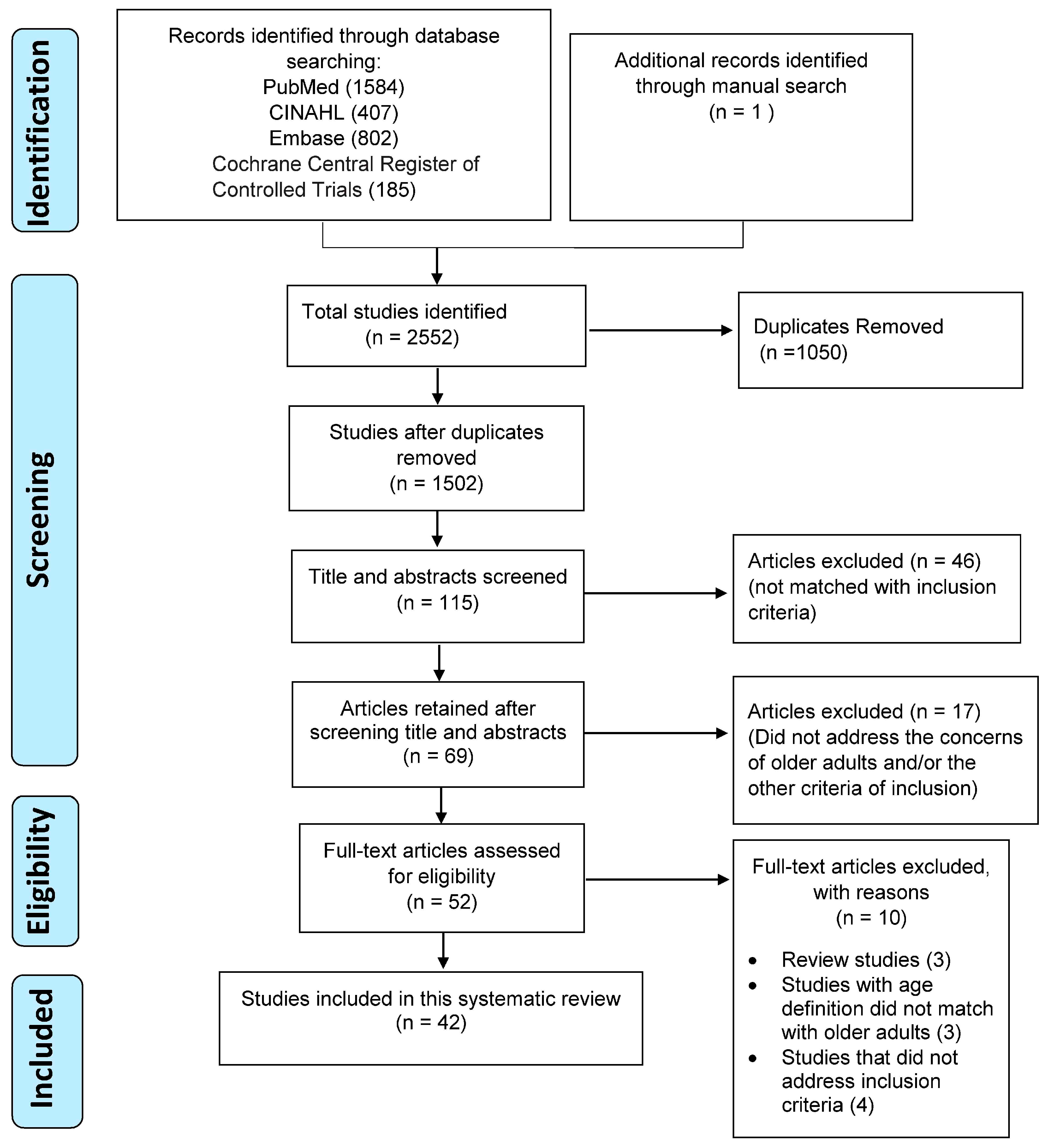
Using the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), we conducted a literature search to identify the eligible articles for this systematic review [13]. In partnership with a research librarian, we developed a search plan and conducted a database search of PubMed, Embase, CINAHL, and Cochrane Central Register of Controlled Trials using the following keywords: “inflammatory bowel disease, Crohn’s disease, ulcerative colitis, older adults, elderly IBD, frailty, quality of life, symptoms, cost of illness, medication outcomes, mental health, social support, burden, and unmet needs”. These keywords were customized based on the prerequisites of each database to identify the articles.
The second author refined the search process by uploading the articles identified via the database search to Covidence, a software program designed to streamline the review process and facilitate collaboration among multiple authors [14]. Covidence helped remove duplicates. The second author then screened the titles and abstracts of the articles, retaining those that met the inclusion criteria. The first author verified the screening process, and no discrepancies were noted between the first and the second author during title and abstract screening, as we have well-defined inclusion criteria. Subsequently, the first, second, third, and fourth authors read all the full-text articles retained for this review based on the inclusion criteria. Lastly, the first author manually reviewed the references of the selected studies to figure out any additional research articles that matched the criteria. All authors agreed to the final list of full-text articles selected for this review.
2.2. Study Selection Criteria
We defined older adults with IBD as those diagnosed with IBD at a younger age and then transitioned to the elderly group (>60 years of age) and adults diagnosed with IBD ≥60 years of age [3]. The inclusion criteria were: (1) studies published in English; (2) quantitative (randomized or non-randomized studies), qualitative, or mixed-method studies that focused on elderly adults with IBD; and (3) studies published from 2012 to 2024.
The concept of addressing the concerns of elderly adults with IBD emerged as the baby boomers reached the elderly category [15]. Since then, more research has focused on addressing the needs of the elderly, particularly evaluating the effectiveness of pharmacological therapies among elderly adults with IBD. Subsequently, several other studies have explored additional healthcare dimensions, such as quality of life (QOL), mental health, healthcare utilization, and causes of hospitalization among elderly adults with IBD [16,17,18,19]. Therefore, we decided to select the timeframe of 2012–2024 to synthesize evidence from the most recently published literature.
We based our definition of elderly adults by age on the United Nations’ criteria of individuals aged 60 years or above [20]. The exclusion criteria were: (1) any type of review or conference abstract; (2) studies that focused on adult (18–59 years old) and pediatric (<18 years old) IBD patients; and (3) studies published before 2012. The search process is summarized in the PRISMA diagram in Figure 1.
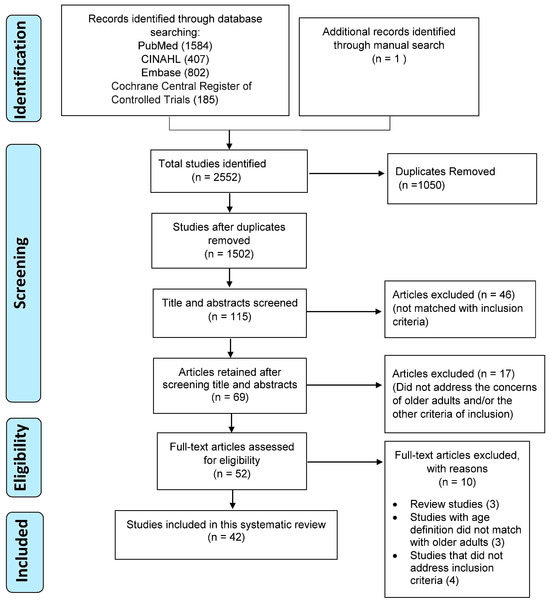
Figure 1.
PRISMA flow diagram.
2.3. Quality Appraisal
The authors conducted the quality appraisal of the selected studies using the Joanna Briggs Institute (JBI) critical appraisal tools [21]. We utilized four JBI quality assessment tools that matched the study designs of the selected articles: the JBI analytical cross-sectional quality assessment tool, the JBI case-control quality assessment tool, the JBI qualitative research quality assessment tool, and the JBI cohort quality assessment tool. These included 8–11 questions based on the study design, with responses of “yes”, “no”, “not applicable”, or “unclear” for each given question. The first author independently conducted the quality appraisal, which was then verified by the second author. Any disagreements were resolved through discussion. The majority of questions for each study were answered with “yes”. The quality appraisal results are summarized in Supplementary Table S1.
2.4. Data Abstraction
The authors extracted data from the articles that met the inclusion criteria. The first author began the data extraction process, and subsequently, the third and fourth authors validated the extracted data. We extracted the following information based on the aims of the study: author details, study setting, study type, age of elderly participants as defined in the studies, the purpose of the study, variables measured, and major findings. Refer to Table 1 for data abstraction results. Because of the diverse study designs, we opted to qualitatively synthesize the findings.

Table 1.
Data Abstraction Table (n = 42). Therapeutic needs of older adults with IBD: A Systematic Review.
3. Results
3.1. Study Characteristics
We included 42 studies that met the inclusion criteria in this systematic review. The study settings varied across countries, with the US dominating with 13 studies, followed by Canada with five studies. Two studies were multinational [26,32]. More than 75% of the studies (n = 25) employed a retrospective design, with investigators using various types of databases (administrative, claims, or electronic medical records) to conduct their research. Only one of the reviewed studies utilized a qualitative design to elicit the perceptions of elderly adults with IBD [54]. The age of elderly adults was predominantly defined by the United Nations definition as >60 years in the majority (n = 23) of the reviewed studies, followed by >65 years in 16 studies. In other studies, the participants’ ages varied from >64, >66, and >70 years. Refer to Table 1 for further study details, which exposes the results of the included studies, mentioning the type of the study, the age of the included patients, the purpose of the study, variables and measures, and major findings.
3.2. Quality of Life
Of the 42 studies selected for this review, only six addressed the QOL of older adults with IBD [7,16,17,25,51]. Three of these studies were prospective [7,17,25], while the others were case-control [16], retrospective [51], and qualitative [54] studies. Except for one study [16], QOL was measured using the short IBD questionnaire [7,17,25,51]. A Chinese-based study used the Short-Form Questionnaire Version 12, while a US-based study employed the Short-Form Questionnaire (SF) Version 14 in addition to the short IBD questionnaire [7,16]. QOL in elderly adults with IBD was found to be lower in four of the reviewed studies [16,17,25,51], with significantly lower QOL noted in two of the findings (p < 0.05–p < 0.001) [17,51]. A Canadian study revealed that health-related QOL was not influenced by age, but a statistically significant association was noted between health-related QOL and psychological disorders in elderly CD patients (p < 0.001) [51]. Decreased health-related QOL was observed in elderly adults with IBD in the Netherlands who had positive clinical (measured via partial Mayo score for patients with UC and the Harvey Bradshaw Index [HBI] for patients with CD) and biochemical disease activity (measured via positive fecal calprotectin and C-reactive protein) [25]. Conversely, a US-based study indicated that older IBD patients have higher IBD-related QOL (measured via a short IBD questionnaire) and mental component of QOL but lower physical QOL; both were measured via the Short-Form Questionnaire Version 12 [7]. The qualitative study did not directly measure the QOL of elderly adults with IBD. Instead, it asked the participants to define QOL. The participants reported that QOL meant their ability to engage in activities they enjoyed, such as traveling and spending time with family [54]. However, the participants also expressed concerns related to loss of independence, mobility, and sensory loss due to aging, which they viewed as barriers to healthcare access [54].
3.3. Symptom Presentation
3.3.1. IBD-Related Symptoms
In general, the symptom presentation of IBD among elderly adults varied in many of the reviewed studies compared to non-elderly adults. Elderly-onset CD patients exhibited fewer GI (abdominal pain, diarrhea) and systemic symptoms but had higher instances of anal fistula and rectal bleeding compared to younger patients. However, elderly-onset UC patients experienced less abdominal pain and rectal bleeding [30]. A retrospective study in France revealed that non-struicturing/non-penetrating disease types were the most frequently noted among both groups of CD patients (those who were diagnosed at the age of 70 years vs. between 60 and 69 years) [36]. Colonic involvement was commonly observed among elderly CD patients [4,36,37], with moderate clinical disease activity [37]. These findings were mirrored in a US-based retrospective cohort study, which noted that the majority of elderly-onset CD was isolated to the colon compared to adult-onset CD (p = 0.048); moreover, non-stricturing/non-penetrating behavior was prominent among both elderly- and adult-onset CD [40]. However, elderly-onset CD had a decreased rate of perianal disease (p = 0.018) and penetrating disease (p = 0.023) compared to adult-onset CD, as confirmed in a later US retrospective study [7]. Conversely, no such differences in disease location were observed between elderly and adult-onset UC [50]. A retrospective cohort study using a Swedish registry showed that stricturing was more common among elderly CD patients [47], while a similar study from Spain reported a higher proportion of complicated disease (p = 0.01) among elderly IBD patients [29]. Less proctitis was noted among elderly UC patients compared to their younger counterparts [35]. Additionally, elderly CD patients presented with nutritional deficiencies, such as iron (p = 0.03), vitamin B12 (p = 0.02), and vitamin D deficiency (p = 0.003), correlated with the duration of CD. No such correlation was observed among elderly UC patients [43].
3.3.2. Geriatric Concerns
Several of the reviewed studies addressed concerns related to older age, such as co-morbidity, geriatric deficit, frailty, and risk of complications [19,25,32,41,43,44,47,49,50,53,54,56,57]. Findings from a prospective study in the Netherlands indicated that 39.9% (n = 405) of patients with severe geriatric deficits had active disease [25]. Of these, 51.6% had deficits in the somatic domain, such as comorbidity, polypharmacy, and nutrition; 43% had deficits in activities of daily living; 22.7% had deficits in physical capacity; 16.5% had deficits in the mental domain; and 23.7% had deficits in the social domain [25]. Similar findings were noted in a large retrospective study in Sweden, where frailty was strongly linked to an increased risk for mortality among elderly adults with IBD. Additionally, a high frailty risk increases the mortality risk from digestive diseases, infections, hematological conditions, respiratory disease, nutrition and metabolic diseases, circulatory disorders, nervous system disorders, and trauma [47].
The reviewed studies highlighted several common co-morbidities among elderly adults with IBD. Findings from multiple studies revealed higher comorbidity rates among older patients compared to their younger counterparts (p < 0.01) [19,56,57]. Elderly IBD patients had significantly greater cardiovascular, metabolic (diabetes), and respiratory comorbidities in both CD and UC [17,36,42,49]. Consistent with the previous studies, higher comorbidity rates were noted among elderly adults with IBD before initiating the Vedolizumab in a retrospective study in the US [44]. Polypharmacy was highly prevalent among elderly adults with IBD; a retrospective study in the US indicated that out of 393 older patients, 94.3% were on ≥3 medications [43]. Participants from a qualitative study reported that their IBD symptoms were the most bothersome than their comorbid conditions [54].
Higher cancer prevalence among elderly adults with IBD was a concern in many of the reviewed studies [44,49,57]. Further analysis of a retrospective study in China indicated a higher cancer incidence rate in general, as well as colorectal cancer, among elderly-onset IBD compared to adult-onset IBD, with a higher cancer-related mortality rate [57]. Additionally, there was an increased incidence of extra-intestinal cancer among elderly-onset IBD patients, with an upward trend since 2016. Diabetes was found to be a risk factor for malignancy, while the use of steroids was a protective factor [57]. Malignancies accounted for the major cause of death in elderly-onset IBD in Canada [38]. Results from a recent case-control study showed that an IBD diagnosis did not increase the overall cancer risk in older adults with IBD [58]. However, a statistically significant association was noted between an IBD diagnosis and colorectal cancer, small intestinal cancer, and intra- and extra-hepatic bile duct cancer. After adjusting for IBD medications, an IBD diagnosis was not related to the risk of extra-intestinal cancers in older adults with IBD [58].
Analysis of treatment-related complications revealed no differences between older patients with adult-onset IBD (AO-IBD) compared to elderly-onset IBD (EO-IBD; p = 0.03) in a retrospective study in the US [53]. The same study showed an increased risk of treatment-related complications in EO-IBD patients with multiple co-morbidities, while improved functional status and better biological reserve predicted worse health outcomes [53]. A retrospective study based on a large national sample showed increased mortality rates, longer hospital stays, and a higher proportion of females among elderly IBD patients [56]. Clostridium difficile was the most common complication found among elderly IBD patients. Sepsis was the major cause of death among both geriatric and non-geriatric IBD patients, according to this national data [56]. Furthermore, being over 65 was associated with higher odds of death among elderly IBD patients (p < 0.001). Increased inpatient mortality was noted for patients older than 65 with IBD, regardless of their comorbidities and disease type [56].
3.4. IBD Medication Utilization Patterns
3.4.1. Biologics
Most of the reviewed studies focused on the safety and efficacy of different IBD medications, comparing elderly IBD patients to non-elderly IBD patients. Biologics were the most commonly analyzed medication group in these reviewed studies [7,29,32,33,34,35,41,42,48,52]. Although anti-TNF groups were the most frequently addressed biologics, integrin receptor antagonists (Vedolizumab) and anti-IL-12 and -23 blockers (Ustekinumab) were also examined [28,29,31,32,37,38,39,44,52,55].
Regarding the use and efficacy of biologics, several studies reported decreased usage and response rates for anti-TNF among elderly IBD patients [7,30,35,41,42,43,46,50]. Additionally, some studies noted increased failure rates with anti-TNF, higher discontinuation rates, and decreased rate of remission also noted in elderly adults [24,33,34,42,48]. Infection and infusion reactions were the most common reasons for stopping anti-TNF therapy [22,33,34]. However, a multinational study based on health administrative databases from 2004 to 2009 revealed an increasing trend in prescribing biologics for elderly adults with IBD [26].
Most recent studies evaluated the effectiveness of other biologics, such as integrin receptor antagonists (Vedolizumab) and anti-IL-12 and anti-23 blockers (Ustekinumab), with varied results [22,26,28,29,31,32,37,38,39,44,52,55]. Four studies compared the effectiveness of Vedolizumab between elderly and non-elderly IBD patients [32,44,52,55]. Clinical, endoscopic, and corticosteroid-free remission after Vedolizumab use was found to be similar between both elderly and non-elderly IBD patients in a multinational study [32], and endoscopic assessment revealed similar mucosal healing in both elderly and adult IBD patients who were on Vedolizumab in a US-based study [55]. However, elderly IBD patients treated with anti-TNFα demonstrated poor response and remission rates to Vedolizumab compared to their younger counterparts [32,52]. Elderly UC patients had decreased clinical remission in response to Vedolizumab, but no difference in endoscopic remission was noted among elderly CD patients [52]. Some studies reported discontinuation of Vedolizumab due to a lack of response among elderly IBD patients [44,52] Although not fatal, the infection rate was higher among elderly IBD patients on Vedolizumab compared to non-elderly IBD patients [32]. Additionally, findings from a matched cohort study in Italy indicated an increased risk of cancer diagnosis among elderly IBD patients who were on Vedolizumab compared to non-elderly patients [52]. Two studies compared the effectiveness of Ustekinumab among elderly versus non-elderly CD patients, yielding mixed results [29,37], The effectiveness of Ustekinumab (measured as steroid-free remission) was comparable between the two age groups, and no difference in adverse effects was observed in a multicenter study in Spain [29]. However, a retrospective cohort study in the US highlighted a significantly lower chance of achieving complete clinical remission after initiating Ustekinumab among elderly CD patients compared to their peers (p = 0.01) [37]. The rate of infusion reaction and other complications (infection, postoperative complications) did not differ between elderly and non-elderly CD patients [37].
Five recent studies compared the effectiveness of three biological groups, namely, anti-TNF, Ustekinumab, and Vedolizumab, among elderly adults with IBD [22,28,31,38,39]. Findings from a UK study indicated that sustained use and serious infection rates were similar among patients who were on Ustekinumab and Vedolizumab. The penetrating nature of CD was positively associated with persistent use of Ustekinumab and Vedolizumab, and disease activity (measured by HBI) significantly reduced after 6 months and at 1 year in both groups [38]. Similarly, a Canada-based study showed no statistical difference in the remission rates among the use of four biologics (Vedolizumab, Adalimumab, Infliximab, and Ustekinumab) among elderly adults with IBD [39]. The risk of infection among elderly IBD patients was comparable between the biologics (Vedolizumab, anti-TNF, and Ustekinumab) in three studies [28,31,39] Pneumonia followed by septicemia were the most common reasons for in-patient hospitalization among the three groups (Vedolizumab vs. Ustekinumab vs. anti-TNF) in a US-based study [31]. Meanwhile, digestive tract infection was the most common among the anti-TNF group, while pulmonary infections were common among elderly IBD patients who used Vedolizumab and Ustekinumab in France [28]. A retrospective US study comparing the safety of anti-TNF versus Vedolizumab indicated that infusion reactions and infection (20%) were the most common reasons for stopping anti-TNF therapy, whereas infection (14%) was the sole reason for stopping Vedolizumab [22]. Additionally, 3% of patients from the anti-TNF group and 1% from the Vedolizumab group developed a new onset of cancer (excluding skin cancer) or recurrence of their previous cancer after initiating the therapy [22].
3.4.2. Immunosuppressant Medications
Contrasting findings were noted regarding the use and outcomes of immunosuppressant medications among elderly IBD patients. The findings of a few studies reported increased use of these medications among elderly adults with IBD [26,41], with one study highlighting that this use was associated with a longer disease course [41]. Conversely, many studies reported decreased use of immunosuppressant medications among elderly IBD patients [7,34,35,36], and one study noted a low cumulative probability of immunosuppressant use among elderly CD patients in Korea [46]. Interestingly, elderly adults with IBD who were on immunosuppressants were found to be at low risk for frailty [47].
3.4.3. 5-Aminosalicylic Acids (5-ASA) and Steroids
Only four of the reviewed studies addressed the use of 5-ASA agents, which are commonly used for maintenance therapy among adults with IBD [26,30,43,49] The findings from a multi-national study indicated that 5-ASA was more commonly used in Canada, while Sulfasalazine was more commonly used in the UK by elderly adults with IBD.
Similarly, a few studies addressed corticosteroid therapy in older adults with IBD [17,41,42,43,53]. In a US-based study, out of 393 participants [50], 0.6% of the older IBD patients were on chronic steroid therapy [43], while a study from Spain showed that more than half (66%) out of 314 patients were on steroids [41]. The use of corticosteroids was significantly associated with depression among elderly adults with IBD (p < 0.01) [17]. Additionally, corticosteroid therapy and prior surgery were associated with an increased risk of treatment-related complications in adult-onset IBD patients in the US [53]. However, findings from a retrospective cohort study in Canada indicated that the majority of elderly IBD patients received steroids within five years of diagnosis [18]. Higher usage of rectal therapy with 5-ASA and topical corticosteroids was noted in Denmark and Canada in a multi-national study [26].
3.5. Surgical Outcomes
Nine of the reviewed studies evaluated the surgical outcomes of elderly adults with IBD, yielding mixed results. Findings from a retrospective cohort study in Canada indicated that elderly adults with UC had a higher five-year cumulative risk of surgery compared to young and middle-aged IBD patients [50]. Similar findings were noted in a retrospective study from Sweden, which reported a higher absolute risk for bowel surgery in elderly adults with IBD (p < 0.001) [35]. However, a UK-based study comparing the surgical risk between elderly- and adult-onset IBD and analyzing the effect of thiopurines on surgical outcomes showed a comparable risk for colectomy between elderly and adult-onset UC in 1, 5, and 10-year risk analyses. Notably, decreased surgical risk (colectomy) was observed among elderly-onset UC patients who were on thiopurines for more than 12 months [23]. Further analyses among elderly adults with CD showed a comparable cumulative risk of surgery between elderly adults with CD and young and middle-aged IBD patients in Canada [50]. By contrast, a UK-based study noted a decreased risk for first intestinal resection in elderly-onset CD compared to adult-onset CD in 1, 5, and 10-year risk analyses [39]. Similar results were observed in a Korean study, which reported a decreased risk for bowel resection in elderly-onset CD patients compared to the adult group (p = 0.067) [46]. A retrospective study based on large US national data also confirmed decreased surgical rates among elderly IBD patients [56]. Out of 314 study participants in a retrospective study in Spain, bowel resections were the most frequently performed surgical intervention (90%) [41]. A case-control study based on a national database from the US compared post-operative complications and death between elderly IBD patients and non-elderly IBD patients [27]. Out of 1707 elderly IBD patients, post-operative mortality (within 30 days) was higher for both elderly UC (p < 0.001) and CD (p < 0.001) patients compared to non-elderly patients. Additionally, longer lengths of stay, increased risk of renal dysfunction post-surgery (p < 0.001), higher rates of infectious complications after surgery (wound dehiscence, shock, pneumonia, ventilator dependence, and urinary tract infections; p < 0.001 for all), increased risk of myocardial infarction and cardiac arrest post-surgery (p < 0.001), and increased need for blood transfusion (p < 0.001) were noted among elderly IBD patients [27]. However, a higher risk for DVT (p < 0.001) was only noted among elderly CD patients [27].
Few studies evaluated the surgical outcomes of IBD medication therapy. Interestingly, a retrospective study from France showed that treatment with systemic steroids reduced the risk of surgery among elderly IBD patients [30]. Post-operative complications were comparable among elderly CD patients who had a surgical resection while on Ustekinumab versus those who were not on Ustekinumab in a retrospective study in the US [37]. Further analysis revealed that the rate of surgery did not differ between those who are more than 70 years old versus those who are between 60 and 69 years old in France [36].
3.6. Healthcare Utilization
Hospitalization rates, ED visits, care provided by a gastroenterologist, and diagnostic imaging rates were compared between elderly and non-elderly IBD patients. In the Netherlands, a higher risk for hospitalization was noted among elderly onset UC at the time of diagnosis and during follow-up at 5 and 10 years [42]. Similar findings were observed in a retrospective study in Canada, where higher hospitalization rates were noted among elderly IBD patients within one year of diagnosis, although this rate decreased in subsequent years [40]. Furthermore, this study reported decreased healthcare utilization among elderly IBD patients compared to their younger counterparts, including a lower chance of gastroenterology visits within one year of diagnosis and at five years post-diagnosis (p < 0.001) [40]. Additionally, diagnostic imaging utilization was significantly higher among elderly UC patients compared to young adults (p < 0.001), with fewer ED visits noted among elderly IBD patients within the first and third years compared to their younger counterparts (p < 0.001) [40]. Compared to previous studies that were older [40,42], findings from a recent retrospective study in Canada indicated decreased colectomy and hospitalization risk among elderly adults with IBD who received care from a gastroenterologist [45]. Another benefit observed with gastroenterologist care included increased use of biologics (within five years of IBD diagnosis) and systemic steroids (within 1 and 5 years of IBD diagnosis), whereas decreased use of immunomodulators was noted among elderly IBD patients whose primary care providers were not gastroenterologists [45]. However, disparities exist in gastroenterologist care among IBD patients living in rural versus urban areas; elderly IBD patients in rural areas were less likely to receive gastroenterology care compared to younger patients across all age groups living in rural areas [45].
A large (n = 15,428) retrospective study in the US that analyzed the costs, annual burden, and reasons for hospitalization among elderly adults with IBD indicated that they had an increased length of stay in hospitals compared to middle-aged and younger patients (p < 0.01), along with increased hospitalization-related costs (p < 0.01) [19] Older IBD patients have less chance to undergo IBD-related procedures and GI surgeries compared to younger IBD patients (p < 0.01). Serious infections (bacteremia, Clostridium difficile, and pneumonia) were the primary cause of hospitalization among older patients (p < 0.01), followed by cardiovascular complications (p < 0.01) in this cohort. Adults >64 years of age were more likely to receive a blood transfusion during hospitalization [19] Interestingly, only one of the reviewed studies addressed the financial concerns of elderly adults with IBD. Participants in this qualitative study raised concerns related to medication costs as a major factor influencing treatment choices, challenges with insurance coverage, and the impact of spending retirement income to manage their IBD [54].
3.7. Mental Health Concerns
Only two of the reviewed studies addressed the mental health concerns of adults with IBD [17,25] One study evaluated the geriatric deficits of 405 elderly adults with IBD and found that 16.5% of them had deficits in the mental domain. Patients with older-onset IBD were more often impaired in the mental domain, including cognitive impairment (16.9% vs. 6.7%; p < 0.001) [25]. Another prospective study in the US indicated that higher levels of disease activity were significantly associated with depression among older adults with both CD (p = 0.005) and UC (p = 0.003). It was also noted that medication adherence was significantly decreased in patients with depression compared to patients without depression [17]. Although not directly related to mental health, participants of a qualitative study expressed the profound impact of social isolation due to their bowel urgency and other IBD symptoms [54]. This social isolation can significantly influence the mental health of older adults with IBD, exacerbating feelings of loneliness and affecting overall well-being.
4. Discussion
This systematic review aimed to assess the therapeutic needs of elderly adults with IBD, focusing on their QOL, symptom presentation, mental health management, IBD medication utilization patterns, surgical outcomes, and healthcare utilization to identify gaps in their IBD management. Findings from this systematic review highlighted several key points: elderly adults with IBD generally experience decreased health-related QOL, more frequently presenting with colonic involvement and less frequently with penetrating disease in the case of CD. Symptom presentations were comparable between elderly versus younger UC patients. Despite an observed trend toward increased biologic prescriptions for the elderly, there was a noted decrease in response rates and poorer rates of remission. The use of immunomodulators and corticosteroids remains prevalent, with mixed results in surgical outcomes among elderly adults with IBD. Healthcare utilization was higher among elderly adults with IBD.; however, affiliation with a gastroenterologist correlated with a decreased risk of hospitalization and surgery. Notably, mental health concerns of elderly IBD patients received insufficient attention in the reviewed studies.
These findings have significant implications for the care of elderly adults with IBD. Four of the reviewed studies reported decreased QOL among elderly adults with IBD. Managing a chronic illness poses numerous challenges for elderly adults, which can compromise their independence and QOL [59]. As a GI tract disorder, IBD significantly impairs QOL due to persistent GI symptoms, such as diarrhea, abdominal pain, nutritional deficits, bowel urgency, and other general symptoms related to fatigue [60]. Coupled with the effects of aging, these chronic symptoms can be particularly difficult for elderly adults to manage, a consideration often overlooked in clinical practice. Healthcare providers should consider and discuss interventions to maintain QOL, including ensuring family and social support and promoting activities that enhance physical functioning.
The expert review by the American Gastroenterological Association (AGA) recommends a comprehensive laboratory analysis of elderly adults with IBD, including blood tests for nutritional factors, such as serum albumin and serum ferritin, and stool testing for pathogens like Clostridium difficile, as needed [2]. Interestingly, only one of the reviewed studies reported nutritional blood profiles [43], and nutritional deficiencies are common factors contributing to geriatric deficits and frailty among older adults with IBD [25,47]. Therefore, dietary management is a key intervention to consider for maintaining functional status and addressing geriatric deficits and frailty among these patients. More research is warranted in this area to address the gaps in the literature and provide optimum nutritional support to adults with IBD.
The IBD medication utilization patterns differed across the reviewed studies, probably due to differences in study settings across the world where healthcare policies and clinical practice guidelines vary. The reviewed studies evaluated the safety and efficacy of different groups of biologics, such as anti-TNF agents (Infliximab and Adalimumab), integrin receptor antagonists (Vedolizumab), and interleukin inhibitors (Ustekinumab), in managing symptoms in older adults with IBD. All these biologics are included in the induction and maintenance algorithm for managing IBD in elderly patients as recommended by the American Gastroenterological Association (AGA) expert review, which suggests that faster-acting biologics may minimize risks associated with corticosteroid therapy in elderly IBD patients [2]. Although Tofacitinib as a Janus kinase inhibitor (JAS) was recommended by the AGA expert review for both induction and maintenance of IBD symptoms in elderly IBD patients, none of the reviewed studies evaluated the safety and efficacy of this medication.
Although biologics have been recommended for managing IBD symptoms in elderly IBD patients, healthcare providers cannot ignore their adverse effects, including the risk of malignancy and infection. The AGA expert review recommends considering the suitability of an elderly adult for the medications recommended in the treatment algorithm by evaluating the risks associated with the therapy, geriatric deficits, and higher comorbid status of the elderly, as well as evaluating renal and hepatic functions, tuberculosis, and hepatitis B status [2]. Additionally, screening the status of thiopurine methyl transferase is recommended before starting thiopurine for elderly IBD patients [2].
Only a few of the studies addressed corticosteroid therapy in this systematic review. The AGA expert review committee recommends the use of Budesonide due to its high first-pass metabolism [2]. Although higher use of rectal steroid therapy was noted in one of the reviewed studies [26], a clinician needs to consider the self-administering ability and mobility status of elderly IBD patients or the ability of their available support system to administer the medication, as well as the strength of their rectal sphincter to retain the rectal forms of corticosteroid therapy [2].
The findings from this review shed light on several unmet needs of elderly adults with IBD. Studies addressing healthcare utilization consistently reported increased hospitalization rates, emergency room visits, and diagnostic imaging among elderly adults with IBD [18,42,45]. However, no one explored the financial concerns related to the increase in healthcare utilization or the costs of the medications. Many elderly adults with IBD may have retired and used their retirement funds to manage IBD-related expenses [54]. Others may be relying on governmental aid or a family member to meet their expenses as they are unable to work due to their declining functional status. In a previously published study, both groups of elderly adults (who acquired IBD at an early age and acquired old versus those who acquired IBD at a later stage) expressed fears and concerns about meeting their financial needs [54]. These financial concerns necessitate more exploration in future research to identify cost-effective strategies and options for support from government and non-government agencies to meet the financial struggles of elderly adults with IBD.
Only two studies among those reviewed addressed the mental health needs of elderly adults with IBD [17,25]. As a chronic illness affecting the GI tract, many older patients with IBD are at risk for developing mental health disorders, including depression, due to a number of reasons. First, they may be socially withdrawn due to their bowel urgency and the associated stigma [54]. Second, some IBD medications, such as corticosteroid use, put an individual at risk for depression [2,17]. Previously published data support the association between depression and medication adherence [25]. Given that medication adherence is vital in managing IBD symptoms, clinical practices need to consider assessment and depression screening of elderly adults with IBD for prompt referral to a mental healthcare team. Social support is another factor directly connected to the mental health status of an individual. Published literature reiterates that social support promotes well-being, improves health outcomes and self-management of IBD, as well as facilitates the management of loneliness and depression [61,62]. Additionally, social support can significantly influence health maintenance, such as adhering to appointments and medications. Therefore, support needs to be promoted not only to manage mental health concerns but also to treat IBD as a disease.
Although AGA experts recommend health maintenance practices such as annual influenza, pneumococcal, and herpes zoster vaccinations [2], none of the reviewed studies evaluated their effectiveness in elderly adults with IBD. Future research should address this gap. Findings from a recent qualitative study reported that elderly adults with IBD verbalized gaps related to informational needs to maintain their routines [54].
Considering the insufficient evidence on any special dietary practices to support the clinical course of IBD and the physiology of aging, recommendations have been made to include vitamin D, protein, and adequate water consumption based on the body weight of older adults with IBD as well as oral nutrition supplements [63,64]. The published literature is inconclusive in support of low FODMAP (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) and anti-inflammatory diet (IBD-AID) for older adults with IBD. A personalized approach to nutrition, considering the IBD disease characteristics and co-morbidity of the individual, has been recommended for older adults with IBD [63,64]. Additionally, there have been recommendations to consider a DASH or Mediterranean diet due to their potential benefits for comorbidities, although empirical evidence on these interventions is lacking among older adults with IBD [63,64]. The AGA recommends including a nutritionist in the multidisciplinary team when managing the care of elderly adults with IBD [2]. Although the dysbiosis of intestinal microbial flora is a major contributing factor to the diagnosis of IBD among elderly adults, no empirical studies have evaluated the effectiveness of probiotics in alleviating symptoms or preventing the onset of IBD in this population. Future studies are warranted to explore the effectiveness of probiotics among older adults with IBD.
The strengths of this review include pooling information from 42 empirical studies that provided data from a large number of elderly adults with IBD. Additionally, we have included studies across the world, such as the US, Canada, Spain, France, and the UK, and provided a worldwide perspective on the management of elderly adults with IBD. The limitations of this review are that the majority of the studies were retrospective studies that focused on electronic medical records or administrative claims, which can probably contribute to errors related to data abstraction. Few observational or prospective studies and limited qualitative studies addressed the perceptions of elderly adults with IBD, highlighting areas for further investigation.
5. Conclusions
This systematic review focused on assessing the therapeutic needs of elderly adults with IBD, focusing on their QOL, symptom presentation, mental health management, IBD medication utilization patterns, surgical outcomes, and healthcare utilization to identify gaps in their IBD management. The findings from this systematic review offer a comprehensive synthesis of the management of elderly adults with IBD and highlight several unmet needs that warrant attention in future research and clinical practice considerations.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/gastroent15030059/s1, Table S1: JBI Critical Appraisal Checklist (n = 42).
Author Contributions
Conceptualization, S.P.D.; Data curation, S.P.D., S.F. and B.L.D.; Formal analysis, S.P.D., S.F. and B.L.D.; Investigation, R.M. and S.P.D.; Methodology, R.M. and S.P.D.; Project administration, S.P.D.; Resources, S.P.D.; Software, R.M. and S.P.D.; Supervision, S.P.D.; Validation, S.P.D., R.M., S.F. and B.L.D.; Visualization, S.P.D., R.M., S.F. and B.L.D.; Writing—original draft: S.P.D.; Writing—review & editing, R.M., S.F. and B.L.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Inflammatory Bowel Disease [Internet]. Centers for Disease Control and Prevention. 2022. Available online: https://www.cdc.gov/ibd/features/IBD-more-chronic-diseases.html (accessed on 22 June 2024).
- Ananthakrishnan, A.N.; Nguyen, G.C.; Bernstein, C.N. AGA Clinical Practice Update on Management of Inflammatory Bowel Disease in Elderly Patients: Expert Review. Gastroenterology 2021, 160, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Taleban, S.; Colombel, J.F.; Mohler, M.J.; Fain, M.J. Inflammatory bowel disease and the elderly: A review. J. Crohns Colitis 2015, 9, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Danpanichkul, P.; Suparan, K.; Arayakarnkul, S.; Jaroenlapnopparat, A.; Polpichai, N.; Fangsaard, P.; Kongarin, S.; Srisurapanont, K.; Sukphutanan, B.; Wanchaitanawong, W.; et al. Global Epidemiology and Burden of Elderly-Onset Inflammatory Bowel Disease: A Decade in Review. J. Clin. Med. 2023, 12, 5142. [Google Scholar] [CrossRef] [PubMed]
- Vieujean, S.; Caron, B.; Jairath, V.; Benetos, A.; Danese, S.; Louis, E.; Peyrin-Biroulet, L. Is it time to include older adults in inflammatory bowel disease trials? A call for action. Lancet Healthy Longev. 2022, 3, e356–e366. [Google Scholar] [CrossRef] [PubMed]
- Kochar, B.; Kalasapudi, L.; Ufere, N.N.; Nipp, R.D.; Ananthakrishnan, A.N.; Ritchie, C.S. Systematic Review of Inclusion and Analysis of Older Adults in Randomized Controlled Trials of Medications Used to Treat Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2021, 27, 1541–1543. [Google Scholar] [CrossRef]
- Velonias, G.; Conway, G.; Andrews, E.; Garber, J.J.; Khalili, H.; Yajnik, V.; Ananthakrishnan, A.N. Older Age- and Health-related Quality of Life in Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2017, 23, 283–288. [Google Scholar] [CrossRef]
- Arnott, I.; Rogler, G.; Halfvarson, J. The Management of Inflammatory Bowel Disease in Elderly: Current Evidence and Future Perspectives. Inflamm. Intest. Dis. 2018, 2, 189–199. [Google Scholar] [CrossRef]
- Sousa, P.; Bertani, L.; Rodrigues, C. Management of inflammatory bowel disease in the elderly: A review. Dig. Liver Dis. 2023, 55, 1001–1009. [Google Scholar] [CrossRef]
- Hong, S.J.; Katz, S. The elderly IBD patient in the modern era: Changing paradigms in risk stratification and therapeutic management. Ther. Adv. Gastroenterol. 2021, 14, 17562848211023399. [Google Scholar] [CrossRef]
- Melmed, G.Y.; Oliver, B.; Hou, J.K.; Lum, D.; Singh, S.; Crate, D.; Almario, C.; Bray, H.; Bresee, C.; Gerich, M.; et al. Quality of care program reduces unplanned health care utilization in patients with inflammatory bowel disease. Am. J. Gastroenterol. 2021, 116, 2410–2418. [Google Scholar] [CrossRef]
- Aromataris, E.; Lockwood, C.; Porritt, K.; Pilla, B.; Jordan, Z. (Eds.) JBI Manual for Evidence Synthesis. 2024. Available online: https://synthesismanual.jbi.global (accessed on 10 June 2024).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software [Internet]. Available online: www.covidence.org (accessed on 10 June 2024).
- Katz, S.; Feldstein, R. Inflammatory bowel disease of the elderly: A wake-up call. Gastroenterol. Hepatol. 2008, 4, 337–347. [Google Scholar] [PubMed] [PubMed Central]
- Tao, Z.; Feng, Q.; Lisa, F. Quality of life and influencing factors in elderly patients with inflammatory bowel disease. World Chin. J. Dig. 2014, 23, 823–827. [Google Scholar]
- Long, M.D.; Kappelman, M.D.; Martin, C.F.; Chen, W.; Anton, K.; Sandler, R.S. Risk factors for depression in the elderly inflammatory bowel disease population. J. Crohns Colitis 2014, 8, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.C.; Sheng, L.; Benchimol, E.I. Health Care utilization in elderly onset inflammatory bowel disease: A population-based study. Inflamm. Bowel Dis. 2015, 21, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.H.; Ohno-Machado, L.; Sandborn, W.J.; Singh, S. Infections and cardiovascular complications are common causes for hospitalization in older patients with inflammatory bowel diseases. Inflamm. Bowel Dis. 2018, 24, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Older Persons [Internet]. United Nations High Commissioner for Refugees. 2024. Available online: https://emergency.unhcr.org/protection/persons-risk/older-persons (accessed on 11 June 2024).
- Munn, Z.; Stone, J.C.; Aromataris, E.; Klugar, M.; Sears, K.; Leonardi-Bee, J.; Barker, T.H. Assessing the risk of bias of quantitative analytical studies: Introducing the vision for critical appraisal within JBI systematic reviews. JBI Evid. Synth. 2023, 21, 467–471. [Google Scholar] [CrossRef]
- Adar, T.; Faleck, D.; Sasidharan, S.; Cushing, K.; Borren, N.Z.; Nalagatla, N.; Ungaro, R.; Sy, W.; Owen, S.C.; Patel, A.; et al. Comparative safety and effectiveness of tumor necrosis factor α antagonists and vedolizumab in elderly IBD patients: A multicentre study. Aliment. Pharmacol. Ther. 2019, 49, 873–879. [Google Scholar] [CrossRef]
- Alexakis, C.; Saxena, S.; Chhaya, V.; Cecil, E.; Curcin, V.; Pollok, R. Do thiopurines reduce the risk of surgery in elderly onset inflammatory bowel disease? A 20-year national population-based cohort study. Inflamm. Bowel Dis. 2017, 23, 672–680. [Google Scholar] [CrossRef]
- Amano, T.; Shinzaki, S.; Asakura, A.; Tashiro, T.; Tani, M.; Otake, Y.; Yoshihara, T.; Iwatani, S.; Yamada, T.; Sakakibara, Y.; et al. Elderly onset age is associated with low efficacy of first anti-tumor necrosis factor treatment in patients with inflammatory bowel disease. Sci. Rep. 2022, 12, 5324. [Google Scholar] [CrossRef]
- Asscher, V.E.R.; Waars, S.N.; van der Meulen-de Jong, A.E.; Stuyt, R.J.L.; Baven-Pronk, A.M.C.; van der Marel, S.; Jacobs, R.J.; Haans, J.J.L.; Meijer, L.J.; Klijnsma-Slagboom, J.D.; et al. Deficits in geriatric assessment associate with disease activity and burden in older patients with inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2022, 20, e1006–e1021. [Google Scholar] [CrossRef] [PubMed]
- Benchimol, E.I.; Cook, S.F.; Erichsen, R.; Long, M.D.; Bernstein, C.N.; Wong, J.; Carroll, C.F.; Frøslev, T.; Sampson, T.; Kappelman, M.D. International variation in medication prescription rates among elderly patients with inflammatory bowel disease. J. Crohns Colitis 2013, 7, 878–889. [Google Scholar] [CrossRef] [PubMed]
- Bollegala, N.; Jackson, T.D.; Nguyen, G.C. Increased postoperative mortality and complications among elderly patients with inflammatory bowel diseases: An analysis of the national surgical quality improvement program cohort. Clin. Gastroenterol. Hepatol. 2016, 14, 1274–1281. [Google Scholar] [CrossRef] [PubMed]
- Bozon, A.; Nancey, S.; Serrero, M.; Caillo, L.; Gilletta, C.; Benezech, A.; Combes, R.; Danan, G.; Akouete, S.; Pages, L.; et al. Risk of infection in elderly patients with inflammatory bowel disease under biologics: A prospective, multicenter, observational, one-year follow-up comparative study. Clin. Res. Hepatol. Gastroenterol. 2023, 47, 102107. [Google Scholar] [CrossRef] [PubMed]
- Casas-Deza, D.; Lamuela-Calvo, L.J.; Gomollón, F.; Arbonés-Mainar, J.M.; Caballol, B.; Gisbert, J.P.; Rivero, M.; Sánchez-Rodríguez, E.; Arias García, L.; Gutiérrez Casbas, A.; et al. Effectiveness and safety of Ustekinumab in elderly patients with Crohn’s disease: Real world evidence from the ENEIDA registry. J. Crohns Colitis 2023, 17, 83–91. [Google Scholar] [CrossRef]
- Charpentier, C.; Salleron, J.; Savoye, G.; Fumery, M.; Merle, V.; Laberenne, J.E.; Vasseur, F.; Dupas, J.L.; Cortot, A.; Dauchet, L.; et al. Natural history of elderly-onset inflammatory bowel disease: A population-based cohort study. Gut 2014, 63, 423–432. [Google Scholar] [CrossRef]
- Cheng, D.; Kochar, B.; Cai, T.; Ritchie, C.S.; Ananthakrishnan, A.N. Comorbidity influences the comparative safety of biologic therapy in older adults with inflammatory bowel diseases. Am. J. Gastroenterol. 2022, 117, 1845–1850. [Google Scholar] [CrossRef]
- Cohen, N.A.; Plevris, N.; Kopylov, U.; Grinman, A.; Ungar, B.; Yanai, H.; Leibovitzh, H.; Isakov, N.F.; Hirsch, A.; Ritter, E.; et al. Vedolizumab is effective and safe in elderly inflammatory bowel disease patients: A binational, multicenter, retrospective cohort study. United Eur. Gastroenterol. J. 2020, 8, 1076–1085. [Google Scholar] [CrossRef]
- de Jong, M.E.; Smits, L.J.T.; van Ruijven, B.; den Broeder, N.; Russel, M.G.V.M.; Römkens, T.E.H.; West, R.L.; Jansen, J.M.; Hoentjen, F. Increased discontinuation rates of anti-TNF therapy in elderly inflammatory bowel disease patients. J. Crohns Colitis 2020, 14, 888–895. [Google Scholar] [CrossRef]
- Desai, A.; Zator, Z.A.; de Silva, P.; Nguyen, D.D.; Korzenik, J.; Yajnik, V.; Ananthakrishnan, A.N. Older age is associated with higher rate of discontinuation of anti-TNF therapy in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2013, 19, 309–315. [Google Scholar] [CrossRef]
- Everhov, Å.H.; Halfvarson, J.; Myrelid, P.; Sachs, M.C.; Nordenvall, C.; Söderling, J.; Ekbom, A.; Neovius, M.; Ludvigsson, J.F.; Askling, J.; et al. Incidence and treatment of patients diagnosed with inflammatory bowel diseases at 60 years or older in Sweden. Gastroenterology 2018, 154, 518–528.e15. [Google Scholar] [CrossRef] [PubMed]
- Fumery, M.; Pariente, B.; Sarter, H.; Charpentier, C.; Armengol Debeir, L.; Dupas, J.L.; Coevoet, H.; Peyrin-Biroulet, L.; dʼAgay, L.; Gower-Rousseau, C.; et al. Natural history of crohn’s disease in elderly patients diagnosed over the age of 70 Years: A population-based study. Inflamm. Bowel Dis. 2016, 22, 1698–1707. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.; Aggarwal, M.; Butler, R.; Achkar, J.P.; Lashner, B.; Philpott, J.; Cohen, B.; Qazi, T.; Rieder, F.; Regueiro, M.; et al. Real-world effectiveness and safety of Ustekinumab in elderly Crohn’s disease patients. Dig. Dis. Sci. 2022, 67, 3138–3147. [Google Scholar] [CrossRef] [PubMed]
- Gebeyehu, G.G.; Fiske, J.; Liu, E.; Limdi, J.K.; Broglio, G.; Selinger, C.; Razsanskaite, V.; Smith, P.J.; Flanagan, P.K.; Subramanian, S. Ustekinumab and Vedolizumab are equally safe and effective in elderly Crohn’s disease patients. Dig. Dis. Sci. 2023, 68, 1983–1994. [Google Scholar] [CrossRef] [PubMed]
- Hahn, G.D.; LeBlanc, J.F.; Golovics, P.A.; Wetwittayakhlang, P.; Qatomah, A.; Wang, A.; Boodaghians, L.; Liu Chen Kiow, J.; Al Ali, M.; Wild, G.; et al. Effectiveness, safety, and drug sustainability of biologics in elderly patients with inflammatory bowel disease: A retrospective study. World, J. Gastroenterol. 2022, 28, 4823–4833. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.K.; Feagins, L.A.; Waljee, A.K. Characteristics and behavior of elderly-onset inflammatory bowel disease: A multi-center US study. Inflamm. Bowel Dis. 2016, 22, 2200–2205. [Google Scholar] [CrossRef]
- Huguet, J.M.; Iborra, M.; Bosca-Watts, M.M.; Maroto, N.; Gil, R.; Cortes, X.; Hervás, D.; Paredes, J.M. Inflammatory bowel disease in patients over the age of 70 y. Does the disease duration influence its behavior? Scand. J. Gastroenterol. 2018, 53, 1079–1084. [Google Scholar] [CrossRef]
- Jeuring, S.F.; van den Heuvel, T.R.; Zeegers, M.P.; Hameeteman, W.H.; Romberg-Camps, M.J.; Oostenbrug, L.E.; Masclee, A.A.; Jonkers, D.M.; Pierik, M.J. Epidemiology and long-term outcome of inflammatory bowel disease diagnosed at elderly age-an increasing distinct entity? Inflamm. Bowel Dis. 2016, 22, 1425–1434. [Google Scholar] [CrossRef]
- Juneja, M.; Baidoo, L.; Schwartz, M.B.; Barrie, A., 3rd; Regueiro, M.; Dunn, M.; Binion, D.G. Geriatric inflammatory bowel disease: Phenotypic presentation, treatment patterns, nutritional status, outcomes, and comorbidity. Dig. Dis. Sci. 2012, 57, 2408–2415. [Google Scholar] [CrossRef]
- Khan, N.; Pernes, T.; Weiss, A.; Trivedi, C.; Patel, M.; Medvedeva, E.; Xie, D.; Yang, Y.-X. Efficacy of Vedolizumab in a nationwide cohort of elderly inflammatory bowel disease patients. Inflamm. Bowel Dis. 2022, 28, 734–744. [Google Scholar] [CrossRef]
- Kuenzig, M.E.; Stukel, T.A.; Kaplan, G.G.; Murthy, S.K.; Nguyen, G.C.; Talarico, R.; Benchimol, E.I. Variation in care of patients with elderly-onset inflammatory bowel disease in Ontario, Canada: A population-based cohort study. J. Can. Assoc. Gastroenterol. 2020, 4, e16–e30. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Na, M.J.; Ye, B.D.; Cheon, J.H.; Im, J.P.; Kim, J.S.; CONNECT Study Group. Clinical characteristics of Korean patients with elderly-onset Crohn’s disease: Results from the prospective connect study. Gut Liver 2022, 16, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Kochar, B.; Jylhävä, J.; Söderling, J.; Ritchie, C.S.; SWIBREG Study Group; Ludvigsson, J.F.; Khalili, H.; Olén, O. Prevalence and implications of frailty in older adults with incident inflammatory bowel diseases: A Nationwide cohort study. Clin. Gastroenterol. Hepatol. 2022, 20, 2358–2365.e11. [Google Scholar] [CrossRef] [PubMed]
- Lobatón, T.; Ferrante, M.; Rutgeerts, P.; Ballet, V.; Van Assche, G.; Vermeire, S. Efficacy and safety of anti-TNF therapy in elderly patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2015, 42, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Mosli, M.H.; Alghamdi, M.K.; Bokhary, O.A.; Alzahrani, M.A.; Takieddin, S.Z.; Galai, T.A.; Alsahafi, M.A.; Saadah, O.I. Inflammatory bowel disease in the elderly: A focus on disease characteristics and treatment patterns. Saudi, J. Gastroenterol. 2023, 29, 212–218. [Google Scholar] [CrossRef]
- Nguyen, G.C.; Bernstein, C.N.; Benchimol, E.I. Risk of surgery and mortality in elderly-onset inflammatory bowel disease: A population-based cohort study. Inflamm. Bowel Dis. 2017, 23, 218–223. [Google Scholar] [CrossRef]
- Perera, L.P.; Bhandari, S.; Liu, R.; Guilday, C.; Zadvornova, Y.; Saeian, K.; Eastwood, D. Advanced age does not negatively impact health-related quality of life in inflammatory bowel disease. Dig. Dis. Sci. 2018, 63, 1787–1793. [Google Scholar] [CrossRef]
- Pugliese, D.; Privitera, G.; Crispino, F.; Mezzina, N.; Castiglione, F.; Fiorino, G.; Laterza, L.; Viola, A.; Bertani, L.; Caprioli, F.; et al. Effectiveness and safety of vedolizumab in a matched cohort of elderly and nonelderly patients with inflammatory bowel disease: The IG-IBD LIVE study. Aliment. Pharmacol. Ther. 2022, 56, 95–109. [Google Scholar] [CrossRef]
- Rozich, J.J.; Luo, J.; Dulai, P.S. Disease- and treatment-related complications in older patients with inflammatory bowel diseases: Comparison of adult-onset vs elderly-onset disease. Inflamm. Bowel Dis. 2021, 27, 1215–1223. [Google Scholar] [CrossRef]
- Rusher, A.; Araka, E.; Ananthakrishnan, A.N.; Ritchie, C.; Kochar, B. IBD Is Like a Tree: Reflections From Older Adults with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2024, izae139. [Google Scholar] [CrossRef]
- Shashi, P.; Gopalakrishnan, D.; Parikh, M.P.; Shen, B.; Kochhar, G. Efficacy and safety of vedolizumab in elderly patients with inflammatory bowel disease: A matched case-control study. Gastroenterol. Rep. 2019, 8, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.; Stein, D.J.; Lipcsey, M.; Li, B.; Feuerstein, J.D. High rates of mortality in geriatric patients admitted for inflammatory bowel disease management. J. Clin. Gastroenterol. 2022, 56, e20–e26. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhang, H.; Yang, H.; Zhang, M.; Qian, J. The incidence rate and risk factors of malignancy in elderly-onset inflammatory bowel disease: A Chinese cohort study from 1998 to 2020. Front. Oncol. 2021, 11, 788980. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; D’Arcy, M.; Barnes, E.L.; Freedman, N.D.; Engels, E.A.; Song, M. Associations of inflammatory bowel disease and subsequent cancers in a population-based study of older adults in the United States. JNCI Cancer Spectr. 2022, 6, pkab096. [Google Scholar] [CrossRef] [PubMed]
- National Council of Aging [Internet]. Get the Facts on Healthy Aging. 2023. Available online: https://www.ncoa.org/article/get-the-facts-on-healthy-aging (accessed on 3 July 2024).
- Khan, S.; Sebastian, S.A.; Parmar, M.P.; Ghadge, N.; Padda, I.; Keshta, A.S.; Minhaz, N.; Patel, A. Factors influencing the quality of life in inflammatory bowel disease: A comprehensive review. Dis. Mon. 2024, 70, 101672. [Google Scholar] [CrossRef]
- Kamp, K.; Holmstrom, A.; Luo, Z.; Wyatt, G.; Given, B. Factors Influencing Received Social Support Among Emerging Adults with Inflammatory Bowel Disease: A Cross-Sectional Study. Gastroenterol. Nurs. 2020, 43, 429–439. [Google Scholar] [CrossRef]
- Son, H.; Cho, H.J.; Cho, S.; Ryu, J.; Kim, S. The Moderating Effect of Social Support between Loneliness and Depression: Differences between the Young-Old and the Old-Old. Int. J. Environ. Res. Public Health 2022, 19, 2322. [Google Scholar] [CrossRef]
- Eder, P.; Niezgódka, A.; Krela-Kaźmierczak, I.; Stawczyk-Eder, K.; Banasik, E.; Dobrowolska, A. Dietary Support in Elderly Patients with Inflammatory Bowel Disease. Nutrients 2019, 11, 1421. [Google Scholar] [CrossRef]
- Mao, Y.; Xu, Y.; Fan, Y.; Lv, B.; Huang, X.; Liang, X. Advancements in malnutrition in elderly inflammatory bowel disease patients. Gastroenterol. Endosc. 2023, 1, 199–206. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).