Itchy Capillary Malformations: Unusual Appearance of Meyerson Phenomenon, a Case Series

 ,
,  ,
,  ,
,  ,
, 
Abstract
1. Introduction
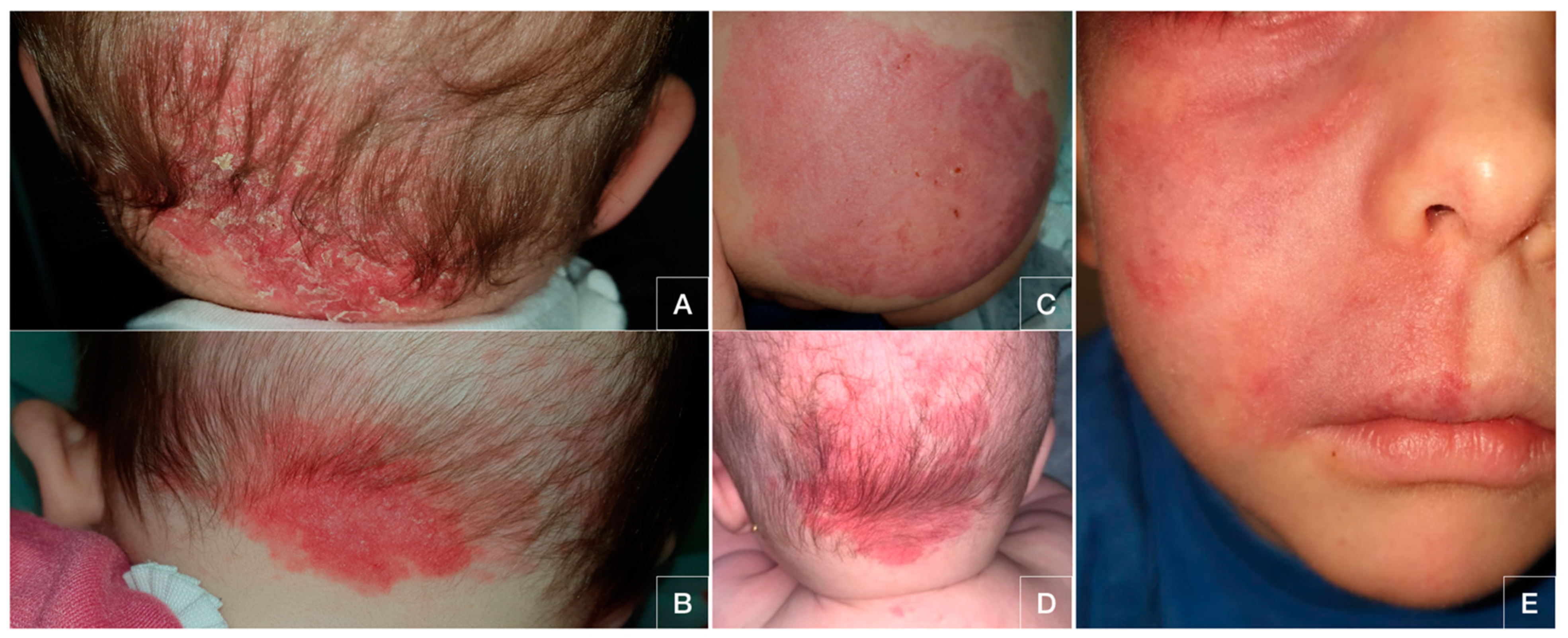
2. Case Presentation
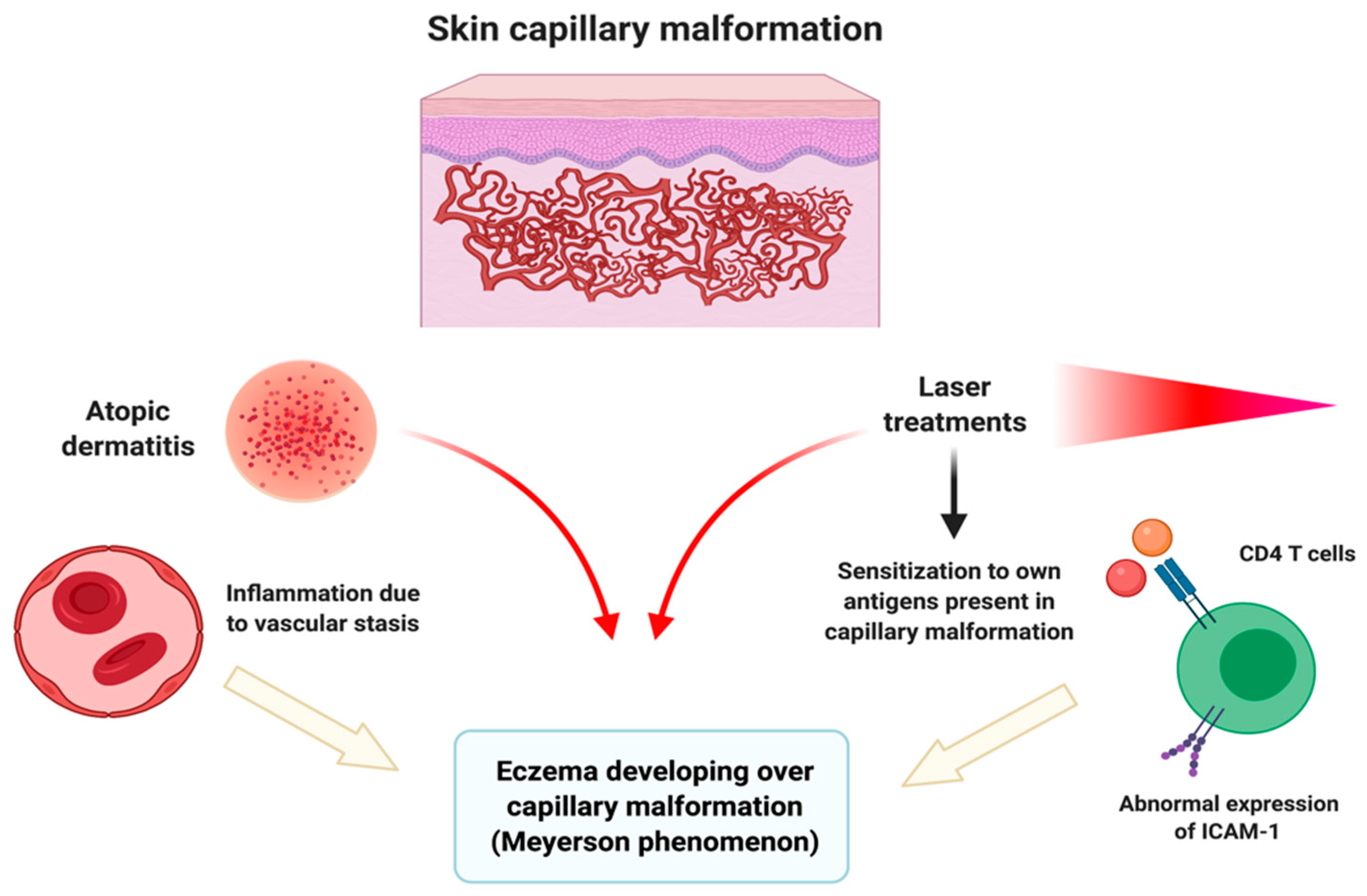
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meyerson, L.B. A peculiar papulosquamous eruption involving pigmented nevi. Arch. Dermatol. 1971, 103, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Rolland, S.; Kokta, V.; Marcoux, D. Meyerson phenomenon in children: Observation in five cases of congenital melanocytic nevi. Pediatr. Dermatol. 2009, 26, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Osorio, I.; González-Sabín, M.; Rodríguez-Díaz, E. Coexistence of Sutton and Meyerson nevi. Actas Dermosifiliogr. 2017, 108, 671. [Google Scholar] [CrossRef] [PubMed]
- Cook-Norris, R.H.; Zic, J.A.; Boyd, A.S. Meyerson’s naevus: A clinical and histopathological study of 11 cases. Australas J. Dermatol. 2008, 49, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Di Altobrando, A.; Neri, I.; Patrizi, A.; Tabanelli, M.; Misciali, C.; Baraldi, C.; Savoia, F. Congenital Melanocytic Nevi With Meyerson Phenomenon: Two Case Reports and Review of the Literature. Dermatol. Pr. Concept. 2020, 10, e2020064. [Google Scholar] [CrossRef] [PubMed]
- Ferneiny, M.; Pansé, I.; Schartz, N.; Battistella, M.; Verola, O.; Morel, P.; Bourrat, E. Disseminated perinaevic Meyerson phenomenon revealing melanoma. Ann. Dermatol. Venereol. 2012, 139, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Kim, Y.C. Eczema within a Capillary Malformation: A Case of Meyerson Phenomenon. Ann. Dermatol. 2016, 28, 781–782. [Google Scholar] [CrossRef] [PubMed]
- Pavlović, M.D.; Adamič, M. Eczema within port wine stain: Spontaneous and laser-induced Meyerson phenomenon. Acta Dermatovenerol. Alp. Pannonica Adriat. 2014, 23, 81–83. [Google Scholar] [CrossRef] [PubMed]
- Simon, V.; Hartschuh, W.; Flux, K. Meyerson-Phenomenon hides a nevus flammeus. JDDG J. Dtsch. Dermatol. Ges. 2011, 9, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Hofer, T. Meyerson phenomenon within a nevus flammeus. Dermatology 2002, 205, 180–183. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient | Gender | Age | Fungal Cultures | Location of Capillary Malformations | Evolution (Treated with Topical Hydrocortisone) |
|---|---|---|---|---|---|
| 1 | Male | 6 months | Negative | Nape of the neck | Good response |
| 2 | Female | 7 months | Nape of the neck | Good response | |
| 3 | Male | 11 months | Gluteal skin | Recurrent eczema | |
| 4 | Female | 4 months | Nape of the neck | Good response | |
| 5 | Male | 2 years | Right hemifacial skin | Good response (appeared after laser treatment) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanchez-Diaz, M.; Montero-Vilchez, T.; Salvador-Rodriguez, L.; Molina-Leyva, A.; Arias-Santiago, S.; Tercedor-Sanchez, J. Itchy Capillary Malformations: Unusual Appearance of Meyerson Phenomenon, a Case Series. Pediatr. Rep. 2021, 13, 131-134. https://doi.org/10.3390/pediatric13010019
Sanchez-Diaz M, Montero-Vilchez T, Salvador-Rodriguez L, Molina-Leyva A, Arias-Santiago S, Tercedor-Sanchez J. Itchy Capillary Malformations: Unusual Appearance of Meyerson Phenomenon, a Case Series. Pediatric Reports. 2021; 13(1):131-134. https://doi.org/10.3390/pediatric13010019
Chicago/Turabian StyleSanchez-Diaz, Manuel, Trinidad Montero-Vilchez, Luis Salvador-Rodriguez, Alejandro Molina-Leyva, Salvador Arias-Santiago, and Jesús Tercedor-Sanchez. 2021. "Itchy Capillary Malformations: Unusual Appearance of Meyerson Phenomenon, a Case Series" Pediatric Reports 13, no. 1: 131-134. https://doi.org/10.3390/pediatric13010019
APA StyleSanchez-Diaz, M., Montero-Vilchez, T., Salvador-Rodriguez, L., Molina-Leyva, A., Arias-Santiago, S., & Tercedor-Sanchez, J. (2021). Itchy Capillary Malformations: Unusual Appearance of Meyerson Phenomenon, a Case Series. Pediatric Reports, 13(1), 131-134. https://doi.org/10.3390/pediatric13010019