
Clinical, Immunological and Inflammatory Characteristics among Mexican Children with Different Subtypes of Juvenile Idiopathic Arthritis: Exploring the Correlation between Anti-Cyclic Citrullinated Peptide (anti-CCP) and Rheumatoid Factor (RF)



Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Clinical Evaluations
2.3. Immunological Evaluations
2.3.1. Rheumatoid Factor (RF)
2.3.2. Antinuclear Antibodies (ANAs)
2.3.3. Anti-Cyclic Citrullinated Peptide Antibodies (Anti-CCPs)
2.3.4. Inflammatory Markers: C-Reactive Protein (CRP) and Erythrocyte Sedimentation Rate (ESR)
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclosure
References
- Cassidy, J.T.; Petty, R.E. Chronic arthritis in children. In Textbook of Pediatric Rheumatology; Elseiver Saunders: Philadelphia, PA, USA, 2011; ISBN 9781416065814. [Google Scholar]
- Minden, K.; Niewerth, M. Klinische formen der juvenilen idiopathischen arthritis und ihre klassifikation. Z. Rheumatol. 2008, 67, 100–110. [Google Scholar] [CrossRef]
- Consolaro, A.; Ruperto, N.; Bazso, A.; Pistorio, A.; Magni-Manzoni, S.; Filocamo, G.; Malattia, C.; Viola, S.; Martini, A.; Ravelli, A. Development and validation of a composite disease activity score for juvenile idiopathic arthritis. Arthritis Care Res. 2009, 61, 658–666. [Google Scholar] [CrossRef]
- Houssien, D.A.; Jónsson, T.; Davies, E.; Scott, D.L. Rheumatoid factor isotypes, disease activity and the outcome of rheumatoid arthritis: Comparative effects of different antigens. Scand. J. Rheumatol. 1998, 27, 46–53. [Google Scholar] [CrossRef]
- Ateş, A.; Kinikli, G.; Turgay, M.; Akay, G.; Tokgöz, G. Effects of rheumatoid factor isotypes on disease activity and severity in patients with rheumatoid arthritis: A comparative study. Clin. Rheumatol. 2007, 26, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.M.; Mccurdy, D.K.; Shaham, B.; Brik, R.; Wietting, H.; Arora, Y.; Lehman, T.J.A.; Hanson, V.; Bernstein, B. High prevalence of iga rheumatoid factor in severe polyarticular-onset juvenile rheumatoid arthritis, but not in systemic-onset or pauciarticular-onset disease. Arthritis Rheum. 1990, 33, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, R.A.; Silva, C.H.M.; Silva, D.A.O.; Sopelete, M.C.; Kiss, M.H.B.; Mineo, J.R.; Ferriani, V.P.L. Is measurement of IgM and IgA rheumatoid factors (RF) in juvenile rheumatoid arthritis clinically useful? Rheumatol. Int. 2007, 27, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Rabinovich, C.E. Treatment of juvenile idiopathic arthritis-associated uveitis: Challenges and update. Curr. Opin. Rheumatol. 2011, 23, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Ravelli, A.; Varnier, G.C.; Oliveira, S.; Castell, E.; Arguedas, O.; Magnani, A.; Pistorio, A.; Ruperto, N.; Magni-Manzoni, S.; Galasso, R.; et al. Antinuclear antibody-positive patients should be grouped as a separate category in the classification of juvenile idiopathic arthritis. Arthritis Rheum. 2011, 63, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Hügle, B.; Hinze, C.; Lainka, E.; Fischer, N.; Haas, J.P. Development of positive antinuclear antibodies and rheumatoid factor in systemic juvenile idiopathic arthritis points toward an autoimmune phenotype later in the disease course. Pediatr. Rheumatol. 2014, 12, 28. [Google Scholar] [CrossRef] [PubMed]
- Syed, R.H.; Gilliam, B.E.; Moore, T.L. Prevalence and significance of isotypes of anti-cyclic citrullinated peptide antibodies in juvenile idiopathic arthritis. Ann. Rheum. Dis. 2008, 67, 1049–1051. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Smidt, N.; Sterne, J.A.C.; Harbord, R.; Burton, A.; Burke, M.; Beynon, R.; Ben-Shlomo, Y.; Axford, J.; Dieppe, P. Systematic review: Accuracy of anti-citrullinated peptide antibodies for diagnosing rheumatoid arthritis. Ann. Intern. Med. 2010, 152, 456–464. [Google Scholar] [CrossRef]
- Avčin, T.; Meroni, P.L.; Cimaz, R.; Falcini, F.; Zulian, F.; Martini, G.; Simonini, G.; Porenta-Bešic, V.; Cecchini, G.; Borghi, M.O. Prevalence and clinical significance of anti-cyclic citrullinated peptide antibodies in juvenile idiopathic arthritis. Ann. Rheum. Dis. 2002, 61, 608–611. [Google Scholar] [CrossRef] [PubMed]
- Hamooda, M.; Fouad, H.; Galal, N.; Sewelam, N.; Megahed, D. Anti-cyclic citrullinated peptide antibodies in children with Juvenile Idiopathic Arthritis. Electron. Physician 2016, 8, 2897. [Google Scholar] [CrossRef] [PubMed]
- Pelajo, C.F.; Angeles-Han, S.T.; Prahalad, S.; Sgarlat, C.M.; Davis, T.E.; Miller, L.C.; Lopez-Benitez, J.M. Evaluation of the association between Hispanic ethnicity and disease activity and severity in a large cohort of patients with juvenile idiopathic arthritis. Rheumatol. Int. 2013, 33, 2549–2554. [Google Scholar] [CrossRef] [PubMed]
- Koniushevska, A.A.; Vaiser, N.V.; Kuzevanova, M.V.; Gerasymenko, V.V.; Tymoshyna, O.V.; Polesova, T.R. Systemic juvenile idiopathic arthritis in the pediatric practice of Donetsk region. Regul. Mech. Biosyst. 2023, 14, 248–259. [Google Scholar] [CrossRef]
- Kwok, J.S.Y.; Hui, K.H.; Lee, T.L.; Wong, W.; Lau, Y.L.; Wong, R.W.S.; Kim, D.L.; Jones, B.M. Anti-cyclic citrullinated peptide: Diagnostic and prognostic values in juvenile idiopathic arthritis and rheumatoid arthritis in a Chinese population. Scand. J. Rheumatol. 2005, 34, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Pang, S.Y.; Liu, H.Y.; Huang, Y.J.; Liu, Y.F.; Dai, Y.M.; Zeng, P. Diagnostic performance of anti-citrullinated protein/peptide antibodies in juvenile idiopathic arthritis. Genet. Mol. Res. 2016, 15. [Google Scholar] [CrossRef]
- Di Matteo, A.; Mankia, K.; Duquenne, L.; Mahler, M.; Corscadden, D.; Mbara, K.; Garcia-Montoya, L.; Nam, J.L.; Emery, P. Third-Generation Anti–Cyclic Citrullinated Peptide Antibodies Improve Prediction of Clinical Arthritis in Individuals at Risk of Rheumatoid Arthritis. Arthritis Rheumatol. 2020, 72, 1820–1828. [Google Scholar] [CrossRef]
- Ruperto, N.; Lovell, D.J.; Berman, A.; Ávila-Zapata, F.; Horneff, G.; Alessio, M.; Becker, M.L.; Belot, A.; Burgos-Vargas, R.; Gamir, M.L.; et al. Patient-Reported Outcomes among Patients Ages Two to Seventeen Years with Polyarticular-Course Juvenile Idiopathic Arthritis Treated With Subcutaneous Abatacept: Two-Year Results from an International Phase III Study. Arthritis Care Res. 2023, 75, 1804–1814. [Google Scholar] [CrossRef]
- Adib, N.; Hyrich, K.; Thornton, J.; Lunt, M.; Davidson, J.; Gardner-medwin, J.; Foster, H.; Baildam, E.; Wedderburn, L.; Thomson, W. Association between duration of symptoms and severity of disease at first presentation to paediatric rheumatology: Results from the Childhood Arthritis Prospective Study. Rheumatology 2008, 47, 991–995. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Omar, A.; Abo-Elyoun, I.; Hussein, H.; Nabih, M.; Atwa, H.; Gad, S.; Emad, Y. Anti-cyclic citrullinated peptide (anti-CCP) antibody in juvenile idiopathic arthritis (JIA): Correlations with disease activity and severity of joint damage (a multicenter trial). Jt. Bone Spine 2013, 80, 38–43. [Google Scholar] [CrossRef]
- Yasui, K.; Sakata, S.; Ochi, H.; Itamura, S.; Hirai, K.; Takenaka, M.; Mitani, O.; Ogawa, K.; Iyoda, K. Onset of polyarticular juvenile idiopathic arthritis with both anti-cyclic citrullinated peptide antibodies and rheumatoid factor in a 3-year-old girl. Pediatr. Rheumatol. 2012, 10, 41. [Google Scholar] [CrossRef]
- Rodríguez, E.U.; Sánchez, P.S. Artritis idiopática juvenil. PediatríaIntegral 2017, 21, 170–182. [Google Scholar]
- Modesto, C.; Antón, J.; Rodriguez, B.; Bou, R.; Arnal, C.; Ros, J.; Tena, X.; Rodrigo, C.; Rotés, I.; Hermosilla, E.; et al. Incidence and prevalence of juvenile idiopathic arthritis in Catalonia (Spain). Scand. J. Rheumatol. 2010, 39, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Kunjir, V.; Venugopalan, A.; Chopra, A. Profile of Indian patients with juvenile onset chronic inflammatory joint disease using the ILAR classification criteria for JIA: A community-based cohort study. J. Rheumatol. 2010, 37, 1756–1762. [Google Scholar] [CrossRef] [PubMed]
- Weakley, K.; Esser, M.; Scott, C. Juvenile idiopathic arthritis in two tertiary centres in the Western Cape, South Africa. Pediatr. Rheumatol. 2012, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Tebo, A.E.; Jaskowski, T.; Davis, K.W.; Whiting, A.; Clifford, B.; Zeft, A.; McNally, B.; Hill, H.R.; Bohnsack, J.; Prahalad, S. Profiling anti-cyclic citrullinated peptide antibodies in patients with juvenile idiopathic arthritis. Pediatr. Rheumatol. 2012, 10, 29. [Google Scholar] [CrossRef] [PubMed]
- Habib, H.M.; Mosaad, Y.M.; Youssef, H.M. Anti-cyclic citrullinated peptide antibodies in patients with juvenile idiopathic arthritis. Immunol. Investig. 2008, 37, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Dewint, P.; Hoffman, I.E.A.; Rogge, S.; Joos, R.; Union, A.; Dehoorne, J.; Delanghe, J.; Veys, E.M.; De Keyser, F.; Elewaut, D. Effect of age on prevalence of anticitrullinated protein/peptide antibodies in polyarticular juvenile idiopathic arthritis. Rheumatology 2006, 45, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Thabah, M.M.; Vaidya, B.; Gupta, S.; Lodha, R.; Kabra, S.K. Anti-cyclic citrullinated peptide antibodies in juvenile idiopathic arthritis. Indian J. Pediatr. 2010, 77, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Syed, R.H.; Gilliam, B.E.; Moore, T.L. Rheumatoid factors and anticyclic citrullinated peptide antibodies in pediatric rheumatology. Curr. Rheumatol. Rep. 2008, 10, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Ferucci, E.D.; Majka, D.S.; Parrish, L.A.; Moroldo, M.B.; Ryan, M.; Passo, M.; Thompson, S.D.; Deane, K.D.; Rewers, M.; Arend, W.P.; et al. Antibodies against Cyclic Citrullinated Peptide Are Associated with HLA—DR4 in Simplex and Multiplex Polyarticular-Onset Juvenile Rheumatoid Arthritis. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 2005, 52, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Skare, T.S.; Nisihara, R.M.; Silva, R.M.; Munhoz Da Silva, D.J.; Gameiro Silva, M.B.; Utiyama, S.R.R. Anti-cyclic citrullinated peptide antibodies in adult patients with juvenile idiopathic arthritis. J. Clin. Rheumatol. 2011, 17, 421–423. [Google Scholar] [CrossRef] [PubMed]
- Kasapçopur, Ö.; Altun, S.; Aslan, M.; Karaarslan, S.; Kamburoglu-Göksel, A.; Saribaş, S.; Arisoy, N.; Kocazeybek, B. Diagnostic accuracy of anti-cyclic citrullinated peptide antibodies in juvenile idiopathic arthritis. Ann. Rheum. Dis. 2004, 63, 1687–1689. [Google Scholar] [CrossRef]
- Ravelli, A.; Martini, A. Juvenile idiopathic arthritis. Lancet 2007, 369, 767–778. [Google Scholar] [CrossRef]
- De Benedetti, F.; Anton, J.; Gattorno, M.; Lachmann, H.; Kone-Paut, I.; Ozen, S.; Frenkel, J.; Simon, A.; Zeft, A.; Ben-Chetrit, E.; et al. Proceedings of the 23rd Paediatric Rheumatology European Society Congress: Part one. Pediatr. Rheumatol. 2017, 15 (Suppl. S1), 37. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 50) | Systemic Arthritis (n = 8) | Enthesitis-Related Arthritis (n = 4) | Oligoarthritis (n = 7) | Seronegative Polyarthritis (n = 14) | Seropositive Polyarthritis (n = 17) | Intergroup Comparison | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Sex | p = 0.014 a,c | |||||||||
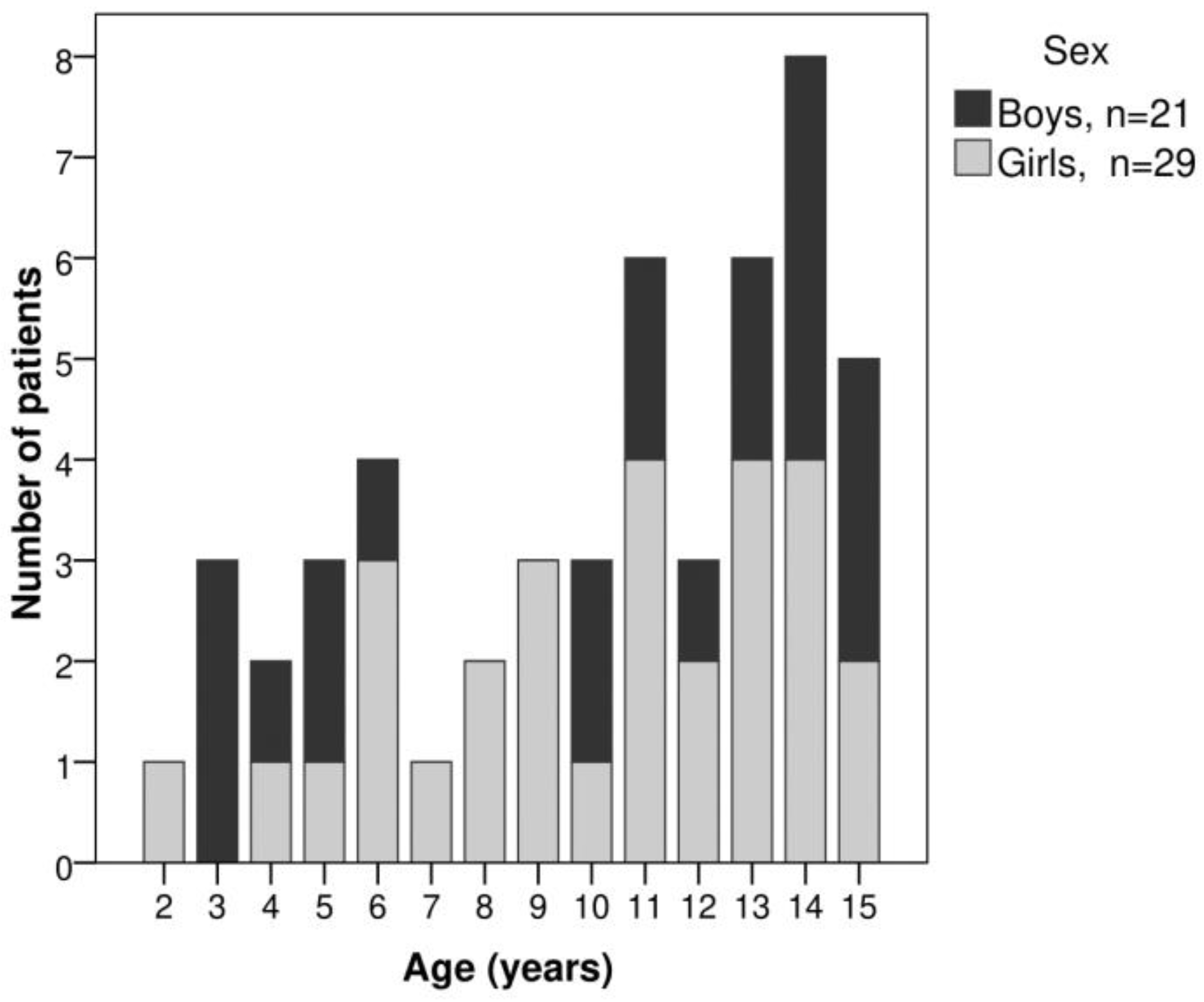
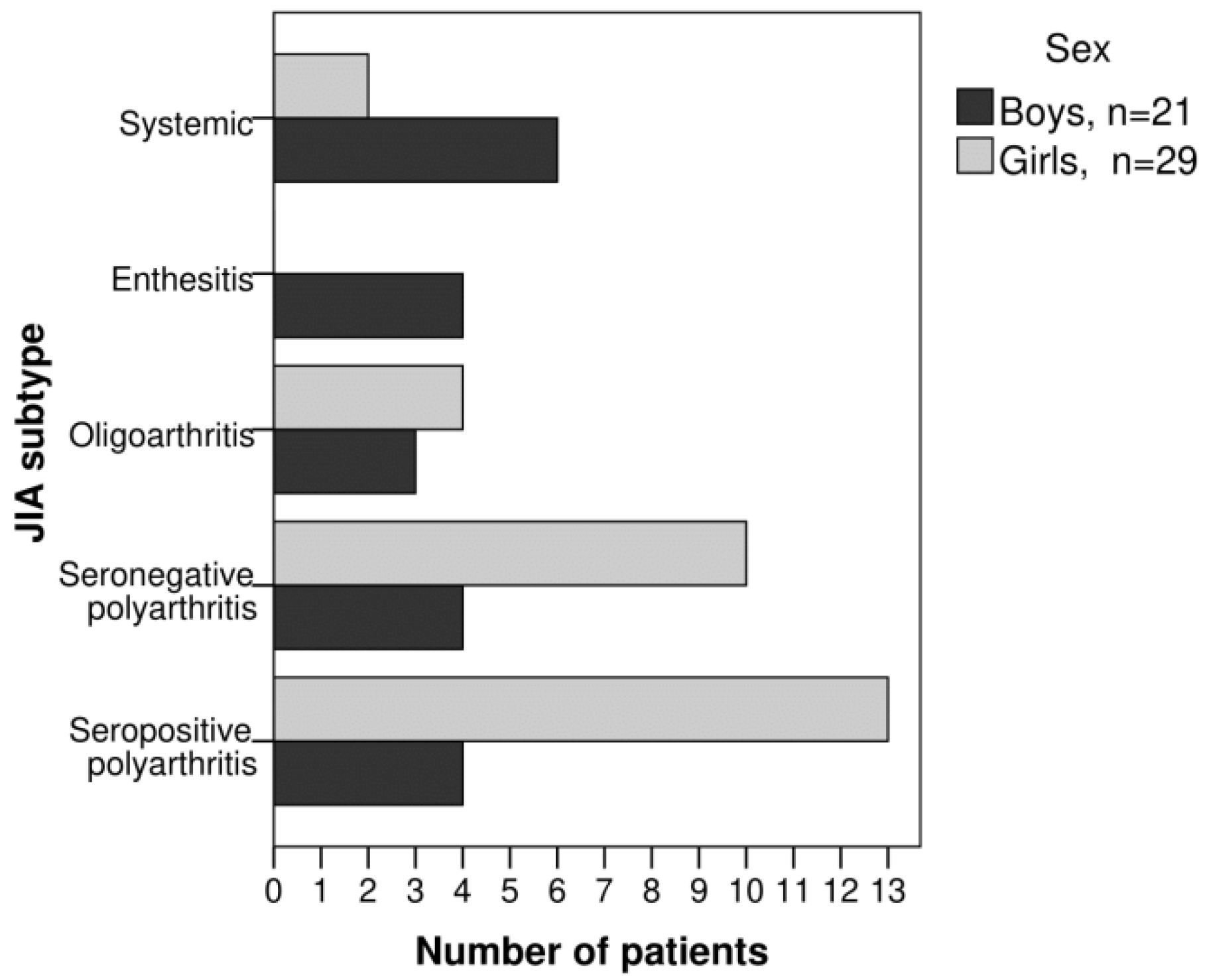
| girls, n (%) | 29 (58%) | 2 (25%) | 0 (0%) | 4 (57%) | 10 (71%) | 13 (76%) | ||||
| boys, n (%) | 21 (42%) | 6 (75%) | 4 (100%) | 3 (43%) | 4 (29%) | 4 (24%) | ||||
| age (years) | 10.56 (3.99) | 8.76 (4.86) | 13.70 (1.91) | 7.66 (3.49) | 9.31 (4.21) | 12.9 (1.98) | p = 0.007 b,c | |||
| active joints | 11.36 (6.72) | 8.25 (3.62) | 6.50 (1.29) | 2.43 (0.98) | 15.00 (7.64) | 14.65 (3.95) | p < 0.001 b,c | |||
| Radiological assessments | ||||||||||
| joint swelling, n (%) | 37 (74%) | 7 (88%) | 4 (100%) | 7 (100%) | 6 (43%) | 13 (76%) | p = 0.019 a,c | |||
| osteopenia, n (%) | 35 (70%) | 4 (50%) | 1 (25%) | 3 (43%) | 13 (93%) | 14 (82%) | p = 0.014 a,c | |||
| joint space narrowing, n (%) | 16 (32%) | 0 (0%) | 0 (0%) | 0 (0%) | 6 (43%) | 10 (59%) | p = 0.004 a,c | |||
| joint erosions, n (%) | 4 (8%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 (14%) | 2 (12%) | p = 0.604 a | |||
| CRP (mg/dL) | 28.6 (43.49) | n = 47 | 70.28 (76.16) | 10.15 (14.31) | 11.19 (8.78) | 16.56 (16.86) | n = 12 | 29.04 (39.21) | n = 16 | p = 0.348 b |
| ESR (mm/hr) | 25.94 (18.64) | n = 47 | 28.50 (20.00) | 8.75 (5.12) | 27.71 (13.31) | 27.75 (17.43) | n = 12 | 26.81 (22.19) | n = 16 | p = 0.225 b |
| RF (IU/mL) | 72.52 (194.00) | 8.28 (0.92) | 8.60 (0.00) | 8.47 (1.09) | 8.6 (0.00) | 196.82 (300.65) | p < 0.001 b,c | |||
| <12 (negative), n (%) | 33 (66%) | 8 (100%) | 4 (100%) | 7 (100%) | 14 (100%) | 0 (0%) | p < 0.001 a,c | |||
| ≥12 (positive), n (%) | 17 (33%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 17 (100%) | p < 0.001 a,c | |||
| log RF, (log [IU/mL]) | 1.29 (0.58) | 0.91 (0.06) | 0.93 (0.00) | 0.92 (0.06) | 0.93 (0.00) | 2.01 (0.48) | p < 0.001 b,c | |||
| anti-CCPs (IU/mL) | 27.97 (56.12) | 9.41 (9.44) | 11.95 (20.45) | 6.29 (7.36) | 9.11 (14.17) | 64.94 (84.49) | p < 0.001 b,c | |||
| <20 (negative) n (%) | 29 (58%) | 6 (75%) | 3 (75%) | 6 (86%) | 11 (79%) | 3 (18%) | p < 0.001 a,c | |||
| ≥20 (positive) n (%) | 21 (42%) | 2 (25%) | 1 (25%) | 1 (14%) | 3 (21%) | 14 (82%) | p < 0.001 a,c | |||
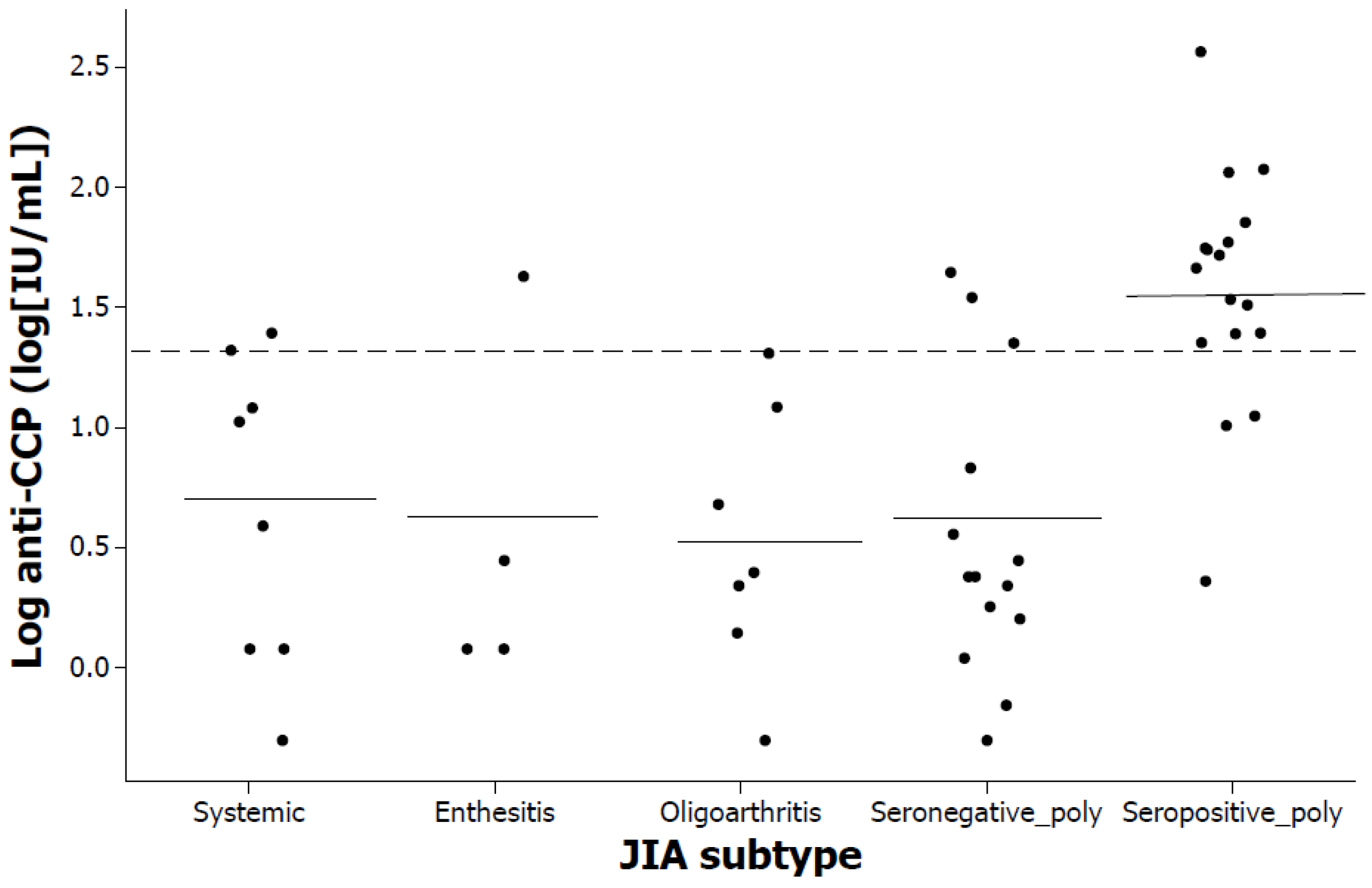
| log anti-CCPs, (log [IU/mL]) | 0.91 (0.73) | 0.66 (0.64) | 0.56 (0.73) | 0.52 (0.55) | 0.54 (0.60) | 1.58 (0.49) | p < 0.001 b,c | |||
| Correlations | CRP | ESR | RF | Anti-CCPs | ||||
|---|---|---|---|---|---|---|---|---|
| r | significance | r | significance | r | significance | r | significance | |
| Age | ||||||||
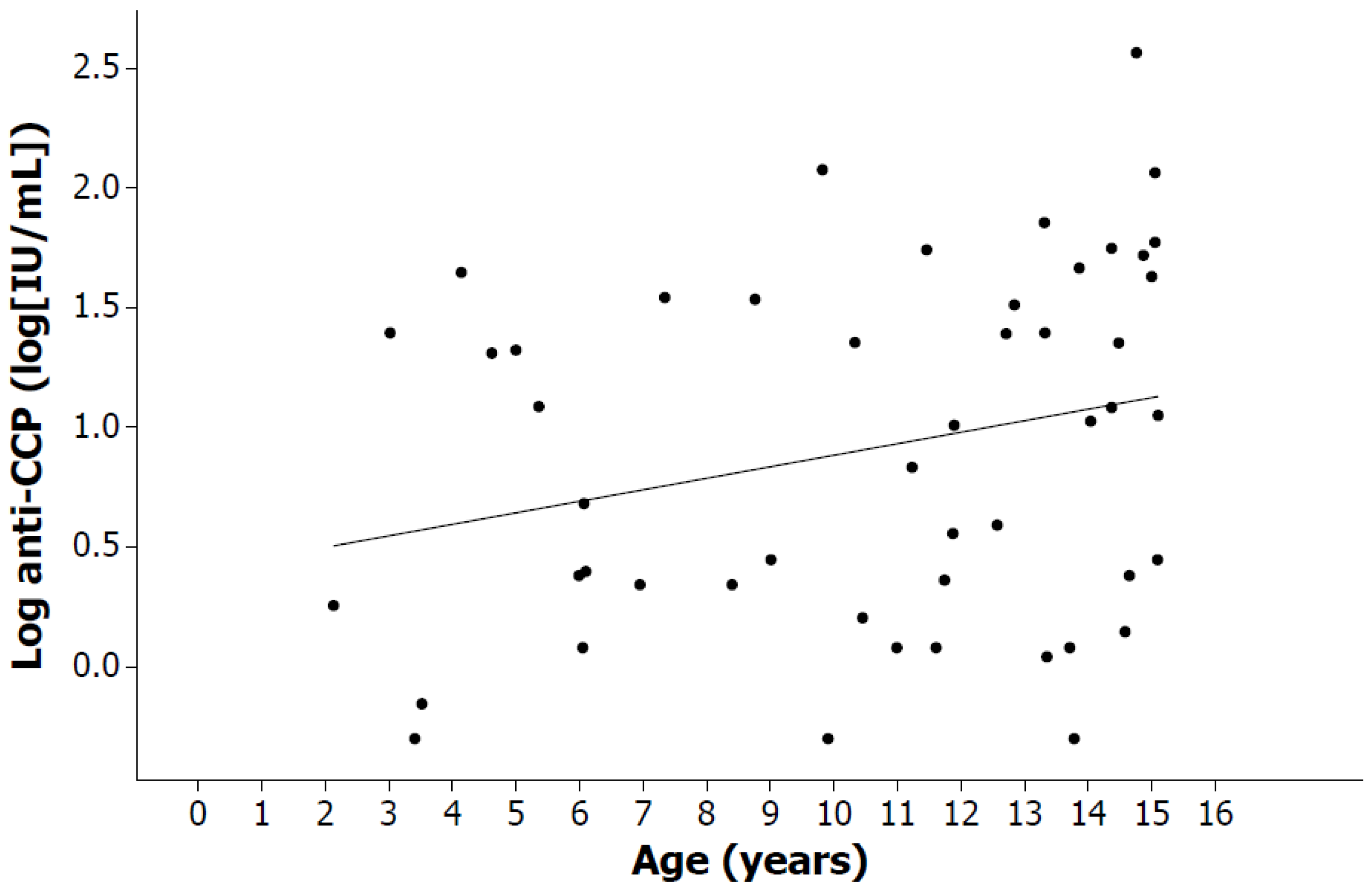
| All | 0.05 | p = 0.731 | −0.14 | p = 0.339 | 0.40 | p = 0.004 a | 0.29 | p = 0.041 a |
| Girls | −0.10 | p = 0.612 | −0.27 | p = 0.159 | 0.51 | p = 0.005 a | 0.32 | p = 0.086 |
| Boys | 0.26 | p = 0.287 | −0.08 | p = 0.745 | 0.35 | p = 0.124 | 0.30 | p = 0.180 |
| CRP | ||||||||
| All | 0.38 | p = 0.008 a | 0.05 | p = 0.734 | −0.04 | p = 0.767 | ||
| Girls | 0.36 | p = 0.058 | 0.12 | p = 0.552 | 0.04 | p = 0.832 | ||
| Boys | 0.50 | p = 0.029 a | −0.02 | p = 0.932 | −0.22 | p = 0.373 | ||
| ESR | ||||||||
| All | <0.01 | p = 0.997 | 0.11 | p = 0.482 | ||||
| Girls | 0.03 | p = 0.866 | 0.04 | p = 0.853 | ||||
| Boys | −0.17 | p = 0.494 | 0.13 | p = 0.603 | ||||
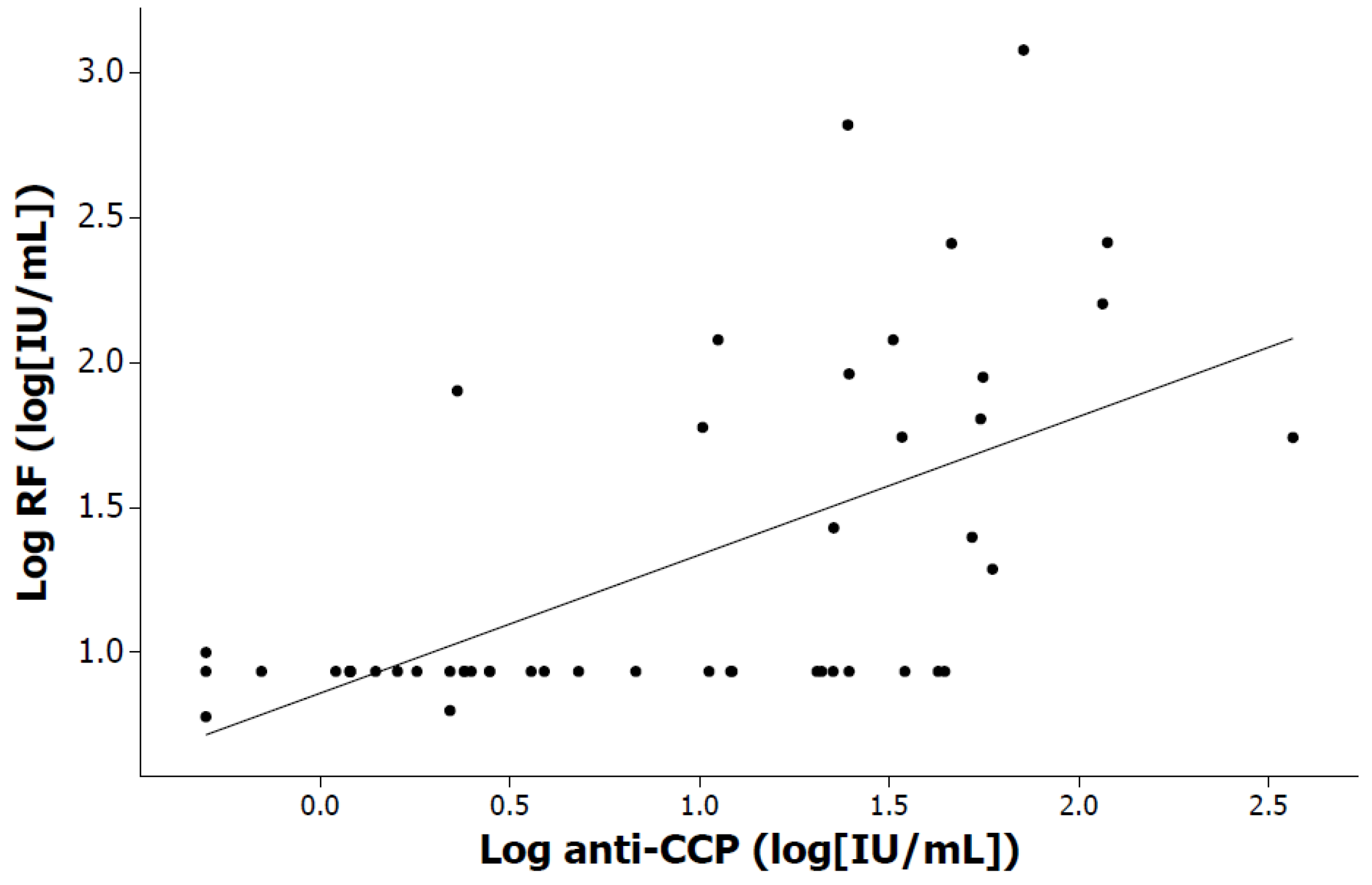
| RF | ||||||||
| All | 0.63 | p < 0.001 a | ||||||
| Girls | 0.60 | p < 0.001 a | ||||||
| Boys | 0.58 | p = 0.006 a | ||||||
| Variables | RF and Anti-CCPs Negative n = 26 | Either RF or Anti-CCPs Positive n= 10 | RF and Anti-CCPs Positive n = 14 | Intergroup Comparison |
|---|---|---|---|---|
| Sex | ||||
| girls, n (%) | 14 (54%) | 4 (40%) | 11 (79%) | p = 0.139 a |
| boys, n (%) | 12 (46%) | 6 (60%) | 3 (21%) | p = 0.139 a |
| age (years) | 9.82 (4.01) | 9.23 (4.90) | 12.89 (2.06) | p = 0.067 b |
| active joints | 9.69 (7.58) | 10.70 (5.70) | 14.93 (4.16) | p = 0.007 b,c |
| Radiological assessments | ||||
| joint swelling, n (%) | 20 (77%) | 7 (70%) | 10 (71%) | p = 0.884 a |
| osteopenia, n (%) | 15 (60%) | 9 (90%) | 11 (79%) | p = 0.118 a |
| joint space narrowing, n (%) | 4 (15%) | 3 (30%) | 9 (64%) | p = 0.007 a,c |
| joint erosions, n (%) | 1 (3.8%) | 1 (10%) | 2 (14.3%) | p = 0.493 a |
| Percentage | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Source | Country | n | Girls/Boys | Systemic Arthritis | Enthesitis-Related Arthritis | Oligoarthritis | Psoriatic | Undifferentiated Arthritis | Seronegative Polyarthritis | Seropositive Polyarthritis |
| Adib et al. 2008 [21] | UK | 427 | 65%/35% | 6.3% | 7.5% | 54.6% | 8.2% | 4.7% | 15.9% | 2.8% |
| Modesto et al. 2010 [26] | Spain | 145 | 64%/36% | 6.9% | 12.4% | 51.0% | 6.2% | 11.1% | 10.3% | 2.1% |
| Kunjir et al. 2010 [27] | India | 235 | 42%/58% | 8.0% | 36.0% | 21.0% | 1.0% | 5.0% | 17.0% | 12.0% |
| Weakley et al. 2012 [28] | South Africa | 78 | 50%/50% | 7.7% | 23.0% | 27.0% | 1.3% | 0.0% | 26.9% | 14.1% |
| Tebo et al. 2012 [29] | US | 334 | 66%/34% | 9.3% | 8.1% | 43.4% | 0.0% | 7.5% | 22.7% | 9.0% |
| Hernández-Huirache et al., 2024 | Mexico | 50 | 58%/42% | 16.0% | 8.0% | 14.0% | 0.0% | 0.0% | 28.0% | 34.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Huirache, H.G.; Armenta-Medina, D.; Rodea-Montero, E.R. Clinical, Immunological and Inflammatory Characteristics among Mexican Children with Different Subtypes of Juvenile Idiopathic Arthritis: Exploring the Correlation between Anti-Cyclic Citrullinated Peptide (anti-CCP) and Rheumatoid Factor (RF). Pediatr. Rep. 2024, 16, 151-162. https://doi.org/10.3390/pediatric16010014
Hernández-Huirache HG, Armenta-Medina D, Rodea-Montero ER. Clinical, Immunological and Inflammatory Characteristics among Mexican Children with Different Subtypes of Juvenile Idiopathic Arthritis: Exploring the Correlation between Anti-Cyclic Citrullinated Peptide (anti-CCP) and Rheumatoid Factor (RF). Pediatric Reports. 2024; 16(1):151-162. https://doi.org/10.3390/pediatric16010014
Chicago/Turabian StyleHernández-Huirache, Hayde Guadalupe, Dagoberto Armenta-Medina, and Edel Rafael Rodea-Montero. 2024. "Clinical, Immunological and Inflammatory Characteristics among Mexican Children with Different Subtypes of Juvenile Idiopathic Arthritis: Exploring the Correlation between Anti-Cyclic Citrullinated Peptide (anti-CCP) and Rheumatoid Factor (RF)" Pediatric Reports 16, no. 1: 151-162. https://doi.org/10.3390/pediatric16010014
APA StyleHernández-Huirache, H. G., Armenta-Medina, D., & Rodea-Montero, E. R. (2024). Clinical, Immunological and Inflammatory Characteristics among Mexican Children with Different Subtypes of Juvenile Idiopathic Arthritis: Exploring the Correlation between Anti-Cyclic Citrullinated Peptide (anti-CCP) and Rheumatoid Factor (RF). Pediatric Reports, 16(1), 151-162. https://doi.org/10.3390/pediatric16010014