

Advances in 3D-Printed Implants for Facial Plastic Surgery


Abstract
1. Introduction
1.1. Challenges in Facial Reconstruction
1.2. Objectives of the Review
- Review the development and impact of 3D-printed implants in facial reconstruction.
- Evaluate the materials currently used for 3D-printed facial implants.
- Discuss CAD-based customization and virtual surgical planning (VSP).
- Explore the clinical applications, advantages, and limitations of 3D printing in reconstructive surgery.
- Highlight future trends, including bioprinting and smart implant systems.
1.3. Methods
- Thin-slice CT or MRI scanning of the defect site.
- Digital segmentation and 3D reconstruction using CAD software (e.g., Mimics, Geomagic).
- Virtual surgical planning (VSP) to simulate the procedure and finalize implant design.
- Material selection based on the surgical indication (e.g., titanium for load-bearing, PEEK for aesthetic).
- 3D printing via SLS or SLA techniques, followed by sterilization and quality checks.
- Approximate production time ranges from 7–10 days, depending on complexity.
1.4. Search Strategy
1.5. Inclusion Criteria
- Peer-reviewed articles from the last 20 years.
- Studies on clinical outcomes, materials, or integration of implants.
- English-language publications.
1.6. Exclusion Criteria
- Articles lacking clinical validation.
- Non-English sources.
- Case reports with small sample sizes.
1.7. Data Extraction and Analysis
2. Evolution of 3D-Printed Implants in Facial Reconstruction
Key Milestones in the Development of 3D-Printed Facial Implants
- 1998: Implementation of the first CAD-designed titanium cranioplasty [7].
- 2011: FDA approval of the first 3D-printed titanium implant for mandibular reconstruction [8].
- 2020s: Emergence of smart implants and bioprinting, offering real-time monitoring capabilities and tissue regeneration potential [9].
3. Types of 3D-Printed Materials for Facial Implants
3.1. Titanium and Titanium Alloys
3.2. Polyetheretherketone (PEEK)
3.3. Biodegradable and Bioactive Materials
3.4. Hybrid and Composite Materials
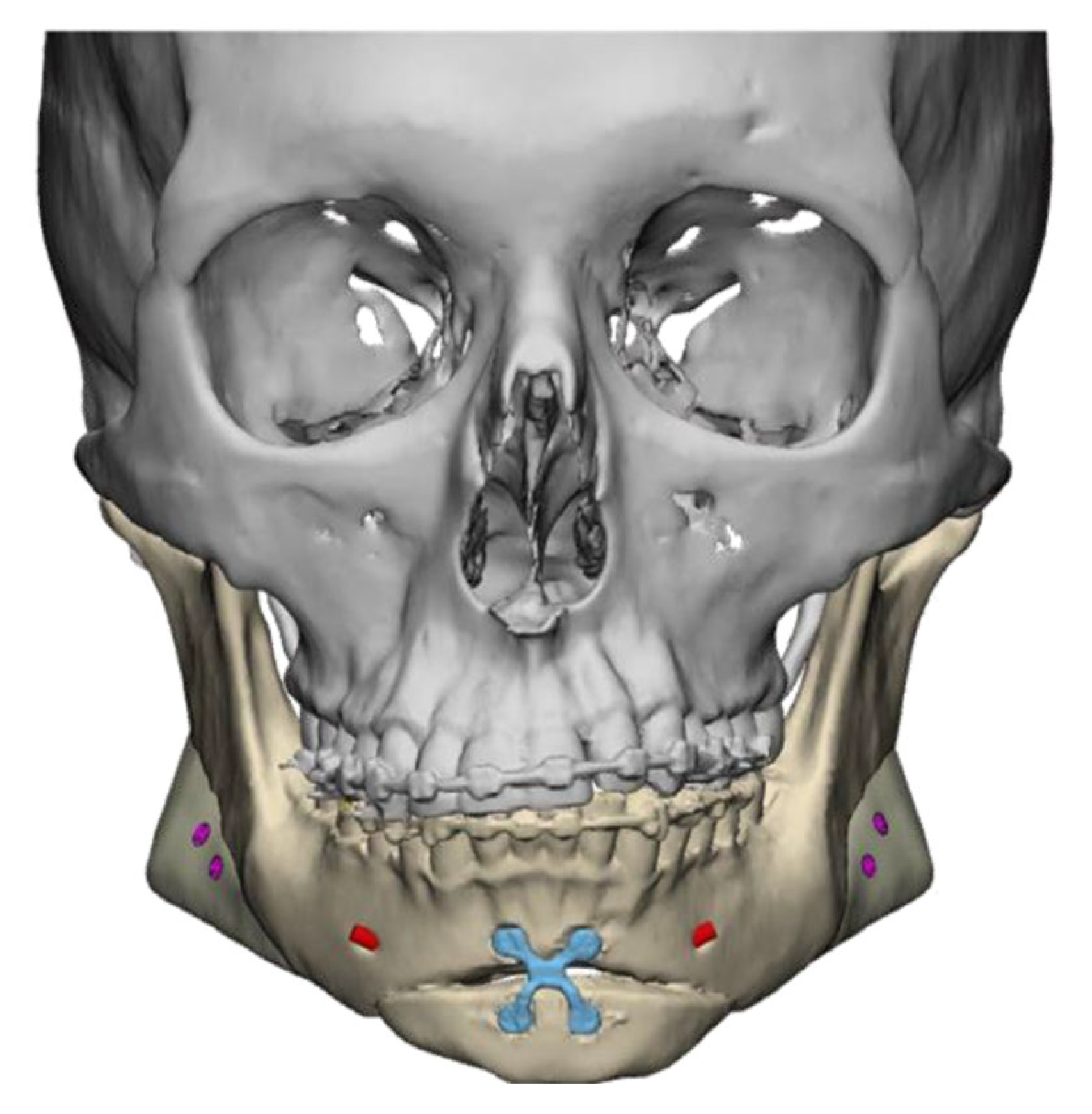
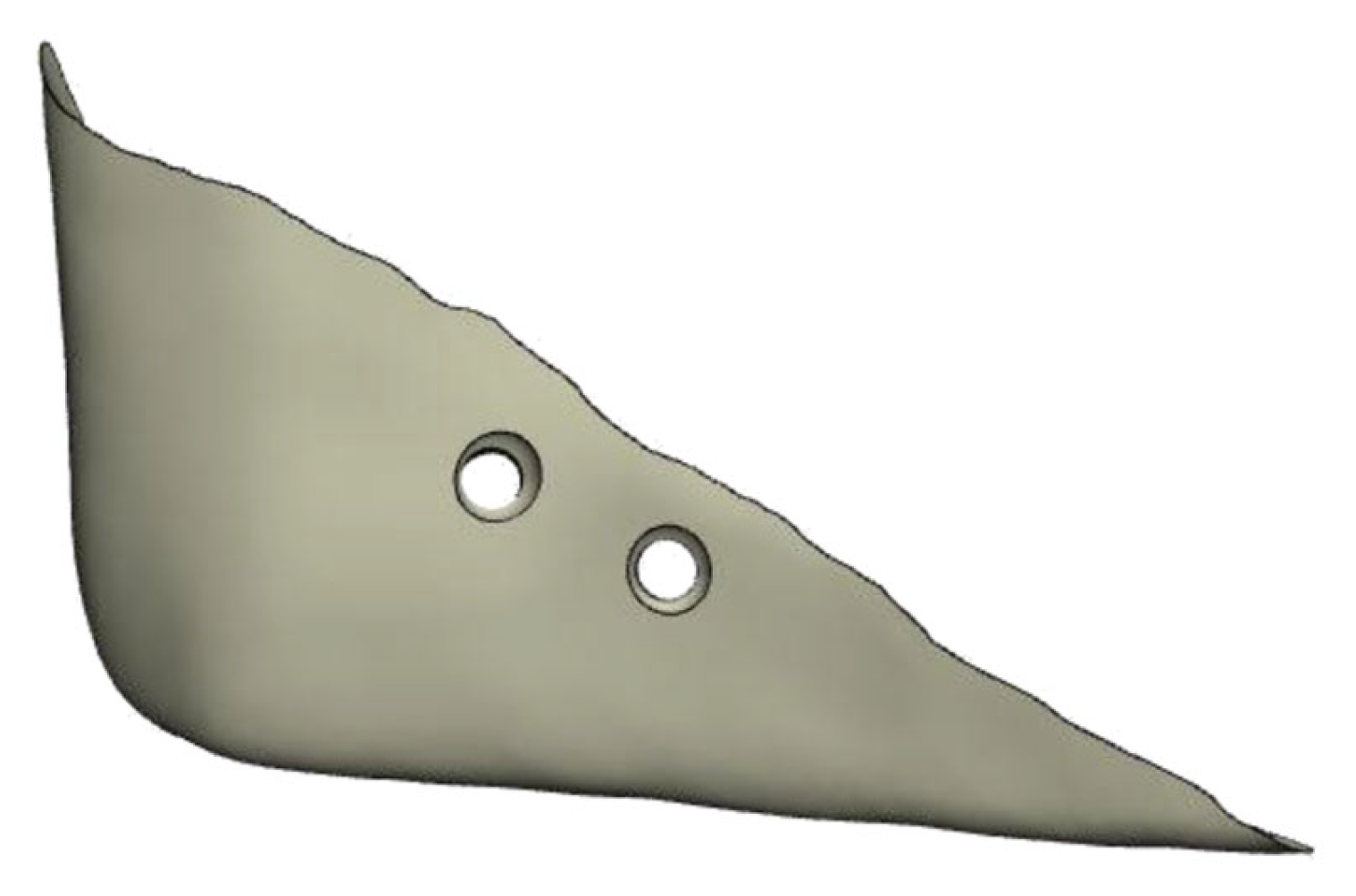
3.5. Customization and Computer-Assisted Design (CAD)
- Indications: PSIs are particularly valuable in cases of complex trauma, oncologic resections, craniofacial syndromes, and aesthetic surgeries requiring high-precision symmetry.
- Preoperative protocol: All patients undergo thin-slice CT imaging. The data are imported into CAD software (e.g., Mimics, Geomagic). Virtual surgical planning (VSP) is conducted collaboratively with the engineering team.
- Material selection:
- ◦
- Titanium: preferred for load-bearing reconstructions (mandible, orbit) in trauma/oncology.
- ◦
- PEEK: selected in aesthetic and revision surgeries due to its flexibility and radiolucency.
- ◦
- Bioresorbables: used in pediatric cases to avoid long-term revision.
- Surgical tips:
- ◦
- Ensure a tight subperiosteal pocket to avoid implant displacement.
- ◦
- Combine implants with soft tissue augmentation (fat grafting) in elderly patients.
- ◦
- Use antibiotic-impregnated coatings or postoperative irrigation for high-infection-risk sites.
- ◦
- Always rehearse placement with a printed biomodel during the planning phase.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material Type | Clinical Indication | Key Advantages | Limitations |
|---|---|---|---|
| Titanium | Trauma, oncologic, load-bearing zones | High strength, osseointegration, durable | Stress shielding, thermal conductivity |
| PEEK | Aesthetic, revision, cranial applications | Radiolucent, bone-like elasticity, biocompatible | Limited osseointegration, costly surface treatment |
| Bioresorbable polymers | Pediatric, regenerative scaffold support | Resorbable, avoids second surgery, tissue growth | Variable degradation, weaker mechanical strength |
| Hybrid/Composite | High-risk infection or osseointegration zones | Combines strength with bioactivity, drug delivery | Complex fabrication, less clinical data |
4. Surgical Applications of 3D-Printed Implants
5. Challenges and Limitations of 3D-Printed Facial Implants
6. Emerging Innovations in 3D-Printed Implants
7. Results
7.1. Reduced Surgical Time and Improved Accuracy
7.2. Advancements in Materials
7.3. Enhanced Patient Outcomes
7.4. Remaining Limitations
- High production and implementation costs.
- Regulatory delays for newer materials and implant types.
- Limited availability in low-resource environments.
8. Conclusions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Oliver, J.D.; Banuelos, J.; Abu-Ghname, A.; Vyas, K.S.; Sharaf, B. Alloplastic cranioplasty reconstruction: A systematic review comparing outcomes with titanium mesh, polymethyl methacrylate, polyether ether ketone, and norian implants in 3591 adult patients. Ann. Plast. Surg. 2019, 82, S289–S294. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.S.; Lal, B.; Bhagat, A.C.; Alagarsamy, R. Medical Imaging for Patient-Specific Implants. In Biomedical Implants; CRC Press: Boca Raton, FL, USA, 2024; pp. 39–60. [Google Scholar]
- Kafle, A.; Luis, E.; Silwal, R.; Pan, H.M.; Shrestha, P.L.; Bastola, A.K. 3D/4D printing of polymers: Fused deposition modelling (FDM), selective laser sintering (SLS), and stereolithography (SLA). Polymers 2021, 13, 3101. [Google Scholar] [CrossRef] [PubMed]
- Wellisz, T. Clinical experience with the Medpor porous polyethylene implant. Aesthetic Plast. Surg. 1993, 17, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A.F.; Yaakob, H.; Khalil, A.; Georges, P. Evaluating patients’ satisfaction level after using 3D printed PEEK facial implants in repairing maxillofacial deformities. Ann. Med. Surg. 2022, 79, 104095. [Google Scholar] [CrossRef]
- Panayotov, I.V.; Orti, V.; Cuisinier, F.; Yachouh, J. Polyetheretherketone (PEEK) for medical applications. J. Mater. Sci. Mater. Med. 2016, 27, 118. [Google Scholar] [CrossRef] [PubMed]
- Capitelli-McMahon, H.; Kahlar, N.; Rahman, S. Titanium Versus Autologous Bone-Based Cranioplasty: A Systematic Review and Meta-Analysis. Cureus 2023, 15, e39516. [Google Scholar] [CrossRef]
- Ziyad, H. 3D printed titanium implants: Colossal FDA-approved leap towards “personalized” maxillo-facial surgery. J. Oral Res. 2017, 6, 282–284. [Google Scholar] [CrossRef]
- Qu, G.; Huang, J.; Gu, G.; Li, Z.; Wu, X.; Ren, J. Smart implants: 4D-printed shape-morphing scaffolds for medical implantation. Int. J. Bioprint. 2023, 9, 764. [Google Scholar] [CrossRef]
- Lim, H.K.; Choi, Y.J.; Choi, W.C.; Song, I.S.; Lee, U.L. Reconstruction of maxillofacial bone defects using patient-specific long-lasting titanium implants. Sci. Rep. 2022, 12, 7538. [Google Scholar] [CrossRef]
- Girones Molera, J.; Mendez, J.A.; San Roman, J. Bioresorbable and nonresorbable polymers for bone tissue engineering. Curr. Pharm. Des. 2012, 18, 2536–2557. [Google Scholar] [CrossRef]
- Li, J.; Yuan, H.; Chandrakar, A.; Moroni, L.; Habibovic, P. 3D porous Ti6Al4V-beta-tricalcium phosphate scaffolds directly fabricated by additive manufacturing. Acta Biomater. 2021, 126, 496–510. [Google Scholar] [CrossRef] [PubMed]
- Domsta, V.; Seidlitz, A. 3D-Printing of Drug-Eluting Implants: An Overview of the Current Developments Described in the Literature. Molecules 2021, 26, 4066. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kernen, F.; Kramer, J.; Wanner, L.; Wismeijer, D.; Nelson, K.; Flügge, T. A review of virtual planning software for guided implant surgery—Data import and visualization, drill guide design and manufacturing. BMC Oral Health 2020, 20, 251. [Google Scholar] [CrossRef] [PubMed]
- Järvinen, S.; Suojanen, J.; Kormi, E.; Wilkman, T.; Kiukkonen, A.; Leikola, J.; Stoor, P. The use of patient specific polyetheretherketone implants for reconstruction of maxillofacial deformities. J. Craniomaxillofac. Surg. 2019, 47, 1072–1076. [Google Scholar] [CrossRef]
- Teal, L.N.; Day, K.M. Virtual Surgical Planning in Craniofacial Surgery. J. Craniofacial Surg. 2019, 30, 2459–2463. [Google Scholar] [CrossRef]
- Singh, S.; Nyberg, E.L.; O’Sullivan, A.N.; Farris, A.; Rindone, A.N.; Zhang, N.; Whitehead, E.C.; Zhou, Y.; Mihaly, E.; Achebe, C.C.; et al. Point-of-care treatment of geometrically complex midfacial critical-sized bone defects with 3D-Printed scaffolds and autologous stromal vascular fraction. Biomaterials 2022, 282, 121392. [Google Scholar] [CrossRef]
- Abebayehu, D.; Spence, A.J.; McClure, M.J.; Haque, T.T.; Rivera, K.O.; Ryan, J.J. Polymer scaffold architecture is a key determinant in mast cell inflammatory and angiogenic responses. J. Biomed. Mater. Res. Part A 2019, 107, 884–892. [Google Scholar] [CrossRef]
- Bär, F.; Berger, L.; Jauer, L.; Kurtuldu, G.; Schäublin, R.; Schleifenbaum, J.H.; Löffler, J.F. Laser additive manufacturing of biodegradable magnesium alloy WE43: A detailed microstructure analysis. Acta Biomater. 2019, 98, 36–49. [Google Scholar] [CrossRef]
- Zhang, M.; Gregory, T.; Hansen, U.; Cheng, C.K. Effect of stress-shielding-induced bone resorption on glenoid loosening in reverse total shoulder arthroplasty. J. Orthop. Res. 2020, 38, 1566–1574. [Google Scholar] [CrossRef]
- Xie, K.; Guo, Y.; Zhao, S.; Wang, L.; Wu, J.; Tan, J.; Yang, Y.; Wu, W.; Jiang, W.; Hao, Y. Partially Melted Ti6Al4V Particles Increase Bacterial Adhesion and Inhibit Osteogenic Activity on 3D-printed Implants: An In Vitro Study. Clin. Orthop. Relat. Res. 2019, 477, 2772–2782. [Google Scholar] [CrossRef]
- Chouirfa, H.; Bouloussa, H.; Migonney, V.; Falentin-Daudré, C. Review of titanium surface modification techniques and coatings for antibacterial applications. Acta Biomater. 2019, 83, 37–54. [Google Scholar] [CrossRef] [PubMed]
- Swift, A.; Liew, S.; Weinkle, S.; Garcia, J.K.; Silberberg, M.B. The Facial Aging Process From the “Inside Out”. Aesthetic Surg. J. 2021, 41, 1107–1119. [Google Scholar] [CrossRef] [PubMed]
- Groen, J.W.; Krastev, T.K.; Hommes, J.; Wilschut, J.A.; Ritt, M.J.P.F.; van der Hulst, R.R.J.W. Autologous Fat Transfer for Facial Rejuvenation: A Systematic Review on Technique, Efficacy, and Satisfaction. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1606. [Google Scholar] [CrossRef] [PubMed]
- Naomi, C. Paxton, Kevin Tetsworth, Maria A. Woodruff, Chapter 33—Personalization for surgical implants. In Digital Human Modeling and Medicine; Paul, G., Doweidar, M.H., Eds.; Academic Press: Cambridge, MA, USA, 2023; pp. 849–874. ISBN 9780128239131. [Google Scholar]
- Baptista, L.S.; Kronemberger, G.S.; Silva, K.R.; Granjeiro, J.M. Spheroids of stem cells as endochondral templates for improved bone engineering. Front. Biosci. 2018, 23, 1969–1986. [Google Scholar] [CrossRef]
- Douglas, A.; Chen, Y.; Elloso, M.; Levschuk, A.; Jeschke, M.G. Bioprinting-By-Design of Hydrogel-Based Biomaterials for In Situ Skin Tissue Engineering. Gels 2025, 11, 110. [Google Scholar] [CrossRef]
- Mahapatra, C.; Kumar, P.; Paul, M.K.; Kumar, A. Angiogenic stimulation strategies in bone tissue regeneration. Tissue Cell 2022, 79, 101908. [Google Scholar] [CrossRef]
- Yang, H.; Ding, H.; Tian, Y.; Wu, C.; Chen, Y.; Shi, H.; Chan, Y.K.; Deng, Y.; Liao, L.; Lai, S. Metal element-fusion peptide heterostructured nanocoatings endow polyetheretherketone implants with robust anti-bacterial activities and in vivo osseointegration. Nanoscale 2024, 16, 12934–12946. [Google Scholar] [CrossRef]
- Zekiy, A.O.; Makurdumyan, D.A.; Matveeva, E.A.; Bogatov, E.A.; Kaliiants, T.V. Antiseptic sealant and a nanocoated implant-abutment interface improve the results of dental implantation. Clin. Implant. Dent. Relat. Res. 2019, 21, 938–945. [Google Scholar] [CrossRef]
- Xu, T.; Chen, Z.; Chen, Z.; Fan, Y.; Mao, H. Development of the Biomaterials Technology for the Infection Resistance. Curr. Pharm. Des. 2018, 24, 886–895. [Google Scholar] [CrossRef]
- López-Valverde, N.; Aragoneses, J.; Rodríguez, C.; Aragoneses, J.M. Effect on osseointegration of dental implants treated with carboxyethylphosphonic acid and functionalized with BMP-2: Preliminary study on a minipig model. Front. Bioeng. Biotechnol. 2023, 11, 1244667. [Google Scholar] [CrossRef]





| Parameter | Patient-Specific Implants (PSIs) | Traditional Methods (Mesh/Grafts) |
|---|---|---|
| Anatomical accuracy | High (custom fit) | Moderate (manual contouring) |
| Operative time | Reduced (pre-fitted) | Longer (intraoperative shaping) |
| Aesthetic outcomes | High symmetry, predictable contours | Variable, surgeon-dependent |
| Risk of donor site morbidity | None | Present (for autografts) |
| Infection risk | Moderate (mitigated with coatings) | Variable |
| Cost | High upfront, cost-effective long-term | Lower upfront, higher revision risk |
| Reimbursement | Limited (cosmetic cases) | More common (trauma/functional) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Birbe Foraster, J. Advances in 3D-Printed Implants for Facial Plastic Surgery. Surg. Tech. Dev. 2025, 14, 22. https://doi.org/10.3390/std14030022
Birbe Foraster J. Advances in 3D-Printed Implants for Facial Plastic Surgery. Surgical Techniques Development. 2025; 14(3):22. https://doi.org/10.3390/std14030022
Chicago/Turabian StyleBirbe Foraster, Joan. 2025. "Advances in 3D-Printed Implants for Facial Plastic Surgery" Surgical Techniques Development 14, no. 3: 22. https://doi.org/10.3390/std14030022
APA StyleBirbe Foraster, J. (2025). Advances in 3D-Printed Implants for Facial Plastic Surgery. Surgical Techniques Development, 14(3), 22. https://doi.org/10.3390/std14030022