
Post-Transplant Cyclophosphamide versus Anti-Thymocyte Globulin in Patients with Hematological Malignancies Treated with Allogeneic Hematopoietic Stem Cell Transplantation from Haploidentical and Matched Unrelated Donors: A Real-Life Experience

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giebel, S.; Labopin, M.; Salmenniemi, U.; Socié, G.; Bondarenko, S.; Blaise, D.; Kröger, N.; Vydra, J.; Grassi, A.; Bonifazi, F.; et al. Posttransplant cyclophosphamide versus antithymocyte globulin in patients with acute lymphoblastic leukemia treated with allogeneic hematopoietic cell transplantation from matched unrelated donors. A study from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Cancer 2023, 129, 3735–3745. [Google Scholar] [CrossRef] [PubMed]
- Luznik, L.; O’Donnell, P.V.; Symons, H.J.; Chen, A.R.; Leffell, M.S.; Zahurak, M.; Gooley, T.A.; Piantadosi, S.; Kaup, M.; Ambinder, R.F.; et al. HLA-haploidentical bone marrow transplantation for hematologic malignancies using nonmyeloablative conditioning and high-dose, posttransplantation cyclophosphamide. Biol. Blood Marrow Transplant. 2008, 14, 641–650. [Google Scholar] [CrossRef]
- Besse, K.; Maiers, M.; Confer, D.; Albrecht, M. On Modeling Human Leukocyte Antigen-Identical Sibling Match Probability for Allogeneic Hematopoietic Cell Transplantation: Estimating the Need for an Unrelated Donor Source. Biol. Blood Marrow Transplant. 2016, 22, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Carreras, E.; Dufour, C.; Mohty, M.; Kröger, N. (Eds.) The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies [Internet], 7th ed.; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Bacigalupo, A.; Lamparelli, T.; Barisione, G.; Bruzzi, P.; Guidi, S.; Alessandrino, P.E.; di Bartolomeo, P.; Oneto, R.; Bruno, B.; Sacchi, N.; et al. Thymoglobulin prevents chronic graft-versus-host disease, chronic lung dysfunction, and late transplant-related mortality: Long-term follow-up of a randomized trial in patients undergoing unrelated donor transplantation. Biol. Blood Marrow Transplant. 2006, 12, 560–565. [Google Scholar] [CrossRef]
- Chang, Y.J.; Wu, D.P.; Lai, Y.R.; Liu, Q.F.; Sun, Y.Q.; Hu, J.; Hu, Y.; Zhou, J.F.; Li, J.; Wang, S.Q.; et al. Antithymocyte Globulin for Matched Sibling Donor Transplantation in Patients With Hematologic Malignancies: A Multicenter, Open-Label, Randomized Controlled Study. J. Clin. Oncol. 2020, 38, 3367–3376. [Google Scholar] [CrossRef] [PubMed]
- Kharfan-Dabaja, M.A.; Parody, R.; Perkins, J.; Lopez-Godino, O.; Lopez-Corral, L.; Vazquez, L.; Caballero, D.; Falantes, J.; Shapiro, J.; Ortí, G.; et al. Tacrolimus plus sirolimus with or without ATG as GVHD prophylaxis in HLA-mismatched unrelated donor allogeneic stem cell transplantation. Bone Marrow Transplant. 2017, 52, 438–444. [Google Scholar] [CrossRef]
- Ali, M.M.; Grønvold, B.; Remberger, M.; Abrahamsen, I.W.; Myhre, A.E.; Tjønnfjord, G.E.; Fløisand, Y.; Gedde-Dahl, T. Addition of Anti-thymocyte Globulin in Allogeneic Stem Cell Transplantation With Peripheral Stem Cells From Matched Unrelated Donors Improves Graft-Versus-Host Disease and Relapse Free Survival. Clin. Lymphoma Myeloma Leuk. 2021, 21, 598–605. [Google Scholar] [CrossRef]
- Bacigalupo, A.; Lamparelli, T.; Bruzzi, P.; Guidi, S.; Alessandrino, P.E.; di Bartolomeo, P.; Oneto, R.; Bruno, B.; Barbanti, M.; Sacchi, N.; et al. Antithymocyte globulin for graft-versus-host disease prophylaxis in transplants from unrelated donors: 2 randomized studies from Gruppo Italiano Trapianti Midollo Osseo (GITMO). Blood 2001, 98, 2942–2947. [Google Scholar] [CrossRef]
- Luznik, L.; Jalla, S.; Engstrom, L.W.; Iannone, R.; Fuchs, E.J. Durable engraftment of major histocompatibility complex-incompatible cells after nonmyeloablative conditioning with fludarabine, low-dose total body irradiation, and posttransplantation cyclophosphamide. Blood 2001, 98, 3456–3464. [Google Scholar] [CrossRef]
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar]
- Shulman, H.M.; Sullivan, K.M.; Weiden, P.L.; McDonald, G.B.; Striker, G.E.; Sale, G.E.; Hackman, R.; Tsoi, M.S.; Storb, R.; Thomas, E.D. Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am. J. Med. 1980, 69, 204–217. [Google Scholar] [CrossRef] [PubMed]
- Hutt, D. Engraftment, Graft Failure, and Rejection. In The European Blood and Marrow Transplantation Textbook for Nurses: Under the Auspices of EBMT [Internet]; Kenyon, M., Babic, A., Eds.; Springer: Cham, Switzerland, 2018; Chapter 13. [Google Scholar] [PubMed]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the intensity of conditioning regimens: Working definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.R.; Sizemore, C.A.; Sanacore, M.; Zhang, X.; Brown, S.; Holland, H.K.; Morris, L.E.; Bashey, A. Haploidentical transplantation using T cell replete peripheral blood stem cells and myeloablative conditioning in patients with high-risk hematologic malignancies who lack conventional donors is well tolerated and produces excellent relapse-free survival: Results of a prospective phase II trial. Biol. Blood Marrow Transplant. 2012, 18, 1859–1866. [Google Scholar] [PubMed]
- Bhamidipati, P.K.; DiPersio, J.F.; Stokerl-Goldstein, K.; Rashidi, A.; Gao, F.; Uy, G.L.; Westervelt, P.; Vij, R.; Schroeder, M.A.; Abboud, C.N.; et al. Haploidentical transplantation using G-CSF-mobilized T-cell replete PBSCs and post-transplantation CY after non-myeloablative conditioning is safe and is associated with favorable outcomes. Bone Marrow Transplant. 2014, 49, 1124–1126. [Google Scholar] [CrossRef] [PubMed]
- Mielcarek, M.; Furlong, T.; O’Donnell, P.V.; Storer, B.E.; McCune, J.S.; Storb, R.; Carpenter, P.A.; Flowers, M.E.; Appelbaum, F.R.; Martin, P.J. Posttransplantation cyclophosphamide for prevention of graft-versus-host disease after HLA-matched mobilized blood cell transplantation. Blood 2016, 127, 1502–1508. [Google Scholar] [CrossRef] [PubMed]
- Moiseev, I.S.; Pirogova, O.V.; Alyanski, A.L.; Babenko, E.V.; Gindina, T.L.; Darskaya, E.I.; Slesarchuk, O.A.; Bondarenko, S.N.; Afanasyev, B.V. Graft-versus-Host Disease Prophylaxis in Unrelated Peripheral Blood Stem Cell Transplantation with Post-Transplantation Cyclophosphamide, Tacrolimus, and Mycophenolate Mofetil. Biol. Blood Marrow Transplant. 2016, 22, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Greco, R.; Lorentino, F.; Albanese, S.; Lupo Stanghellini, M.T.; Giglio, F.; Piemontese, S.; Clerici, D.; Lazzari, L.; Marcatti, M.; Mastaglio, S.; et al. Posttransplantation Cyclophosphamide- and Sirolimus-Based Graft-versus-Host-Disease Prophylaxis in Allogeneic Stem Cell Transplant. Transplant. Cell. Ther. 2021, 27, 776.e1–776.e13. [Google Scholar] [CrossRef]
- Lee, M.W.; Yeon, S.H.; Seo, W.H.; Ryu, H.; Lee, H.J.; Yun, H.J.; Jo, D.Y.; Song, I.C. A comparison of post-transplantation cyclophosphamide versus antithymocyte-globulin in patients with hematological malignancies undergoing HLA-matched unrelated donor transplantation. Medicine 2020, 99, e21571. [Google Scholar] [CrossRef]
- Dybko, J.; Sobczyk-Kruszelnicka, M.; Makuch, S.; Agrawal, S.; Dudek, K.; Giebel, S.; Gil, L. The Benefits of the Post-Transplant Cyclophosphamide in Both Haploidentical and Mismatched Unrelated Donor Setting in Allogeneic Stem Cells Transplantation. Int. J. Mol. Sci. 2023, 24, 5764. [Google Scholar] [CrossRef]
- van Gorkom, G.; Billen, E.; Van Elssen, C.; van Gelder, M.; Bos, G. Real-world experience: Introduction of T cell replete haploidentical transplantations in a single center. EJHaem 2021, 2, 440–448. [Google Scholar] [CrossRef]
- Falkenburg, J.H.F.; Jedema, I. Graft versus tumor effects and why people relapse. Hematol. Am. Soc. Hematol. Educ. Program 2017, 2017, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Ahlmann, M.; Hempel, G. The effect of cyclophosphamide on the immune system: Implications for clinical cancer therapy. Cancer Chemother. Pharmacol. 2016, 78, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Maurer, K.; Ho, V.T.; Inyang, E.; Cutler, C.; Koreth, J.; Shapiro, R.M.; Gooptu, M.; Romee, R.; Nikiforow, S.; Antin, J.H.; et al. Posttransplant cyclophosphamide vs tacrolimus-based GVHD prophylaxis: Lower incidence of relapse and chronic GVHD. Blood Adv. 2023, 7, 3903–3915. [Google Scholar] [CrossRef] [PubMed]
- Ishio, T.; Sugita, J.; Tateno, T.; Hidaka, D.; Hayase, E.; Shiratori, S.; Okada, K.; Goto, H.; Onozawa, M.; Nakagawa, M.; et al. Hematogones Predict Better Outcome in Allogeneic Hematopoietic Stem Cell Transplantation Irrespective of Graft Sources. Biol. Blood Marrow Transplant. 2018, 24, 1990–1996. [Google Scholar] [CrossRef]
- Mehta, R.S.; Saliba, R.M.; Chen, J.; Rondon, G.; Hammerstrom, A.E.; Alousi, A.; Qazilbash, M.; Bashir, Q.; Ahmed, S.; Popat, U.; et al. Post-transplantation cyclophosphamide versus conventional graft-versus-host disease prophylaxis in mismatched unrelated donor haematopoietic cell transplantation. Br. J. Haematol. 2016, 173, 444–455. [Google Scholar] [CrossRef] [PubMed]
- Retière, C.; Willem, C.; Guillaume, T.; Vié, H.; Gautreau-Rolland, L.; Scotet, E.; Saulquin, X.; Gagne, K.; Béné, M.C.; Imbert, B.M.; et al. Impact on early outcomes and immune reconstitution of high-dose post-transplant cyclophosphamide vs anti-thymocyte globulin after reduced intensity conditioning peripheral blood stem cell allogeneic transplantation. Oncotarget 2018, 9, 11451–11464. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.J.; Vader, J.M.; Slade, M.; DiPersio, J.F.; Westervelt, P.; Romee, R. Cardiomyopathy in patients after posttransplant cyclophosphamide-based hematopoietic cell transplantation. Cancer 2017, 123, 1800–1809. [Google Scholar] [CrossRef] [PubMed]
- Yeh, J.; Whited, L.; Saliba, R.M.; Rondon, G.; Banchs, J.; Shpall, E.; Champlin, R.; Popat, U. Cardiac toxicity after matched allogeneic hematopoietic cell transplant in the posttransplant cyclophosphamide era. Blood Adv. 2021, 5, 5599–5607. [Google Scholar] [CrossRef] [PubMed]
- Duléry, R.; Mohty, R.; Labopin, M.; Sestili, S.; Malard, F.; Brissot, E.; Battipaglia, G.; Médiavilla, C.; Banet, A.; Van de Wyngaert, Z.; et al. Early Cardiac Toxicity Associated With Post-Transplant Cyclophosphamide in Allogeneic Stem Cell Transplantation. JACC Cardio Oncol. 2021, 3, 250–259. [Google Scholar] [CrossRef]
- Onishi, Y.; Mori, T.; Yamazaki, H.; Takenaka, K.; Yamaguchi, H.; Shingai, N.; Ozawa, Y.; Iida, H.; Ota, S.; Uchida, N.; et al. Cyclosporine/methotrexate versus tacrolimus/methotrexate with or without anti-thymocyte globulin as GVHD prophylaxis in adult patients with aplastic anemia. Ann. Hematol. 2021, 100, 217–228. [Google Scholar] [CrossRef]
- Piñana, J.L.; Valcárcel, D.; Fernández-Avilés, F.; Martino, R.; Rovira, M.; Barba, P.; Martínez, C.; Brunet, S.; Sureda, A.; Carreras, E.; et al. MTX or mycophenolate mofetil with CsA as GVHD prophylaxis after reduced-intensity conditioning PBSCT from HLA-identical siblings. Bone Marrow Transplant. 2010, 45, 1449–1456. [Google Scholar] [CrossRef] [PubMed]
- Ruggeri, A.; Sun, Y.; Labopin, M.; Bacigalupo, A.; Lorentino, F.; Arcese, W.; Santarone, S.; Gülbas, Z.; Blaise, D.; Messina, G.; et al. Post-transplant cyclophosphamide versus anti-thymocyte globulin as graft- versus-host disease prophylaxis in haploidentical transplant. Haematologica 2017, 102, 401–410. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | PTCY Cohort | ATG Cohort | p Value |
|---|---|---|---|
| n = 24 | n= 16 | ||
| Median age, years (range) | 51 (20–71) | 45 (21–61) | 0.39 |
| Gender, n (%) | 0.25 | ||
| Male | 11 (46) | 5 (31) | |
| Female | 13 (54) | 11 (69) | |
| Hematologic malignancy, n (%) | 0.63 | ||
| AML | 15 (63) | 12 (75) | |
| ALL | 5 (21) | 4 (25) | |
| MM | 3 (12) | - | |
| Other | 1 (4) | - | |
| Stem cell source, n (%) | 0.05 | ||
| Peripheral blood | 11 (46) | 12 (75) | |
| Bone marrow | 13 (54) | 4 (25) | |
| Time to transplant, months, median (range) | 11 (1–35) | 9 (1–44) | 0.23 |
| Stem cells infused, ×106/kg, median (range) | 3.70 (0.60–7.90) | 4.78 (1–8.29) | 0.05 |
| Type of donor, n (%) | 0.001 | ||
| Sister/brother | 7 (30) | 13 (72) | |
| Mother/father | 2 (8) | 2 (12) | |
| Son/daughter | 13 (54) | 1 (6) | |
| MUD | 2 (8) | - | |
| CMV serostatus, n (%) | 0.5 | ||
| R+/D+ | 17 (71) | 12 (75) | |
| R−/D+ | 3 (13) | 2 (12) | |
| R+/D− | 2 (8) | 1 (6) | |
| R−/D− | 2 (8) | 1 (6) | |
| Conditioning regimen, n (%) | 0.001 | ||
| TBF | 22 (92) | 5 (31) | |
| BU-FLU | 1 (4) | 9 (56) | |
| FLU-MEL | 1 (4) | - | |
| R-TBF | - | 2 (13) | |
| Type of conditioning, n (%) | 0.07 | ||
| Myeloablative | 17 (71) | 15 (94) | |
| Reduced intensity | 7 (29) | 1 (6) | |
| Immunosuppressive drugs, n (%) | 0.001 | ||
| CSA + MTX | - | 10 (63) | |
| CSA + tacrolimus | - | 6 (37) | |
| CSA + MMF | 24 (100) | - | |
| Engraftment failure, n (%) | 2 (8) | 3 (19) | 0.32 |
| Neutrophil engraftment, days, median (range) | 20 (11–36) | 16 (10–25) | 0.01 |
| Platelet engraftment, days, median (range) | 29 (11–184) | 16 (10–37) | 0.03 |
| Acute GvHD, sites, n (%) | 11 (46) | 6 (37) | 0.72 |
| Skin | 8 (32) | 4 (25) | |
| Intestine | 6 (24) | 1 (6) | |
| Liver | 4 (16) | 2 (13) | |
| Acute GvHD grading, n (%) | 0.8 | ||
| Grade I–II | 10 (40) | 5 (31) | |
| Grade III–IV | 1 (4) | 1 (6) | |
| Chronic GvHD, sites, n (%) | 10 (42) | 5 (31) | 0.8 |
| Skin | 7 (28) | 5 (31) | |
| Intestine | 2 (8) | 2 (13) | |
| Liver | 4 (16) | 1 (6) | |
| Lung | 1 (4) | 1 (6) | |
| Eyes | 1 (4) | - | |
| Chronic GvHD grading, n (%) | 0.7 | ||
| Mild | 6 (24) | 3 (19) | |
| Severe | 4 (16) | 2 (13) | |
| Donor lymphocyte infusion, n (%) | 3 (12) | 2 (13) | 0.97 |
| Hematological relapse, n (%) | 4 (16) | 8 (50) | 0.02 |
| All-cause deaths, n (%) | 9 (36) | 12 (75) | 0.02 |
| Causes of death, n (%) | 0.03 | ||
| Relapse | 3 (13) | 8 (50) | |
| GvHD | 3 (13) | 1(6) | |
| Infections | 3 (13) | 1(6) | |
| Others | - | 2 (12) | |
| Transplant-related mortality, n (%) | 4 (17) | 4 (25) | 0.56 |
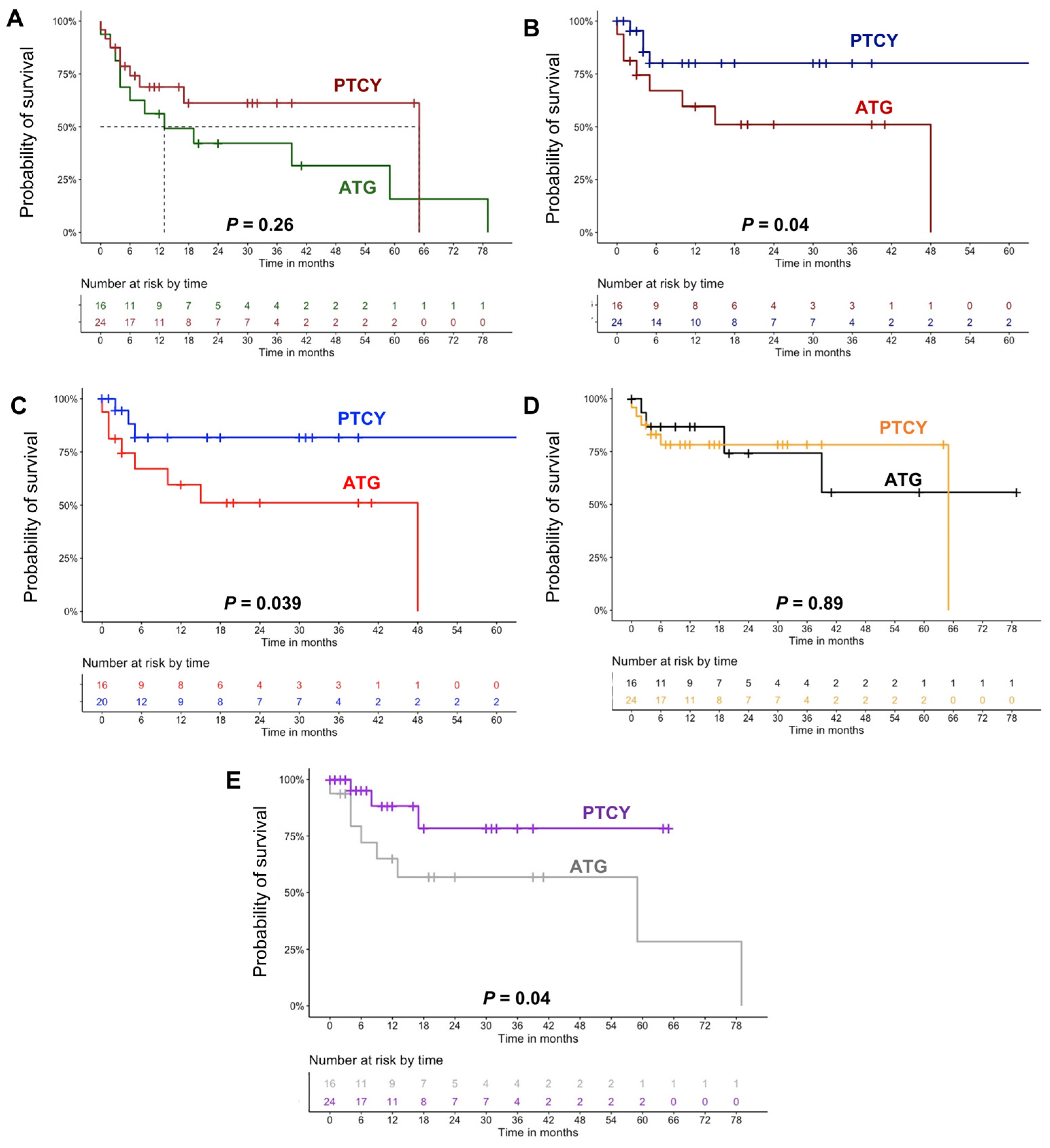
| 2-year relapse-free survival | 80% | 51% | 0.04 |
| 2-year overall survival | 61% | 42% | 0.26 |
| Dependent Variable = GvHD Occurrence | OR | 95%CI | p Value |
|---|---|---|---|
| PTCY [yes] | 1.27 | 0.34–4.69 | 0.72 |
| Gender [female] | 1.52 | 0.41–5.61 | 0.52 |
| Age, years | 0.96 | 0.91–1.01 | 0.12 |
| Bone marrow HSCs | 0.21 | 0.05–0.86 | 0.03 |
| Number of infused HSCs | 1.36 | 0.95–1.96 | 0.09 |
| Donor type [sister/brother] | 1.71 | 0.47–6.16 | 0.40 |
| RIC | 1.37 | 0.27–6.67 | 0.69 |
| Conditioning with TBF | 0.9 | 0.5–2.45 | 0.8 |
| Dependent Variable = Relapse | OR | 95%CI | p Value |
| PTCY [yes] | 0.2 | 0.04–0.85 | 0.03 |
| Gender [female] | 0.9 | 0.22–3.58 | 0.88 |
| Age, years | 0.98 | 0.93–1.03 | 0.57 |
| Bone marrow HSCs | 0.57 | 0.14–2.36 | 0.44 |
| Number of infused HSCs | 1.21 | 0.86–1.70 | 0.27 |
| Donor type [sister/brother] | 2.6 | 0.64–10.9 | 0.17 |
| RIC | 1.34 | 0.23–7.97 | 0.73 |
| Conditioning with TBF | 0.7 | 0.4–2 | 0.5 |
| Dependent Variable = Neutrophil Engraftment | β | 95%CI | p Value |
| Gender [female] | −0.3 | −4.54/3.82 | 0.86 |
| Age, years | −0.1 | −0.24/0.04 | 0.17 |
| PTCY [yes] | 5 | 1.23/8.81 | 0.01 |
| Bone marrow HSCs | 5.23 | 1.59/8.88 | 0.01 |
| Number of infused HSCs | −0.8 | −1.8/0.15 | 0.09 |
| Donor type [sister/brother] | −1 | −5.1/3.02 | 0.61 |
| RIC | 0.24 | −4.73/5.22 | 0.1 |
| Dependent Variable = Platelet Engraftment | β | 95%CI | p Value |
| Gender [female] | 3.7 | −17.9/25.3 | 0.72 |
| Age, years | 0.32 | −0.44/1.09 | 0.4 |
| PTCY [yes] | 17 | 0.5/35 | 0.04 |
| Bone marrow HSCs | 16.1 | −3.7/34 | 0.1 |
| Number of infused HSCs | −5.1 | −10.3/−0.01 | 0.09 |
| Donor type [sister/brother] | −0.2 | −4.1/2.04 | 0.57 |
| RIC | 3.67 | −24.4/31.8 | 0.89 |
| Dependent Variable = GvHD Occurrence | OR | 95%CI | p Value |
|---|---|---|---|
| Age, years | 0.95 | 0.62–1.91 | 0.16 |
| Bone marrow HSCs | 0.29 | 0.03–2.75 | 0.28 |
| Number of infused HSCs | 1.09 | 0.62–1.91 | 0.74 |
| Dependent Variable = Relapse | OR | 95%CI | p Value |
| PTCY [yes] | 0.08 | 0.01–0.89 | 0.03 |
| Age, years | 0.98 | 0.92–1.05 | 0.72 |
| Number of infused HSCs | 1.1 | 0.72–1.66 | 0.65 |
| Donor type [sister/brother] | 2.03 | 0.59–6.98 | 0.25 |
| Dependent Variable = Neutrophil Engraftment | β | 95%CI | p Value |
| Age, years | −0.1 | −0.2/0.01 | 0.07 |
| PTCY [yes] | 4 | 0.5/7.70 | 0.03 |
| Bone marrow HSCs | 4.1 | 0.67–7.69 | 0.02 |
| Dependent Variable = Platelet Engraftment | β | 95%CI | p Value |
| Age, years | 0.26 | −0.47/1.01 | 0.47 |
| PTCY [yes] | 4 | −5.65/36.8 | 0.14 |
| Bone marrow HSCs | 11.9 | −9.06/32 | 0.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serio, B.; Storti, G.; D’Addona, M.; Santoro, L.; Frieri, C.; De Novellis, D.; Marano, L.; De Santis, G.; Guariglia, R.; Manfra, I.; et al. Post-Transplant Cyclophosphamide versus Anti-Thymocyte Globulin in Patients with Hematological Malignancies Treated with Allogeneic Hematopoietic Stem Cell Transplantation from Haploidentical and Matched Unrelated Donors: A Real-Life Experience. Hematol. Rep. 2024, 16, 234-243. https://doi.org/10.3390/hematolrep16020023
Serio B, Storti G, D’Addona M, Santoro L, Frieri C, De Novellis D, Marano L, De Santis G, Guariglia R, Manfra I, et al. Post-Transplant Cyclophosphamide versus Anti-Thymocyte Globulin in Patients with Hematological Malignancies Treated with Allogeneic Hematopoietic Stem Cell Transplantation from Haploidentical and Matched Unrelated Donors: A Real-Life Experience. Hematology Reports. 2024; 16(2):234-243. https://doi.org/10.3390/hematolrep16020023
Chicago/Turabian StyleSerio, Bianca, Gabriella Storti, Matteo D’Addona, Lidia Santoro, Camilla Frieri, Danilo De Novellis, Luana Marano, Giovanna De Santis, Roberto Guariglia, Ilenia Manfra, and et al. 2024. "Post-Transplant Cyclophosphamide versus Anti-Thymocyte Globulin in Patients with Hematological Malignancies Treated with Allogeneic Hematopoietic Stem Cell Transplantation from Haploidentical and Matched Unrelated Donors: A Real-Life Experience" Hematology Reports 16, no. 2: 234-243. https://doi.org/10.3390/hematolrep16020023
APA StyleSerio, B., Storti, G., D’Addona, M., Santoro, L., Frieri, C., De Novellis, D., Marano, L., De Santis, G., Guariglia, R., Manfra, I., Urciuoli, E., Luponio, S., Marotta, S., Morini, D., Rizzo, M., Palmieri, F., Cantore, N., Giudice, V., Risitano, A. M., & Selleri, C. (2024). Post-Transplant Cyclophosphamide versus Anti-Thymocyte Globulin in Patients with Hematological Malignancies Treated with Allogeneic Hematopoietic Stem Cell Transplantation from Haploidentical and Matched Unrelated Donors: A Real-Life Experience. Hematology Reports, 16(2), 234-243. https://doi.org/10.3390/hematolrep16020023