Abstract
Data on antibody response (AR) after vaccination against SARS-CoV2 in hematopoietic stem-cell transplantation setting (HSCT) were initially scarce, mainly due to the exclusion of such patients from approval studies. Shortly after the worldwide application of vaccination against SARS-CoV-2 in vulnerable populations such as patients with hematologic malignancies, limited single-center trials, including HSCT patients, were published. However, there was a great heterogeneity between them regarding the type of underlying malignancy, co-current treatment, type of vaccine, method of AR measurement, and time point of AR measurement. Herein, we present the results of a prospective study on AR after vaccination for SARS-CoV-2 using the BNT162b2 vaccine in a cohort of 54 HSCT recipients—mostly autologous from a single Unit—along with a broad review of the current literature. In our cohort, the AR positivity rate at 1 month was 80.8% and remained positive in 85.7% of patients at 3 months after vaccination. There were only nine non-responders, who were more heavily pretreated and more frequently hypogammaglobulinemic compared to responders. High antibody titers (AT), [AT ≥ 1000 U/mL], were detected in 38.5% and 30.6% of the patients at m1 and m3, respectively. A significant decline in AT between m1 and m3 was demonstrated—p < 0.0001; median AT1 and AT3 were 480.5 and 293 U/mL, respectively. A novel finding of our study was the negative impact of IgA hypogammaglobulinemia on response to vaccination. Other negative significant factors were treatment with anti-CD20 antibody at vaccination and vaccination within 18 months from HSCT. Our data indicate that HSCT recipients elicit a positive response to the BNT162b2 vaccine against SARS-CoV-2 when vaccinated at 6 months post-transplant, and vaccination should be offered to this patient population even within the post-pandemic COVID-19 era.
1. Introduction
Patients with hematologic malignancies (HM) demonstrate a higher risk of severe COVID-19 disease, reflected in the doubled mortality rate of the unselected HM population compared to the control group (14% versus 7%) in a large population-based study []. Based on a large meta-analysis of observational data on HM patients with COVID-19 disease, the overall mortality rate in hospitalized adults is estimated at around 40%, ranging from 23% to 70% in various studies []. Moreover, the clinical outcome of hematopoietic stem-cell transplantation (HSCT) recipients is even more unfavorable; the risk of COVID-19 lower respiratory tract disease exceeds 80% with incidence of ICU admission ranging from 20% to 25% and overall mortality >25% [,].
HSCT is considered the standard of care for a variety of HM, albeit it is associated with significant secondary immunodeficiency. Thus, prophylactic vaccination for common pathogens is strongly recommended for the protection of this vulnerable population. During the first two years of the COVID-19 pandemic, vaccination has been the most effective measure against SARS-CoV-2 infection due to the limited therapeutic options. However, HSCT recipients have been excluded from the initial vaccination studies, resulting in uncertainty concerning its efficacy in inducing adequate responses. Lower antibody titers have been observed in solid organ transplantation recipients [] and in patients with chronic lymphocytic leukemia (CLL) treated with anti-CD20 antibodies [,], while data regarding outcomes in HSCT recipients are limited.
We here report the results of a prospectively designed study on antibody response to vaccination for SARS-CoV-2 using the BNT162b2 vaccine in a cohort of 54 HSCT recipients from a single Unit.
2. Materials and Methods
This monocentric prospective study included HM patients without previously documented SARS-CoV-2 infection having undergone HSCT—autologous (auto-HSCT) or allogeneic(allo-HSCT)—at least 6 months before and within 5 years from the time of vaccination. All patients were vaccinated between March and May 2021 with two doses of the BNT162b2 vaccine (Pfizer–BioNTech COVID-19 vaccine, New York, NY, United States-Mainz, Germany) as part of the National Public Health Organization Vaccination Program in Greece against SARS-CoV-2 disease. Informed consent was given by all participants. Blood samples for antibody titers (AT) were collected before the first dose (m0)—to exclude previous asymptomatic infection- as well as at 1 month (m1) and at 3 months (m3) after the second dose (δ2) of the vaccination. The serum was separated and preserved at −20 °C until AT measurement at each time point: AT0, AT1, and AT3.
Serum antibodies against SARS-CoV-2 were measured with Elecsys Anti-SARS-CoV-2 S immunoassay (Roche Diagnostics International AG, Rotkreuz, Switzerland), which uses a recombinant protein representing the receptor-binding domain (RBD) on the S1 subunit of the spike antigen in a double-antigen sandwich assay format. Numeric values ≥0.8 U/mL are interpreted as “positive”, with the analytical range of the assay measuring between 0.4 and 250 U/mL, reaching up to 2500 U/mL for 10-fold diluted samples. Median AT in healthy individuals at 1 month after vaccination is reported to be ≥1000 U/mL, measured by the same method [].
Seroconversion, i.e., a positive antibody response (AR), was defined as any value ≥0.8 U/mL. Patient and disease characteristics, type and timing of HSCT, ongoing treatment, and laboratory parameters were examined as possible prognostic factors for response to vaccination. Non-parametric tests were used for such comparisons. Related samples Wilcoxon signed rank test were used to examine differences between AT1 and AT3. Prognostic factor analysis was performed in two ways: firstly, qualitatively for a positive vs. negative AR by Chi-square and secondly, quantitatively with antibody titers as a continuous variable. p-values < 0.05 were considered statistically significant, and all p-values were 2-sided. Statistical analyses were carried out with IBM SPSS Statistics version 25. Time interval between HSCT and vaccination (TITV) was defined as the time between stem cell infusion and δ2. No treatment (NT) was defined as not having received any treatment for the underlying HM for a period of more than 6 months before δ2. Hypogammaglobulinemia was defined as values below the lower normal limit level for each class of immunoglobulins: IgG < 7 g/L, IgA < 0.7 g/L, and IgM < 0.4 g/L.
3. Results
Fifty-four (54) patients were included in this prospective study. Their characteristics are depicted in Table 1. Briefly, their median age was 56 (19–71) years, and 30 were male. There were only four patients who had undergone sibling allo-HSCT; all four of them had acute leukemia: two acute myelogenous and two acute lymphoblastic. The remaining 50 patients (92%) had been subjected to auto-HSCT: 31 for lymphoma (12 for Hodgkin lymphoma (HL), 19 for non-Hodgkin lymphoma (NHL)) and 19 for multiple myeloma (MM). One patient who had undergone autologous HSCT for transformed follicular lymphoma experienced multiple relapses and finally developed secondary myelodysplastic syndrome with monosomy, and seven were receiving azacitidine at the time of vaccination.

Table 1.
Patients’ Characteristics.
Samples were available at both time points, i.e., at m1 and at m3 post-vaccination, in 47/54 patients (87%), while five patients had measurements at m1 only and two patients at m3 only. With the cut-off value of 0.8 U/mL for positivity, 42 out of 52 patients (80.8%) and 42 out of 49 patients (85.7%) had a positive AR at m1 and m3, respectively. Thus, only 19.2% and 14.3% did not elicit any AR at the prespecified time points, respectively.
When focusing on the characteristics of patients with absent AR, we identified 10 patients with undetectable antibodies at m1. Among these 10 patients, only 1 converted to positive with high AT3 (97.9 U/mL) and was considered as a responder. Another patient developed a very low AT3 (1.38 U/mL), which is very close to the cut-off value of 0.8 U/mL and was considered a non-responder; measurement at m3 was unavailable for two patients. The characteristics of these nine non-responders are shown in Table 2. The comparison of these non-responders to the remaining patients revealed that the formers were more heavily pretreated (the median number of previous lines of therapy was five vs. three for patients with AR, p = 0.05), and they were more frequently hypogammaglobulinemic [7/9 non-responders (78%) vs. 14.7% of responders, p = 0.004]. Treatment at vaccination also differed significantly. The distribution of treatment among non-responders vs. responders was the following: 22.2% vs. 59.5% were off any treatment, 0% vs. 26.2% were receiving lenalidomide, 33.3% vs. 47.0% were on anti-CD20 antibody, and 44.4% vs. 9.5% were on other therapy, respectively.
Table 2.
Characteristics of patients with no detectable antibody response.
The distribution of AT is shown in Table 3; no patient had detectable antibodies before vaccination. High titers, i.e., AT ≥ 1000 U/mL, were detected in 38.5% and 30.6% of the patients at m1 and m3, respectively. There was a significant correlation between AT1 and AT3 (p < 0.0001).
Table 3.
Distribution of antibody titers at 1- and 3-months post-vaccination.
This observation highlights the fact that patients with high AT1 did so at m3, as well, while patients with lower titers at m1 had a similar magnitude of AT3. On the other hand, a significant decline in AT between m1 and m3 was demonstrated, p < 0.0001; median AT1 and AT3 were 480.5 (0.4–25,000) and 293 (0.4–7869)U/mL, respectively (Figure 1).
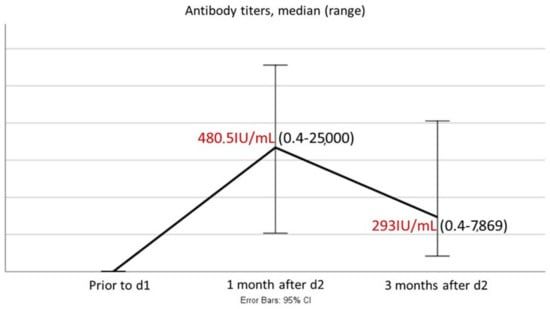
Figure 1.
Variability of antibody titers between 1 and 3 months post-vaccination (median AT, 1 and 3 months post-vaccination, are colored with red).
Specifically, AT decreased in 75% of the patients and increased in 17%, while antibodies remained undetectable in 11% of patients with available both AT1 and AT3 (Figure 2).
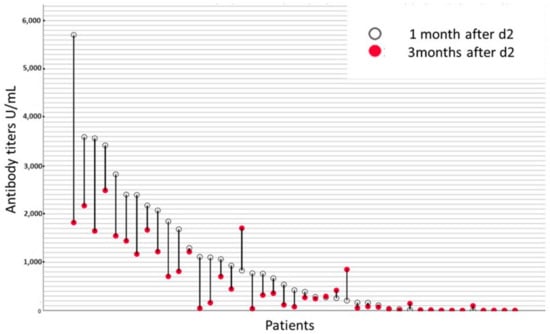
Figure 2.
Kinetics of antibody titers between 1- and 3-months post-vaccination at each individual patient.
Then, we investigated potential predictive factors for immunogenicity of BNT162b2. We correlated disease and patient parameters firstly with seroconversion (positive AR) and secondly with the magnitude of AR (AT at m1 and m3). Age, sex, type of HSCT, and absolute lymphocyte/monocyte counts did not prove significant. There was a trend for underlying HM to correlate both with seroconversion and AT (p = 0.06 for both): HL patients displayed the highest AT1 (median: 2118 U/mL), followed by MM (median: 330.0 U/mL), while NHL patients had the lowest AT (median: 121.15 U/mL). However, most likely, this observation is confounded by the treatment received at the time of vaccination. Interestingly, all four acute leukemia patients who had undergone allogeneic HSCT had high AT (AT1 were 538.0 U/mL, 1065 U/mL, 2174 U/mL, and 3591 U/mL, for the four patients).
Factors that proved statistically significant for seroconversion and the magnitude of AT are depicted in Table 4.
Table 4.
Significant prognostic factors for antibody response.
3.1. Treatment
The most significant factor was the type of treatment at the time of vaccination (p < 0.0001). Patients on anti-CD20 antibodies had the lowest AT (median AT1 and AT3 0.4 U/mL), followed by those on other chemotherapies (median AT1 = 9755 U/mL and AT3 = 95.85 U/mL), while the ones on lenalidomide, although positive, they displayed lower AT (median AT1 = 210.0 U/mL and AT3 = 118.0 U/mL). Patients off any treatment had significantly higher AT: median 1488 U/mL at m1 and 1193 U/mL at m3. Among the five patients who were on anti-CD20 antibodies at the time of vaccination, three did not elicit any AR and are described in Table 2. One patient had a negative AR at m1 and a positive AR at m3 (AT3 = 97.9 U/mL), and the remaining one had 423.0 U/mL and 77.8 U/mL at m1 and m3, respectively. Among eight patients receiving other therapies at vaccination, four did not develop any AR and are also depicted in Table 2, while the remaining four had AT ranging between 18.5 U/mL and 1844 U/mL at m1 and between 46.7 and 850.0 U/mL at m3. All 11 patients on lenalidomide at the time of vaccination had a positive AR; only one with very low titers (AT1 = 10.2 U/mL and AT3 = 4.06 U/mL). Additionally, more heavily pretreated patients (≥3 lines of previous therapies) had significantly lower AT, both at m1 and m3, p = 0.016 and p = 0.026, respectively. However, the seroconversion rate did not differ significantly according to the number of previous lines of treatment.
3.2. Hypogammaglobulinemia
Low IgG levels, either at the threshold of 7 g/L or 5 g/L, did not reach statistical significance. Surprisingly, IgA hypogammaglobulinemia predicted both for a lower seroconversion rate at m1 and m3, as well as for significantly lower AT at both time points. More specifically, 50% and 60% of patients with IgA < 0.7 g/L had a positive AR at m1 and m3 vs. 86% and 89% for patients with normal IgA levels, respectively (p = 0.019 and p = 0.046). Median AT at m1 for IgA hypogammaglobulinemic patients was 5.3 U/mL vs. 388.0 U/mL for those with normal IgA levels (p = 0.02). This difference remained significant at m3 with corresponding values of 25.38 U/mL and 269.0 U/mL). Due to this unexpected finding, we further investigated the impact of “any class hypogammaglobulinemia” (IgG and/or IgA and/or IgM levels lower than normal) vs. no hypogammaglobulinemia (IgG and IgA and IgM within normal range). We found that hypogammaglobulinemia of any class was significantly associated with decreased seroconversion rate and lower AT. More specifically, 16/25 patients (64%) with any class hypogammaglobulinemia developed a positive AR at m1 vs. 16/17 (94%) among those with normal immunoglobulins of all classes (p = 0.02). Moreover, the median AT1 was 110 U/mL for those with any class hypogammaglobulinemia vs. 1065 U/mL for the ones with normal immunoglobulin levels (p = 0.018). The corresponding AT3 values were 86.7 U/mL vs. 850.0 U/mL, p = 0.017.
Based on the above observations and in order to further elucidate the role of IgA hypogammaglobulinemia, we identified three groups of patients: group A: patients with normal levels of all classes of immunoglobulins; group B: patients with normal IgA levels and lower than normal levels of the other two classes of immunoglobulins (either IgG or IgM or both); group C: IgA hypogammaglobulinemia, irrespectively of the values of the other two immunoglobulin classes. Group A (n = 15) depicted the highest AT1, followed by group B (n = 14), while group C (n = 10) had the lowest AR; AT1 was 539.0 U/mL vs. 277.0 U/mL vs. 5.3 U/mL, respectively (p = 0.049). The corresponding values at m3 post-vaccination were 704.0 U/mL, 203.0 U/mL, and 25.3 U/mL for groups A, B, and C, respectively.
3.3. Time between HSCT and Vaccination
Patients vaccinated within 18 months post-HSCT had lower AT at m1 compared to the ones who were vaccinated ≥18 months after HSCT, p = 0.037, but at m3, this difference was not significant (p = 0.29).
4. Discussion
Recent data on COVID-19 disease in HSCT recipients indicate poor short-term outcomes in both autologous and allogeneic settings; 30-day overall survival after COVID-19 diagnosis was estimated at around 67–68% []. Factors such as older age, poor performance status, comorbidities, and high-level immunosuppression were associated with increased mortality []. Thus, preventing COVID-19 disease by vaccination of HSCT recipients against SARS-CoV-2 is of uttermost importance. Conditioning regimens, maintenance therapies after transplantation—such as anti-CD20 antibodies, immunomodulatory drugs, and FLT3 inhibitors, presence and treatment of graft-versus-host disease, and persistent hypogammaglobulinemia are the main factors negatively affecting immune response following vaccination of HSCT recipients [,].
In August 2021, the CDC’s primary recommendation on booster doses in immunocompromised patients included HSCT recipients within the last 2 years or those under immunosuppressive treatment (https://www.cdc.gov/coronavirus/2019ncov/vaccines/recommendations/immuno.html, accessed on 1 September 2021). However, this recommendation was mainly based on a small case series of solid-organ transplant recipients []. More recently (March 2022), ASH and ASCT recommendations strongly recommended vaccination for HSCT recipients, their caregivers, family, and household contacts. Despite that, objective data still remain scarce regarding the type of transplant, time of vaccination, and efficacy of different vaccines, as well as the duration of the immune response.
Table 5 summarizes single-center studies that examined the serologic response of two doses of the BNT162b2 (Pfizer) vaccine against SARS-CoV-2 in HSCT recipients [,,,,,,,,,,,,,,,,,]. The time point of AR measurement varied between these studies: the median time of AT measurement ranged between 18 and 38 days post δ2. They mainly include allo-HSCT recipients, and the positivity rate for AR ranges between 55% and 96%. In addition, most of them provide no information about AT. The threshold of “protective” titers has not been established and differs according to the methodology used, the timing of measurement, and the characteristics of the population studied.
Table 5.
Single-center studies that examined the serologic response of two doses of the BNT162b2 (Pfizer) vaccine against SARS-CoV-2 in hematopoietic stem-cell transplantation recipients.
The novelty of our study relies on the fact that this was a prospectively designed study, with all patients having been treated in a single Transplantation Unit and, most importantly, measurements having been performed at pre-specified time points. Moreover, our study included two sequential prospectively defined measurements at 1 and 3 months post δ2, trying to elucidate the short-term kinetics of antibody responses in transplanted patients. Only Tamari et al. have analyzed AT in HSCT recipients at two time points [].
Data on AR after vaccination with the BNT162b2 vaccine against SARS-CoV2 in auto-HSCT recipients are limited. There are seven other studies with a number of auto-HSCT patients ranging between 38 and 86 [,,,,,,]. Our study included 54 patients, among whom the majority (50 patients) had undergone auto-HSCT. Although all four patients who had undergone sibling allo-HSCT for acute leukemia had high AT, we cannot draw conclusions regarding allo-HSCT from our data. Thus, our analysis focuses on auto-HSCT.
Our first observation is that >80% of transplanted patients do elicit AR against SARS-CoV-2 after BNT162b2 vaccine. According to a large meta-analysis of 49 studies in adults with HM without allogeneic or autologous HSCT, the pooled AR was 50%, 58%, 61%, and 76% for patients with CLL, aggressive B-NHL, indolent B-NHL, and multiple myeloma []. Thus, auto-HSCT per se does not represent a risk factor for blunted AR. Consequently, HSCT recipients should be vaccinated, similarly to the general population. This observation is in accordance with most published studies [,,,,,,,,,,,,,,,,,]. Only two investigators [,] reported lower seroconversion rates (60% and 67%). However, both of these analyses were retrospective; different types of vaccines were used, and the time of measurement varied [,]. There are only three other studies using exclusively the BNT162b2 vaccine. All of them have reported AR rates of ≥87% [,,], which compares favorably with the 81% and 86% AR rates at 1 and 3 months post-vaccination in our analysis. Furthermore, >30% of our patients had high titers, i.e., ≥1000 U/mL, which has been reported as the median value for healthy individuals at 1 month post vaccination []. We chose to include patients who had been transplanted at least 6 months before, according to the usual vaccination programs for other pathogens followed by most HSCT centers []. Few other investigators [,,] reported measurement of AT. Comparisons between studies regarding AT cannot be performed due to the different methodologies used. Moreover, the clinical significance of specific AT thresholds is unknown. A drawback of our analysis is the absence of a healthy control (HC) group. Tamari et al., who included an HC group, did find significantly lower AT in auto-HSCT patients compared to HC, while the qualitative seroconversion rate was reported as 100% in HC vs. 87% in the transplant group [].
Our second observation is the declining trend of AT between m1 and m3. However, approximately 85% of the patients had a positive antibody response at m3. Thus, the usual practice of administering a booster dose between 3 and 6 months after the previous vaccine dose seems rational for HSCT recipients, as well. As mentioned above, only Tamari et al. performed measurements at two time points. Their study was a prospective observational one with a similar design to ours, including 61 autologous recipients. In contrast to our results, they reported a significant increase in AT between the first and the second measurement. However, they chose a different schedule: the first measurement was at 1 month, and the second measurement was at 3 months post-first dose, while we measured AT at 1 and 3 months post-second dose []. Practically, both chosen time points of measurement were approximately 1 month earlier than in our analysis, and this difference might explain the contradiction in AT kinetics between their study and ours.
Our third observation is that specific factors may predict the magnitude of AR in HSCT recipients. We found that treatment at vaccination, ≥3 lines of previous therapy, hypogammaglobulinemia, and an interval of <18 months between vaccination and HSCT predict a blunted AR.
Active disease-oriented treatment, especially within 6 months before vaccination has been reported as a negative factor for response by other investigators, as well [,]. We found that patients of any treatment had the highest positivity rate (92%) and the highest AT compared to all others on any kind of treatment within 6 months. Rituximab-treated patients demonstrated the lowest AR: among our five patients who had received rituximab, three patients were negative, one patient was negative at m1 but seroconverted at m3, while only one patient elicited a positive antibody response at both time points. It is widely known from B-NHL and CLL patients that B-cell lymphodepleting treatment with anti-CD20 antibodies is a major determinant of a diminished antibody response []. In the auto-HSCT setting, anti-CD20 treatment is associated with >50% failure in seroconversion rate [,]. The largest study including rituximab-treated patients by Auttore et al., specifically, demonstrated that those treated with Rituximab within 6 months from vaccination had an inferior AR than those treated >6–≤12 months and >12 months; 13% vs. 50% vs. 87%, respectively []. In their study, similarly to ours, the distribution of lymphoma and myeloma patients was well balanced in contrast to others that included more myeloma patients and consequently did not find rituximab as a significant factor [,,]. Other specific treatments that have been associated with a blunted AR are daratumumab [] (Tamari) and steroids []. In our patient population, lenalidomide maintenance did not have an impact on the seroconversion rate but was associated with lower AT compared to any treatment group. A similar observation was reported by Tamari et al. []. In our analysis, although the number of previous therapies did not correlate with seroconversion failure, we found that patients who had <3 lines of treatment had significantly higher AT at both time points. Such a correlation has not been reported yet by others. With respect to the TITV, two other studies have identified a time interval of <12 months as a negative predictive factor [,]. In our analysis, patients with TITV <18 months elicited significantly lower AT at 1 month compared to those with TITV ≥18 months, but the seroconversion rate was similar.
Another reported predictive parameter for blunted AR is an absolute number of circulating CD19+ B-cells <50/μL at vaccination [] or ≤100/μL at 30 days post-vaccination [].
Our most important and novel observation is the impact of IgA hypogammaglobulinemia on response to vaccination. Most studies on hypogammaglobulinemia and anti-SARS-CoV-2 vaccination have generally focused on IgG levels. Thus, IgG hypogammaglobulinemia (<5 g/L) has been identified as a risk factor for blunted AR [,]. On the other side, IgA response has been shown as an important factor of early neutralization of SARS-CoV-2 virus after infection, while there is limited data showing both increased positivity for anti-SARS-CoV-2 IgA in the serum and mucosal secretions after immunization []. In the HSCT setting, only Tamari et al. reported an inferior AR for patients with IgG levels <5 g/L; however, this was at a non-significant level []. No other investigator has analyzed immunoglobulin levels in the auto-HSCT setting. We performed a detailed analysis of the effect of immunoglobulin levels of all classes and showed that hypogammaglobulinemia of any class (IgG, IgA, or IgM) was associated with significantly lower AT. Most importantly, IgA below the lower normal limit proved to be even more significant. Thus, 50% and 40% of patients with IgA <0.7 g/L had a negative AR at m1 and m3, respectively. Moreover, AT was significantly lower at both time points for IgA hypogammaglobulinemic patients. Based on these findings, we further investigated the impact of IgA hypogammaglobulinemia in combination with abnormalities of other classes of immunoglobulins. We identified three groups of equally distributed number of patients. Patients with normal levels of all immunoglobulin classes displayed the highest AT; those with normal IgA levels but low levels of either/and IgG or IgM had the second highest AT, while the ones with lower-than-normal IgA irrespectively of IgG and IgM levels had the lowest AT. This observation highlights the importance of IgA levels in eliciting proper response to vaccination. Thus, measuring not only IgG but also IgM and IgA levels is essential for predicting HSCT recipients with inadequate AR.
We identified nine patients—16.6% of the whole patient population—who had absent AR. These non-responders differed from responders in many aspects: they were more heavily pretreated, and almost 80% were hypogammaglobulinemic vs. ~15% of responders. Additionally, approximately 80% of non-responders were on active treatment at vaccination, in contrast to 40% of responders.
Regarding the limitations of our study, it should be noted that it included a relatively small number of patients. Secondly, we have not examined the B-cell and T-cell subpopulations of these patients. Moreover, our study lacks analysis of other cellular immunity markers and especially lacks the measurement of neutralizing antibodies against SARS-CoV-2. Lastly, our study did not include a healthy control group AR in order to be compared with HSCT recipients, and it lacks long-term measurement of AR of these patients in order to identify the durability of their response.
HSCT recipients are particularly vulnerable to SARS-CoV-2 infection due to profound immune dysfunction and the prolonged timeline for immune reconstitution, especially in heavily pretreated patients in the early transplantation period (<12 months). Hopefully, encouraging preliminary data suggests that SARS-CoV-2 vaccination reduces the severity of breakthrough COVID-19 infection in this population with mortality <10% []. In our cohort, there was no breakthrough infection. Thus, these observations are important when designing preventive measures within the continuing COVID-19 pandemic for vulnerable subgroups of citizens. Especially nowadays, where preventive monoclonal antibodies have become available but are still in limited supply, careful prioritization of people at high risk should be applied. In this context, auto-HSCT per se does not represent a high-risk feature, and these patients should follow the National Vaccination Programs since they elicit adequate AR. On the other hand, hypogammaglobulinemic patients, especially IgA, those on lymphoma or myeloma treatment, especially with monoclonal antibodies, heavily treated patients, and those who are close to HSCT are the ones who are less likely to respond to vaccination and should receive prophylactic monoclonal antibodies against SARS-CoV-2. Another aspect based on these observations is that post-transplant treatment should be given with caution during the pandemic, especially if administered as maintenance. Although the morbidity and mortality of COVID-19 disease have decreased with the newer virus strains, immunocompromised patients may still experience serious complications. Moreover, SARS-CoV-2 infection may lead to delays in treatment with serious consequences in disease outcomes. Even nowadays immunization represents the major intervention against SARS-CoV-2 in patients with hematologic malignancies undergoing auto-HSCT.
5. Conclusions
Conclusively, over 80% of patients who have undergone HSCT do elicit antibody responses after vaccination with the BNT162b2 vaccine (Pfizer–BioNTech COVID-19 vaccine, New York, NY, United States-Mainz, Germany) against SARS-CoV-2 with a declining trend over a 3-month period. Treatment given post-transplant and especially anti-CD20, as well as hypogammaglobulinemia, are the major determinants of AR, rather than transplantation itself.
Author Contributions
Conceptualization, J.V.A. and M.K.A.; methodology, J.V.A., E.L., G.S., M.M., E.K., I.D., I.V., A.N.G., A.K. (Anastasia Kopsaftopoulou), A.M., A.P. (Alexia Piperidou), A.K. (Anestis Karapaschalidis), M.-E.L., D.G., M.-P.A., P.P. (Panagiota Petsa), E.B., M.P.S., A.G.P., P.T., P.P. (Panayiotis Panayiotidis), T.P.V., A.P. (Angeliki Papanagiotou) and M.K.A.; software, M.K.A.; validation, J.V.A. and M.K.A.; formal analysis, J.V.A. and M.K.A.; investigation, J.V.A., E.L., G.S., M.M., E.K., I.D., I.V., A.N.G., A.K. (Anastasia Kopsaftopoulou), A.M., A.P. (Alexia Piperidou), A.K. (Anestis Karapaschalidis), M.-E.L., D.G., M.-P.A., P.P. (Panagiota Petsa), E.B., M.P.S., A.G.P., P.T., P.P. (Panayiotis Panayiotidis), T.P.V., A.P. (Angeliki Papanagiotou) and M.K.A.; resources, J.V.A., E.L., G.S., M.M., E.K., I.D., I.V., A.N.G., A.K. (Anastasia Kopsaftopoulou.), A.M., A.P. (Alexia Piperidou), A.K. (Anestis Karapaschalidis), M.-E.L., D.G., M.-P.A., P.P. (Panagiota Petsa), E.B., M.P.S., A.G.P., P.T., P.P.(Panayiotis Panayiotidis), T.P.V., A.P. (Angeliki Papanagiotou) and M.K.A.; data curation, J.V.A. and M.K.A.; writing—original draft preparation, J.V.A. and M.K.A.; writing—review and editing, J.V.A. and M.K.A.; visualization, J.V.A. and M.K.A.; supervision, M.K.A.; project administration, M.K.A.; funding acquisition, M.K.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The authors would like to clarify that this prospective study was not conducted as part of an experimental process on humans. Instead, during the SARS-CoV-2 pandemic, there was a strong recommendation globally by the WHO and other known medical associations (such as CDC, ASH, and ASCT) for vaccination of patients with hematologic malignancies initially with two doses of the BNT162b2 vaccine. In Greece, all these patients, including patients with hematologic malignancies having undergone stem-cell transplantation, were vaccinated as part of the National Vaccination Program against SARS-CoV-2 designed and undertaken by the Greek Ministry of Health, according to the international guidelines. As a result, neither the Ethics Committee nor Institutional Review Board approval was required for this study. However, as mentioned in the manuscript, all participants in this prospective analysis have given informed consent in order to perform the collection of blood samples and the measurement of their antibody response.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
No new data was created or analyzed in this study. Data is contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Yigenoglu, T.N.; Ata, N.; Altuntas, F.; Bascı, S.; Dal, M.S.; Korkmaz, S.; Namdaroglu, S.; Basturk, A.; Hacıbekiroglu, T.; Dogu, M.H.; et al. The Outcome of COVID-19 in Patients with Hematological Malignancy. J. Med. Virol. 2021, 93, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Vijenthira, A.; Gong, I.Y.; Fox, T.A.; Booth, S.; Cook, G.; Fattizzo, B.; Martín-Moro, F.; Razanamahery, J.; Riches, J.C.; Zwicker, J.; et al. Outcomes of Patients with Hematologic Malignancies and COVID-19: A Systematic Review and Meta-Analysis of 3377 Patients. Blood 2020, 136, 2881. [Google Scholar] [CrossRef]
- Sharma, A.; Bhatt, N.S.; St Martin, A.; Abid, M.B.; Bloomquist, J.; Chemaly, R.F.; Dandoy, C.; Gauthier, J.; Gowda, L.; Perales, M.A.; et al. Clinical Characteristics and Outcomes of COVID-19 in Haematopoietic Stem-Cell Transplantation Recipients: An Observational Cohort Study. Lancet Haematol. 2021, 8, e185–e193. [Google Scholar] [CrossRef]
- Ljungman, P.; de la Camara, R.; Mikulska, M.; Tridello, G.; Aguado, B.; Zahrani, M.A.; Apperley, J.; Berceanu, A.; Bofarull, R.M.; Calbacho, M.; et al. COVID-19 and Stem Cell Transplantation; Results from an EBMT and GETH Multicenter Prospective Survey. Leukemia 2021, 35, 2885–2894. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 MRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv, T.; Shorer Arbel, Y.; Scarfò, L.; et al. Efficacy of the BNT162b2 MRNA COVID-19 Vaccine in Patients with Chronic Lymphocytic Leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Gavriatopoulou, M.; Fotiou, D.; Giatra, C.; Asimakopoulos, I.; Dimou, M.; Sklirou, A.D.; Ntanasis-Stathopoulos, I.; Darmani, I.; Briasoulis, A.; et al. Poor Neutralizing Antibody Responses in 132 Patients with CLL, NHL and HL after Vaccination against SARS-CoV-2: A Prospective Study. Cancers 2021, 13, 4480. [Google Scholar] [CrossRef]
- Werbel, W.A.; Boyarsky, B.J.; Ou, M.T.; Massie, A.B.; Tobian, A.A.R.; Garonzik-Wang, J.M.; Segev, D.L. Safety and Immunogenicity of a Third Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Case Series. Ann. Intern. Med. 2021, 174, 1330–1332. [Google Scholar] [CrossRef]
- Attolico, I.; Tarantini, F.; Carluccio, P.; Schifone, C.P.; Delia, M.; Gagliardi, V.P.; Perrone, T.; Gaudio, F.; Longo, C.; Giordano, A.; et al. Serological Response Following BNT162b2 Anti-SARS-CoV-2 MRNA Vaccination in Haematopoietic Stem Cell Transplantation Patients. Br. J. Haematol. 2022, 196, 928–931. [Google Scholar] [CrossRef]
- Autore, F.; Stirparo, L.; Innocenti, I.; Papa, E.; Marchesi, F.; Togni, C.; Mariani, S.; Torrieri, L.; Salvatori, M.; Fazio, F.; et al. Immunogenicity of SARS-CoV-2 Vaccination in Patients Undergoing Autologous Stem Cell Transplantation. A Multicentric Experience. Front. Oncol. 2022, 12, 897937. [Google Scholar] [CrossRef]
- Canti, L.; Humblet-Baron, S.; Desombere, I.; Neumann, J.; Pannus, P.; Heyndrickx, L.; Henry, A.; Servais, S.; Willems, E.; Ehx, G.; et al. Predictors of Neutralizing Antibody Response to BNT162b2 Vaccination in Allogeneic Hematopoietic Stem Cell Transplant Recipients. J. Hematol. Oncol. 2021, 14, 174. [Google Scholar] [CrossRef] [PubMed]
- Chevallier, P.; Coste-Burel, M.; Le Bourgeois, A.; Peterlin, P.; Garnier, A.; Béné, M.C.; Imbert, B.; Drumel, T.; Le Gouill, S.; Moreau, P.; et al. Safety and Immunogenicity of a First Dose of SARS-CoV-2 MRNA Vaccine in Allogeneic Hematopoietic Stem-Cells Recipients. EJHaem 2021, 2, 520–524. [Google Scholar] [CrossRef] [PubMed]
- Chiarucci, M.; Paolasini, S.; Isidori, A.; Guiducci, B.; Loscocco, F.; Capalbo, M.; Visani, G. Immunological Response Against SARS-COV-2 After BNT162b2 Vaccine Administration Is Impaired in Allogeneic but Not in Autologous Stem Cell Transplant Recipients. Front. Oncol. 2021, 11, 737300. [Google Scholar] [CrossRef]
- Dhakal, B.; Abedin, S.; Fenske, T.; Chhabra, S.; Ledeboer, N.; Hari, P.; Hamadani, M. Response to SARS-CoV-2 Vaccination in Patients after Hematopoietic Cell Transplantation and CAR T-Cell Therapy. Blood 2021, 138, 1278–1281. [Google Scholar] [CrossRef] [PubMed]
- Mamez, A.C.; Pradier, A.; Giannotti, F.; Petitpas, A.; Urdiola, M.F.; Vu, D.L.; Masouridi-Levrat, S.; Morin, S.; Dantin, C.; Clerc-Renaud, D.; et al. Antibody Responses to SARS-CoV2 Vaccination in Allogeneic Hematopoietic Stem Cell Transplant Recipients. Bone Marrow Transplant. 2021, 56, 3094–3096. [Google Scholar] [CrossRef]
- Matkowska-Kocjan, A.; Owoc-Lempach, J.; Chruszcz, J.; Kuźnik, E.; Szenborn, F.; Jurczenko, L.; Wójcik, M.; Banyś, D.; Szenborn, L.; Ussowicz, M. The COVID-19 MRNA BNT163b2 Vaccine Was Well Tolerated and Highly Immunogenic in Young Adults in Long Follow-Up after Haematopoietic Stem Cell Transplantation. Vaccines 2021, 9, 1209. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Ferreira, V.H.; Kothari, S.; Pasic, I.; Mattsson, J.I.; Kulasingam, V.; Humar, A.; Mah, A.; Delisle, J.S.; Ierullo, M.; et al. Safety and Immunogenicity After a Three-Dose SARS-CoV-2 Vaccine Schedule in Allogeneic Stem Cell Transplant Recipients. Transplant. Cell Ther. 2022, 28, 706.e1–706.e10. [Google Scholar] [CrossRef]
- Le Bourgeois, A.; Coste-Burel, M.; Guillaume, T.; Peterlin, P.; Garnier, A.; Béné, M.C.; Chevallier, P. Safety and Antibody Response After 1 and 2 Doses of BNT162b2 MRNA Vaccine in Recipients of Allogeneic Hematopoietic Stem Cell Transplant. JAMA Netw. Open 2021, 4, e2126344. [Google Scholar] [CrossRef]
- Leclerc, M.; Redjoul, R.; Le Bouter, A.; Beckerich, F.; Robin, C.; Parinet, V.; Pautas, C.; Menouche, D.; Bouledroua, S.; Roy, L.; et al. Determinants of SARS-CoV-2 Waning Immunity in Allogeneic Hematopoietic Stem Cell Transplant Recipients. J. Hematol. Oncol. 2022, 15, 27. [Google Scholar] [CrossRef]
- Piñana, J.L.; López-Corral, L.; Martino, R.; Montoro, J.; Vazquez, L.; Pérez, A.; Martin-Martin, G.; Facal-Malvar, A.; Ferrer, E.; Pascual, M.J.; et al. SARS-CoV-2-Reactive Antibody Detection after SARS-CoV-2 Vaccination in Hematopoietic Stem Cell Transplant Recipients: Prospective Survey from the Spanish Hematopoietic Stem Cell Transplantation and Cell Therapy Group. Am. J. Hematol. 2022, 97, 30–42. [Google Scholar] [CrossRef]
- Ram, R.; Hagin, D.; Kikozashvilli, N.; Freund, T.; Amit, O.; Bar-On, Y.; Beyar-Katz, O.; Shefer, G.; Moshiashvili, M.M.; Karni, C.; et al. Safety and Immunogenicity of the BNT162b2 MRNA COVID-19 Vaccine in Patients after Allogeneic HCT or CD19-Based CART Therapy-A Single-Center Prospective Cohort Study. Transplant. Cell Ther. 2021, 27, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Redjoul, R.; Le Bouter, A.; Beckerich, F.; Fourati, S.; Maury, S. Antibody Response after Second BNT162b2 Dose in Allogeneic HSCT Recipients. Lancet 2021, 398, 298–299. [Google Scholar] [CrossRef] [PubMed]
- Salvini, M.; Maggi, F.; Damonte, C.; Mortara, L.; Bruno, A.; Mora, B.; Brociner, M.; Mattarucchi, R.; Ingrassia, A.; Sirocchi, D.; et al. Immunogenicity of Anti-SARS-CoV-2 Comirnaty Vaccine in Patients with Lymphomas and Myeloma Who Underwent Autologous Stem Cell Transplantation. Bone Marrow Transplant. 2022, 57, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Shem-Tov, N.; Yerushalmi, R.; Danylesko, I.; Litachevsky, V.; Levy, I.; Olmer, L.; Lusitg, Y.; Avigdor, A.; Nagler, A.; Shimoni, A.; et al. Immunogenicity and Safety of the BNT162b2 MRNA COVID-19 Vaccine in Haematopoietic Stem Cell Transplantation Recipients. Br. J. Haematol. 2022, 196, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Tamari, R.; Politikos, I.; Knorr, D.A.; Vardhana, S.A.; Young, J.C.; Marcello, L.A.T.; Doddi, S.; Devlin, S.M.; Ramanathan, L.V.; Pessin, M.S.; et al. Predictors of Humoral Response to SARS-CoV-2 Vaccination after Hematopoietic Cell Transplantation and CAR T-Cell Therapy. Blood Cancer Discov. 2021, 2, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Yakushijin, K.; Funakoshi, Y.; Ohji, G.; Hojo, W.; Sakai, H.; Saeki, M.; Hirakawa, Y.; Matsumoto, S.; Sakai, R.; et al. The Safety and Immunogenicity of the BNT162b2 MRNA COVID-19 Vaccine in Japanese Patients after Allogeneic Stem Cell Transplantation. Vaccines 2022, 10, 158. [Google Scholar] [CrossRef] [PubMed]
- Gagelmann, N.; Passamonti, F.; Wolschke, C.; Massoud, R.; Niederwieser, C.; Adjallé, R.; Mora, B.; Ayuk, F.; Kröger, N. Antibody Response after Vaccination against SARS-CoV-2 in Adults with Hematological Malignancies: A Systematic Review and Meta-Analysis. Haematologica 2022, 107, 1840–1849. [Google Scholar] [CrossRef] [PubMed]
- Cordonnier, C.; Einarsdottir, S.; Cesaro, S.; Di Blasi, R.; Mikulska, M.; Rieger, C.; de Lavallade, H.; Gallo, G.; Lehrnbecher, T.; Engelhard, D.; et al. Vaccination of Haemopoietic Stem Cell Transplant Recipients: Guidelines of the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis 2019, 19, e200–e212. [Google Scholar] [CrossRef] [PubMed]
- Montague, B.T.; Wipperman, M.F.; Chio, E.; Crow, R.; Hooper, A.T.; O’Brien, M.P.; Simões, E.A.F. Elevated Serum IgA Following Vaccination against SARS-CoV-2 in a Cohort of High-Risk First Responders. Sci. Rep. 2022, 12, 14932. [Google Scholar] [CrossRef]
- Luis Piñana, J.; Vazquez, L.; Calabuig, M.; López-Corral, L.; Martin-Martin, G.; Villalon, L.; Sanz-Linares, G.; Conesa-Garcia, V.; Sanchez-Salinas, A.; Gago, B.; et al. One-Year Breakthrough SARS-CoV-2 Infection and Correlates of Protection in Fully Vaccinated Hematological Patients. Blood Cancer J. 2023, 13, 8. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).