Abstract
Antimicrobial resistance (AMR) is an ongoing phenomenon. It is a significant public health issue that has existed long before the coronavirus disease of 2019 (COVID-19) pandemic. It develops as microorganisms undergo genetic mutations that allow them to survive despite antimicrobial treatment. This process is highly associated with excessive and often unnecessary antimicrobial pharmacotherapy, which was often discussed during the COVID-19 pandemic. This article explores how the pandemic has affected antimicrobial stewardship by shifting the focus away from antimicrobial resistance, as well as the impact of enhanced antibiotic usage and measures such as lockdowns, mandatory testing and vaccination on antimicrobial resistance. Although these measures were regarded as successful in terms of limiting the pandemic, they have significantly contributed to an already escalating AMR issue. Outpatient methods in primary care and intensive care units aiming to prevent severe COVID-19 disease have contributed to the spread of multidrug-resistant bacteria, while laboratories burdened with COVID-19 testing have indirectly interrupted the detection of these bacteria. In this review, we summarize the pathogens whose AMRe has been greatly affected by COVID-19 measures and emphasize the importance of efficient antimicrobial stewardship in future pandemic and non-pandemic states to promote the responsible use of antibiotics and minimize AMR.
1. Introduction
The coronavirus disease of 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome corona virus 2 (SARS-CoV-2), resulted in significant global impacts, ranging from direct health consequences to widespread disruption of many aspects of daily life, as well as social and economic challenges such as healthcare capacity issues and supply chain disruptions [1]. Since it was initially detected in China (Wuhan) in 2019, the virus has rapidly spread and, to this day, affected over 32.7 million people with more than 1 million fatal outcomes globally [2]. To promptly respond to this serious global health threat and avoid the total collapse of public health systems, health authorities worldwide had to establish and implement various aggressive prevention measures. These measures included lockdowns, social distancing, requirements for face masks, rigorous hygiene measures, development of rapid COVID-19 tests, implementation of mandatory testing, vaccination, as well as isolation (i.e., quarantine of diagnosed patients and their contacts) and travel restrictions [2,3]. Although it has been reported that these activities contributed to the reduced spread of other infectious diseases, including pneumococcal disease and influenza, it became clear that the COVID-19 pandemic and its treatment-related policies set aside an essential issue—antimicrobial resistance (AMR) [1,2]. Even before the pandemic outbreak, it was reported that by 2050, the number of deaths per year due to AMR would reach 10 million if required rigorous measures against AMR were not implemented [4]. Increased antibiotic consumption, personal protective equipment, biocides and other personal care products have contributed to the changed global landscape of AMR [1,3]. From an economic point of view, according to the World Bank, high levels of antibiotic resistance would reduce the GDP (gross domestic product) by 3.8% by the year 2050 [5]. Furthermore, hospitals crowded with COVID-19 patients enabled the increased spread of multidrug-resistance (MDR) bacteria, and the main work of laboratories, detection of the COVID-19 virus, indirectly interrupted the detection of MDR bacteria [6]. The aim of this review is to explore how measures taken during the COVID-19 pandemic affected AMR as well as changes in antimicrobial stewardship. We also highlight the importance of controlled management of these issues in future pandemic crises as well as in non-pandemic states.
2. AMR before COVID-19 Pandemic
AMR is the ability of various microorganisms to adapt to and survive different chemical agents that are designed either to slow their growth and help affected organisms in the fight against infection or to eliminate the microorganism. Long before the COVID-19 pandemic, the world was aware of the threat that came with the unsupervised and unnecessary use of antimicrobial agents. Even the discoverer of penicillin, Sir Alexandar Fleming, was aware of this potential issue and tried to bring it to the public’s attention [7,8]. Today, studies suggest that the single use of antibiotics has immediate and lasting effects on resistance for up to 4 years, and thus continuous use leads to a neverending cycle [9]. It is considered that the last 80 years of antimicrobial misuse in veterinary, human medicine and animal husbandry have accelerated the increase in the number of MDR bacteria, although MDR-related genes have been found in the gut bacteria of people in the most remote areas [10]. AMR was even discussed at the G8 summit in June 2013, and the conclusion was that it is the “major health security challenge of the 21st century” and may be a pandemic of its own kind. This meeting had a significant effect on US health care, as in the following year the Centers for Disease Control and Prevention (CDC) issued the National Strategy for Combating Antibiotic Resistance [11]. In 2017, the World Health Organisation (WHO) published a list of priority resistant bacterial species. The list grouped these bacteria into 3 subsections based on priority—bacteria with critical, high and medium priority. This type of division is still relevant today, showing the same bacteria but with a much greater sense of urgency [12]. Hospital wards, especially intensive care units, are a major source of nosocomial infections. The chance of acquiring infection in a hospital setting increases with time spent in the hospital, number of interactions (patient to patient or patient to healthcare worker), medical interventions (foreign body placement, surgery, etc.) and the patient’s condition. One of the clinical presentations of COVID-19 is pneumonia, often resulting in the requirement of breathing assistance via ventilators. Ventilators are a common cause of hospital-acquired pneumonia, called ventilator-associated pneumonia (VAP), which is the most common and the most fatal one [13,14]. One study, conducted in Barcelona [15], also suggested that COVID-19 patients were most commonly superinfected in hospital settings.
Briefly, bacteria can be divided into two major groups: Gram-positive and Gram-negative. Without getting into microbiology, it is necessary to know that Gram-negative bacteria are prone to developing microbial resistance due to the complex build of their outer layer [16]. Gram-positive bacteria are less likely to develop resistance and, according to the WHO in 2017, only two Gram-positive bacteria made the high-priority list—Enterococcus faecium and Staphylococcus aureus. The most common resistant pathogens with high priority were Acinetobacter baumannii, Pseudomonas aeruginosa and Enterobacteriaceae (Escherichia coli, Klebsiella pneumoniae, Enterobacter spp.) [12].
Acinetobacter baumannii is one of the most complex bacteria with multiple pathways to avoid or destroy antibiotic molecules, thus easily becoming multidrug-resistant. Resistance to amoxicillin, penicillin, carbapenems and aminoglycosides and their combinations are frequently observed. It is a common cause of urinary tract infections (UTIs), pneumonia and sepsis [17].
Pseudomonas aeruginosa is another important Gram-negative bacterium that is a common cause of ventilator-associated pneumonia (VAP), meaning that it is present in most intensive care units (ICUs). This bacteria also has multiple ways of defending against antimicrobial agents, easily developing resistance to generational cephalosporines (ceftazidime and cefepime), carbapenems and aminoglycosides (e.g., gentamycin) [18].
Enterobacteriaceae are the most common causes of UTIs and subsequent sepsis in critically ill patients. Their mechanism of developing antibiotic resistance is the production of an enzyme called beta-lactamase, which degrades beta-lactam antibiotics, namely, amoxicillin, penicillin and generational cephalosporines. Among them, Klebsiella pneumoniae is commonly resistant to carbapenem antimicrobials [19,20].
All these bacteria fall under the umbrella acronym, ESKAPE (Enterococcus faecies, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa and Enterobacter spp.), purposely spelled this way to emphasize how easily they become resistant and highlight the importance of their prevention, rather than treatment [21].
One way of tracking antibiotic usage in a particular geographic location is by sampling the local water bodies such as rivers or lakes and wastewater treatment plants [22]. This is possible mainly due to the pharmacodynamic properties of most antibiotics. Studies suggest that nearly 50–90% of antibiotics are not metabolized and are excreted, either in urine or feces, in their active form into the environment [23]. Furthermore, over 50% of unused antimicrobials are being disposed of in an inappropriate manner [24]. Combining these factors with misuse and overuse in human medicine triggers even more antibiotic resistance, as most of the wastewater treatment methods are not sufficient [23,25]. In particular, water sampled from city canals in Hanoi, Vietnam, before the pandemic already showed excessive concentrations of sulfamethoxazole, amoxicillin and erythromycin, confirming claims of a pre-existing public health threat that could now be exacerbated by the latest pandemic. Other geographic locations have an excess of different antimicrobials; nonetheless, they all lead to the same global public health problem: AMR and the promotion of antibiotic resistance genes (ARGs) [26]. Research conducted by analyzing water systems around Wuhan, China, in the summer and autumn of 2020 has shown that the total concentrations of PPCPs (pharmaceuticals and personal care products) were comparable to earlier measured values but there was a significant increase in macrolides and their metabolic byproducts of up to 78.9%, showing increased public demand for macrolides [27].
3. Antibiotic Use during the COVID-19 Pandemic
Initially, early in the pandemic, uncertainty and contagion fears reduced the overall number of outpatients, thus reducing the gross number of antibiotics prescribed. From April 2020 until July 2020, the numbers steadily increased for most antibiotics, including clindamycin, doxycycline, nitrofurantoin and cephalexin, and returned to pre-pandemic levels for others, i.e., azithromycin [28,29,30,31]. Some studies suggest this rebound was due to the reinstitution of in-person visits and telemedicine [32].
In the majority of cases, first-line contact was primary care physicians. As they rely heavily on antibiotics in their daily practices, with more than 81% of all antibiotic usage in the UK, the pandemic was no exception [33]. On average, 74% of COVID patients received antibiotic treatment, whereas only 17.4% had confirmed bacterial super/coinfection, with some studies suggesting a lower number at 8% of bacterial coinfections [6,34]. More often than not, they treated COVID-19 patients as they would any other community-acquired pneumonia, despite being unable to affect the virus itself. This is because any COVID-19 infection could have been easily presented as a bacterial superinfection, which is a daunting, sometimes impossible diagnosis [35,36]. The previous influenza pandemic in 2009 taught us that bacterial coinfection is a negative prognostic factor, hence the precautionary antibiotic prescribing [37]. More than 50% of viral pneumonia deaths correlate with bacterial superinfection [38,39], making it difficult to distinguish between rational and irrational antibiotic prescribing. An aggravating factor is that COVID-19 infection often presents with non-specific symptoms such as fever and persistent cough, making the differential diagnosis range-wide, especially in Third World countries, i.e., Zimbabwe, where tuberculosis and other bacterial infections as well as malaria are also very common [40], making antibiotic use a rational choice. Diarrhea is also a common symptom of COVID-19 infection, but it could also be the most common unwanted effect of antibiotic therapy. Early diarrhea could mean COVID-19, but late diarrhea should be treated as a possible Clostridium difficile infection, leading to further antibiotic therapy being indicated [41].
Some studies suggest that within the first 14 days of a positive COVID-19 infection, the most commonly used antibiotic agents were co-amoxiclav and doxycycline [1,33]. Other studies show that macrolides and cephalosporins (ceftriaxone) were among the most often prescribed antimicrobial therapy in mild to moderate COVID-19 infections, especially macrolides due to their anti-inflammatory properties [42,43]. The macrolide importance lies within their anti-inflammatory effects on airways. They have been shown to downregulate prolonged inflammation, reduce mucus production and decrease bacterial pathogenicity. Self-limiting adverse effects such as nausea, vomiting and diarrhea are easy to manage, making them generally well accepted by the patients [44]. Increased consumption of the same or similar antimicrobials is a worldwide phenomenon as multiple studies conducted in geographically distant areas have concluded [42,45]. This alone led to the doubling of azithromycin consumption globally [42]. Increased consumption of azithromycin, ceftriaxone and levofloxacin was noted in intensive care units as early as April 2020 [45]. Similar widespread use of azithromycin has been implicated in trachoma treatment among children from 1 to 9 years of age. As a form of prevention, azithromycin is periodically used to prevent infection with Chlamydia trachomatis. Although it has been proven effective in preventing trachoma, caution is advised, as it has the potential to increase macrolide resistance in C. trachomatis as well as in other common pathogens. Follow-up studies show macrolide resistance in S. pneumoniae with incentive to decrease over time. E. coli and S. aureus resistance has also been noted [46,47,48]. Given that there was already a minimum of 30% of overall frequent bacterial species resistant to azithromycin before its use spiked, it is believed that reason for concern is real [49].
Furthermore, viral M-pro protease could be the target of the fluoroquinolones and block viral multiplication, thus justifying their role as a complementary therapy in moderate to severe illness [50]. Fluoroquinolones could prove beneficial in limiting oxidative lung reaction by modulating the NO pathway, reducing lung damage and increasing survival rate [51]. The combined antiviral and modulatory effects of fluoroquinolones are enough for them to fit into the COVID-19 treatment guidelines and recommendations [50].
The empiric use of the aforementioned antibiotic agents in primary care is consistent with their therapeutic use in most hospital settings and could have been negotiated as a precaution [52]; however, the WHO has recommended using antibiotics only if a bacterial coinfection is highly suspected in mild to moderate COVID cases [53].
COVID-associated bacterial superinfection is a common cause of hospital-acquired pneumonia. Guidelines suggest treatment with broad-spectrum antibiotics; namely, third-generation cephalosporines (ceftazidime and cefepime), quinolones and carbapenems or according to the antibiogram results of the cultivated organism [54].
Other studies suggest that antibiotic usage is of poor predictive value in terms of survival [55]. It could even deplete the gut microbiota, leading to decreased immune function and lower antibody production, thus snowballing into more infections [56] and proving restrictive guidelines more reasonable [57].
While the SARS-CoV-2 presented a great challenge itself, an additional issue during COVID-19 patient treatment was the superinfections. Causes of superinfections during COVID-19 include weakened immune responses, prolonged hospital stays, invasive medical procedures, the overuse or misuse of antibiotics, as well as corticosteroid therapy [58]. In addition to antimicrobial therapy, glucocorticoids were administered as supportive therapy in fighting COVID-19 as a proven effective treatment, mainly because of their immunosuppressive effect, preventing inflammation and excessive tissue damage (predominantly in the lungs). This has been shown as an efficient method in patients with severe illness and proven to decrease overall 28-day mortality [59]. Suppressing immunity, however, has well-known disadvantages, enabling superinfections in treated patients, mostly bacterial, as well as viral and fungal [60,61]. Most studies define co-infection when it is diagnosed within the first 48 h, whereas superinfections are those infections diagnosed 48 h after hospital admission or disease onset.
Although the WHO recently declared the end of the COVID-19 global health emergency [62], the evidence regarding superinfections during COVID-19 incidence, causes, risk factors and their clinical significance is still scarce. In 2021, a cross-sectional study involving 399 patients diagnosed with COVID-19 in Colombia explored the prevalence of bacterial superinfection as well as its causative pathogens. The results showed that bacterial superinfection prevalence in hospitalized patients was 49.6%, and Klebsiella pneumoniae and Klebsiella oxytoca was the causative pathogen in most cases. Staphylococcus aureus was the second most frequent [60]. The summarized findings of the most frequent pathogens of this study have been adapted and presented in Figure 1.
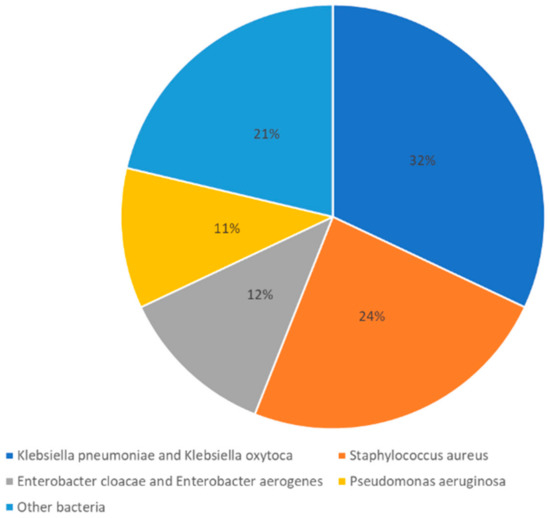
Figure 1.
Most frequent causative pathogens of bacterial superinfections in hospitalized patients with COVID-19. Adapted from a cross-section study [60].
Similar results have been reported by a more recent study regarding superinfections in patients with COVID-19 admitted to the ICU; however, with a much smaller sample size [63]. Another recent retrospective study was done in Western Romania with a larger sample size that included 407 eligible patients that were hospitalized for COVID-19. The study reported a total of 46 samples positive for pathogenic bacteria in their sputum cultures, while 67 patients had positive sputum cultures for commensal bacteria associated with respiratory tissue. Additionally, 51 sputum cultures were positive for fungi. The remaining sputum cultures showed no signs of infection. Figure 2 adapted and summarized these findings [64].
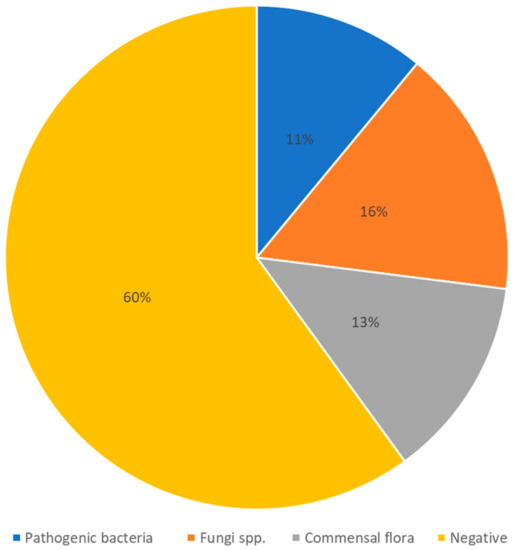
Figure 2.
Most frequently isolatedpathogens from sputum of hospitalized patients with COVID-19. Adapted from a retrospective study [64].
Regarding fungi, the most frequently isolated were the opportunistic pathogens Candida spp. and Aspergillus spp. Notable was also an increased number of yeast infections and infections by the highly opportunistic Mucorales spp., which causes mucormycosis [64,65]. For example, mucormycosis in patients with COVID-19 has a mortality rate of around 30%. Hyperglycemia was identified as the main predisposing factor induced by steroid therapy; occasionally it was preexisting because of diabetes mellitus type 2 or both [65].
Among pathogenic bacteria, Pseudomonas aeruginosa was isolated in 31.5% of positive sputum samples. The second most common was Klebsiella pneumoniae in 26.2% of positive sputum samples.
Regarding commensal flora, Streptococcus pneumoniae was isolated in 34.1%, followed by methicillin-sensitive (21.6%) and methicillin-resistant (17.0%) Staphylococcus aureus [64].
The most concerning finding was that almost 80% of isolated bacteria showed multidrug resistance [64]. Similar findings can be seen in a study conducted by Alcantar-Curiel et al., which concluded that the number is even above 80% [66]. Using non-selective, non-effective antimicrobials in cases like these could promote multidrug resistance even further and continue the chain reaction.
4. Antimicrobial Stewardship
Antimicrobial stewardship is a time-consuming and tedious process of planning, organizing and counselling physicians all over the world in what are the best treatment options with minimal unintended effects. It is also a necessity, given that the availability of antimicrobials is the most powerful treatment option. In Europe, for example, the European Center for Disease Control (CDC) is the main stewardship body for the European Union and the European Economic Area (EEA) [67,68,69,70]. The Centres for Disease Control and Prevention (CDC) is responsible for the US area. Umbrella organizations promote stewardship and publish guidelines, but real-time stewardship, also called diagnostic stewardship, is one of the key roles of clinical microbiology laboratories. Real-time correlation with clinical findings, biochemical analysis (namely, procalcitonin serum levels as a sepsis biomarker) and PCR results can optimize therapy usage by discontinuing or changing treatment plans [71]. A conservative procalcitonin cutoff value in patients with COVID-19 was established at PCT 0.25 ng/mL, with PCT values below 0.25 ng/mL being strongly indicative against bacterial coinfection, thus justifying wide-spectrum antibiotics being withheld [72]. Antimicrobial stewardship programs were already implemented in most hospital settings and healthcare systems but there were none in disaster planning or emergency response. Prior to the COVID-19 pandemic, in 2018, a journal article summarized the outcome of a survey conducted among 244 active members of different stewardship programs. The outcome reported was, in some measure, 85% effectiveness in the past 2 years, with 67% reported savings and 20% reported decreased rate in drug-resistant microbials [73]. Showing how effective these programs can be and how seamless they could be, it is frustrating that most microbiology laboratories were swamped with PCR COVID-19 testing and there was not enough manpower to coordinate PCR test results with clinical findings in real time [74,75]. As we can now see, antimicrobial stewardship was yet another COVID-19 victim. Global panic, changes in clinical care delivery and global supply chain issues contributed to the downfall of stewardship programs [71]. In one of New York’s hospitals, the main problem with conducting ASPs during the pandemic was consistency. With the increased influx of critically ill patients, many wards, for example, pediatric wards, were transformed into ICUs. Newly made ICUs had outsourced staff that were not familiar with the hospital’s operating procedures and that is when ASP programs started to fall behind, by postscript reviewing of the justification for different antimicrobials administered [76]. If they had been properly staffed and prepared, this could have been an opportunity to conduct ASPs and maintain responsible antibiotic usage [74]. Between the first two Waves in September 2020, a multidisciplinary team consisting of an array of medical specialists evaluated therapeutic effects during the 1st Wave to prepare and optimize therapy for the 2nd Wave. This led to discouragement in the use of some wide-spectrum antibiotics such as meropenem without altering the overall survival rate [77]. By providing clinically adequate patient evaluation, maintaining quality control at a high level, speeding up diagnostics, having a reasonable approach to therapy and continuously re-evaluating common practices, we could curb the AMR [78,79].
5. AMR Stewardship Challenges during and Post-COVID AMR Status
Whereas in 2019 the CDC saw a 19% reduction in MDR bacterial infections, 2020 has told a different story. An estimated 15% increase from 2019 to 2020 in MDR hospital infections has been noted. The COVID-19 pandemic has influenced all measures for battling against antibiotic resistance. Stewardship programs were less effective by testing less and allowing more. Preventing other hospital-acquired infections was much harder because more patients were in need of invasive medical devices such as catheters and intravenous cannulas. These foreign bodies can form a biofilm consisting of many different bacterial and fungal species [69,80]. It is often specific to an individual, but it mostly differs from ward to ward. Biofilm formation is one of the risk factors for contracting multidrug-resistant bacterial infection [81]. Antibiotics have been uncritically used, even for mild to moderate COVID-19 disease, thus increasing antimicrobial burden, inducing bacterial adaptation mechanisms and increasing resistance. According to the CDC’s 2022 special report, there is a concerning threat following this pandemic. The CDC has divided most common resistant pathogens into three groups based on the level of concern for global health: urgent, serious and concerning [69,82]. We provide summarized information regarding these groups in Table 1.

Table 1.
Summarized CDC information regarding antimicrobial resistant pathogens based on the level of concern after COVID-19.
A study conducted by Langford et al. suggests that Gram-positive bacteria, specifically methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococci (VRE) have not been affected by COVID-19, as there was no change in the incidence of these pathogens during the pandemic [83]. On the contrary, a more comprehensive systematic review conducted by Abubakar et al. points out that the pandemic only sped up an already rising incidence and prevalence of both MRSA and VRE. This discrepancy could be explained by the varying incidence trends in different regions, hospitals and even in different hospital wards [84]. Nonetheless, multiple studies show a significant increase in Gram-negative resistant bacteria [83,85]. A systematic review conducted by Sulayyim et al. reviewed 23 studies, all of them showing increases in the number of antibiotic-resistant bacteria. The most commonly isolated species were Acinetobacter baumannii, Klebsiella pneumoniae, Escherichia coli and Pseudomonas aeruginosa, without reporting increased MRSA or VRE incidence [86]. Infections with resistant Gram-negative bacteria also had a higher incidence in one Iranian hospital. Escherichia coli was the most commonly isolated bacteria with antibiogram results, showing resistance to ampicillin, cefazolin and cefepime in 89.6%, 74.0% and 71.4% of bacteria, respectively. The second most common was Klebsiella pneumoniae, which also showed the highest resistance to ampicillin (98.1%), levofloxacin (92.9%) and ceftazidime (92.4%). Next in line was Pseudomonas aeruginosa, with resistance to imipenem (91.8%), meropenem (91.5%) and cefepime (87.1%), and finally, Acinetobacter baumannii, with around 94% of samples being resistant to cephalosporins (cefotaxime, ceftazidime and ceftriaxone) [85]. Similarly, other studies point out that Klebsiella pneumoniae and Acinetobacter baumannii among other pathogens also show resistance numbers around 80% [87,88]. Klebsiella pneumoniae has also been shown to be a problem in Italy, spreading across the ICU via endotracheal tubes and prolonged patient-staff contact [89]. Comparing these percentages with pre-pandemic numbers strongly suggests that AMR poses a more serious threat to public health because of the pandemic. For example, the numbers were compared in a Turkish study by Bahce et al., showing increased resistance to ceftazidime and levofloxacin in Pseudomonas aeruginosa, as well as higher counts of resistant Acinetobacter baumannii [90].
6. Other Measures
Social distancing, avoiding close-up meetings with others, is one of the key public measures undertaken to slow down the rapid spread of COVID-19. Social distancing is meant to slow down the viral spread among asymptomatic individuals while isolation is meant for symptomatic patients and quarantining is a way of restricting the movement of those in direct contact with infected patients [91,92]. It is shown that it not only lowers the rate of infection but also reduces individual risk of contracting the novel coronavirus as well as other respiratory transmitted viruses [92,93]. There is a low chance of a single measure being effective but combining these 3 aforementioned measures has proven to be of value. Numbers suggest that the timely implementation of these measures reduces the infection rate by a minimum of 80% [94]. Social distancing has proven effective in preventing all types of respiratory infections, not only COVID-19 [93]. Physical distancing was not sustainable for lower income classes, as they were being isolated from work, making it difficult to comply with strict restrictions thus leading to a low compliance rate and low effectiveness of physical distancing.
Travel restrictions might contribute to decreasing AMR and the prevalence of AROs. People coming from countries with high AMR prevalence could become unaffected carriers of multidrug-resistant pathogens and move them from one location to another, thus creating a new AMR gene pool [95,96]. We can only speculate whether short-term travel restrictions have any long-term consequences.
Telephone appointments are playing a bigger role in primary care settings. To avoid transmission among other patients and staff, primary care physicians opted to advise remotely. This made assessing patients’ health much more challenging, as it felt riskier and wrong not to give medicine to worried, ill patients. Therefore, many GPs prescribed antibiotics to cover any possibility [97,98]. There is no doubt that remote consultations are becoming more popular among both patients and doctors, but for now, there is inconclusive evidence showing higher prescription rates. For instance, for UTIs, general practitioners are more likely to prescribe antibiotics remotely [99]. However, few studies also show higher prescriptions for RTI, and some show lower prescription rates [100,101]. To summarize, telemedicine might have fast-tracked the patient–doctor interaction but has not made a significant difference [32].
Face masks were and still are a huge controversy in the public eye, but the scientific community mostly agree that they were effective at reducing germ transmission. A prime example to support this claim is that there was a significant decrease in the number of reported influenza cases and pneumonia in general [102]. From an environmental aspect, besides plastic pollution, the use of facial masks has another problem and it is their disposal. Study by Zhou et al. investigated the dissemination of antibiotic-resistance genes (ARGs) through discarded facemasks and revealed that these masks may potentially offer a hiding place for the accumulation of ARGs in the marine ecosystem and thus contribute to increased AMR [103].
7. Future Directions
In general, the chance of spreading AMR is reduced by using precise and effective antimicrobial therapy in patients; it could potentially save the life of a patient with a serious infection caused by bacteria resistant to antibiotics. The problem with common laboratory methods—that they have long turnaround times and need up to a few days to identify and classify bacteria—should be explored to a greater extent. One of the main goals of the “National Action Plan for Combating Antibiotic-Resistant Bacteria 2020–2025” is to develop innovative rapid diagnostic tests to identify and characterize resistant bacteria. Development of these tests is costly, technically demanding and requires utility study on their use in clinical settings. Currently, there are some genotypic tests approved by the FDA which identify genes and mutations responsible for AMR and give results in less than a few hours but they still need to be proven in clinical practice [104]. This can be achieved by further developing stewardship programs and continuously educating medical staff as well as the general population [105]. Future pandemics are unavoidable, and healthcare systems all over the globe should work together towards finding effective and sustainable prevention methods and predicting future pathogens.
8. Conclusions
Unjustified antimicrobial pharmacotherapy was a problem long before the pandemic outbreak. Overuse of antibiotics during the pandemic has only exacerbated this issue. As identified by the CDC and summarized in this review, the pathogens with levels of antimicrobial resistance most affected by the overuse of antibiotics during the pandemic are Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa and Acinetobacter baumannii. Antimicrobial stewardship programs are crucial for promoting the responsible use of antibiotics; however, they have been greatly impacted by the COVID-19 pandemic.
Pharmacovigilance regarding antimicrobial use and effective antimicrobial stewardship are crucial in the fight against AMR. This requires coordinated efforts between clinical microbiology laboratories, healthcare providers and policymakers, as well as the education of patients about this issue. Efficient antimicrobial stewardship can mitigate the risk of antibiotic-resistant infections and ensure that future pandemics do not divert attention and resources away from this critical health threat.
Author Contributions
Writing the manuscript O.K. and F.K., updating text A.P., A.L. and L.K., literature searches V.M. and T.O.K., critical reviewing of the manuscript A.P., F.K., A.A.T., R.S. and M.S., organization and editing of the manuscript M.S., R.S., A.A.T. and O.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rizvi, S.G.; Ahammad, S.Z. COVID-19 and antimicrobial resistance: A cross-study. Sci. Total Environ. 2022, 807, 150873. [Google Scholar] [CrossRef]
- Lai, C.C.; Chen, S.Y.; Ko, W.C.; Hsueh, P.R. Increased antimicrobial resistance during the COVID-19 pandemic. Int. J. Antimicrob. Agents 2021, 57, 106324. [Google Scholar] [CrossRef] [PubMed]
- Knight, G.M.; Glover, R.E.; McQuaid, C.F.; Olaru, I.D.; Gallandat, K.; Leclerc, Q.J.; Fuller, N.M.; Willcocks, S.J.; Hasan, R.; van Kleef, E.; et al. Antimicrobial resistance and COVID-19: Intersections and implications. eLife 2021, 10, e64139. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Bornman, C.; Zafer, M.M. Antimicrobial Resistance Threats in the emerging COVID-19 pandemic: Where do we stand? J. Infect. Public Health 2021, 14, 555–560. [Google Scholar] [CrossRef]
- Jonas, O.B.; Irwin, A.; Berthe, F.C.J.; Le Gall, F.G.; Marquez, P.V. Drug-Resistant Infections: A Threat to Our Economic Future (Vol. 2): Final Report (English); HNP/Agriculture Global Antimicrobial Resistance Initiative: Washington, DC, USA, 2017. [Google Scholar]
- Ruiz-Garbajosa, P.; Cantón, R. COVID-19: Impact on prescribing and antimicrobial resistance. Rev. Esp. Quimioter. 2021, 34 (Suppl. S1), 63–68. [Google Scholar] [CrossRef]
- McEwen, S.A.; Collignon, P.J. Antimicrobial Resistance: A One Health Perspective. Microbiol. Spectr. 2018, 6, 521–547. [Google Scholar] [CrossRef]
- Christaki, E.; Marcou, M.; Tofarides, A. Antimicrobial Resistance in Bacteria: Mechanisms, Evolution, and Persistence. J. Mol. Evol. 2020, 88, 26–40. [Google Scholar] [CrossRef]
- Rahman, S.; Kesselheim, A.S.; Hollis, A. Persistence of resistance: A panel data analysis of the effect of antibiotic usage on the prevalence of resistance. J. Antibiot. 2023, 76, 270–278. [Google Scholar] [CrossRef]
- D’Costa, V.M.; King, C.E.; Kalan, L.; Morar, M.; Sung, W.W.L.; Schwarz, C.; Froese, D.; Zazula, G.; Calmels, F.; Debruyne, R.; et al. Antibiotic resistance is ancient. Nature 2011, 477, 451–461. [Google Scholar] [CrossRef]
- Ferri, M.; Ranucci, E.; Romagnoli, P.; Giaccone, V. Antimicrobial resistance: A global emerging threat to public health systems. Crit. Rev. Food Sci. Nutr. 2017, 57, 2857–2876. [Google Scholar] [CrossRef]
- Asokan, G.V.; Ramadhan, T.; Ahmed, E.; Sanad, H. WHO Global Priority Pathogens List: A Bibliometric Analysis of Medline-PubMed for Knowledge Mobilization to Infection Prevention and Control Practices in Bahrain. Oman Med. J. 2019, 34, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Modi, A.R.; Kovacs, C.S. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleve. Clin. J. Med. 2020, 87, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Richards, M.J.; Edwards, J.R.; Culver, D.H.; Gaynes, R.P. Nosocomial infections in medical intensive care units in the United States. National Nosocomial Infections Surveillance System. Crit. Care Med. 1999, 27, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Moyes, R.B.; Reynolds, J.; Breakwell, D.P. Differential staining of bacteria: Gram stain. Curr. Protoc. Microbiol. 2009, 15, A.3C.1–A.3C.8. [Google Scholar] [CrossRef]
- Lee, C.R.; Lee, J.H.; Park, M.; Park, K.S.; Bae, I.K.; Kim, Y.B.; Cha, C.J.; Jeong, B.C.; Lee, S.H. Biology of Acinetobacter baumannii: Pathogenesis, Antibiotic Resistance Mechanisms, and Prospective Treatment Options. Front. Cell Infect. Microbiol. 2017, 7, 55. [Google Scholar] [CrossRef]
- Pachori, P.; Gothalwal, R.; Gandhi, P. Emergence of antibiotic resistance. Genes Dis. 2019, 6, 109–119. [Google Scholar] [CrossRef]
- Paterson, D.L. Resistance in gram-negative bacteria: Enterobacteriaceae. Am. J. Med. 2006, 119, S20–S28, discussion S62–S70. [Google Scholar] [CrossRef]
- Mijović, G.; Čizmović, L.; Vuković, M.N.; Stamatović, S.; Lopičić, M. Antibiotic consumption in hospitals and resistance rate of Klebsiella pneumoniae and Escherichia coli in Montenegro. Acta Clin. Croat. 2020, 59, 469–479. [Google Scholar] [CrossRef]
- Santajit, S.; Indrawattana, N. Mechanisms of Antimicrobial Resistance in ESKAPE Pathogens. Biomed Res. Int. 2016, 2016, 2475067. [Google Scholar] [CrossRef]
- Russell, J.N.; Yost, C.K. Alternative, environmentally conscious approaches for removing antibiotics from wastewater treatment systems. Chemosphere 2021, 263, 128177. [Google Scholar] [CrossRef] [PubMed]
- Watkinson, A.J.; Murby, E.J.; Costanzo, S.D. Removal of antibiotics in conventional and advanced wastewater treatment: Implications for environmental discharge and wastewater recycling. Water Res. 2007, 41, 4164–4176. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt-Farrell, N. The landscape of antibiotic resistance. Environ. Health Perspect. 2009, 117, A244–A250. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Guo, J.; Jiang, Y.; Shao, Y. High concentration and high dose of disinfectants and antibiotics used during the COVID-19 pandemic threaten human health. Environ. Sci. Eur. 2021, 33, 11. [Google Scholar] [CrossRef] [PubMed]
- Tran, N.H.; Hoang, L.; Nghiem, L.D.; Nguyen, N.M.H.; Ngo, H.H.; Guo, W.; Trinh, Q.T.; Mai, N.H.; Chen, H.; Nguyen, D.D.; et al. Occurrence and risk assessment of multiple classes of antibiotics in urban canals and lakes in Hanoi, Vietnam. Sci. Total Environ. 2019, 692, 157–174. [Google Scholar] [CrossRef]
- Chen, X.; Lei, L.; Liu, S.; Han, J.; Li, R.; Men, J.; Li, L.; Wei, L.; Sheng, Y.; Yang, L.; et al. Occurrence and risk assessment of pharmaceuticals and personal care products (PPCPs) against COVID-19 in lakes and WWTP-river-estuary system in Wuhan, China. Sci. Total Environ. 2021, 792, 148352. [Google Scholar] [CrossRef]
- Buehrle, D.J.; Nguyen, M.H.; Wagener, M.M.; Clancy, C.J. Impact of the Coronavirus Disease 2019 Pandemic on Outpatient Antibiotic Prescriptions in the United States. Open Forum Infect. Dis. 2020, 7, ofaa575. [Google Scholar] [CrossRef]
- Armitage, R.; Nellums, L.B. Antibiotic prescribing in general practice during COVID-19. Lancet Infect. Dis. 2021, 21, e144. [Google Scholar] [CrossRef]
- Alzueta, N.; Echeverría, A.; García, P.; Sanz, L.; Gil-Setas, A.; Beristain, X.; Aldaz, P.; Garjón, J. Impact of COVID-19 Pandemic in Antibiotic Consumption in Navarre (Spain): An Interrupted Time Series Analysis. Antibiotics 2023, 12, 318. [Google Scholar] [CrossRef]
- Bednarčuk, N.; Golić Jelić, A.; Stoisavljević Šatara, S.; Stojaković, N.; Marković Peković, V.; Stojiljković, M.P.; Popović, N.; Škrbić, R. Antibiotic Utilization during COVID-19: Are We Over-Prescribing? Antibiotics 2023, 12, 308. [Google Scholar] [CrossRef]
- Yao, P.; Clark, S.; Gogia, K.; Hafeez, B.; Hsu, H.; Greenwald, P. Antibiotic Prescribing Practices: Is There a Difference between Patients Seen by Telemedicine Versus Those Seen In-Person? Telemed. J. e-Health 2020, 26, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Aylin, P.; Rawson, T.; Gilchrist, M.; Majeed, A.; Holmes, A. Investigating the impact of COVID-19 on primary care antibiotic prescribing in North West London across two epidemic waves. Clin. Microbiol. Infect. 2021, 27, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Chedid, M.; Waked, R.; Haddad, E.; Chetata, N.; Saliba, G.; Choucair, J. Antibiotics in treatment of COVID-19 complications: A review of frequency, indications, and efficacy. J. Infect. Public Health 2021, 14, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Abelenda-Alonso, G.; Padullés, A.; Rombauts, A.; Gudiol, C.; Pujol, M.; Alvarez-Pouso, C.; Jodar, R.; Carratalà, J. Antibiotic prescription during the COVID-19 pandemic: A biphasic pattern. Infect. Control Hosp. Epidemiol. 2020, 41, 1371–1372. [Google Scholar] [CrossRef]
- Sehgal, K.; Fadel, H.J.; Tande, A.J.; Pardi, D.S.; Khanna, S. Outcomes in Patients with SARS-CoV-2 and Clostridioides difficile Coinfection. Infect. Drug Resist. 2021, 14, 1645–1648. [Google Scholar] [CrossRef] [PubMed]
- Viasus, D.; Paño-Pardo, J.R.; Pachón, J.; Campins, A.; López-Medrano, F.; Villoslada, A.; Fariñas, M.C.; Moreno, A.; Rodríguez-Baño, J.; Oteo, J.A.; et al. Factors associated with severe disease in hospitalized adults with pandemic (H1N1) 2009 in Spain. Clin. Microbiol. Infect. 2011, 17, 738–746. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Mirzaei, R.; Goodarzi, P.; Asadi, M.; Soltani, A.; Aljanabi, H.A.A.; Jeda, A.S.; Dashtbin, S.; Jalalifar, S.; Mohammadzadeh, R.; Teimoori, A.; et al. Bacterial co-infections with SARS-CoV-2. IUBMB Life 2020, 72, 2097–2111. [Google Scholar] [CrossRef]
- Chitungo, I.; Dzinamarira, T.; Nyazika, T.K.; Herrera, H.; Musuka, G.; Murewanhema, G. Inappropriate Antibiotic Use in Zimbabwe in the COVID-19 Era: A Perfect Recipe for Antimicrobial Resistance. Antibiotics 2022, 11, 244. [Google Scholar] [CrossRef]
- Granata, G.; Schiavone, F.; Pipitone, G.; Taglietti, F.; Petrosillo, N. Antibiotics Use in COVID-19 Patients: A Systematic Literature Review. J. Clin. Med. 2022, 11, 7207. [Google Scholar]
- Giacomelli, A.; Ridolfo, A.L.; Oreni, L.; Vimercati, S.; Albrecht, M.; Cattaneo, D.; Rimoldi, S.G.; Rizzardini, G.; Galli, M.; Antinori, S. Consumption of antibiotics at an Italian university hospital during the early months of the COVID-19 pandemic: Were all antibiotic prescriptions appropriate? Pharmacol. Res. 2021, 164, 105403. [Google Scholar] [CrossRef] [PubMed]
- Parasher, A. COVID-19: Current understanding of its Pathophysiology, Clinical presentation and Treatment. Postgrad. Med. J. 2021, 97, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Shinkai, M.; Rubin, B.K. Macrolides and airway inflammation in children. Paediatr. Respir. Rev. 2005, 6, 227–235. [Google Scholar] [CrossRef]
- Nestler, M.J.; Godbout, E.; Lee, K.; Kim, J.; Noda, A.J.; Taylor, P.; Pryor, R.; Markley, J.D.; Doll, M.; Bearman, G.; et al. Impact of COVID-19 on pneumonia-focused antibiotic use at an academic medical center. Infect. Control Hosp. Epidemiol. 2021, 42, 915–916. [Google Scholar] [CrossRef] [PubMed]
- Haug, S.; Lakew, T.; Habtemariam, G.; Alemayehu, W.; Cevallos, V.; Zhou, Z.; House, J.; Ray, K.; Porco, T.; Rutar, T.; et al. The decline of pneumococcal resistance after cessation of mass antibiotic distributions for trachoma. Clin. Infect. Dis. 2010, 51, 571–574. [Google Scholar] [CrossRef]
- Gaynor, B.D.; Chidambaram, J.D.; Cevallos, V.; Miao, Y.; Miller, K.; Jha, H.C.; Bhatta, R.C.; Chaudhary, J.S.; Osaki Holm, S.; Whitcher, J.P.; et al. Topical ocular antibiotics induce bacterial resistance at extraocular sites. Br. J. Ophthalmol. 2005, 89, 1097–1099. [Google Scholar] [CrossRef]
- O’Brien, K.S.; Emerson, P.; Hooper, P.J.; Reingold, A.L.; Dennis, E.G.; Keenan, J.D.; Lietman, T.M.; Oldenburg, C.E. Antimicrobial resistance following mass azithromycin distribution for trachoma: A systematic review. Lancet Infect. Dis. 2019, 19, e14–e25. [Google Scholar] [CrossRef]
- Serisier, D.J. Risks of population antimicrobial resistance associated with chronic macrolide use for inflammatory airway diseases. Lancet Respir. Med. 2013, 1, 262–274. [Google Scholar] [CrossRef]
- Karampela, I.; Dalamaga, M. Could Respiratory Fluoroquinolones, Levofloxacin and Moxifloxacin, Prove to be Beneficial as an Adjunct Treatment in COVID-19? Arch. Med. Res. 2020, 51, 741–742. [Google Scholar] [CrossRef]
- Enoki, Y.; Ishima, Y.; Tanaka, R.; Sato, K.; Kimachi, K.; Shirai, T.; Watanabe, H.; Chuang, V.T.; Fujiwara, Y.; Takeya, M.; et al. Pleiotropic Effects of Levofloxacin, Fluoroquinolone Antibiotics, against Influenza Virus-Induced Lung Injury. PLoS ONE 2015, 10, e0130248. [Google Scholar] [CrossRef]
- Bendala Estrada, A.D.; Calderón Parra, J.; Fernández Carracedo, E.; Muiño Míguez, A.; Ramos Martínez, A.; Muñez Rubio, E.; Rubio-Rivas, M.; Agudo, P.; Arnalich Fernández, F.; Estrada Perez, V.; et al. Inadequate use of antibiotics in the COVID-19 era: Effectiveness of antibiotic therapy. BMC Infect. Dis. 2021, 21, 1144. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Clinical Management: Living Guidance, 25 January 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Fattorini, L.; Creti, R.; Palma, C.; Pantosti, A. Bacterial coinfections in COVID-19: An underestimated adversary. Ann. Ist. Super. Sanita 2020, 56, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Rosca, A.; Balcaen, T.; Lanoix, J.P.; Michaud, A.; Moyet, J.; Marcq, I.; Schmit, J.L.; Bloch, F.; Deschasse, G. Mortality risk and antibiotic use for COVID-19 in hospitalized patients over 80. Biomed. Pharmacother. 2022, 146, 112481. [Google Scholar] [CrossRef] [PubMed]
- Kelly, P. Antibiotics blunt flu immunity. Science 2019, 366, 197–198. [Google Scholar] [CrossRef]
- Sieswerda, E.; de Boer, M.G.J.; Bonten, M.M.J.; Boersma, W.G.; Jonkers, R.E.; Aleva, R.M.; Kullberg, B.J.; Schouten, J.A.; van de Garde, E.M.W.; Verheij, T.J.; et al. Recommendations for antibacterial therapy in adults with COVID-19—An evidence based guideline. Clin. Microbiol. Infect. 2021, 27, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Boulos, M.; Bassal, T.; Layyous, A.; Basheer, M.; Assy, N. Inflammation in COVID-19: A Risk for Superinfections. COVID 2022, 2, 1609–1624. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; Cavalcanti, A.B.; et al. Association between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef]
- Cataño-Correa, J.C.; Cardona-Arias, J.A.; Porras Mancilla, J.P.; García, M.T. Bacterial superinfection in adults with COVID-19 hospitalized in two clinics in Medellín-Colombia, 2020. PLoS ONE 2021, 16, e0254671. [Google Scholar] [CrossRef]
- Ripa, M.; Galli, L.; Poli, A.; Oltolini, C.; Spagnuolo, V.; Mastrangelo, A.; Muccini, C.; Monti, G.; De Luca, G.; Landoni, G.; et al. Secondary infections in patients hospitalized with COVID-19: Incidence and predictive factors. Clin. Microbiol. Infect. 2021, 27, 451–457. [Google Scholar] [CrossRef]
- Harris, E. WHO Declares End of COVID-19 Global Health Emergency. JAMA 2023. [Google Scholar] [CrossRef]
- Yoon, S.M.; Lee, J.; Lee, S.M.; Lee, H.Y. Incidence and clinical outcomes of bacterial superinfections in critically ill patients with COVID-19. Front. Med. 2023, 10, 1079721. [Google Scholar] [CrossRef] [PubMed]
- Cut, T.G.; Mavrea, A.; Cumpanas, A.A.; Novacescu, D.; Oancea, C.I.; Bratosin, F.; Marinescu, A.R.; Laza, R.; Mocanu, A.; Pescariu, A.S.; et al. A Retrospective Assessment of Sputum Samples and Antimicrobial Resistance in COVID-19 Patients. Pathogens 2023, 12, 620. [Google Scholar] [CrossRef]
- Alshahawey, M.G.; El-Housseiny, G.S.; Elsayed, N.S.; Alshahrani, M.Y.; Wakeel, L.M.; Aboshanab, K.M. New insights on mucormycosis and its association with the COVID-19 pandemic. Future Sci. OA 2022, 8, FSO772. [Google Scholar] [CrossRef]
- Alcántar-Curiel, M.D.; Huerta-Cedeño, M.; Jarillo-Quijada, M.D.; Gayosso-Vázquez, C.; Fernández-Vázquez, J.L.; Hernández-Medel, M.L.; Zavala-Pineda, M.; Morales-Gil, M.; Hernández-Guzmán, V.A.; Bolaños-Hernández, M.I.; et al. Gram-negative ESKAPE bacteria bloodstream infections in patients during the COVID-19 pandemic. PeerJ 2023, 11, e15007. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2015. Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net); European Centre for Disease Prevention and Control: Solna, Sweden, 2015. [Google Scholar]
- America, S.f.H.E.O.; America, I.D.S.O.; Society, P.I.D. Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect. Control Hosp. Epidemiol. 2012, 33, 322–327. [Google Scholar] [CrossRef]
- COVID-19: US Impact on Antimicrobial Resistance; Special Report; US Department of Health and Human Services: Atlanta, GA, USA, 2022.
- Maganha de Almeida Kumlien, A.C.; González-Villalobos, E.; Balcázar, J.L. Making waves: How does the emergence of antimicrobial resistance affect policymaking? Water Res. 2021, 206, 117772. [Google Scholar] [CrossRef]
- Lynch, C.; Mahida, N.; Gray, J. Antimicrobial stewardship: A COVID casualty? J. Hosp. Infect. 2020, 106, 401–403. [Google Scholar] [CrossRef]
- Williams, E.J.; Mair, L.; de Silva, T.I.; Green, D.J.; House, P.; Cawthron, K.; Gillies, C.; Wigfull, J.; Parsons, H.; Partridge, D.G. Evaluation of procalcitonin as a contribution to antimicrobial stewardship in SARS-CoV-2 infection: A retrospective cohort study. J. Hosp. Infect. 2021, 110, 103–107. [Google Scholar] [CrossRef]
- Doernberg, S.B.; Abbo, L.M.; Burdette, S.D.; Fishman, N.O.; Goodman, E.L.; Kravitz, G.R.; Leggett, J.E.; Moehring, R.W.; Newland, J.G.; Robinson, P.A.; et al. Essential Resources and Strategies for Antibiotic Stewardship Programs in the Acute Care Setting. Clin. Infect. Dis. 2018, 67, 1168–1174. [Google Scholar] [CrossRef]
- Stevens, M.P.; Patel, P.K.; Nori, P. Involving antimicrobial stewardship programs in COVID-19 response efforts: All hands on deck. Infect. Control Hosp. Epidemiol. 2020, 41, 744–745. [Google Scholar] [CrossRef]
- Mayi, B.S.; Mainville, M.; Altaf, R.; Lanspa, M.; Vaniawala, S.; Ollerhead, T.A.; Raja, A. A Crucial Role for Antimicrobial Stewardship in the Midst of COVID-19. J. Microbiol. Biol. Educ. 2021, 22, ev22i1-2285. [Google Scholar] [CrossRef]
- Kubin, C.J.; Loo, A.S.; Cheng, J.; Nelson, B.; Mehta, M.; Mazur, S.; So, W.; Calfee, D.P.; Singh, H.K.; Greendyke, W.G.; et al. Antimicrobial stewardship perspectives from a New York City hospital during the COVID-19 pandemic: Challenges and opportunities. Am. J. Health Syst. Pharm. 2021, 78, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Chan, X.H.S.; O’Connor, C.J.; Martyn, E.; Clegg, A.J.; Choy, B.J.K.; Soares, A.L.; Shulman, R.; Stone, N.R.H.; De, S.; Bitmead, J.; et al. Reducing broad-spectrum antibiotic use in intensive care unit between first and second waves of COVID-19 did not adversely affect mortality. J. Hosp. Infect. 2022, 124, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Getahun, H.; Smith, I.; Trivedi, K.; Paulin, S.; Balkhy, H.H. Tackling antimicrobial resistance in the COVID-19 pandemic. Bull. World Health Organ. 2020, 98, 442–442A. [Google Scholar] [CrossRef]
- Medic, D.; Bozic Cvijan, B.; Bajcetic, M. Impact of Antibiotic Consumption on Antimicrobial Resistance to Invasive Hospital Pathogens. Antibiotics 2023, 12, 259. [Google Scholar] [CrossRef]
- Gonzalez-Zorn, B. Antibiotic use in the COVID-19 crisis in Spain. Clin. Microbiol. Infect. 2021, 27, 646–647. [Google Scholar] [CrossRef]
- Jamal, M.; Ahmad, W.; Andleeb, S.; Jalil, F.; Imran, M.; Nawaz, M.A.; Hussain, T.; Ali, M.; Rafiq, M.; Kamil, M.A. Bacterial biofilm and associated infections. J. Chin. Med. Assoc. 2018, 81, 7–11. [Google Scholar] [CrossRef]
- Kadri, S.S. Key Takeaways From the U.S. CDC’s 2019 Antibiotic Resistance Threats Report for Frontline Providers. Crit. Care Med. 2020, 48, 939–945. [Google Scholar] [CrossRef]
- Langford, B.J.; Soucy, J.R.; Leung, V.; So, M.; Kwan, A.T.H.; Portnoff, J.S.; Bertagnolio, S.; Raybardhan, S.; MacFadden, D.R.; Daneman, N. Antibiotic resistance associated with the COVID-19 pandemic: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2023, 29, 302–309. [Google Scholar] [CrossRef]
- Abubakar, U.; Al-Anazi, M.; Alanazi, Z.; Rodríguez-Baño, J. Impact of COVID-19 pandemic on multidrug resistant gram positive and gram negative pathogens: A systematic review. J. Infect. Public Health 2023, 16, 320–331. [Google Scholar] [CrossRef]
- Khoshbakht, R.; Kabiri, M.; Neshani, A.; Khaksari, M.N.; Sadrzadeh, S.M.; Mousavi, S.M.; Ghazvini, K.; Ghavidel, M. Assessment of antibiotic resistance changes during the COVID-19 pandemic in northeast of Iran during 2020–2022: An epidemiological study. Antimicrob. Resist. Infect. Control 2022, 11, 121. [Google Scholar] [CrossRef] [PubMed]
- Sulayyim, H.J.A.; Ismail, R.; Hamid, A.A.; Ghafar, N.A. Antibiotic Resistance during COVID-19: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 11931. [Google Scholar] [CrossRef] [PubMed]
- Boorgula, S.Y.; Yelamanchili, S.; Kottapalli, P.; Naga, M.D. An Update on Secondary Bacterial and Fungal Infections and Their Antimicrobial Resistance Pattern (AMR) in COVID-19 Confirmed Patients. J. Lab. Physicians 2022, 14, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Khurana, S.; Singh, P.; Sharad, N.; Kiro, V.V.; Rastogi, N.; Lathwal, A.; Malhotra, R.; Trikha, A.; Mathur, P. Profile of co-infections & secondary infections in COVID-19 patients at a dedicated COVID-19 facility of a tertiary care Indian hospital: Implication on antimicrobial resistance. Indian J. Med. Microbiol. 2021, 39, 147–153. [Google Scholar] [CrossRef]
- Tiri, B.; Sensi, E.; Marsiliani, V.; Cantarini, M.; Priante, G.; Vernelli, C.; Martella, L.A.; Costantini, M.; Mariottini, A.; Andreani, P.; et al. Antimicrobial Stewardship Program, COVID-19, and Infection Control: Spread of Carbapenem-Resistant Klebsiella Pneumoniae Colonization in ICU COVID-19 Patients. What Did Not Work? J. Clin. Med. 2020, 9, 2744. [Google Scholar] [CrossRef]
- Bahçe, Y.G.; Acer, Ö.; Özüdoğru, O. Evaluation of bacterial agents isolated from endotracheal aspirate cultures of COVID-19 general intensive care patients and their antibiotic resistance profiles compared to pre-pandemic conditions. Microb. Pathog. 2022, 164, 105409. [Google Scholar] [CrossRef]
- Aquino, E.M.L.; Silveira, I.H.; Pescarini, J.M.; Aquino, R.; Souza-Filho, J.A.; Rocha, A.S.; Ferreira, A.; Victor, A.; Teixeira, C.; Machado, D.B.; et al. Social distancing measures to control the COVID-19 pandemic: Potential impacts and challenges in Brazil. Cien. Saude Colet. 2020, 25, 2423–2446. [Google Scholar] [CrossRef]
- Fazio, R.H.; Ruisch, B.C.; Moore, C.A.; Granados Samayoa, J.A.; Boggs, S.T.; Ladanyi, J.T. Social distancing decreases an individual’s likelihood of contracting COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2023131118. [Google Scholar] [CrossRef]
- Kim, M.C.; Kweon, O.J.; Lim, Y.K.; Choi, S.H.; Chung, J.W.; Lee, M.K. Impact of social distancing on the spread of common respiratory viruses during the coronavirus disease outbreak. PLoS ONE 2021, 16, e0252963. [Google Scholar] [CrossRef]
- Daghriri, T.; Ozmen, O. Quantifying the Effects of Social Distancing on the Spread of COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 5566. [Google Scholar] [CrossRef]
- Murray, A.K. The Novel Coronavirus COVID-19 Outbreak: Global Implications for Antimicrobial Resistance. Front. Microbiol. 2020, 11, 1020. [Google Scholar] [CrossRef]
- Arcilla, M.S.; van Hattem, J.M.; Haverkate, M.R.; Bootsma, M.C.J.; van Genderen, P.J.J.; Goorhuis, A.; Grobusch, M.P.; Lashof, A.M.O.; Molhoek, N.; Schultsz, C.; et al. Import and spread of extended-spectrum β-lactamase-producing Enterobacteriaceae by international travellers (COMBAT study): A prospective, multicentre cohort study. Lancet Infect. Dis. 2017, 17, 78–85. [Google Scholar] [CrossRef]
- Borek, A.J.; Maitland, K.; McLeod, M.; Campbell, A.; Hayhoe, B.; Butler, C.C.; Morrell, L.; Roope, L.S.J.; Holmes, A.; Walker, A.S.; et al. Impact of the COVID-19 Pandemic on Community Antibiotic Prescribing and Stewardship: A Qualitative Interview Study with General Practitioners in England. Antibiotics 2021, 10, 1531. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T. A trade-off: Antimicrobial resistance and COVID-19. Bioethics 2021, 35, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, A.; Paone, S.; Martich, G.D.; Albert, S.M.; Shevchik, G.J. A comparison of care at e-visits and physician office visits for sinusitis and urinary tract infection. JAMA Intern. Med. 2013, 173, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Mehrotra, A.; Gidengil, C.A.; Poon, S.J.; Uscher-Pines, L.; Ray, K.N. Quality of Care for Acute Respiratory Infections during Direct-To-Consumer Telemedicine Visits for Adults. Health Aff. 2018, 37, 2014–2023. [Google Scholar] [CrossRef] [PubMed]
- Uscher-Pines, L.; Mulcahy, A.; Cowling, D.; Hunter, G.; Burns, R.; Mehrotra, A. Access and Quality of Care in Direct-to-Consumer Telemedicine. Telemed. J. e-Health 2016, 22, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Chiu, N.C.; Chi, H.; Tai, Y.L.; Peng, C.C.; Tseng, C.Y.; Chen, C.C.; Tan, B.F.; Lin, C.Y. Impact of Wearing Masks, Hand Hygiene, and Social Distancing on Influenza, Enterovirus, and All-Cause Pneumonia during the Coronavirus Pandemic: Retrospective National Epidemiological Surveillance Study. J. Med. Internet Res. 2020, 22, e21257. [Google Scholar] [CrossRef]
- Zhou, S.Y.; Lin, C.; Yang, K.; Yang, L.Y.; Yang, X.R.; Huang, F.Y.; Neilson, R.; Su, J.Q.; Zhu, Y.G. Discarded masks as hotspots of antibiotic resistance genes during COVID-19 pandemic. J. Hazard Mater. 2022, 425, 127774. [Google Scholar] [CrossRef]
- Banerjee, R.; Patel, R. Molecular diagnostics for genotypic detection of antibiotic resistance: Current landscape and future directions. JAC-Antimicrob. Resist. 2023, 5, dlad018. [Google Scholar] [CrossRef]
- Adebisi, Y.A.; Alaran, A.J.; Okereke, M.; Oke, G.I.; Amos, O.A.; Olaoye, O.C.; Oladunjoye, I.; Olanrewaju, A.Y.; Ukor, N.A.; Lucero-Prisno, D.E. COVID-19 and Antimicrobial Resistance: A Review. Infect. Dis. 2021, 14, 11786337211033870. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).