
Selected Livestock-Associated Zoonoses as a Growing Challenge for Public Health

 , , , , and
, , , , and 
Abstract
:1. Background
2. Q Fever
3. Brucellosis
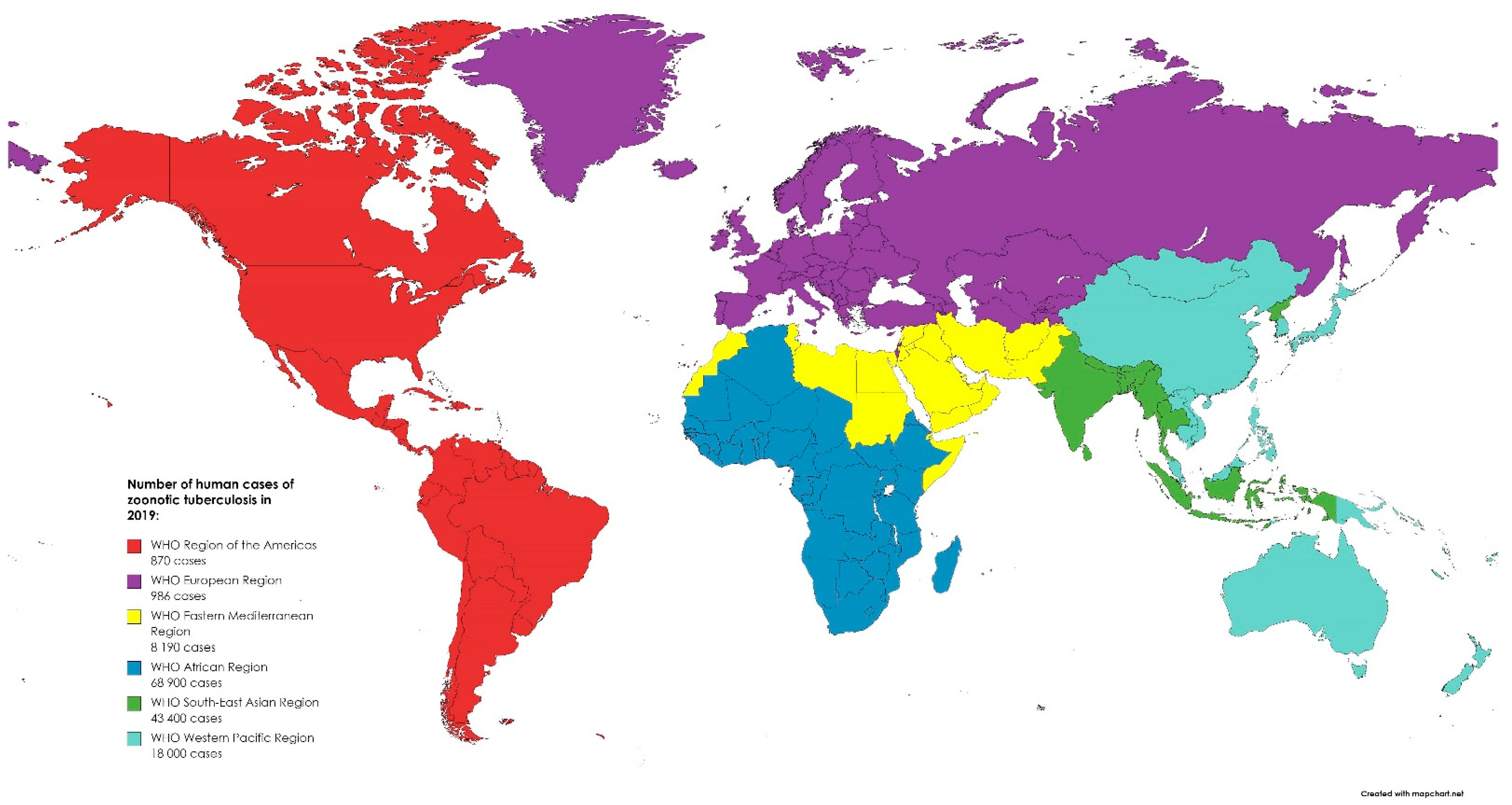
4. Tuberculosis Caused by Mycobacterium bovis and Mycobacterium caprae
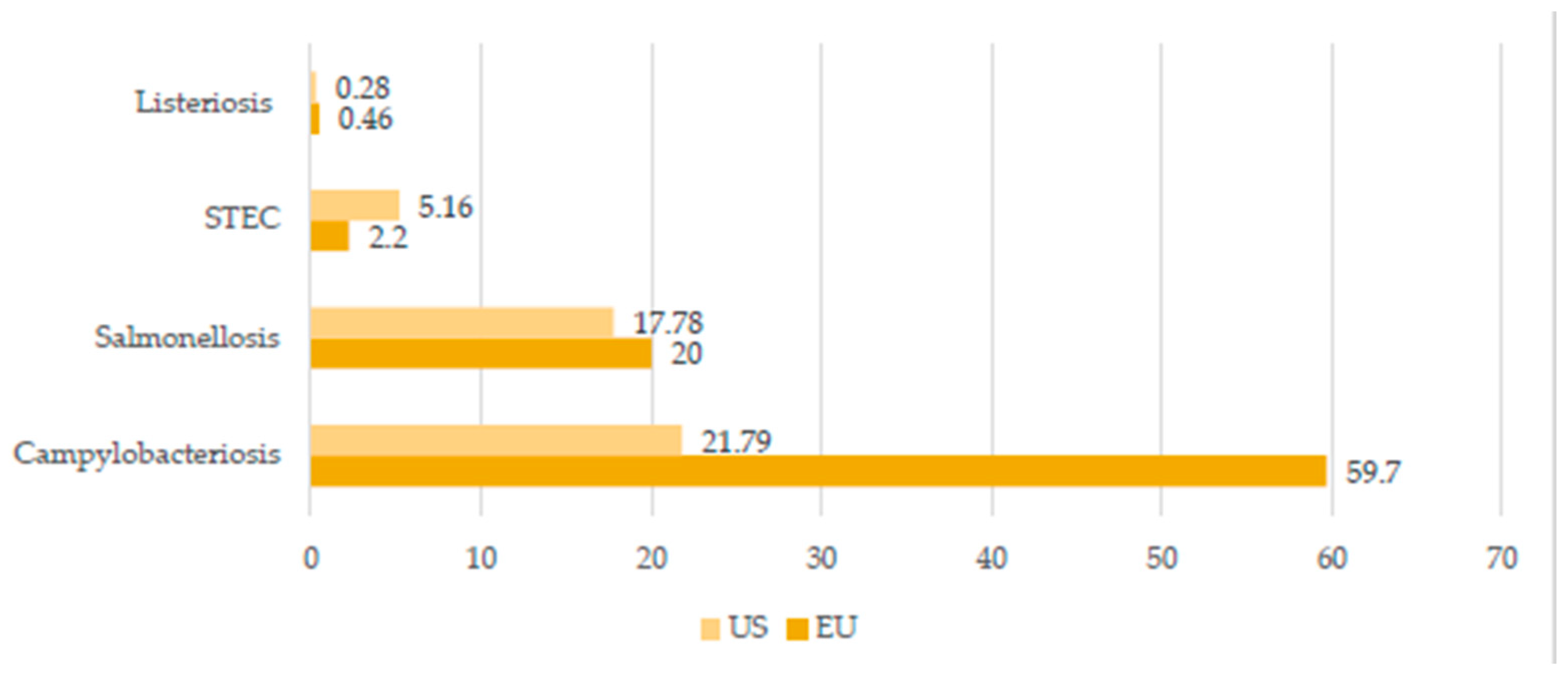
5. Shiga Toxin-Producing Escherichia coli (STEC)
6. Trichinellosis
7. Yersiniosis
8. Salmonellosis
9. Campylobacteriosis
10. Influenza
11. Listeriosis
12. Glanders
13. West Nile Fever
14. Melioidosis
15. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects 2019: Highlights (ST/ESA/SER.A/423); United Nations: New York, NY, USA, 2019. [Google Scholar]
- FAO. World Food and Agriculture—Statistical Yearbook 2021; FAO: Rome, Italy, 2021. [Google Scholar] [CrossRef]
- World Organization for Animal Health Official Website. Available online: https://www.oie.int/en/what-we-do/global-initiatives/one-health/ (accessed on 25 November 2021).
- Pomorska-Mól, M.; Włodarek, J.; Gogulski, M.; Rybska, M. Review: SARS-CoV-2 Infection in farmed minks—An overview of current knowledge on occurrence, disease and epidemiology. Animal 2021, 15, 100272. [Google Scholar] [CrossRef]
- European Food Safety Authority; European Centre for Disease Prevention and Control. The European Union One Health 2019 Zoonoses Report; EFS2; 2021; Volume 19, pp. 1–286. Available online: https://efsa.onlinelibrary.wiley.com/doi/full/10.2903/j.efsa.2021.6406 (accessed on 5 December 2021).
- Centers for Disease Control and Prevention Official Website. Available online: https://www.cdc.gov/onehealth/pdfs/us-ohzdp-report-508.pdf (accessed on 25 November 2021).
- Centers for Disease Control and Prevention. National Notifiable Diseases Surveillance System, 2019 Annual Tables of Infectious Disease Data; CDC Division of Health Informatics and Surveillance: Atlanta, GA, USA, 2021.
- Kemunto, N.; Mogoa, E.; Osoro, E.; Bitek, A.; Kariuki Njenga, M.; Thumbi, S.M. Zoonotic disease research in East Africa. BMC Infect. Dis. 2018, 18, 545. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Cao, L.; Zhu, X.-Q. Major emerging and re-emerging zoonoses in China: A matter of global health and socioeconomic development for 1.3 billion. Int. J. Infect. Dis. 2014, 25, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wille, M.; Geoghegan, J.L.; Holmes, E.C. How accurately can we assess zoonotic risk? PLoS Biol. 2021, 19, e3001135. [Google Scholar] [CrossRef] [PubMed]
- Belay, E.D.; Kile, J.C.; Hall, A.J.; Barton-Behravesh, C.; Parsons, M.B.; Salyer, S.; Walke, H. Zoonotic disease programs for enhancing global health security. Emerg. Infect. Dis. 2017, 23, S65. [Google Scholar] [CrossRef] [Green Version]
- Acharya, K.P.; Acharya, N.; Phuyal, S.; Upadhyaya, M.; Lasee, S. One-Health approach: A best possible way to control rabies. One Health 2020, 10, 100161. [Google Scholar] [CrossRef]
- Kruse, H.; Kirkemo, A.-M.; Handeland, K. Wildlife as source of zoonotic infections. Emerg. Infect. Dis. 2004, 10, 2067–2072. [Google Scholar] [CrossRef]
- Rocklöv, J.; Dubrow, R. Climate change: An enduring challenge for vector-borne disease prevention and control. Nat. Immunol. 2020, 21, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Eldin, C.; Mélenotte, C.; Mediannikov, O.; Ghigo, E.; Million, M.; Edouard, S.; Mege, J.-L.; Maurin, M.; Raoult, D. From Q fever to Coxiella burnetii infection: A paradigm change. Clin. Microbiol. Rev. 2017, 30, 115–190. [Google Scholar] [CrossRef] [Green Version]
- Amjadi, O.; Rafiei, A.; Mardani, M.; Zafari, P.; Zarifian, A. A review of the immunopathogenesis of brucellosis. Infect. Dis. 2019, 51, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Kozińska, M.; Krajewska-Wędzina, M.; Augustynowicz-Kopeć, E. Mycobacterium caprae—the first case of the human infection in Poland. Ann. Agric. Environ. Med. 2020, 27, 151–153. [Google Scholar] [CrossRef]
- World Health Organization; Food and Agriculture Organization of the United Nations. World Organisation for Animal Health Roadmap for Zoonotic Tuberculosis; World Health Organization: Geneva, Switzerland, 2017; ISBN 978-92-4-151304-3. [Google Scholar]
- Bilska-Zając, E.; Różycki, M.; Korpysa-Dzirba, W.; Bełcik, A.; Ziętek-Barszcz, A.; Włodarczyk-Ramus, M.; Gontarczyk, A.; Cencek, T. Trichinella outbreaks on pig farms in Poland in 2012–2020. Pathogens 2021, 10, 1504. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen-Ninios, R.; Fredriksson-Ahomaa, M.; Maijala, R.; Korkeala, H. High prevalence of pathogenic Yersinia enterocolitica in pig cheeks. Food Microbiol. 2014, 43, 50–52. [Google Scholar] [CrossRef]
- Smith, G.J.D.; Vijaykrishna, D.; Bahl, J.; Lycett, S.J.; Worobey, M.; Pybus, O.G.; Ma, S.K.; Cheung, C.L.; Raghwani, J.; Bhatt, S.; et al. Origins and evolutionary genomics of the 2009 swine-origin H1N1 influenza A epidemic. Nature 2009, 459, 1122–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, T.; Couceiro, J.N.S.S.; Kelm, S.; Baum, L.G.; Krauss, S.; Castrucci, M.R.; Donatelli, I.; Kida, H.; Paulson, J.C.; Webster, R.G.; et al. Molecular basis for the generation in pigs of influenza A viruses with pandemic potential. J. Virol. 1998, 72, 7367–7373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, K.P.; Olsen, C.W.; Setterquist, S.F.; Capuano, A.W.; Donham, K.J.; Thacker, E.L.; Merchant, J.A.; Gray, G.C. Are swine workers in the United States at increased risk of infection with zoonotic influenza virus? Clin. Infect. Dis. 2006, 42, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Popa, G.L.; Popa, M.I. Salmonella spp. infectio—A continuous threat worldwide. Germs 2021, 11, 88–96. [Google Scholar] [CrossRef]
- Roadmap to Reducing Salmonella Driving Change through Science-Based Policy; Food Safety the U.S. Department of Agriculture: Washington, DC, USA, 2020.
- Derrick, E.H. “Q” fever, a new fever entity: Clinical features, diagnosis and laboratory investigation. Med. J. Aust. 1937, 2, 281–299. [Google Scholar] [CrossRef]
- Miller, H.K.; Priestley, R.A.; Kersh, G.J. Transmission of Coxiella burnetii by ingestion in mice. Epidemiol. Infect. 2020, 148, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Pechstein, J.; Schulze-Luehrmann, J.; Lührmann, A. Coxiella burnetii as a useful tool to investigate bacteria-friendly host cell compartments. Int. J. Med. Microbiol. Suppl. 2018, 308, 77–83. [Google Scholar] [CrossRef]
- España, P.P.; Uranga, A.; Cillóniz, C.; Torres, A. Q fever (Coxiella burnetii). Semin. Respir. Crit. Care. Med. 2020, 41, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Kersh, G.J.; Priestley, R.; Massung, R.F. Stability of Coxiella burnetii in stored human blood: C. burnetii stability in blood. Transfusion 2013, 53, 1493–1496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Signs, K.A.; Stobierski, M.G.; Gandhi, T.N. Q fever cluster among raw milk drinkers in Michigan, 2011. Clin. Infect. Dis. 2012, 55, 1387–1389. [Google Scholar] [CrossRef] [Green Version]
- Angelakis, E.; Raoult, D. Q fever. Vet. Microbiol. 2010, 140, 297–309. [Google Scholar] [CrossRef] [Green Version]
- Epelboin, L.; Chesnais, C.; Boulle, C.; Drogoul, A.-S.; Raoult, D.; Djossou, F.; Mahamat, A. Q fever pneumonia in French Guiana: Prevalence, Risk Factors, and Prognostic Score. Clin. Infect. Dis. 2012, 55, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Galińska, E.M.; Zagórski, J. Brucellosis in humans—Etiology, diagnostics, clinical forms. Ann. Agric. Environ. Med. 2013, 20, 6. [Google Scholar]
- Franco, M.P.; Mulder, M.; Gilman, R.H.; Smits, H.L. Human brucellosis. Lancet Infect. Dis. 2007, 7, 775–786. [Google Scholar] [CrossRef]
- Głowacka, P.; Żakowska, D.; Naylor, K.; Niemcewicz, M.; Bielawska-Drózd, A. Brucella—virulence factors, pathogenesis and treatment. Pol. J. Microbiol. 2018, 67, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Rubach, M.P.; Halliday, J.E.B.; Cleaveland, S.; Crump, J.A. Brucellosis in low-income and middle-income countries. Curr. Opin. Infect. Dis. 2013, 26, 404–412. [Google Scholar] [CrossRef] [Green Version]
- Tuon, F.F.; Gondolfo, R.B.; Cerchiari, N. Human-to-human transmission of Brucella—A systematic review. Trop. Med. Int. Health 2017, 22, 539–546. [Google Scholar] [CrossRef] [Green Version]
- Hull, N.C.; Schumaker, B.A. Comparisons of Brucellosis between human and veterinary medicine. Infect. Ecol. Epidemiol. 2018, 8, 1500846. [Google Scholar] [CrossRef]
- Awah-Ndukum, J.; Mouiche, M.M.M.; Kouonmo-Ngnoyum, L.; Bayang, H.N.; Manchang, T.K.; Poueme, R.S.N.; Kouamo, J.; Ngu-Ngwa, V.; Assana, E.; Feussom, K.J.M.; et al. Seroprevalence and risk factors of brucellosis among slaughtered indigenous cattle, abattoir personnel and pregnant women in Ngaoundéré, Cameroon. BMC Infect. Dis. 2018, 18, 611. [Google Scholar] [CrossRef] [Green Version]
- Mai, H.M.; Irons, P.C.; Kabir, J.; Thompson, P.N. A large seroprevalence survey of brucellosis in cattle herds under diverse production systems in Northern Nigeria. BMC Vet. Res. 2012, 8, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, R.; Xie, S.; Lu, X.; Sun, L.; Zhou, Y.; Zhang, Y.; Wang, K. A systematic review and meta-analysis of epidemiology and clinical manifestations of human brucellosis in China. BioMed Res. Int. 2018, 2018, 5712920. [Google Scholar] [CrossRef] [PubMed]
- Prodinger, W.M.; Indra, A.; Koksalan, O.K.; Kilicaslan, Z.; Richter, E. Mycobacterium caprae infection in humans. Expert Rev. Anti Infect. Ther. 2014, 12, 1501–1513. [Google Scholar] [CrossRef] [PubMed]
- Kaneene, J.B.; Miller, R.; de Kantor, I.N.; Thoen, C.O. Tuberculosis in wild animals. Int. J. Tuberc. Lung Dis. 2010, 14, 1508–1512. [Google Scholar] [PubMed]
- Khan, M.; Islam, M.M.; Ferdous, J.; Alam, M. An overview on epidemiology of tuberculosis. Mymensingh Med. J. 2019, 28, 259–266. [Google Scholar]
- El-Sayed, A.; El-Shannat, S.; Kamel, M.; Castañeda-Vazquez, M.A.; Castañeda-Vazquez, H. Molecular epidemiology of Mycobacterium bovis in humans and cattle. Zoonoses Public Health 2016, 63, 251–264. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Michel, A.L.; Müller, B.; van Helden, P.D. Mycobacterium bovis at the animal–human interface: A problem, or not? Vet. Microbiol. 2010, 140, 371–381. [Google Scholar] [CrossRef] [Green Version]
- Grange, J.M. Mycobacterium bovis infection in human beings. Tuberculosis 2001, 81, 71–77. [Google Scholar] [CrossRef]
- Jalava, K.; Jones, J.A.; Goodchild, T.; Clifton-Hadley, R.; Mitchell, A.; Story, A.; Watson, J.M. No increase in human cases of Mycobacterium bovis disease despite resurgence of infections in cattle in the United Kingdom. Epidemiol. Infect. 2007, 135, 40–45. [Google Scholar] [CrossRef]
- Palmer, M.V. Mycobacterium bovis: Characteristics of wildlife reservoir hosts. Transbound. Emerg. Dis. 2013, 60, 1–13. [Google Scholar] [CrossRef] [PubMed]
- De Lisle, G.W.; Schlundt, J.; Schmitt, S.M.; O’Brien, D.J. Tuberculosis in free-ranging wildlife: Detection, diagnosis and management. Rev. Sci. Tech. OIE 2002, 21, 317–334. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, L.M.; Daborn, C.J. The epidemiology of Mycobacterium bovis infections in animals and man: A review. Tuberc. Lung Dis. 1995, 76, 1–46. [Google Scholar] [CrossRef]
- Karmali, M.A.; Gannon, V.; Sargeant, J.M. Verocytotoxin-producing Escherichia coli (VTEC). Vet. Microbiol. 2010, 140, 360–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, R.; Shao, K.; Yang, X.; Bai, X.; Fu, S.; Sun, H.; Xu, Y.; Wang, H.; Li, Q.; Hu, B.; et al. High prevalence of non-O157 shiga toxin-producing Escherichia coli in beef cattle detected by combining four selective agars. BMC Microbiol. 2019, 19, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Persad, A.K.; LeJeune, J.T. Animal reservoirs of shiga toxin-producing Escherichia coli. Microbiol. Spectr. 2015, 2, 211–230. [Google Scholar] [CrossRef]
- Gonzalez, A.; Cerqueira, A. Shiga toxin-producing Escherichia Coli in the animal reservoir and food in Brazil. J. Appl. Microbiol. 2020, 128, 1568–1582. [Google Scholar] [CrossRef] [Green Version]
- Hussein, H.S.; Sakuma, T. Prevalence of shiga toxin-producing Escherichia coli in dairy cattle and their products. J. Dairy Sci. 2005, 88, 450–465. [Google Scholar] [CrossRef] [Green Version]
- Ballem, A.; Gonçalves, S.; Garcia-Meniño, I.; Flament-Simon, S.C.; Blanco, J.E.; Fernandes, C.; Saavedra, M.J.; Pinto, C.; Oliveira, H.; Blanco, J.; et al. Prevalence and serotypes of shiga toxin-producing Escherichia coli (STEC) in dairy cattle from northern Portugal. PLoS ONE 2020, 15, e0244713. [Google Scholar] [CrossRef]
- Tack, D.M.; Kisselburgh, H.M.; Richardson, L.C.; Geissler, A.; Griffin, P.M.; Payne, D.C.; Gleason, B.L. Shiga toxin-producing Escherichia coli outbreaks in the United States, 2010–2017. Microorganisms 2021, 9, 1529. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Oh, K.-H.; Cho, S.-H.; Kim, S.-H.; Lee, B.-K.; Yoo, S.-J.; Lim, H.-S.; Park, M.-S. Anti-shiga toxin immunoglobulin G antibodies in healthy South Korean slaughterhouse workers. Scand. J. Infect. Dis. 2012, 44, 168–173. [Google Scholar] [CrossRef]
- Bai, X.; Wang, H.; Xin, Y.; Wei, R.; Tang, X.; Zhao, A.; Sun, H.; Zhang, W.; Wang, Y.; Xu, Y.; et al. Prevalence and characteristics of shiga toxin-producing Escherichia coli isolated from retail raw meats in China. Int. J. Food Microbiol. 2015, 200, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Morales, M.A.; Ludovisi, A.; Amati, M.; Cherchi, S.; Tonanzi, D.; Pozio, E. Differentiation of Trichinella species (Trichinella spiralis/Trichinella britovi versus Trichinella pseudospiralis) using western blot. Parasites Vectors 2018, 11, 631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pozio, E. Searching for Trichinella: Not all pigs are created equal. Trends Parasitol. 2014, 30, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Faber, M.; Schink, S.; Mayer-Scholl, A.; Ziesch, C.; Schonfelder, R.; Wichmann-Schauer, H.; Stark, K.; Nockler, K. Outbreak of trichinellosis due to wild boar meat and evaluation of the effectiveness of post exposure prophylaxis, Germany, 2013. Clin. Infect. Dis. 2015, 60, e98–e104. [Google Scholar] [CrossRef]
- Gottstein, B.; Pozio, E.; Nöckler, K. Epidemiology, diagnosis, treatment, and control of trichinellosis. Clin. Microbiol. Rev. 2009, 22, 127–145. [Google Scholar] [CrossRef] [Green Version]
- Bilska-Zajac, E.; Tonanzi, D.; Pozio, E.; Rozycki, M.; Cencek, T.; Thompson, P.C.; Rosenthal, B.M.; La Rosa, G. Genetic evidence substantiates transmission of Trichinella spiralis from one swine farm to another. Parasites Vectors 2021, 14, 359. [Google Scholar] [CrossRef] [PubMed]
- Severini, S.; Fenoglio, L.M.; Giraudo, A. Atypical case of trichinellosis. Am. J. Med. Sci. 2014, 348, 347. [Google Scholar] [CrossRef]
- Pozio, E.; Zarlenga, D.S. New pieces of the Trichinella puzzle. Int. J. Parasitol. 2013, 43, 983–997. [Google Scholar] [CrossRef]
- Vieira-Pinto, M.; Fernandes, A.R.G.; Santos, M.H.; Marucci, G. Trichinella britovi infection in wild boar in Portugal. Zoonoses Public Health 2021, 68, 103–109. [Google Scholar] [CrossRef]
- Commission Implementing Regulations (EU) 2015/1375; European Commision: Brussels, Belgium, 2015.
- Bottone, E.J. Yersinia enterocolitica: The charisma continues. Clin. Microbiol. Rev. 1997, 10, 20. [Google Scholar]
- Drummond, N.; Murphy, B.P.; Ringwood, T.; Prentice, M.B.; Buckley, J.F.; Fanning, S. Yersinia enterocolitica: A brief review of the issues relating to the zoonotic pathogen, public health challenges, and the pork production chain. Foodborne Pathog. Dis. 2012, 9, 179–189. [Google Scholar] [CrossRef]
- Fredriksson-Ahomaa, M.; Bucher, M.; Hank, C.; Stolle, A.; Korkeala, H. High prevalence of Yersinia enterocolitica 4:O3 on pig offal in Southern Germany: A slaughtering technique problem. Syst. Appl. Microbiol. 2001, 24, 457–463. [Google Scholar] [CrossRef]
- Schaake, J.; Drees, A.; Grüning, P.; Uliczka, F.; Pisano, F.; Thiermann, T.; von Altrock, A.; Seehusen, F.; Valentin-Weigand, P.; Dersch, P. Essential role of invasion for colonization and persistence of Yersinia enterocolitica in its natural reservoir host, the pig. Infect. Immun. 2014, 82, 960–969. [Google Scholar] [CrossRef] [Green Version]
- Tauxe, R.V.; Wauters, G.; Goossens, V.; Noyen, R.V.; Vandepitte, J.; Martin, S.M.; Mol, P.D.; Thiers, G. Yersinia enterocolitica infections and pork: The missing link. Lancet 1987, 329, 1129–1132. [Google Scholar] [CrossRef]
- Le Guern, A.-S.; Martin, L.; Savin, C.; Carniel, E. Yersiniosis in France: Overview and potential sources of infection. Int. J. Infect. Dis. 2016, 46, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espenhain, L.; Riess, M.; Müller, L.; Colombe, S.; Ethelberg, S.; Litrup, E.; Jernberg, C.; Kühlmann-Berenzon, S.; Lindblad, M.; Hove, N.K.; et al. Cross-border outbreak of Yersinia enterocolitica O3 associated with imported fresh spinach, Sweden and Denmark, March 2019. Eurosurveillance 2019, 24, 1900368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eden, K.V.; Rosenberg, M.L.; Stoopler, M.; Wood, B.T.; Highsmith, A.K.; Skaliy, P.; Wells, J.G.; Feeley, J.C. Waterborne gastrointestinal illness at a ski resort. Public Health Rep. 1977, 92, 245. [Google Scholar] [PubMed]
- Chlebicz, A.; Śliżewska, K. Campylobacteriosis, salmonellosis, yersiniosis, and listeriosis as zoonotic foodborne diseases: A review. Ont. J. Environ. Res. Public Health 2018, 15, 863. [Google Scholar] [CrossRef] [Green Version]
- Duan, R.; Liang, J.; Zhang, J.; Chen, Y.; Wang, J.; Tong, J.; Guo, B.; Hu, W.; Wang, M.; Zhao, J.; et al. Prevalence of Yersinia enterocolitica bioserotype 3/O:3 among children with diarrhea, China, 2010–2015. Emerg. Infect. Dis. 2017, 23, 1502–1509. [Google Scholar] [CrossRef] [Green Version]
- Jajere, S.M. A review of Salmonella enterica with particular focus on the pathogenicity and virulence factors, host specificity and antimicrobial resistance including multidrug resistance. Vet. World 2019, 12, 504–521. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; He, Y.; Mann, D.A.; Deng, X. Global spread of Salmonella enteritidis via centralized sourcing and international trade of poultry breeding stocks. Nat. Commun. 2021, 12, 5109. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Official Website. Influenza (Avian and Other Zoonotic). Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(avian-and-other-zoonotic) (accessed on 25 November 2021).
- Kurtz, J.R.; Goggins, J.A.; McLachlan, J.B. Salmonella infection: Interplay between the bacteria and host immune system. Immunol. Lett. 2017, 190, 42–50. [Google Scholar] [CrossRef]
- Stanaway, J.D.; Parisi, A.; Sarkar, K.; Blacker, B.F.; Reiner, R.C.; Hay, S.I.; Nixon, M.R.; Dolecek, C.; James, S.L.; Mokdad, A.H.; et al. The global burden of non-typhoidal Salmonella invasive disease: A systematic analysis for the global burden of disease study 2017. Lancet Infect. Dis. 2019, 19, 1312–1324. [Google Scholar] [CrossRef] [Green Version]
- Upton, M. Scale and structures of the poultry sector and factors inducing change: Intercountry differences and expected trends. In Poultry in the 21st Century: Avian Influenza and Beyond; FAO: Rome, Italy, 2007; Volume 36. [Google Scholar]
- Kim, S.-H.; Chelliah, R.; Ramakrishnan, S.R.; Perumal, A.S.; Bang, W.-S.; Rubab, M.; Daliri, E.B.-M.; Barathikannan, K.; Elahi, F.; Park, E.; et al. Review on stress tolerance in Campylobacter jejuni. Front. Cell. Infect. Microbiol. 2021, 10, 596570. [Google Scholar] [CrossRef]
- Myintzaw, P.; Jaiswal, A.K.; Jaiswal, S. A Review on campylobacteriosis associated with poultry meat consumption. Food Rev. Int. 2021, 2021, 1–15. [Google Scholar] [CrossRef]
- Silva, J.; Leite, D.; Fernandes, M.; Mena, C.; Gibbs, P.A.; Teixeira, P. Campylobacter spp. as a foodborne pathogen: A review. Front. Microbiol. 2011, 2, 200. [Google Scholar] [CrossRef] [Green Version]
- Wyszyńska, A.K.; Godlewska, R. Lactic Acid Bacteria—A promising tool for controlling chicken Campylobacter infection. Front. Microbiol. 2021, 12, 703441. [Google Scholar] [CrossRef] [PubMed]
- Hakeem, M.J.; Lu, X. Survival and control of Campylobacter in poultry production rnvironment. Front. Cell. Infect. Microbiol. 2021, 10, 615049. [Google Scholar] [CrossRef] [PubMed]
- Kürekci, C.; Sakin, F.; Epping, L.; Knüver, M.-T.; Semmler, T.; Stingl, K. Characterization of Campylobacter spp. strains isolated from wild birds in turkey. Front. Microbiol. 2021, 12, 712106. [Google Scholar] [CrossRef]
- Haimesaat, M.M.; Backert, S.; Alter, T.; Bereswill, S. Human campylobacteriosis—A serious infectious threat in a One Health perspective. Curr. Top. Microbiol. Immunol. 2021, 431, 1. [Google Scholar] [CrossRef]
- Guo, J.; Song, W.; Ni, X.; Liu, W.; Wu, J.; Xia, W.; Zhou, X.; Wang, W.; He, F.; Wang, X.; et al. Pathogen change of avian influenza virus in the live poultry market before and after vaccination of poultry in southern China. Virol. J. 2021, 18, 213. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Wang, Y.; Liu, H.; Guo, F.; Doi, S.A.; Smith, C.; Clements, A.C.A.; Edwards, J.; Huang, B.; Soares Magalhães, R.J. Effectiveness of market-level biosecurity at reducing exposure of poultry and humans to avian influenza: A systematic review and meta-analysis. J. Infect. Dis. 2018, 218, 1861–1875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urbaniak, K.; Markowska-Daniel, I.; Kowalczyk, A.; Kwit, K.; Pomorska-Mól, M.; Frącek, B.; Pejsak, Z. Reassortment process after co-infection of pigs with avian H1N1 and swine H3N2 influenza viruses. BMC Vet. Res. 2017, 13, 215. [Google Scholar] [CrossRef] [Green Version]
- Turlewicz-Podbielska, H.; Pomorska-Mól, M. Swine diseases caused by circoviruses and swine influenza according to data from the 11th European Symposium of Porcine Health Management (ESPHM) in Utrecht. Życie Wet. 2019, 94, 804–809. [Google Scholar]
- World Health Organization Official Website. Influenza A (H1N1) Outbreak. Available online: https://www.who.int/emergencies/situations/influenza-a-(h1n1)-outbreak (accessed on 1 December 2021).
- Chastagner, A.; Enouf, V.; Peroz, D.; Hervé, S.; Lucas, P.; Quéguiner, S.; Gorin, S.; Beven, V.; Behillil, S.; Leneveu, P.; et al. Bidirectional human–swine transmission of seasonal influenza A(H1N1)Pdm09 virus in pig herd, France, 2018. Emerg. Infect. Dis. 2019, 25, 1940–1943. [Google Scholar] [CrossRef] [Green Version]
- Gray, G.C.; McCarthy, T.; Capuano, A.W.; Setterquist, S.F.; Olsen, C.W.; Alavanja, M.C.; Lynch, C.F. Swine workers and swine influenza virus infections. Emerg. Infect. Dis. 2007, 13, 1871–1878. [Google Scholar] [CrossRef]
- Alexander, D.J.; Brown, I.H. Recent zoonoses caused by influenza A viruses. Rev. Sci. Tech. OIE 2000, 19, 197–225. [Google Scholar] [CrossRef]
- Tang, J.W.; Shetty, N.; Lam, T.T.-Y. Features of the new pandemic influenza A/H1N1/2009 virus: Virology, epidemiology, clinical and public health aspects. Curr. Opin. Pulm. Med. 2010, 16, 235–241. [Google Scholar] [CrossRef]
- Mancera Gracia, J.C.; Pearce, D.S.; Masic, A.; Balasch, M. Influenza A virus in swine: Epidemiology, challenges and vaccination strategies. Front. Vet. Sci. 2020, 7, 647. [Google Scholar] [CrossRef]
- Ma, W. Swine influenza virus: Current status and challenge. Virus Res. 2020, 288, 198118. [Google Scholar] [CrossRef] [PubMed]
- Saunders-Hastings, P.; Crispo, J.A.G.; Sikora, L.; Krewski, D. Effectiveness of personal protective measures in reducing pandemic influenza transmission: A systematic review and meta-analysis. Epidemics 2017, 20, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.Y.; Cowling, B.J.; Aiello, A.E. Hand hygiene and risk of influenza virus infections in the community: A systematic review and meta-analysis. Epidemiol. Infect. 2014, 142, 922–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayim-Akonor, M.; Mertens, E.; May, J.; Harder, T. Exposure of domestic swine to influenza A viruses in Ghana suggests unidirectional, reverse zoonotic transmission at the human–animal interface. Zoonoses Public Health 2020, 67, 697–707. [Google Scholar] [CrossRef]
- Diriba, K.; Awulachew, E.; Diribsa, K. The prevalence of Listeria species in different food items of animal and plant origin in Ethiopia: A systematic review and meta-analysis. Eur. J. Med. Res. 2021, 26, 60. [Google Scholar] [CrossRef]
- Lopes-Luz, L.; Mendonça, M.; Bernardes Fogaça, M.; Kipnis, A.; Bhunia, A.K.; Bührer-Sékula, S. Listeria monocytogenes: Review of pathogenesis and virulence determinants—Targeted immunological assays. Crit. Rev. Microbiol. 2021, 47, 647–666. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Tao, X.; Liu, S.; Zhao, Y.; Yang, X. An update review on Listeria infection in pregnancy. Infect. Drug Resist. 2021, 14, 1967–1978. [Google Scholar] [CrossRef]
- Buchanan, R.L.; Gorris, L.G.M.; Hayman, M.M.; Jackson, T.C.; Whiting, R.C. A Review of Listeria monocytogenes: An update on outbreaks, virulence, dose-response, ecology, and risk assessments. Food Control 2017, 75, 1–13. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Cloutier, A.K.; Rozak, D.A.; Khan, M.S.; Niwa, H.; Uchida-Fujii, E.; Katayama, Y.; Tuanyok, A. A novel selective medium for the isolation of Burkholderia mallei from equine specimens. BMC Vet. Res. 2019, 15, 133. [Google Scholar] [CrossRef] [Green Version]
- Khan, I.; Wieler, L.H.; Melzer, F.; Elschner, M.C.; Muhammad, G.; Ali, S.; Sprague, L.D.; Neubauer, H.; Saqib, M. Glanders in animals: A review on epidemiology, clinical presentation, diagnosis and countermeasures: Glanders in solipeds. Transbound. Emerg. Dis. 2013, 60, 204–221. [Google Scholar] [CrossRef] [PubMed]
- Kettle, A.N.B.; Wernery, U. Glanders and the risk for its introduction through the international movement of horses. Equine Vet. J. 2016, 48, 654–658. [Google Scholar] [CrossRef] [PubMed]
- Van Zandt, K.E.; Greer, M.T.; Gelhaus, H.C. Glanders: An overview of infection in humans. Orphanet J. Rare. Dis. 2013, 8, 131. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, H.N.; Smith, M.E.; Hayoun, M.A. Glanders and Melioidosis; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Rossi, S.L.; Ross, T.M.; Evans, J.D. West Nile Virus. Clin. Lab. Med. 2010, 30, 47–65. [Google Scholar] [CrossRef]
- Hadfield, J.; Brito, A.F.; Swetnam, D.M.; Vogels, C.B.F.; Tokarz, R.E.; Andersen, K.G.; Smith, R.C.; Bedford, T.; Grubaugh, N.D. Twenty years of West Nile Virus spread and evolution in the Americas visualized by Nextstrain. PLoS Pathog. 2019, 15, e1008042. [Google Scholar] [CrossRef] [Green Version]
- McVey, D.S.; Wilson, W.C.; Gay, C.G. West Nile Virus. Rev. Sci. Tech. Off. Int. Epizoot. 2015, 34, 431–439. [Google Scholar] [CrossRef]
- Simulundu, E.; Ndashe, K.; Chambaro, H.M.; Squarre, D.; Reilly, P.M.; Chitanga, S.; Changula, K.; Mukubesa, A.N.; Ndebe, J.; Tembo, J.; et al. West Nile Virus in farmed crocodiles, Zambia, 2019. Emerg. Infect. Dis. 2020, 26, 811–814. [Google Scholar] [CrossRef]
- Sule, W.F.; Oluwayelu, D.O.; Hernández-Triana, L.M.; Fooks, A.R.; Venter, M.; Johnson, N. Epidemiology and ecology of West Nile Virus in sub-saharan Africa. Parasites Vectors 2018, 11, 414. [Google Scholar] [CrossRef] [Green Version]
- Moniuszko-Malinowska, A.; Czupryna, P.; Dunaj, J.; Zajkowska, J.; Siemieniako, A.; Pancewicz, S. Zakażenia wirusem zachodniego Nilu i Usutu—Zagrożenie występowaniem w Polsce. Prz. Epidemiol. 2016, 70, 99–102. [Google Scholar]
- Papa, A. West Nile Virus Infections in Humans—Focus on Greece. J. Clin. Virol. 2013, 58, 351–353. [Google Scholar] [CrossRef] [PubMed]
- Limmathurotsakul, D.; Thammasart, S.; Warrasuth, N.; Thapanagulsak, P.; Jatapai, A.; Pengreungrojanachai, V.; Anun, S.; Joraka, W.; Thongkamkoon, P.; Saiyen, P.; et al. Melioidosis in animals, Thailand, 2006–2010. Emerg. Infect. Dis. 2012, 18, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Sprague, L.D.; Neubauer, H. Melioidosis in animals: A review on epizootiology, diagnosis and clinical presentation. J. Vet. Med. Ser. B 2004, 51, 305–320. [Google Scholar] [CrossRef] [PubMed]
- Chakravorty, A.; Heath, C.H. Melioidosis: An updated review. Aust. J. Gen. Pract. 2019, 48, 327–332. [Google Scholar] [CrossRef]
- Virk, H.S.; Mukhopadhyay, C.; Wiersinga, W.J. Melioidosis: A neglected cause of community-acquired pneumonia. Semin. Respir. Crit. Care Med. 2020, 41, 496–508. [Google Scholar] [CrossRef]
- Le Tohic, S.; Montana, M.; Koch, L.; Curti, C.; Vanelle, P. A review of melioidosis cases imported into Europe. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1395–1408. [Google Scholar] [CrossRef]
- Gassiep, I.; Armstrong, M.; Norton, R. Human melioidosis. Clin. Microbiol. Rev. 2020, 33, 6–19. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Disease | Aetiological Agent | Human Symptoms | Transmission Route | Epidemiology | References |
|---|---|---|---|---|---|
| Q fever | Coxiellaburnetti | Self-limited febrile illness, pneumonia, hepatitis, and endocarditis | Inhalation of aerosolized bacteria, ingestion, transfusion of blood, and sexual transmission | EU—950 human cases in 2019 USA—178 human cases in 2019 | [5] [6] [15] |
| Brucellosis | Brucellaabortus, B. melitensis, B. canis, B. suis | Systematic syndrome (fever, sweat, chills, and fatigue), located presentations (epididymoorchitis and spondylodiscitis), neurobrucellosis, and endocarditis | Contaminated food and dairy products, occupational contact, and inhalation | World—around 500,000 human cases per year EU—310 human cases in 2019 USA—80–120 cases annually | [5] [6] [16] |
| Tuberculosis | Mycobacterium bovis M. caprae | Generalized symptoms (fever, fatigue, arthralgia, and muscle pain), respiratory and cardiac complications, hepatitis, osteoarthritis, central nervous system dysfunction, and orchitis/epididymitis | Inhalation of aerosol, infected milk, dairy products, and meat | EU—147 human cases in 2019 USA—7174 human cases in 2020 | [5] [17] [18] |
| Trichinellosis | Trichinella sp. | Diarrhea, abdominal pain at first, fever, myalgia, myocarditis, facial oedemas, and encephalitis | Ingestion of raw or undercooked muscle tissue containing encysted larvae | EU—96 human cases in 2019 USA—90 human cases during 2008–2012 | [5] [6] [19] |
| Yersiniosis | Yersinia enterocolitica, Y. pseudotuberculosis | Fever, vomiting, abdominal pain, and bloody diarrhea | Eating raw or undercooked pork; ingestion of dairy products, seafood, and vegetables; or drinking contaminated water | EU—6961 human cases USA—nearly 117,000 illnesses per year | [5] [6] [20] |
| Swine influenza | Swine influenza virus (SIV) | Sneezing, coughing, difficult breathing, fever, lethargy, and decreased appetite | Contact with respiratory discharges or inhalation of exhalated aerosol by sick pig | No specific epidemiological data available, spread worldwide | [21] [22] [23] |
| Salmonellosis | Salmonella sp. | Acute enterocolitis accompanied by inflammatory diarrhea, abdominal pain, fever, nausea, and vomiting | Ingestion of uncooked contaminated foods (eggs, milk, and meat), drinking contaminated water, direct contact with infected animals, their feces and environment, and human-to-human transmission through fecal–oral route | EU—87,923 human cases in 2019 USA—about 1.35 million human illnesses per year Sub-Saharan Africa—535,500 cases of non-typhoidal salmonellosis in 2019 | [5] [6] [24] [25] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Libera, K.; Konieczny, K.; Grabska, J.; Szopka, W.; Augustyniak, A.; Pomorska-Mól, M. Selected Livestock-Associated Zoonoses as a Growing Challenge for Public Health. Infect. Dis. Rep. 2022, 14, 63-81. https://doi.org/10.3390/idr14010008
Libera K, Konieczny K, Grabska J, Szopka W, Augustyniak A, Pomorska-Mól M. Selected Livestock-Associated Zoonoses as a Growing Challenge for Public Health. Infectious Disease Reports. 2022; 14(1):63-81. https://doi.org/10.3390/idr14010008
Chicago/Turabian StyleLibera, Kacper, Kacper Konieczny, Julia Grabska, Wiktoria Szopka, Agata Augustyniak, and Małgorzata Pomorska-Mól. 2022. "Selected Livestock-Associated Zoonoses as a Growing Challenge for Public Health" Infectious Disease Reports 14, no. 1: 63-81. https://doi.org/10.3390/idr14010008
APA StyleLibera, K., Konieczny, K., Grabska, J., Szopka, W., Augustyniak, A., & Pomorska-Mól, M. (2022). Selected Livestock-Associated Zoonoses as a Growing Challenge for Public Health. Infectious Disease Reports, 14(1), 63-81. https://doi.org/10.3390/idr14010008