



Otic Capsule Dehiscences Simulating Other Inner Ear Diseases: Characterization, Clinical Profile, and Follow-Up—Is Ménière’s Disease the Sole Cause of Vertigo and Fluctuating Hearing Loss?

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion Criteria
2.3. Complementary Tests
2.4. Treatment
2.5. Postoperative Follow-Up
3. Results
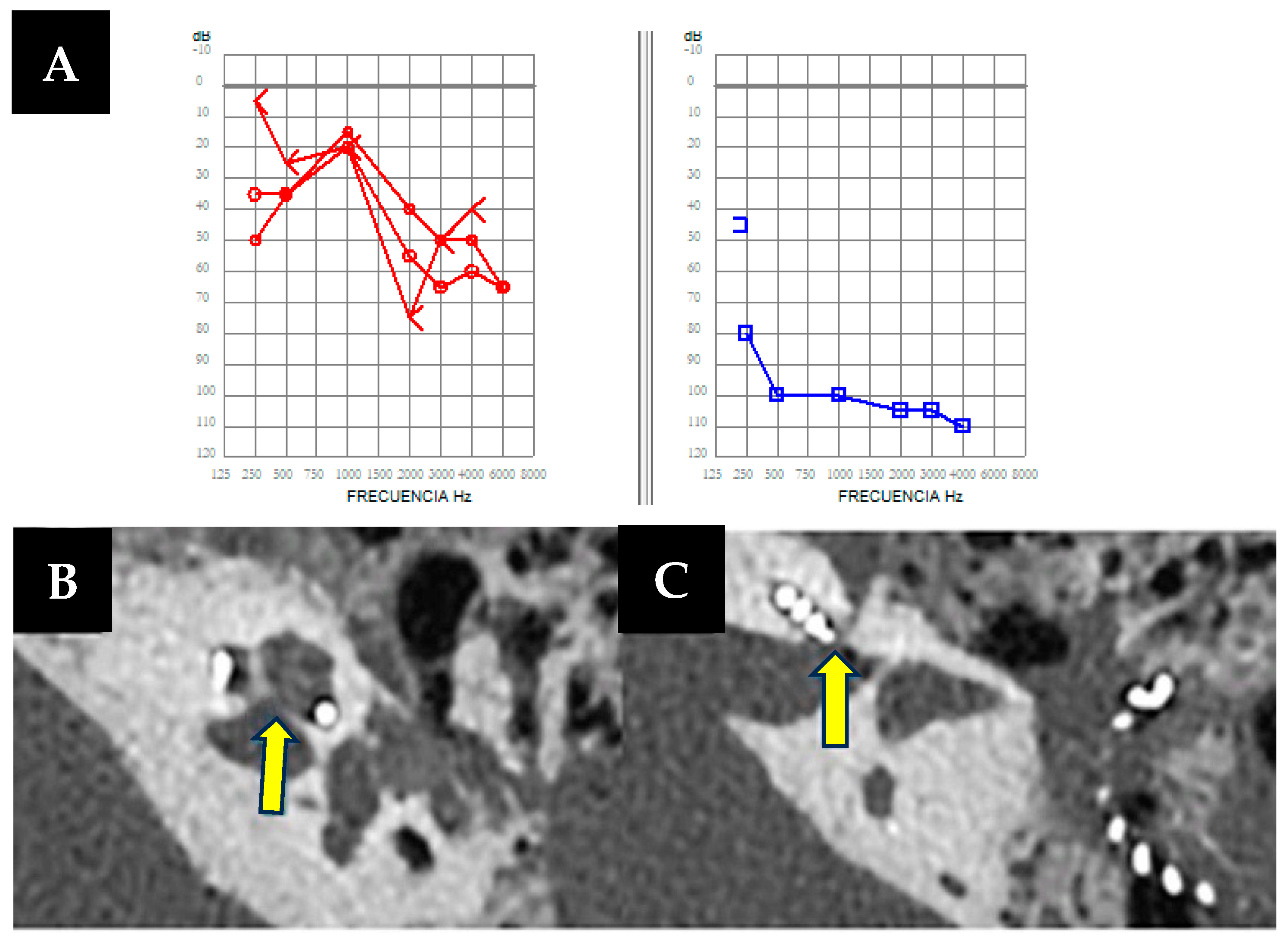
3.1. Case 1
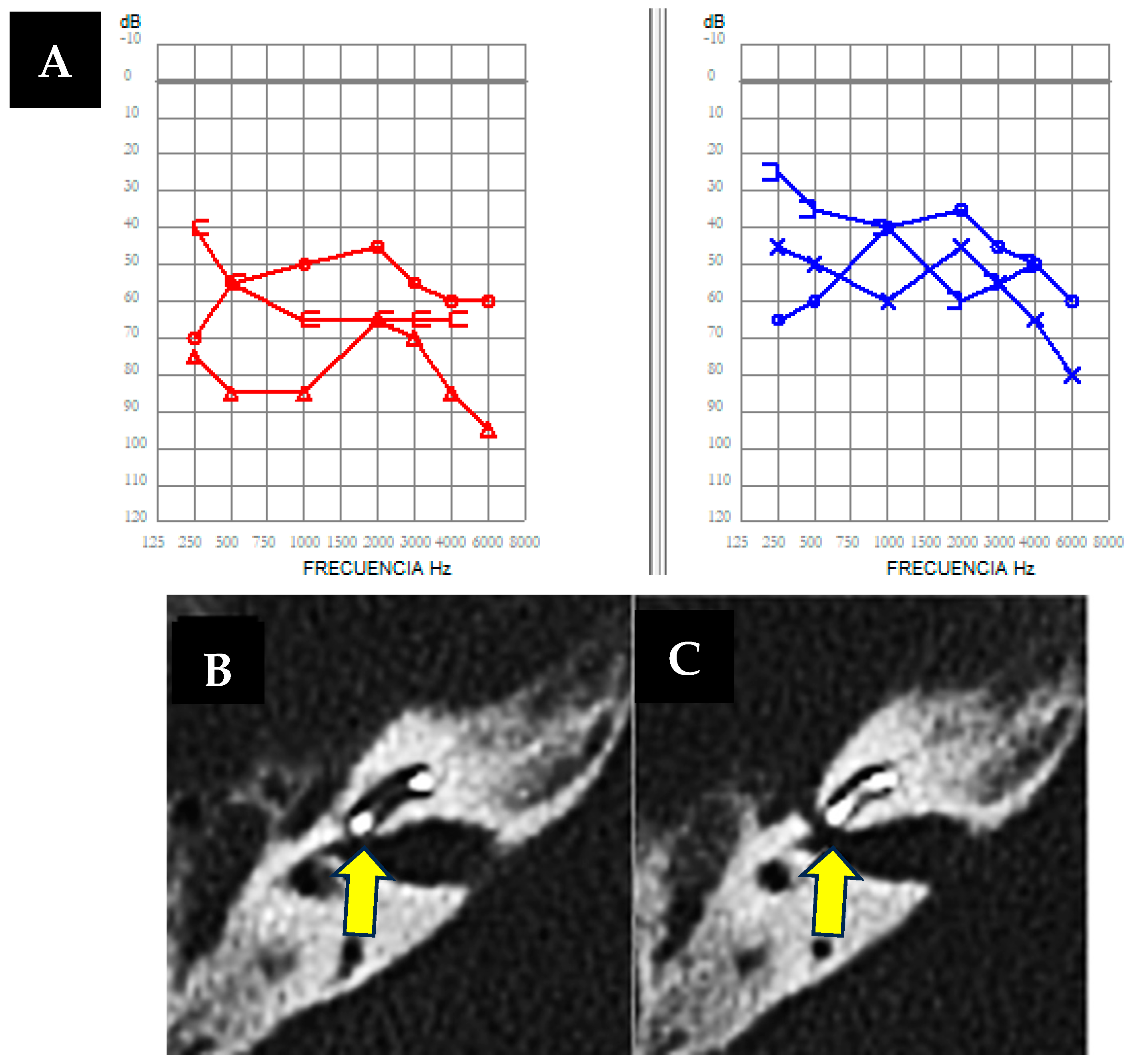
3.2. Case 2
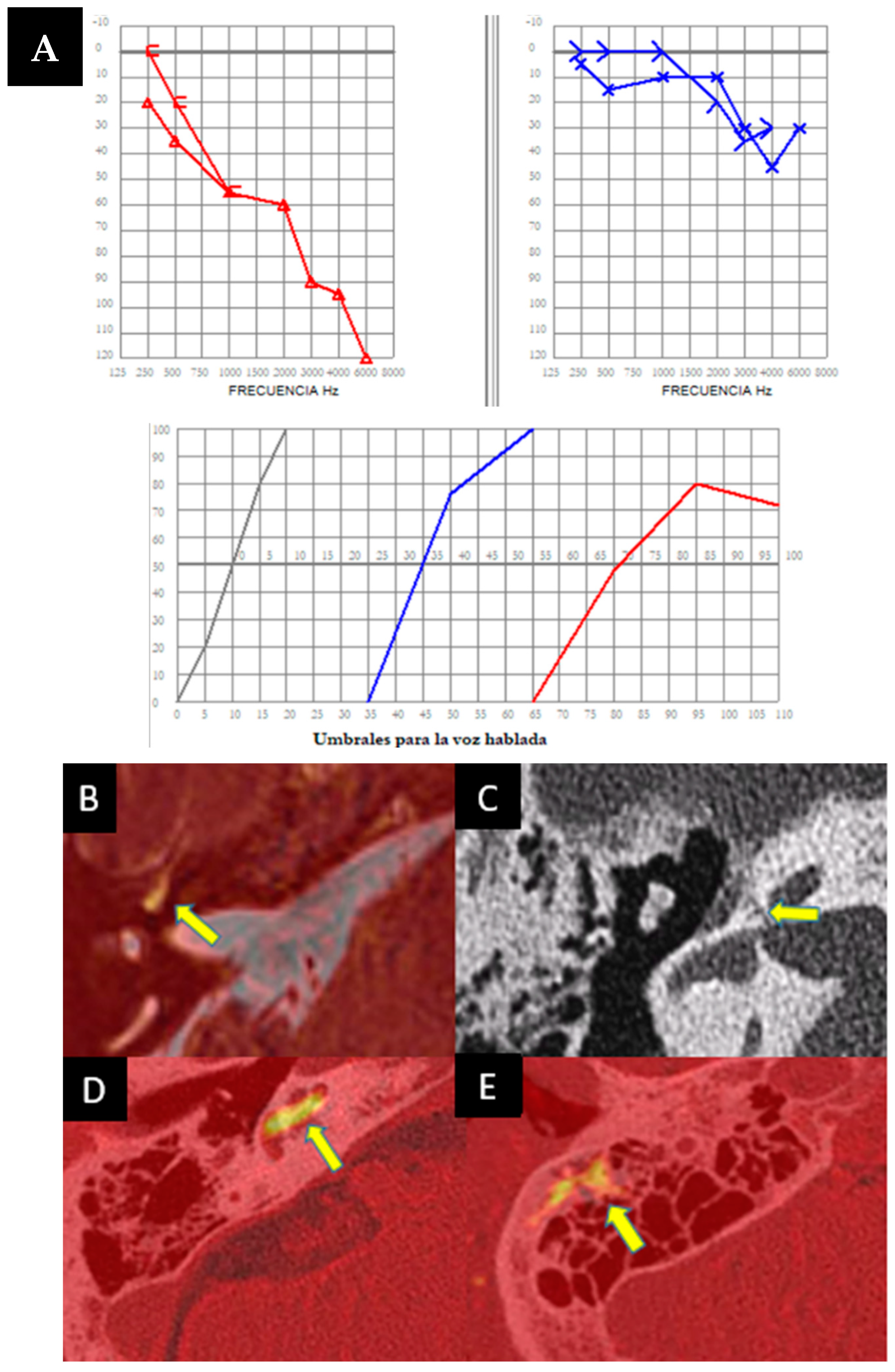
3.3. Case 3
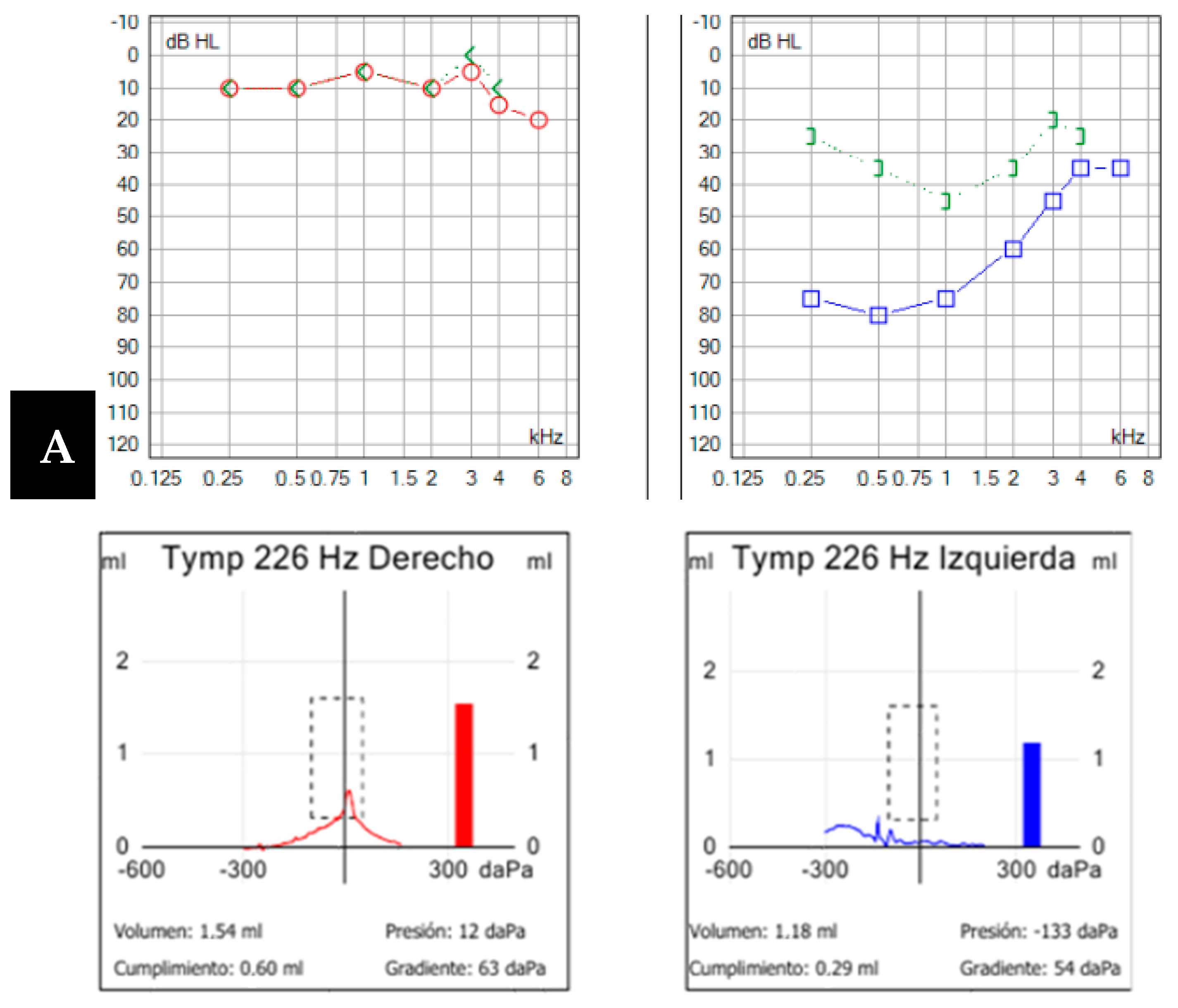
3.4. Case 4
3.5. Case 5
3.6. Case 6
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wackym, P.A.; Agrawal, Y.; Ikezono, T.; Balaban, C.D. Editorial: Third Window Syndrome. Front. Neurol. 2021, 18, 12. [Google Scholar] [CrossRef]
- Minor, L.B.; Solomon, D.; Zinreich, J.S.; Zee, D.S. Vértigo inducido por sonido y/o presión debido a la dehiscencia ósea del canal semicircular superior. Arco Otolaryngol. Cabeza Cuello Cirugía 2018, 124, 249–258. [Google Scholar]
- Jackler, R.K.; Luxford, W.M.; House, W.F. Congenital malformations of the inner ear: A classification based on embryogenesis. Laryngoscope 1987, 97, 2–14. [Google Scholar] [CrossRef]
- Khan, A.M.; Levine, S.; Nadol, J.B., Jr. The widely patent cochleovestibular communication of Edward Cock is a distinct inner ear malformation: Implications for cochlear implantation. Ann. Otol. Rhinol. Laryngol. 2006, 115, 595–606. [Google Scholar] [CrossRef]
- Lopez-Escamez, J.A.; Carey, J.; Chung, W.-H.; Goebel, J.A.; Magnusson, M.; Mandalà, M.; Newman-Toker, D.E.; Strupp, M.; Suzuki, M.; Trabalzini, F.; et al. Diagnostic criteria for Meniere’s disease. J. Vestib. Res. 2015, 25, 1–7. [Google Scholar] [CrossRef]
- Garaycochea, O.; Domínguez, P.D.; Manrique, M.; Manrique-Huarte, R. Cochlear-Internal Canal and Cochlear-Facial Dehiscence: A Novel Entity. J. Int. Adv. Otol. 2018, 14, 334–336. [Google Scholar] [CrossRef] [PubMed]
- Koroulakis, D.J.; Reilly, B.K.; Whitehead, M.T. Cochlear–facial dehiscence in a pediatric patient. Pediatr. Radiol. 2020, 50, 750–752. [Google Scholar] [CrossRef]
- Van Damme, J.P.; Heylen, G.; Gilain, C.; Garin, P. Pulsatile tinnitus associated with dehiscent internal carotid artery: An irremediable condition? Auris Nasus Larynx 2017, 44, 612–615. [Google Scholar] [CrossRef] [PubMed]
- Merchant, S.N.; Rosowski, J.J. Conductive hearing loss caused by third-window lesions of the inner ear. Otol. Neurotol. 2008, 29, 282–289. [Google Scholar] [CrossRef]
- Ho, M.L.; Moonis, G.; Halpin, C.F.; Curtin, H.D. Spectrum of third window abnormalities: Semicircular canal dehiscence and beyond. Am. J. Neuroradiol. 2017, 38, 2–9. [Google Scholar] [CrossRef]
- Webster, K.E.; Galbraith, K.; Lee, A.; Harrington-Benton, N.A.; Judd, O.; Kaski, D.; Maarsingh, O.R.; MacKeith, S.; Ray, J.; Van Vugt, V.A.; et al. Intratympanic gentamicin for Ménière’s disease. Cochrane Database Syst. Rev. 2023, 2023, CD015246. [Google Scholar]
- Eftekharian, A.; Amizadeh, M. Cerebrospinal fluid gusher in cochlear implantation. Cochlear Implants Int. 2014, 15, 179–184. [Google Scholar] [CrossRef]
- Fang, C.; Chung, S.; Blake, D.; Vazquez, A.; Li, C.; Carey, J.P.; Francis, H.W.; Jyung, R.W. Prevalence of cochlear-facial dehiscence in a study of 1,020 temporal bone specimens. Otol. Neurotol. 2016, 37, 967–972. [Google Scholar] [CrossRef]
- Chi, F.L.; Ren, D.D.; Dai, C.F. Variety of Audiologic Manifestations in Patients With Superior Semicircular Canal Dehiscence. Otol. Neurotol. 2010, 31, 2–10. [Google Scholar] [CrossRef]
- Wackym, P.A.; Balaban, C.D.; Zhang, P.; Siker, D.A.; Hundal, J.S. Third Window Syndrome: Surgical Management of Cochlea-Facial Nerve Dehiscence. Front Neurol. 2019, 10, 1281. [Google Scholar] [CrossRef] [PubMed]
- Reynard, P.; Idriss, S.; Ltaief-Boudrigua, A.; Bertholon, P.; Pirvan, A.; Truy, E.; Thai-Van, H.; Ionescu, E.C. Proposal for a Unitary Anatomo-Clinical and Radiological Classification of Third Mobile Window Abnormalities. Front. Neurol. 2022, 12, 792545. [Google Scholar] [CrossRef] [PubMed]
- Cloutier, J.F.; Belair, M.; Saliba, I. Superior semicircular canal dehiscence: Positive predictive value of high-resolution CT scanning. Eur. Arch. Otorhinolaryngol. 2018, 265, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Saxby, A.J.; Gowdy, C.; Fandino, M.; Chadha, N.K.; Kozak, F.K.; Sargent, M.A.; Lea, J. Radiological prevalence of superior and posterior semicircular canal dehiscence in children. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 411–418. [Google Scholar] [CrossRef]
- Krombach, G.A.; Di Martino, E.; Martiny, S.; Prescher, A.; Haage, P.; Buecker, A.; Günther, R.W. Dehiscence of the superior and/or posterior semicircular canal: Delineation on T2-weighted axial three-dimensional turbo spin-echo images, maximum intensity projections and volume-rendered images. Eur. Arch. Oto-Rhino-Laryngol. Head Neck 2006, 263, 111–117. [Google Scholar] [CrossRef]
- Gürkov, R. Menière and Friends. Otol. Neurotol. 2017, 38, e539–e544. [Google Scholar] [CrossRef]
- Naganawa, S.; Kawai, H.; Sone, M.; Ikeda, M. Ratio of Vestibular Endolymph in Patients with Isolated Lateral Semicircular Canal Dysplasia. Magn. Reson. Med. Sci. 2015, 14, 203–210. [Google Scholar] [CrossRef]
- Sone, M.; Yoshida, T.; Morimoto, K.; Teranishi, M.; Nakashima, T.; Naganawa, S. Endolymphatic hydrops in superior canal dehiscence and large vestibular aqueduct syndromes. Laryngoscope 2015, 126, 1446–1450. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pacient | Hipoacusis | Tinnitus/ Fullness | Vertigo Attacks | Vestibular Tests | Other | md/eh | Final Diagnose | |
|---|---|---|---|---|---|---|---|---|
| CASE 1 | MAN 73 YEARS | R: 40 dB L:100 dB | YES | NO | VHIT NORMAL VEMP NORMAL | LEFT GUSHER | NO | DEHISCENCIE COCHLEO-ICA |
| CASE 2 | MAN 53 YEARS | R: 80 dB L: 55 dB | YES | YES | VHIT ALTERED VEMP ALTERED | RIGHT GUSHER | YES | MD + DOUBLE DEHISCENCE |
| CASE 3 | MAN 54 YEARS | R:50 dB L: 26 dB | YES | YES | VHIT ALTERED VEMP ALTERED | - | YES | DEHISCENCIE COCHLEA-FACIAL. + MD |
| CASE 4 | WOMAN 39 YEARS | R:10 dB L: 52 dB | YES | NO | VHIT NORMAL VEMP NORMAL | - | NO | DEHISCENCIE COCHLEO-CAROTID |
| CASE 5 | MAN 18 YEARS | R:7 dB L: 26 dB | YES | NO | VHIT NORMAL VEMP ALTERED | TULIO AND HENNEBERT | NO | DEHISCENCE JUGULAR-PSC |
| CASE 6 | MAN 46 YEARS | R:12 dB L: 23 dB | YES | NO | VHIT NORMAL VEMP ALTERED | TULIO AND HENNEBERT | NO | DEHISCENCE YUGULAR-VA + DEHISCENCE SSC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorente-Piera, J.; Prieto-Matos, C.; Manrique-Huarte, R.; Garaycochea, O.; Domínguez, P.; Manrique, M. Otic Capsule Dehiscences Simulating Other Inner Ear Diseases: Characterization, Clinical Profile, and Follow-Up—Is Ménière’s Disease the Sole Cause of Vertigo and Fluctuating Hearing Loss? Audiol. Res. 2024, 14, 372-385. https://doi.org/10.3390/audiolres14020032
Lorente-Piera J, Prieto-Matos C, Manrique-Huarte R, Garaycochea O, Domínguez P, Manrique M. Otic Capsule Dehiscences Simulating Other Inner Ear Diseases: Characterization, Clinical Profile, and Follow-Up—Is Ménière’s Disease the Sole Cause of Vertigo and Fluctuating Hearing Loss? Audiology Research. 2024; 14(2):372-385. https://doi.org/10.3390/audiolres14020032
Chicago/Turabian StyleLorente-Piera, Joan, Carlos Prieto-Matos, Raquel Manrique-Huarte, Octavio Garaycochea, Pablo Domínguez, and Manuel Manrique. 2024. "Otic Capsule Dehiscences Simulating Other Inner Ear Diseases: Characterization, Clinical Profile, and Follow-Up—Is Ménière’s Disease the Sole Cause of Vertigo and Fluctuating Hearing Loss?" Audiology Research 14, no. 2: 372-385. https://doi.org/10.3390/audiolres14020032
APA StyleLorente-Piera, J., Prieto-Matos, C., Manrique-Huarte, R., Garaycochea, O., Domínguez, P., & Manrique, M. (2024). Otic Capsule Dehiscences Simulating Other Inner Ear Diseases: Characterization, Clinical Profile, and Follow-Up—Is Ménière’s Disease the Sole Cause of Vertigo and Fluctuating Hearing Loss? Audiology Research, 14(2), 372-385. https://doi.org/10.3390/audiolres14020032