
Evaluation of Antibiotic Prescribing Pattern and Appropriateness among Hospitalized Pediatric Patients: Findings from a Malaysian Teaching Hospital


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Study Population and Data Collection
2.3. Measurement
2.4. Sample Size
- n′ = sample size with finite population correction,
- N = population size,
- Z = Z statistic for a level of confidence, which is 1.96,
- P = expected proportion of inappropriate antibiotic use in hospitalized pediatrics, and
- d = precision, which is considered as 0.05.
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
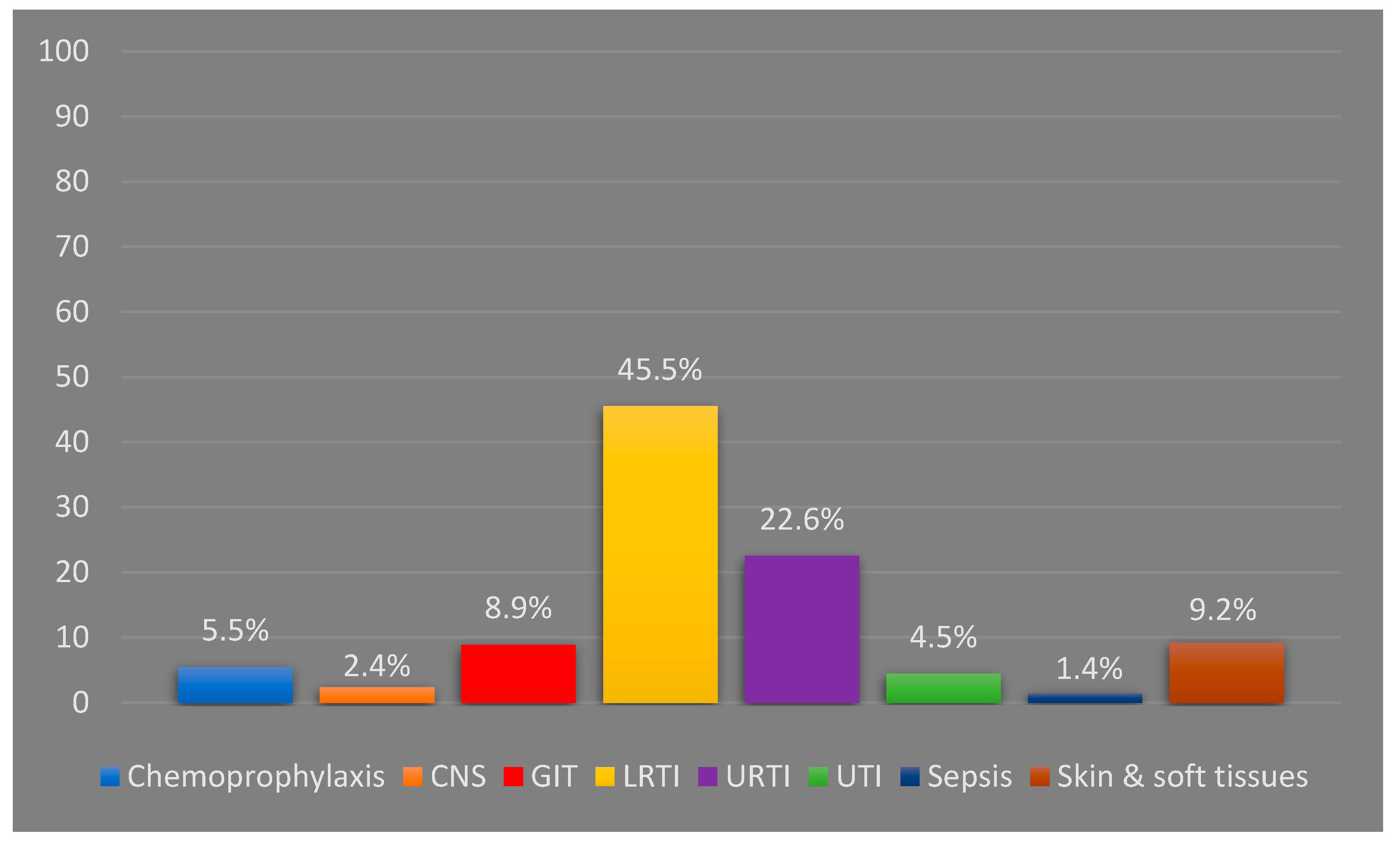
3.2. The Pattern and Indications of Antibiotics
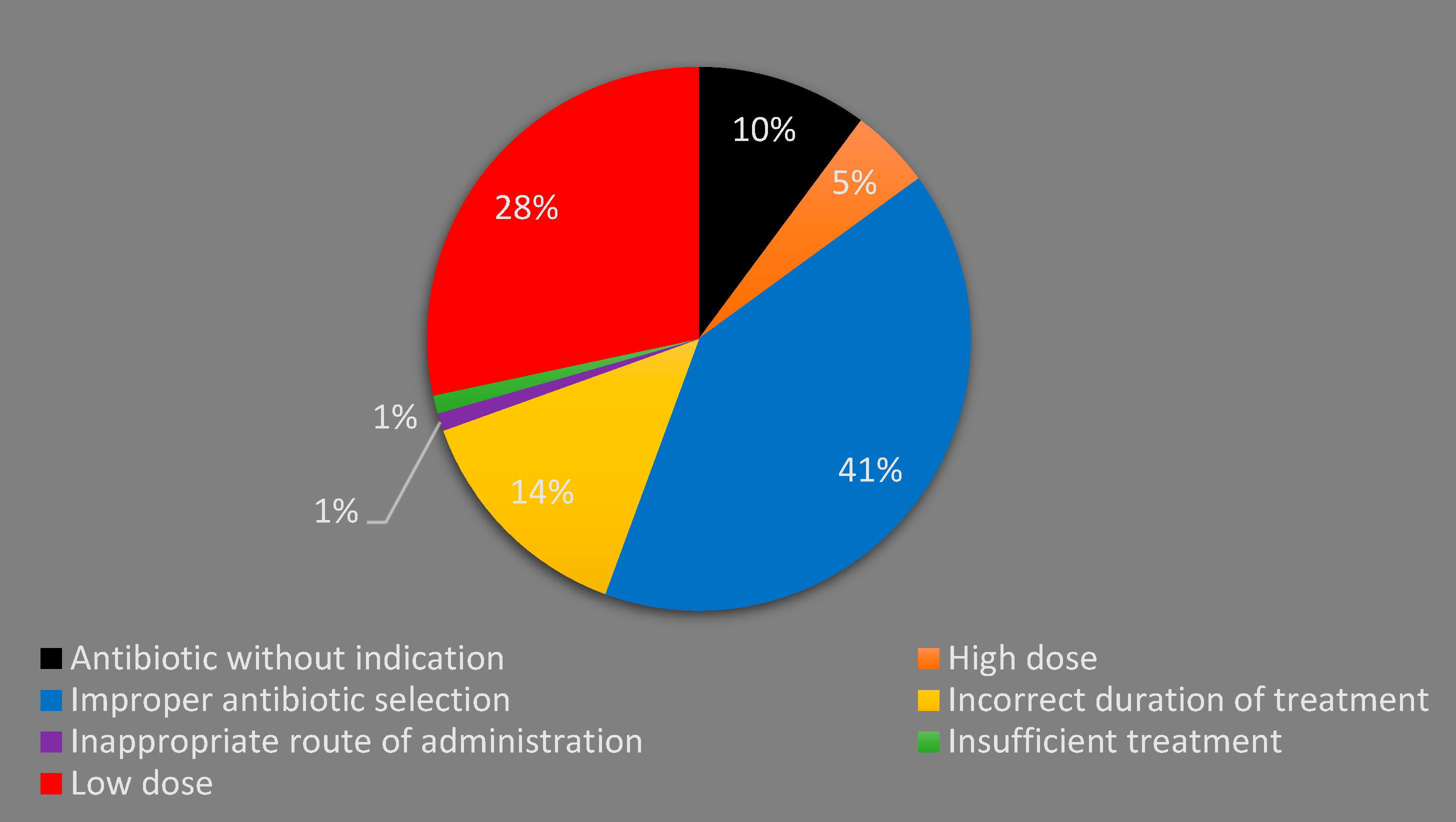
3.3. Inappropriate Antibiotic Prescribing
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. The Evolving Threat of Antimicrobial Resistance: Options for Action. 2012, pp. 1–119. Available online: http://www.ijmr.org.in/article.asp?issn=0971-5916;year=2014;volume=139;issue=1;spage=182;epage=183;aulast=Kapi (accessed on 8 November 2022).
- Smith, M.J.; Gerber, J.S.; Hersh, A.L. Inpatient antimicrobial stewardship in pediatrics: A systematic review. J. Pediatr. Infect. Dis. Soc. 2015, 4, e127–e135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sema, F.D.; Asres, E.D.; Wubeshet, B.D. Evaluation of Rational Use of Medicine Using WHO/INRUD Core Drug Use Indicators at Teda and Azezo Health Centers, Gondar Town, Northwest Ethiopia. Integr. Pharm. Res. Pract. 2021, 10, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Habboush, Y.; Guzman, N. Antibiotic Resistance; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK513277/ (accessed on 9 November 2022).
- Ferrer, A.P.S.; Sucupira, A.C.S.L.; Grisi, S.J.F.E. Causes of hospitalization among children ages zero to nine years old in the city of São Paulo, Brazil. Clinics 2010, 65, 35–44. [Google Scholar] [CrossRef] [Green Version]
- Leyenaar, J.A.K.; Ralston, S.L.; Shieh, M.S.; Pekow, P.S.; Mangione-Smith, R.; Lindenauer, P.K. Epidemiology of pediatric hospitalizations at general hospitals and freestanding children’s hospitals in the United States. J. Hosp. Med. 2016, 11, 743–749. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, A.M.; Awad, A.I. Drug use practices at pediatric hospitals of Khartoum State, Sudan. Ann. Pharmacother. 2010, 44, 1986–1993. [Google Scholar] [CrossRef] [PubMed]
- Umar, L.W.; Isah, A.; Musa, S.; Umar, B. Prescribing pattern and antibiotic use for hospitalized children in a Northern Nigerian Teaching Hospital. Ann. Afr. Med. 2018, 17, 26–32. [Google Scholar] [CrossRef]
- Sharma, M.; Damlin, A.; Pathak, A.; Lundborg, C.S. Antibiotic prescribing among pediatric inpatients with potential infections in two private sector hospitals in Central India. PLoS ONE 2015, 10, e0142317. [Google Scholar] [CrossRef]
- Chaw, P.S.; Schlinkmann, K.M.; Raupach-Rosin, H.; Karch, A.; Pletz, M.W.; Huebner, J.; Nyan, O.; Mikolajczyk, R. Antibiotic use on paediatric inpatients in a teaching hospital in the Gambia, a retrospective study. Antimicrob Resist Infect Control. Antimicrob. Resist. Infect. Control 2018, 7, 82. [Google Scholar] [CrossRef] [Green Version]
- Ceyhan, M.; Yildirim, I.; Ecevit, C.; Aydogan, A.; Ornek, A.; Salman, N.; Somer, A.; Hatipoğlu, N.Y.; Camcioglu, Y.; Alhan, E.; et al. Inappropriate antimicrobial use in Turkish pediatric hospitals: A multicenter point prevalence survey. Int. J. Infect. Dis. 2010, 14, e55–e61. [Google Scholar] [CrossRef] [Green Version]
- Iftikhar, S.; Sarwar, M.R.; Saqib, A.; Sarfraz, M.; Shoaib, Q.U.A. Antibiotic prescribing practices and errors among hospitalized pediatric patients suffering from acute respiratory tract infections: A multicenter, cross-sectional study in pakistan. Medicina 2019, 55, 44. [Google Scholar] [CrossRef]
- Chavez-Bueno, S.; Stull, T.L. Antibacterial Agents in Pediatrics. Infect. Dis. Clin. N. Am. 2009, 23, 865–880. [Google Scholar] [CrossRef]
- Pradeepkumar, B.; Alameri, T.; Narayana, G.; Reddy, Y.; Ramaiah, J. Assessment of antibiotic prescribing pattern in pediatric patients: A cross-sectional hospital-based survey. CHRISMED J. Health Res. 2017, 4, 235–237. [Google Scholar] [CrossRef]
- Tham, D.W.J.; Abubakar, U.; Tangiisuran, B. Prevalence and predictors of antibiotic use among children visiting the Emergency Department in a Tertiary Hospital in Malaysia. Eur. J. Pediatr. 2020, 179, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Tan, G.H.; Chan, H.K.; Jamal, L.M.; Hamidon, M.H.; Oi, A.C.; Yap, Y.T.; Khoo, Y.H. Antibiotic Prescribing Practice for Paediatric Outpatients across Non-specialised Regional Hospitals in Kedah State, Malaysia. Asia Pac. J. Pediatr. Child Health 2018, 1, 24–31. [Google Scholar]
- Zawawi, N.M.; Sathianathan, S.; Eddian, N.; Singh, M.K.J.B.; Sarangapani, N.; Nayan, N.S.N.; Grewal, A.K. Prescribing Pattern of Antibiotics in the General Pediatrics Ward of Tengku Ampuan Rahimah Hospital (HTAR): A Prospective Study. Pharm. Res. Rep. 2020, 3, 68. [Google Scholar]
- Rosli, R.; Ming, L.C.; Aziz, N.A.; Manan, M.M. A retrospective analysis of spontaneous adverse drug reactions reports relating to paediatric patients. PLoS ONE 2016, 11, e0155385. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health Malaysia. National Antibiotic Guideline, 2nd ed.; Ministry of Health Malaysia: Kuala Lumpur, Malaysia, 2014.
- Ministry of Health Malaysia. National Antibiotic Guideline, 3rd ed.; Ministry of Health Malaysia: Kuala Lumpur, Malaysia, 2019.
- Department of Statistics Malaysia. Current Population Estimates, Malaysia. 2020. Available online: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=155&bul_id=ZjJOSnpJR21sQWVUcUp6ODRudm5JZz09&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09 (accessed on 9 November 2022).
- Naing, L.; Winn, T.; Rusli, B.N. Practical Issues in Calculating the Sample Size for Prevalence Studies. Arch. Orofac. Sci. 2006, 1, 9–14. [Google Scholar]
- Adnan, S. Point prevalence surveillance on antimicrobial in major specialist hospital in Malaysia. Int. J. Infect. Dis. 2020, 101, 98–99. [Google Scholar] [CrossRef]
- Mora, Y.; Avila-Agüero, M.L.; Umaa, M.A.; Jiménez, A.L.; París, M.M.; Faingezicht, I. Epidemiologic observations of the judicious use of antibiotics in a pediatric teaching hospital. Int. J. Infect. Dis. 2002, 6, 74–77. [Google Scholar] [CrossRef] [Green Version]
- Salas, A.A.; Aranda, E. Antibiotic prescribing patterns as empirical therapy among hospitalized patients in a Bolivian paediatric teaching hospital. Acta Pædiatr. 2007, 96, 1533–1535. [Google Scholar] [CrossRef]
- Choudhury, D.K.; Bezbaruah, B.K. Antibiotic prescriptions pattern in paediatric in-patient department gauhati medical college and hospital, Guwahati. J. Appl. Pharm. Sci. 2013, 3, 144–148. [Google Scholar]
- Miao, R.; Wan, C.; Wang, Z.; Zhu, Y.; Zhao, Y.; Zhang, L.; Liu, J.; Qin, J.; Xia, J.; Yan, H. Inappropriate antibiotic prescriptions among pediatric inpatients in different type hospitals. Medicina 2020, 99, e18714. [Google Scholar]
- Oğuz, E.; Bebitoğlu, B.T.; Nuhoğlu, Ç.; Çağ, Y.; Hodzic, A.; Temel, F.; Çırtlık, P.; Dalkılıç, A.E.K. Evaluation of antibiotic use among hospitalised patients in a paediatric department of a training hospital in Turkey. Int. J. Clin. Pract. 2021, 75, e13782. [Google Scholar] [CrossRef] [PubMed]
- Yehualaw, A.; Taferre, C.; Bantie, A.T.; Demsie, D.G. Appropriateness and Pattern of Antibiotic Prescription in Pediatric Patients at Adigart General Hospital, Tigray, Ethiopia. BioMed Res. Int. 2021, 2021, 6640892. [Google Scholar] [CrossRef]
- Piedra, P.A.; Stark, A.R. Bronchiolitis in Infants and Children: Treatment, Outcome, and Prevention. UpToDate. 2021. Available online: https://www.uptodate.com/contents/bronchiolitis-in-infants-and-children-treatment-outcome-and-prevention?search=bronchiolitischildren&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 (accessed on 9 November 2022).
- Tang, K.L.; Wimmer, B.C.; Akkawi, M.E.; Ming, L.C.; Ibrahim, B. Incidence and pattern of medication errors in a general paediatric ward in a developing nation. Res. Soc. Adm. Pharm. 2018, 14, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Permala, J.; Hassali, M.A.; Awaisu, A.; Shafie, A.A. Dosing information in a standard drug reference: Are pediatrics still therapeutically neglected? Pediatr. Int. 2010, 52, 290–295. [Google Scholar] [CrossRef]
- Llewelyn, M.J.; Fitzpatrick, J.M.; Darwin, E.; Tonkin-Crine, S.; Gorton, C.; Paul, J.; Peto, T.E.A.; Yardley, L.; Hopkins, S.; Walker, A.S. The antibiotic course has had its day. BMJ 2017, 358, j3418. [Google Scholar] [CrossRef] [Green Version]
- Langford, B.J.; Morris, A.M. Is it time to stop counselling patients to “finish the course of antibiotics”? Can. Pharm. J. 2017, 150, 349–350. [Google Scholar] [CrossRef] [Green Version]
- Dedefo, M.G.; Mitike, A.H.; Angamo, M.T. Incidence and determinants of medication errors and adverse drug events among hospitalized children in West Ethiopia. BMC Pediatr. 2016, 16, 81. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | N (%) * |
|---|---|
| Gender | |
| Male | 169 (57.9) |
| Female | 123 (42.1) |
| Age (year) | |
| <1 | 55 (18.8) |
| 1–3 | 118 (40.4) |
| 3–6 | 62 (21.2) |
| >6 years | 57 (19.5) |
| Mean ± SD | 3.4 ± 2.9 |
| Median (range) | 2.5 (0.1–12) |
| Duration of hospitalization (days) | |
| Mean ± SD | 3.5 ± 1.96 |
| Median (range) | 3.0 (1–13) |
| Having a history of medical illness(es) | |
| Yes | 132 (45.2) |
| No | 160 (54.8) |
| The most common diagnosis | |
| Pneumonia | 120 (41.1) |
| Tonsilitis | 30 (10.3) |
| Pharyngitis | 21 (7.2) |
| Gastroenteritis | 12 (4.1) |
| Urinary tract infection | 10 (3.4) |
| Number of antibiotics used in the ward | |
| 1 | 209 (71.6) |
| 2 | 74 (25.3) |
| 3 | 9 (3.1) |
| Discharged with antibiotic | |
| Yes | 245 (83.9) |
| No | 47 (16.1) |
| Total ** duration of antibiotic treatment (days) | |
| Mean ± SD | 6.79 ± 3 |
| Median (range) | 7 (1–30) |
| Having IAP | |
| No IAP | 123 (42.1) |
| One type of IAP | 155 (53.1) |
| Two types of IAP | 14 (4.8) |
| Antibiotic Class | Antibiotic Agent | N (%) In-Ward | N (%) At Discharge |
|---|---|---|---|
| Penicillins | Amoxicillin | 3 (0.78) | 2 (0.70) |
| Ampicillin | 15 (3.90) | 11 (3.87) | |
| Cloxacillin | 18 (4.68) | 14 (4.93) | |
| Benzylpenicillin | 7 (1.82) | 1 (0.35) | |
| Phenoxymethylpenicillin | 4 (1.04) | 5 (1.75) | |
| Penicillins + beta-lactamase inhibitor | Amoxicillin + clavulanic acid | 98 (25.45) | 79 (27.82) |
| Piperacillin + tazobactam | 2 (0.52) | - | |
| Macrolide | Azithromycin | 102 (26.49) | 84 (29.58) |
| Clarithromycin | 3 (0.78) | 3 (1.06) | |
| Erythromycin | 2 (0.52) | 3 (1.06) | |
| Second gen. cephalosporines | Cefuroxime | 88 (22.86) | 80 (28.07) |
| Third gen. cephalosporines | Ceftriaxone | 20 (5.19) | - |
| Ceftazidime | 1 (0.26) | - | |
| Cefotaxime | 2 (0.52) | - | |
| Fourth gen. cephalosporines | Cefepime | 1 (0.26) | 1 (0.35) |
| Aminoglycosides | Gentamicin | 7 (1.82) | 1 (0.35) |
| Amikacin | 1 (0.26) | - | |
| Carbapenems | Carbapenem | 1 (0.26) | - |
| Meropenem | 1 (0.26) | - | |
| Sulfonamide | Sulfamethoxazole + trimethoprim | 2 (0.52) | 1 (0.35) |
| Glycopeptides | Vancomycin | 2 (0.52) | - |
| Lincosamides | Clindamycin | 1 (0.26) | - |
| Imidazole derivatives | Metronidazole | 4 (1.04) | |
| Total | 385 (100) | 285 (100) |
| Variable | Unstandardized Coefficient (B) | p Value | OR | 95% CI for OR | |
|---|---|---|---|---|---|
| Gender (Male) | 0.004 | 0.986 | 1.005 | 0.598 | 1.687 |
| Age categories | 0.275 | ||||
| 1–3 years | −0.349 | 0.343 | 0.705 | 0.343 | 1.450 |
| 3–6 years | −0.800 | 0.054 | 0.449 | 0.199 | 1.015 |
| >6 years | −0.479 | 0.262 | 0.619 | 0.268 | 1.432 |
| Having a history of medical illness(es) | 0.092 | 0.728 | 1.096 | 0.654 | 1.836 |
| Days of hospitalization | 0.040 | 0.582 | 1.041 | 0.903 | 1.199 |
| Type of the infection | 0.002 | ||||
| CNS | 0.382 | 0.696 | 1.466 | 0.215 | 9.980 |
| GIT | 0.831 | 0.219 | 2.295 | 0.610 | 8.631 |
| LRTI | 0.493 | 0.389 | 1.638 | 0.533 | 5.038 |
| Sepsis | −0.909 | 0.483 | 0.403 | 0.032 | 5.122 |
| Skin and soft tissues | 0.262 | 0.692 | 1.299 | 0.355 | 4.758 |
| URTI | 1.968 | 0.002 | 7.158 | 2.081 | 24.624 |
| UTI | 1.226 | 0.127 | 3.406 | 0.704 | 16.475 |
| Number of AB used | 0.040 | ||||
| Two antibiotics | 0.620 | 0.047 | 1.859 | 1.009 | 3.425 |
| Three antibiotics | 1.949 | 0.079 | 7.023 | 0.797 | 61.911 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akkawi, M.E.; Taffour, R.M.; AL-Shami, A.M. Evaluation of Antibiotic Prescribing Pattern and Appropriateness among Hospitalized Pediatric Patients: Findings from a Malaysian Teaching Hospital. Infect. Dis. Rep. 2022, 14, 889-899. https://doi.org/10.3390/idr14060089
Akkawi ME, Taffour RM, AL-Shami AM. Evaluation of Antibiotic Prescribing Pattern and Appropriateness among Hospitalized Pediatric Patients: Findings from a Malaysian Teaching Hospital. Infectious Disease Reports. 2022; 14(6):889-899. https://doi.org/10.3390/idr14060089
Chicago/Turabian StyleAkkawi, Muhammad Eid, Randa Mahmoud Taffour, and Abdulkareem Mohammed AL-Shami. 2022. "Evaluation of Antibiotic Prescribing Pattern and Appropriateness among Hospitalized Pediatric Patients: Findings from a Malaysian Teaching Hospital" Infectious Disease Reports 14, no. 6: 889-899. https://doi.org/10.3390/idr14060089
APA StyleAkkawi, M. E., Taffour, R. M., & AL-Shami, A. M. (2022). Evaluation of Antibiotic Prescribing Pattern and Appropriateness among Hospitalized Pediatric Patients: Findings from a Malaysian Teaching Hospital. Infectious Disease Reports, 14(6), 889-899. https://doi.org/10.3390/idr14060089