



Hearing Results after Transmastoid Superior Semicircular Canal Plugging for Superior Semicircular Canal Dehiscence: A Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods

| Author, Year | Type of Study | Ears | Patients | Mean Age (SD) | Male/ Female | Mean Follow-Up Time | Frequency (kHz) | Mean AC pre-OP (SD) | Mean AC post-OP (SD) | Mean BC pre-OP (SD) | Mean BC post-OP (SD) | Mean ABG pre-OP (SD) | Mean ABG post-OP (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ellsperman S.E. et al., 2021 [19] | Retrospective | 26 | 26 | 55 (10.2) | 8/18 | 20 | 0.5, 1, 2, 4 | 28.1 (19.6) | 26.9 (13.3) | 17.9 (16.5) | 17.4 (12.9) | 22.8 (11.1) | 18.7 (9.6) |
| Kawamura Y. et al., 2022 [15] | Retrospective | 7 | 7 | 53.3 (13.7) | 2/5 | 12.3 | 0.5, 1, 2, 4 | 20.5 (10.6) | 20.4 (7.7) | 15 (9.1) | 18.8 (9.9) | 8 (6.4) | 3 (5.3) |
| Gersdorff G. et al., 2022 [20] | Retrospective | 30 * | 27 | 52 (10.6) | 11/16 | 19 | 0.25, 0.5, 1, 2, 3, 4 | 31.85 (33.3) | 29.2 (37.1) | 14.5 (23.88) | 21.5 (25.5) | 15.6 (15.5) | 10 (11.8) |
| Lin K.F. et al., 2021 [21] | Retrospective | 29 | 29 | 51.2 (NA) | NA | 16.4 | 0.5, 1, 2, 3 | 25.6 (18.9) | 29.5 (20) | 17.5 (16) | 22.3 (18.4) | 8.1 (6.4) | 7.2 (7) |
| Nieto P. et al., 2021 [22] | Retrospective | 9 | 9 | 52.7 (10) | 3/6 | 9 | 0.5, 1, 2, 4 | 23.6 (15.7) | 26.4 (14) | 15 (13.4) | 16.9 (12.6) | NA | NA |
| Stultiens J.J.A. et al., 2022 [23] | Prospective | 4 | 4 | 51.5 (6.4) | 3/1 | 2 | 1, 2, 4 | 35 (21.8) | 38 (20.3) | 31.75 (19.6) | 33.25 (20.5) | 3.25 (2.8) | 4.75 (1.9) |
| Somers T. et al., 2014 [24] | Retrospective | 11 * | 10 | 51.5 (14.1) | 5/6 | 7.5 | 0.5, 1, 2, 4 | 31.6 (26.7) | 40.3 (25.5) | 14.8 (19.1) | 19.6 (20.6) | 23.4 (14.9) | 20 (14.9) |
| Van Haesendonck G. et al., 2016 [25] | Retrospective | 13 * | 12 | 51.5 (5.7) | 6/7 | 5.6 | 0.5, 1, 2, 4 | 24.3 (12.8) | 19.8 (9.5) | 13 (9.4) | 15.1 (7.1) | 12.9 (9.1) | 5 (4.7) |
| Deschenes G.R. et al., 2009 [26] | Retrospective | 3 * | 2 | 44.5 (5.5) | 2/1 | 3.5 | 0.5, 1, 2, 4 | 18.3 (1.1) | 10 (4.6) | 10 (0.6) | 10.4 (5.2) | 9.1 (0.6) | 13.85 (8.83) |
| Morrison M. et al., 2022 + 2 Insel cases [27] | Retrospektive | 3 | 3 | 53 | 2/1 | 2.8 | 0.5, 1, 2, 4 | 42 (7.6) | 39.1 (2.1) | 20 (3) | 27.4 (4) | 15.8 (10.9) | 12.5 (6.7) |
| Shaul C. et al., 2023 [28] | Retrospective | 24 * | 23 | 54 | 8/15 | 12 | 0.5, 1, 2 | 26.4 (16) | 26.5 (19) | 13.7 (17) | 20.5 (18) | 12.7 (8) | 5.9 (6) |
| Cocca S. et al., 2022 ** [29] | Case report | 1 | 1 | 34 | 0/1 | 2 | 0.5, 1, 2, 4 | 50 | 27.5 | 23.75 | 22.5 | 21.3 | 5 |
| Dang, P.T. et al., 2014 ** [30] | Case report | 1 | 1 | 52 | 1/0 | 9 | 0.5, 1, 2, 4 | 41.25 | 27.5 | 33.75 | 23.75 | 7.5 | 3.75 |
| Kirtane M.V. et al., 2009 ** [31] | Case report | 1 | 1 | 37 | 1/0 | 2 | 0.5, 1, 2, 4 | 31.25 | 38.75 | 6.25 | 22.5 | 12.5 | 11.3 |
| Wijaya C. et al., 2012 ** [32] | Case report | 1 | 1 | 48 | 1/0 | 6 | 0.5, 1, 2, 4 | 63.75 | 73.75 | 45 | 67.5 | 17.5 | 7.5 |
| McCall A.A. et al., 2011 ** [33] | Case report | 1 | 1 | 15 | 0/1 | 12 | 0.5, 1, 2, 4 | 5 | 2.5 | −1.25 | 0 | 6.3 | 2.5 |
| Total *** | 11 studies | 159 | 152 | 52.6 (10.2) | 50/76 | 14.1 | 25.1 (11) | 22.2 (10.5) | 15.3 (11.2) | 18.8 (12.1) | 11.5 (10.2) | 8.4 (8.6) |
| Preoperative | Postoperative | |||||||
|---|---|---|---|---|---|---|---|---|
| Study | Aural Fullness | Autophony | Tinnitus | Hyperacusis | Aural Fullness | Autophony | Tinnitus | Hyperacusis |
| Ellsperman S.E. et al., 2021 [19] | NA | NA | NA | NA | NA | NA | NA | NA |
| Kawamura Y. et al., 2022 [15] | 4 | 6 | 2 | 5 | 0 | 0 | 0 | NA |
| Gersdorff G. et al., 2022 [20] | 19 | 29 | 18 | 9 | 1 | 1 | 7 | 0 |
| Lin K.F. et al., 2021 [21] | NA | NA | NA | NA | NA | NA | NA | NA |
| Nieto P. et al., 2021 [22] | 5 | 7 | 6 | NA | 1 | 0 | 1 | NA |
| Stultiens J.J.A. et al., 2022 [23] | NA | 4 | 4 | NA | NA | 0 | NA | NA |
| Somers T. et al., 2014 [24] | NA | 9 | 2 | 2 | NA | 0 | 2 | 0 |
| Van Haesendonck G. et al., 2016 [25] | NA | 1 | 9 | 8 | NA | 1 | 3 | 2 |
| Deschenes G.R. et al., 2009 [26] | NA | 1 | 1 | NA | NA | NA | NA | NA |
| Morrison M. et al., 2022 + 2 Insel cases [27] | 1 | 2 | 2 | 2 | 0 | 0 | 2 | 0 |
| Shaul C. et al., 2023 [28] | 9 | 18 | 16 | 4 | 1 | 1 | 3 | 1 |
| Cocca S. et al., 2022 [29] | 1 | 1 | NA | 1 | 1 | 0 | 1 | 1 |
| Dang, P.T. et al., 2014 [30] | NA | 1 | NA | NA | NA | 0 | NA | NA |
| Kirtane M.V. et al., 2009 [31] | 1 | NA | 1 | NA | 0 | NA | NA | NA |
| Wijaya C. et al., 2012 [32] | 0 | NA | 0 | NA | 0 | NA | 0 | NA |
| Total (rate of patients with remaining symptoms) | 41 | 79 | 62 | 31 | 4 (9.7%) | 3 (3.7%) | 19 (30%) | 4 (12.9%) |
| Preoperative | Postoperative | |||||
|---|---|---|---|---|---|---|
| Study | Tullio Sign | Hennebert Sign | Oscillopsia | Tullio Sign | Hennebert Sign | Oscillopsia |
| Ellsperman S.E. et al., 2021 [19] | NA | NA | NA | NA | NA | NA |
| Kawamura Y. et al., 2022 [15] | 2 | 1 | NA | NA | 0 | NA |
| Gersdorff G. et al., 2022 [20] | 19 | NA | 11 | 2 | NA | 2 |
| Lin K.F. et al., 2021 [21] | NA | NA | NA | NA | NA | NA |
| Nieto P. et al., 2021 [22] | 0 | 4 | 6 | NA | 0 | 1 |
| Stultiens J.J.A. et al., 2022 [23] | NA | NA | NA | NA | NA | NA |
| Somers T. et al., 2014 [24] | 3 | NA | 1 | 0 | NA | 0 |
| Van Haesendonck G. et al., 2016 [25] | 5 | NA | NA | 1 | NA | NA |
| Deschenes G.R. et al., 2009 [26] | 1 | 1 | NA | 0 | 0 | NA |
| Morrison M. et al., 2022 + 2 Insel cases [27] | 2 | 1 | 1 | 0 | 0 | 0 |
| Shaul C. et al., 2023 [28] | 15 | NA | 4 | 0 | NA | 0 |
| Cocca S. et al., 2022 [29] | 0 | 1 | NA | NA | 0 | NA |
| Dang, P.T. et al., 2014 [30] | 1 | 1 | 1 | 0 | 0 | 0 |
| Kirtane M.V. et al., 2009 [31] | NA | 1 | NA | NA | 0 | NA |
| Wijaya C. et al., 2012 [32] | 0 | 1 | NA | 0 | 0 | NA |
| Total (rate of patients with remaining symptoms) | 48 | 11 | 24 | 3 (6%) | 0 (0%) | 3 (12.5%) |
3. Results
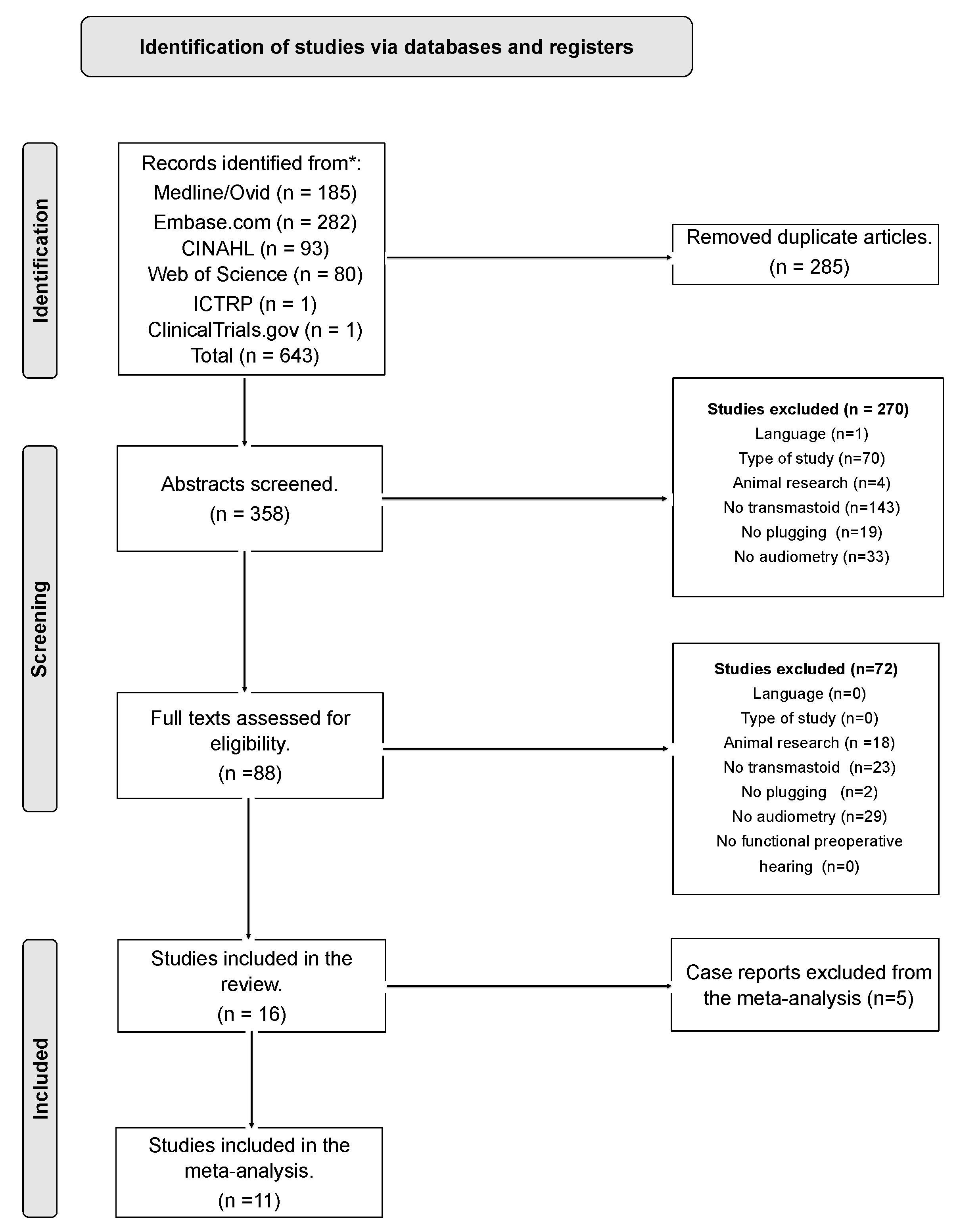
3.1. Search Results and Study Selection
3.2. Characteristics of Patients
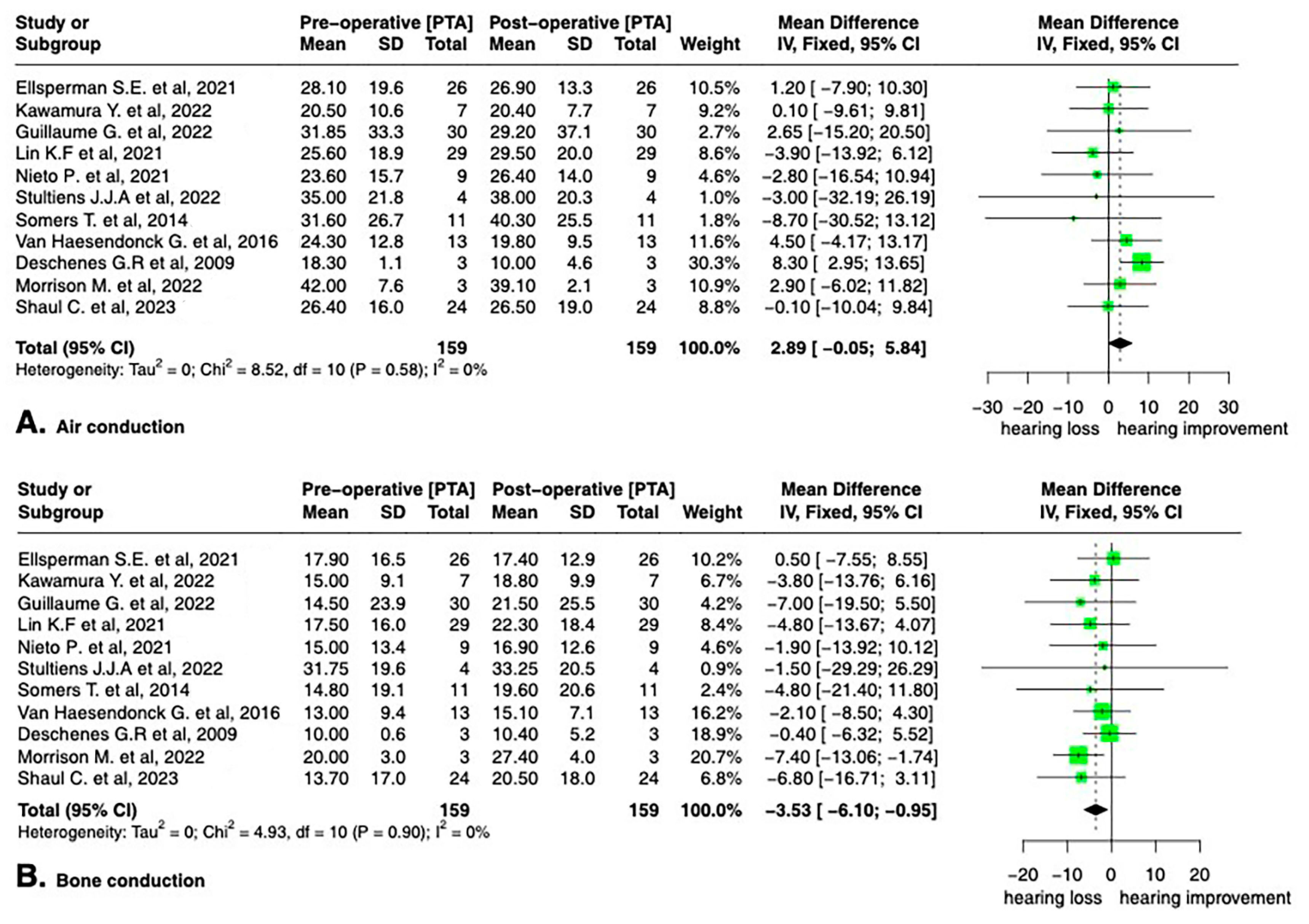
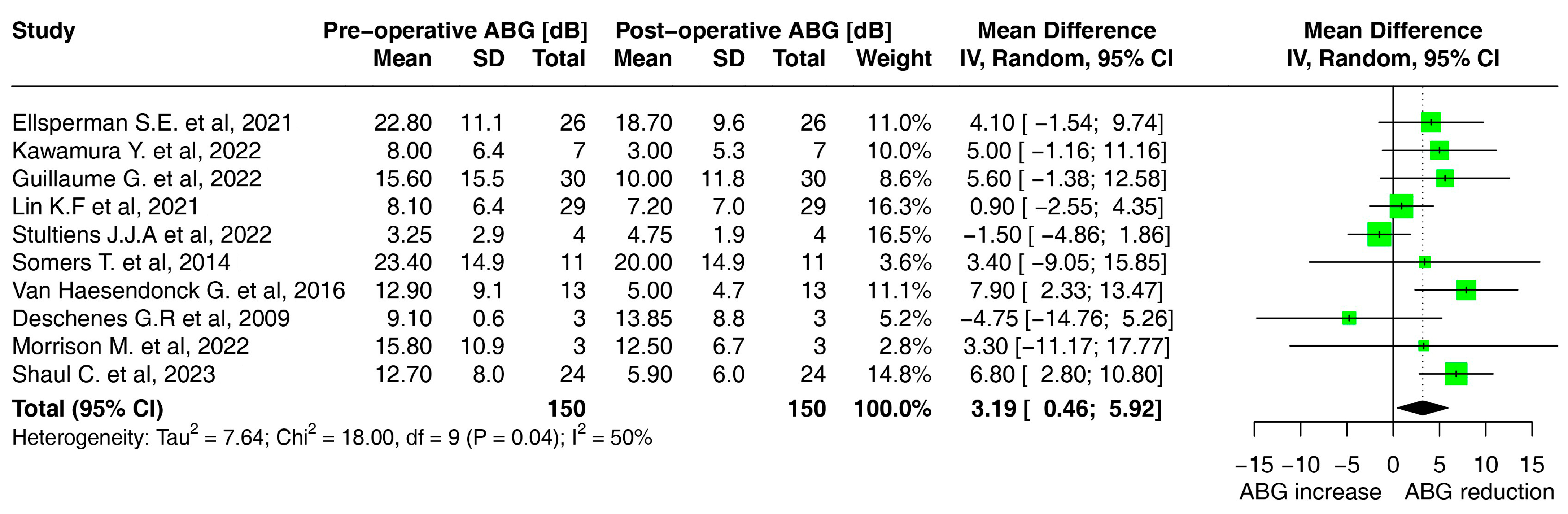
3.3. Hearing Outcomes
3.4. Clinical Symptoms before and after Surgery
3.5. Surgical Complications
4. Consecutive Case Series
5. Discussion
5.1. Hearing Preservation after Plugging
5.2. Symptoms Resolution
5.3. Surgical Approach and Complications
5.4. Limitations
5.5. Future Implications
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ward, B.K.; van de Berg, R.; van Rompaey, V.; Bisdorff, A.; Hullar, T.E.; Welgampola, M.S.; Carey, J.P. Superior Semicircular Canal Dehiscence Syndrome: Diagnostic Criteria Consensus Document of the Committee for the Classification of Vestibular Disorders of the Bárány Society. J. Vestib. Res. Equilib. Orientat. 2021, 31, 131–141. [Google Scholar] [CrossRef]
- Minor, L.B.; Solomon, D.; Zinreich, J.S.; Zee, D.S. Sound- and/or Pressure-Induced Vertigo Due to Bone Dehiscence of the Superior Semicircular Canal. Arch. Otolaryngol.—Head Neck Surg. 1998, 124, 249–258. [Google Scholar] [CrossRef]
- Minor, L.B. Clinical Manifestations of Superior Semicircular Canal Dehiscence. Laryngoscope 2005, 115, 1717–1727. [Google Scholar] [CrossRef] [PubMed]
- Ziylan, F.; Kinaci, A.; Beynon, A.J.; Kunst, H.P.M. A Comparison of Surgical Treatments for Superior Semicircular Canal Dehiscence: A Systematic Review. Otol. Neurotol. 2017, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ward, B.K.; Carey, J.P.; Minor, L.B. Superior Canal Dehiscence Syndrome: Lessons from the First 20 Years. Front. Neurol. 2017, 8, 177. [Google Scholar] [CrossRef]
- Steenerson, K.K.; Crane, B.T.; Minor, L.B. Superior Semicircular Canal Dehiscence Syndrome. Semin. Neurol. 2020, 40, 151–159. [Google Scholar] [CrossRef]
- Schmuziger, N.; Allum, J.; Buitrago-Téllez, C.; Probst, R. Incapacitating Hypersensitivity to One’s Own Body Sounds Due to a Dehiscence of Bone Overlying the Superior Semicircular Canal. A Case Report. Eur. Arch. Oto-Rhino-Laryngol. 2006, 263, 69–74. [Google Scholar] [CrossRef]
- Minor, L.B.; Carey, J.P.; Cremer, P.D.; Lustig, L.R.; Streubel, S.-O.; Ruckenstein, M.J. Dehiscence of Bone Overlying the Superior Canal as a Cause of Apparent Conductive Hearing Loss. Otol. Neurotol. 2003, 24, 270–278. [Google Scholar] [CrossRef]
- Watson, S.R.; Halmagyi, G.M.; Colebatch, J.G. Vestibular Hypersensitivity to Sound (Tullio Phenomenon). Neurology 2000, 54, 722–728. [Google Scholar] [CrossRef]
- Vlastarakos, P.V.; Proikas, K.; Tavoulari, E.; Kikidis, D.; Maragoudakis, P.; Nikolopoulos, T.P. Efficacy Assessment and Complications of Surgical Management for Superior Semicircular Canal Dehiscence: A Meta-Analysis of Published Interventional Studies. Eur. Arch. Oto-Rhino-Laryngol. 2009, 266, 177–186. [Google Scholar] [CrossRef]
- Mueller, S.A.; Vibert, D.; Haeusler, R.; Raabe, A.; Caversaccio, M. Surgical Capping of Superior Semicircular Canal Dehiscence. Eur. Arch. Oto-Rhino-Laryngol. 2013, 271, 1369–1374. [Google Scholar] [CrossRef]
- Agrawal, S.K.; Parnes, L.S. Transmastoid Superior Semicircular Canal Occlusion. Otol. Neurotol. 2008, 29, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, D.; Yamazaki, M.; Ohta, J.; Kadowaki, S.; Nomura, K.; Hidaka, H.; Oshima, T.; Kawase, T.; Katori, Y. Closure Technique for Labyrinthine Fistula by ‘Underwater’ Endoscopic Ear Surgery. Laryngoscope 2014, 124, 2616–2618. [Google Scholar] [CrossRef]
- Creighton, F.X.J.; Zhang, L.; Ward, B.; Carey, J.P. Hearing Outcomes for an Underwater Endoscopic Technique for Transmastoid Repair of Superior Semicircular Canal Dehiscence. Otol. Neurotol. 2021, 42, E1691–E1697. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, Y.; Yamauchi, D.; Kobayashi, T.; Ikeda, R.; Kawase, T.; Katori, Y. Hearing Outcomes of Transmastoid Plugging for Superior Canal Dehiscence Syndrome by Underwater Endoscopic Surgery: With Special Reference to Transient Bone Conduction Increase in Early Postoperative Period. Otol. Neurotol. 2022, 43, 368–375. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Ellsperman, S.E.; Telian, S.A.; Kileny, P.R.; Welch, C.M. Auditory Outcomes Following Transmastoid and Middle Cranial Fossa Approaches for Superior Semicircular Canal Dehiscence Repair. Otol. Neurotol. 2021, 42, 1544–1552. [Google Scholar] [CrossRef]
- Gersdorff, G.; Blaivie, C.; de Foer, B.; Deggouj, N.; Wyckmans, F.; Somers, T. Evaluation of the Transmastoid Plugging Approach for Superior Semicircular Canal Dehiscences: A Retrospective Series of 30 Ears. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 4861–4869. [Google Scholar] [CrossRef]
- Lin, K.F.; Bojrab, D.I.I.; Fritz, C.G.; Vandieren, A.; Babu, S.C. Hearing Outcomes After Surgical Manipulation of the Membranous Labyrinth During Superior Semicircular Canal Dehiscence Plugging or Posterior Semicircular Canal Occlusion. Otol. Neurotol. 2021, 42, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Nieto, P.; Gallois, Y.; Molinier, C.; Deguine, O.; Marx, M. Surgical Treatments of Superior Semicircular Canal Dehiscence: A Single-Centre Experience in 63 Cases. Laryngoscope Investig. Otolaryngol. 2021, 6, 1414–1420. [Google Scholar] [CrossRef] [PubMed]
- Stultiens, J.J.A.; Guinand, N.; Van Rompaey, V.; Fornos, A.P.; Kunst, H.P.M.; Kingma, H.; van de Berg, R. The Resilience of the Inner Ear—Vestibular and Audiometric Impact of Transmastoid Semicircular Canal Plugging. J. Neurol. 2022, 269, 5229–5238. [Google Scholar] [CrossRef]
- Zhao, Y.C.; Somers, T.; van Dinther, J.; Vanspauwen, R.; Husseman, J.; Briggs, R. Transmastoid Repair of Superior Semicircular Canal Dehiscence. J. Neurol. Surg. Part B Skull Base 2012, 73, 225–229. [Google Scholar] [CrossRef]
- Van Haesendonck, G.; Van de Heyning, P.; Van Rompaey, V. Retrospective Cohort Study on Hearing Outcome after Transmastoid Plugging in Superior Semicircular Canal Dehiscence Syndrome: Our Experience. Clin. Otolaryngol. 2016, 41, 601–606. [Google Scholar] [CrossRef]
- Deschenes, G.R.; Hsu, D.P.; Megerian, C.A. Outpatient Repair of Superior Semicircular Canal Dehiscence via the Transmastoid Approach. Laryngoscope 2009, 119, 1765–1769. [Google Scholar] [CrossRef] [PubMed]
- Morrison, M.; Korda, A.; Wagner, F.; Caversaccio, M.D.; Mantokoudis, G. Case Report: Fremitus Nystagmus in Superior Canal Dehiscence Syndrome. Front. Neurol. 2022, 13, 844687. [Google Scholar] [CrossRef]
- Shaul, C.; Weder, S.; Dragovic, A.; Gerard, J.-M.; Briggs, R.J.S. Trans-Mastoid Plugging of Superior Semicircular Canal Dehiscence: Long-Term Follow-Up. Eur. Arch. Oto-Rhino-Laryngol. 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Cocca, S.; Mignacco, G.; Mandalà, M.; Giannitto, C.; Esposito, A.A.; Porcino, S. A ‘Double’ Third Window Syndrome: The Case of Semicircular Canal Dehiscence in Twin Sisters. Rep. Med. Imaging 2022, 15, 1–7. [Google Scholar] [CrossRef]
- Dang, P.T.; A Kennedy, T.; Gubbels, S.P. Simultaneous, Unilateral Plugging of Superior and Posterior Semicircular Canal Dehiscences to Treat Debilitating Hyperacusis. J. Laryngol. Otol. 2014, 128, 174–178. [Google Scholar] [CrossRef]
- Kirtane, M.V.; Sharma, A.; Satwalekar, D. Transmastoid Repair of Superior Semicircular Canal Dehiscence. J. Laryngol. Otol. 2009, 123, 356–358. [Google Scholar] [CrossRef] [PubMed]
- Wijaya, C.; Dias, A.; Conlon, B. Superior Semicircular Canal Occlusion-Transmastoid Approach. Int. J. Surg. Case Rep. 2012, 3, 42–44. [Google Scholar] [CrossRef] [PubMed]
- McCall, A.A.; McKenna, M.J.; Merchant, S.N.; Curtin, H.D.; Lee, D.J. Superior Canal Dehiscence Syndrome Associated with the Superior Petrosal Sinus in Pediatric and Adult Patients. Otol. Neurotol. 2011, 32, 1312–1319. [Google Scholar] [CrossRef]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing Heterogeneity in Meta-Analysis: Q Statistic or I 2 Index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Crovetto, M.; Areitio, E.; Elexpuru, J.; Aguayo, F. Transmastoid Approach for Resurfacing of Superior Semicircular Canal Dehiscence. Auris Nasus Larynx 2008, 35, 247–249. [Google Scholar] [CrossRef]
- Gioacchini, F.M.; Alicandri-Ciufelli, M.; Kaleci, S.; Scarpa, A.; Cassandro, E.; Re, M. Outcomes and Complications in Superior Semicircular Canal Dehiscence Surgery: A Systematic Review. Laryngoscope 2016, 126, 1218–1224. [Google Scholar] [CrossRef]
- Allsopp, T.; Kim, A.H.; Robbins, A.M.; Page, J.C.; Dornhoffer, J.L. Quality of Life Outcomes after Transmastoid Plugging of Superior Semicircular Canal Dehiscence. Am. J. Otolaryngol.—Head Neck Med. Surg. 2020, 41, 102287. [Google Scholar] [CrossRef]
- Pletcher, S.D.; Oghalai, J.S.; Reeck, J.B.; Cheung, S.W. Management of Superior Canal Dehiscence Syndrome with Extensive Skull-Base Deficiency. ORL 2005, 67, 192–195. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michailidou, E.; Rüegg, P.O.; Karrer, T.; Korda, A.; Weder, S.; Kompis, M.; Caversaccio, M.; Mantokoudis, G. Hearing Results after Transmastoid Superior Semicircular Canal Plugging for Superior Semicircular Canal Dehiscence: A Meta-Analysis. Audiol. Res. 2023, 13, 730-740. https://doi.org/10.3390/audiolres13050065
Michailidou E, Rüegg PO, Karrer T, Korda A, Weder S, Kompis M, Caversaccio M, Mantokoudis G. Hearing Results after Transmastoid Superior Semicircular Canal Plugging for Superior Semicircular Canal Dehiscence: A Meta-Analysis. Audiology Research. 2023; 13(5):730-740. https://doi.org/10.3390/audiolres13050065
Chicago/Turabian StyleMichailidou, Efterpi, Pascal Oliver Rüegg, Tanya Karrer, Athanasia Korda, Stefan Weder, Martin Kompis, Marco Caversaccio, and Georgios Mantokoudis. 2023. "Hearing Results after Transmastoid Superior Semicircular Canal Plugging for Superior Semicircular Canal Dehiscence: A Meta-Analysis" Audiology Research 13, no. 5: 730-740. https://doi.org/10.3390/audiolres13050065
APA StyleMichailidou, E., Rüegg, P. O., Karrer, T., Korda, A., Weder, S., Kompis, M., Caversaccio, M., & Mantokoudis, G. (2023). Hearing Results after Transmastoid Superior Semicircular Canal Plugging for Superior Semicircular Canal Dehiscence: A Meta-Analysis. Audiology Research, 13(5), 730-740. https://doi.org/10.3390/audiolres13050065