


Frequency and Antibiotic Susceptibility Patterns of Streptococcus agalactiae Strains Isolated from Women in Yaounde, Cameroon
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Type, Location and Duration of the Study
2.2. Study Population, Selection Criteria and Sampling Method
2.3. Data and Sample Collection Method
2.4. Sample Analysis
2.5. Data Analysis and Interpretation
2.6. Ethical Considerations
2.7. Limitation of the Study
3. Results
3.1. General Characteristics of the Population
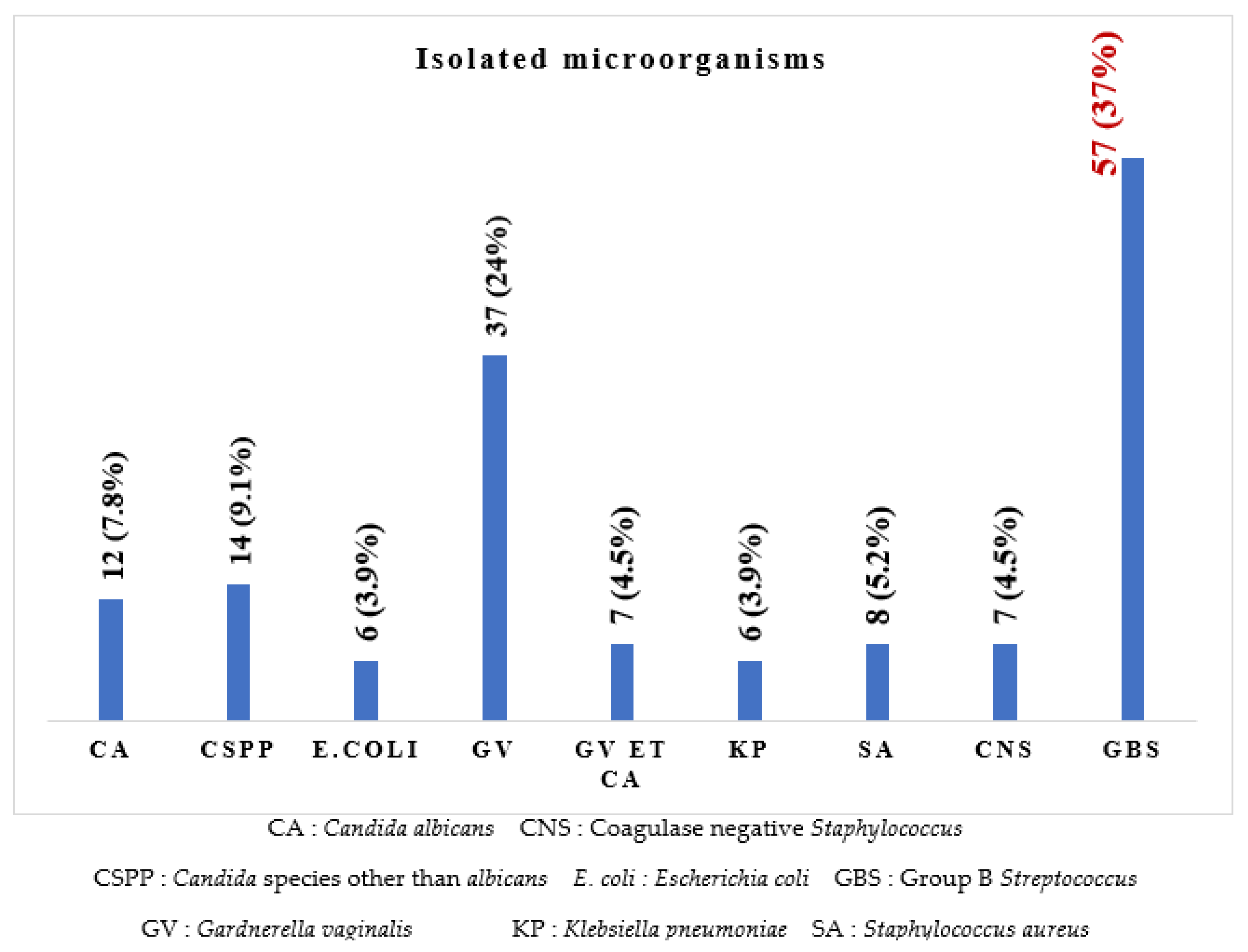
3.2. Frequency of Identified Microorganisms
3.3. Antibiotic Resistance Profile of Streptococcus agalactiae
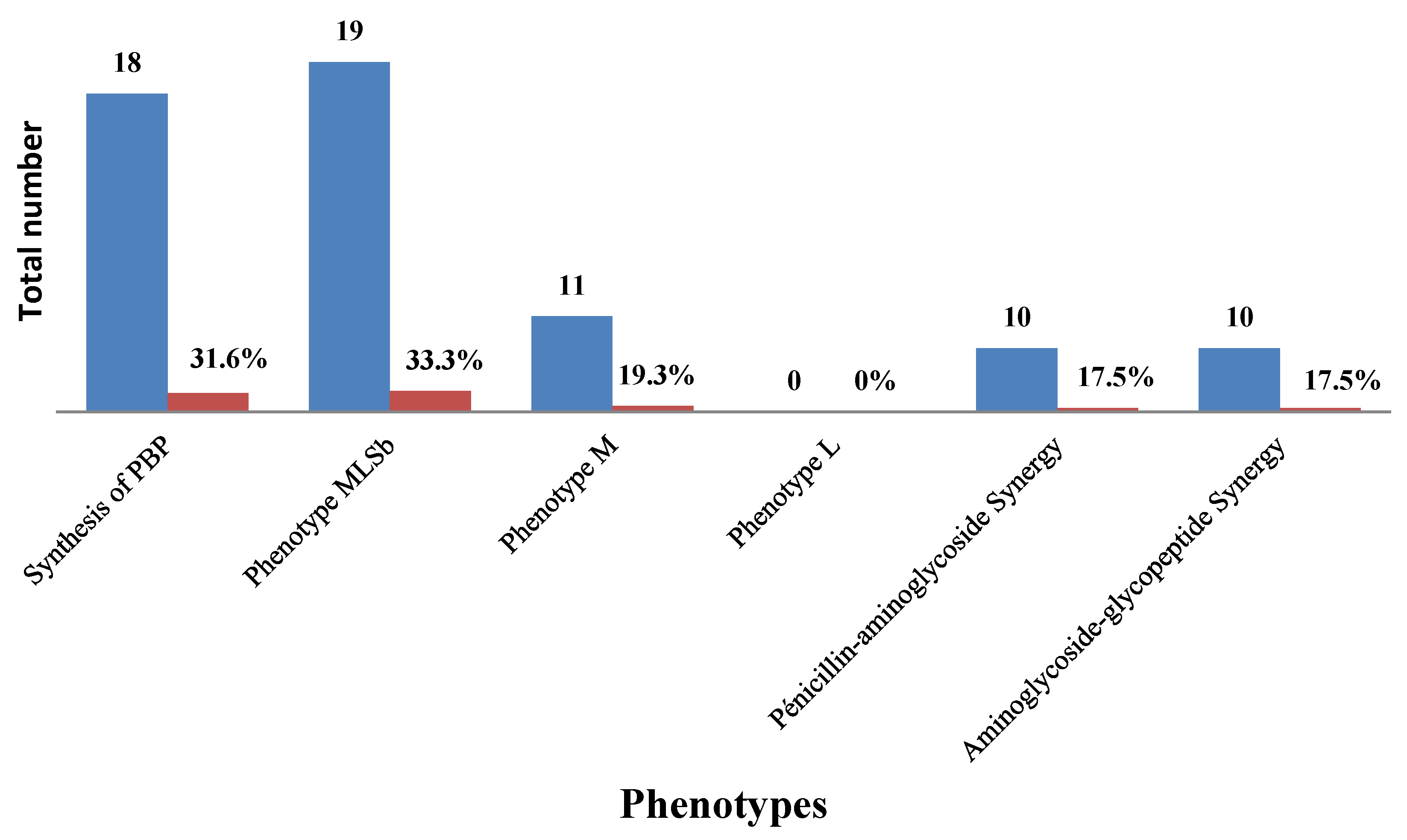
3.4. Resistance Phenotypes
3.5. Risk Factors Associated with GBS Infection in Women
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Otaguiri, E.S.; Morguette, A.E.; Tavares, E.R.; dos Santos, P.M.; Morey, A.T.; Cardoso, J.D.; Perugini, M.R.; Yamauchi, L.M.; Yamada-Ogatta, S.F. Commensal Streptococcus agalactiae isolated from patients seen at University Hospital of Londrina, Paraná, Brazil: Capsular types, genotyping, antimicrobial susceptibility and virulence determinants. BMC Microbiol. 2013, 13, 297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccinelli, G.; Biscaro, V.; Gargiulo, F.; Caruso, A.; De Francesco, M.A. Characterization and antibiotic susceptibility of Streptococcus agalactiae isolates causing urinary tract infections. Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 2015, 34, 1–6. [Google Scholar] [CrossRef] [PubMed]
- El Aila, N.A.; Tency, I.; Claeys, G.; Saerens, B.; Cools, P.; Verstraelen, H.; Temmerman, M.; Verhelst, R.; Vaneechoutte, M. Comparison of different sampling techniques and of different culture methods for detection of group B streptococcus carriage in pregnant women. BMC Infect. Dis. 2010, 10, 285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joachim, A.; Matee, M.I.; Massawe, F.A.; Lyamuya, E.F. Maternal and neonatal colonisation of group B streptococcus at Muhimbili National Hospital in Dar es Salaam, Tanzania: Prevalence, risk factors and antimicrobial resistance. BMC Public Health 2009, 9437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dipersio, L.P.; Dipersio, J.R. Identification of an erm(T) gene in strains of inducibly clindamycin-resistant group B Streptococcus. Diagn. Microbiol. Infect. Dis. 2007, 57, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Verani, J.R.; McGee, L.; Schrag, S.J. Prevention of perinatal group B streptococcal disease--revised guidelines from CDC, MMWR Recommendations and reports: Morbidity and mortality weekly report Recommendations and reports. CDC Recomm. Rep. 2010, 59, 1–32. [Google Scholar]
- Gizachew, M.; Tiruneh, M.; Moges, F.; Tessema, B. Streptococcus agalactiae maternal colonization, antibiotic resistance and serotype profiles in Africa: A meta-analysis. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 14. [Google Scholar] [CrossRef] [Green Version]
- Gygax, S.E.; Schuyler, J.A.; Kimmel, L.E.; Trama, J.P.; Mordechai, E.; Adelson, M.E. Erythromycin and clindamycin resistance in group B streptococcal clinical isolates. Antimicrob. Agents Chemother. 2006, 50, 1875–1877. [Google Scholar] [CrossRef] [Green Version]
- Nkembe, N.M.; Kamga, H.G.; Baiye, W.A.; Chafa, A.B.; Njotang, P.N. Streptococcus agalactiae prevalence and antimicrobial susceptibility pattern in vaginal and anorectal swabs of pregnant women at a tertiary hospital in Cameroon. BMC Res. Notes 2018, 11, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adawaye, C.; Michel, T.; Paul, A.J.; Therese, N.; Hortense, G.; Koanga, M.; Sinata, K.S. Vaginal colonization and resistance profile of group B Streptococcus among pregnant women in Yaounde Gynecology, Ob-stetric and Pediatric Hospital in Cameroon. J. Clin. Med. Res. 2014, 6, 16–21. [Google Scholar]
- Tounaire, M. Recommandation pour la pratique clinique, infections cervico-vaginales et grossesse. CNGOF. Available online: http://www.cngof.fr/pratiques-cliniques/recommandations-pour-la-pratique-clinique (accessed on 24 September 2022).
- Giuliano, C.; Patel, C.R.; Kale-Pradhan, P.B. A Guide to Bacterial Culture Identification and Results Interpretation. PT 2019, 44, 192–200. [Google Scholar]
- Lennete, H.E.; Balows, A.; Hausler, W.J., Jr.; Shadomy, H.J. Manual of Clinical Microbiology, 4th ed.; American Association of Microbiology Press: Washington, DC, USA, 1985; pp. 263–277. [Google Scholar]
- Gupta, K.; Grigoryan, L.; Trautner, B. Urinary tract infection. Ann. Intern Med. 2017, 167, 49–64. [Google Scholar] [CrossRef]
- Montes, K.; Ortiz, B.; Galindo, C.; Figueroa, I.; Braham, S.; Fontecha, G. Identification of Candida Species from Clinical Samples in a Honduran Tertiary Hospital. Pathogens 2019, 8, 237. [Google Scholar] [CrossRef] [PubMed]
- Hudzicki, J. Kirby-Bauer, Diffusion Susceptibility Test Protocol. American Society for Microbiology: Washington, DC, USA, 2009. [Google Scholar]
- Quiroga, M.; Pegels, E.; Oviedo, P.; Pereyra, E.; Vergara, M. Susceptibility patterns and prevalence of GBS isolated from pregnant women in Misiones, Argentina. Braz. J. Microbiol. 2008, 39, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.S.; Walsh, A.; Crowleyet, B. Role of efux in macrolide resistance in β-hemolytic streptococci of groups A, B, C and G collected in an Irish teaching hospital. J. Med. Microbiol. 2011, 60, 262–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desjardins, M.; Delgaty, K.L.; Ramotar, K.; Seetaram, C.; Toye, B. Prevalence and mechanisms of erythromycin resistance in group A and group B streptococcus: Implications for reporting susceptibility results. J. Med. Microbiol. 2004, 42, 5620–5623. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.M.; Asrat, D.; Fenta, D.A.; Chaka, T.E.; Woldeamanuel, Y. Group B Streptococcus colonization rate and serotype distribution among pregnant women and their newborns at Adama Hospital Medical College, Ethiopia. Sci. Rep. 2020, 10, 9301. [Google Scholar] [CrossRef]
- Vinnemeier, C.D.; Brust, P.; Owusu-Dabo, E.; Sarpong, N.; Sarfo, E.Y.; Bio, Y.; Rolling, T.; Dekker, D.; Adu-Sarkodie, Y.; Eberhardt, K.A.; et al. Group B Streptococci serotype distribution in pregnant women in Ghana: Assessment of potential coverage through future vaccines. Trop. Med. Int. Health 2015, 20, 1516–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gizachew, M.; Tiruneh, M.; Moges, F.; Adefris, M.; Tigabu, Z.; Tessema, B. Streptococcus agalactiae from Ethiopian pregnant women; prevalence, associated factors and antimicrobial resistance: Alarming for prophylaxis. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 3. [Google Scholar] [CrossRef] [PubMed]
- Valère, M.K.; Mengouna, J.-R.; Essiben, F.; Gonsu Kamga, H. Colonisation Génitale et Profil de Sensibilité du Streptocoque du Groupe B chez les Femmes Enceintes dans deux Hôpitaux de Yaoundé. Health Sci. Dis. 2017, 18. Available online: https://www.hsd-fmsb.org/index.php/hsd/article/view/925 (accessed on 24 September 2022).
- Cheng, Z.; Qu, P.; Ke, P.; Yang, X.; Zhou, Q.; Lan, K.; He, M.; Cao, N.; Qin, S.; Huang, X. Antibiotic Resistance and Molecular Epidemiological Characteristics of Streptococcus agalactiae Isolated from Pregnant Women in Guangzhou, South China. Can. J. Infect. Dis. Med. Microbiol. 2020, 2020, 1368942. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.C.; Sutcliffe, J.; Courvalin, P.; Jensen, L.B.; Rood, J.; Seppala, H. Nomenclature for macrolide and macrolide-lincosamide-streptogramin B resistance determinants. Antimicrob. Agents Chemother. 1999, 43, 2823–2830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hraoui, M.; Boutiba-Ben, B.I.; Rachdi, M.; Slim, A.; Ben Redjeb, S. Macrolide and tetracycline resistance in clinical strains of Streptococcus agalactiae isolated in Tunisia. J. Med. Microbiol. 2012, 61, 1109–1113. [Google Scholar] [CrossRef] [PubMed]
- Back, E.E.; O’Grady, E.J.; Back, J.D. High Rates of Perinatal Group B Streptococcus Clindamycin and Erythromycin Resistance in an Upstate New York Hospital. Antimicrob Agents Chemother 2012, 56, 739–742. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Nasaj, M.; Hosseini, S.M.; Arabestani, M.R. Survey of strain distribution and antibiotic resistance pattern of group B streptococci (Streptococcus agalactiae) isolated from clinical specimens. GMS Hyg. Infect. Control. 2016, 11, Doc18. [Google Scholar]
- Hansen, S.M.; Uldbjerg, N.; Kilian, M.; Sørensen, U.B. Dynamics of Streptococcus agalactiae colonization in women during and after pregnancy and in their infants. J. Clin. Microbiol. 2004, 42, 83–89. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total Number | Percentage (%) |
|---|---|---|
| Pregnant women | 90 | 55.2 |
| Non-pregnant women | 73 | 44.8 |
| Age group (in years) | ||
| 17–25 | 41 | 25.1 |
| 26–34 | 57 | 35 |
| 35–43 | 2 | 19.6 |
| 44–52 | 20 | 12.3 |
| 53 and above | 13 | 8 |
| Mean age: 32.34 years ± 10.48 | ||
| Gestational age (in weeks) | ||
| 27–31 | 41 | 45.6 |
| 32–36 | 22 | 24.4 |
| 37–41 | 27 | 30 |
| Sample type | ||
| Vaginal swab | 138 | 84.7 |
| Urine | 25 | 15.3 |
| Number of GBS strains isolated | ||
| Pregnant women | 34 | 59.6 |
| Non-pregnant women | 23 | 40.3 |
| Antibiotics | Resistant n/57 | Percentages (%) |
|---|---|---|
| Penicillin G | 34 | 58.8% |
| Oxacillin | 34 | 58.8% |
| Amoxicillin | 40 | 70.6% |
| Ceftazidim | 27 | 47.1% |
| Vancomycin | 34 | 58.8% |
| Gentamycin | 27 | 47.1% |
| Streptomycin | 50 | 88.2% |
| Erythromycin | 27 | 47.1% |
| Clindamycin | 37 | 64.7% |
| Tetracycline | 50 | 88.2% |
| Doxycycline | 57 | 100% |
| Chloramphenicol | 50 | 88.2% |
| Norfloxacin | 17 | 29.4% |
| Levofloxacin | 10 | 17.6% |
| Cotrimoxazol | 57 | 100% |
| Bacitracin | 57 | 100% |
| MAR index | Number of isolates/57 | |
| 00 | 08 | 14% |
| 0.1 | 22 | 38.6% |
| 0.2 | 13 | 22.8% |
| 0.3 | 09 | 15.8% |
| 0.5 | 03 | 5.3% |
| 0.7 | 02 | 3.5% |
| Variable | GBS | Total n (%) | p-Value | ||
|---|---|---|---|---|---|
| No | Yes | ||||
| Pregnancy | No | 50 (94.3%) | 23 (40.3%) | 73 (44.8%) | 0.019 |
| Yes | 56 (80.0%) | 34 (59.6%) | 90 (55.2%) | ||
| Gestational age (in weeks) | 27–31 | 25 (73.5%) | 16 (39.0%) | 41 (45.6%) | 0.025 |
| 32–36 | 15 (93.8%) | 7 (31.8%) | 22 (24.4%) | ||
| 37–41 | 16 (80.0%) | 11 (40.7%) | 27 (30.0%) | ||
| Age (in years) | 17–25 | 27 (81.8%) | 17 (41.5%) | 41 (25.1%) | 0.890 |
| 26–34 | 43 (87.7%) | 14 (24.6%) | 57 (35%) | ||
| 35–43 | 21 (87.5%) | 11 (34.4%) | 32 (19.6%) | ||
| 44–52 | 11 (91.7%) | 9 (45.0%) | 20 (12.3%) | ||
| 53 and above | 4 (80.0%) | 9 (69.2%) | 13 (8.0%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Djuikoue, C.I.; Djoulako, P.D.D.; Wouambo, R.K.; Foutsa, R.Y.; Ngatcheu, D.E.; Apalata, T. Frequency and Antibiotic Susceptibility Patterns of Streptococcus agalactiae Strains Isolated from Women in Yaounde, Cameroon. Microbiol. Res. 2022, 13, 954-962. https://doi.org/10.3390/microbiolres13040068
Djuikoue CI, Djoulako PDD, Wouambo RK, Foutsa RY, Ngatcheu DE, Apalata T. Frequency and Antibiotic Susceptibility Patterns of Streptococcus agalactiae Strains Isolated from Women in Yaounde, Cameroon. Microbiology Research. 2022; 13(4):954-962. https://doi.org/10.3390/microbiolres13040068
Chicago/Turabian StyleDjuikoue, Cécile Ingrid, Paule Dana Djouela Djoulako, Rodrigue Kamga Wouambo, Rosine Yemetio Foutsa, Dorine Ekeu Ngatcheu, and Teke Apalata. 2022. "Frequency and Antibiotic Susceptibility Patterns of Streptococcus agalactiae Strains Isolated from Women in Yaounde, Cameroon" Microbiology Research 13, no. 4: 954-962. https://doi.org/10.3390/microbiolres13040068
APA StyleDjuikoue, C. I., Djoulako, P. D. D., Wouambo, R. K., Foutsa, R. Y., Ngatcheu, D. E., & Apalata, T. (2022). Frequency and Antibiotic Susceptibility Patterns of Streptococcus agalactiae Strains Isolated from Women in Yaounde, Cameroon. Microbiology Research, 13(4), 954-962. https://doi.org/10.3390/microbiolres13040068