
Skull Vibration-Induced Nystagmus in Superior Semicircular Canal Dehiscence: A New Insight into Vestibular Exploration—A Review

 ,
,  ,
,  , ,
, , 


Abstract
1. Introduction
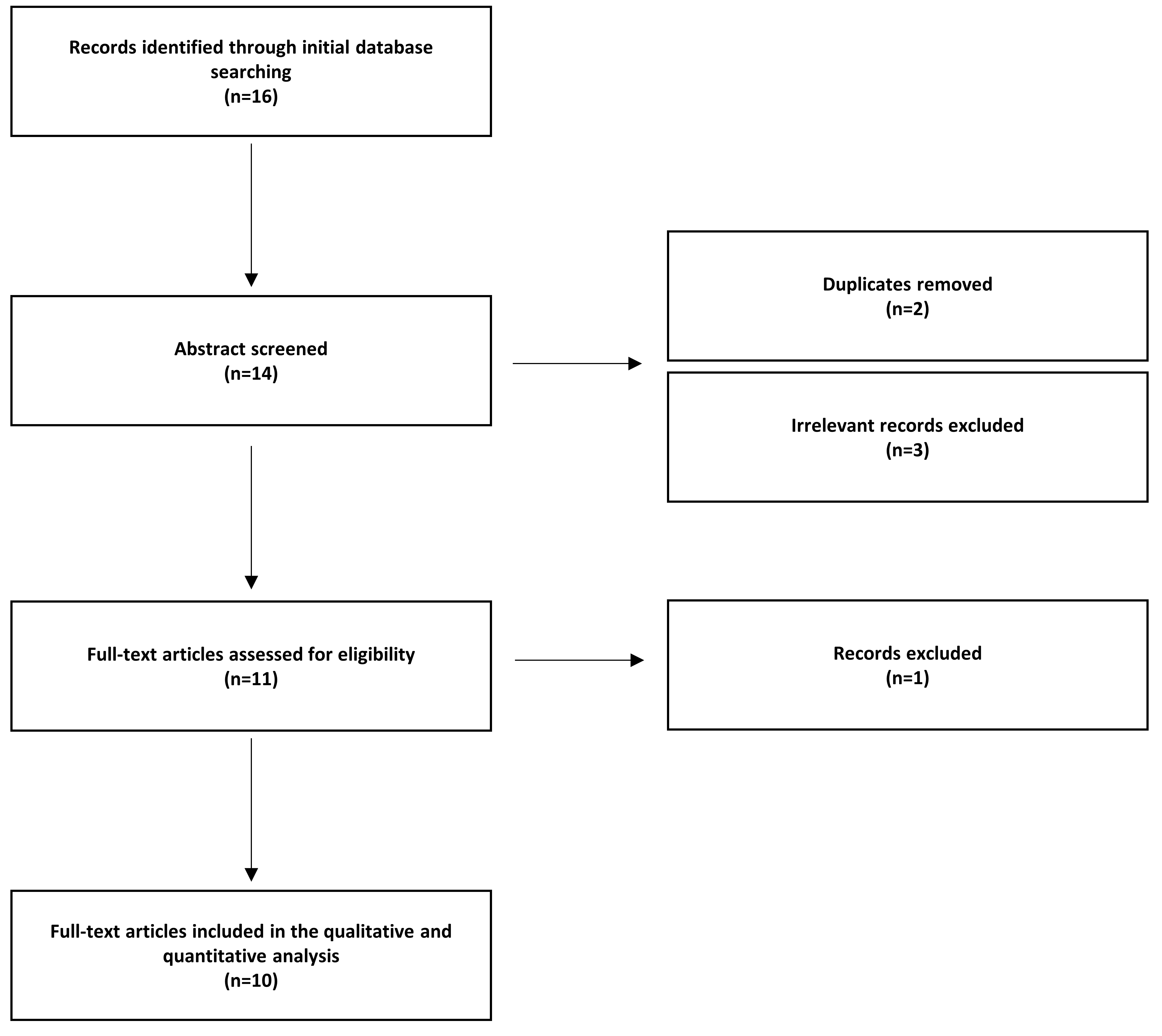
2. Methodology
2.1. Search Strategy
2.2. Study Selection Criteria
2.3. Study Data Extraction
3. SVIN Results in the SCD
4. Discussion
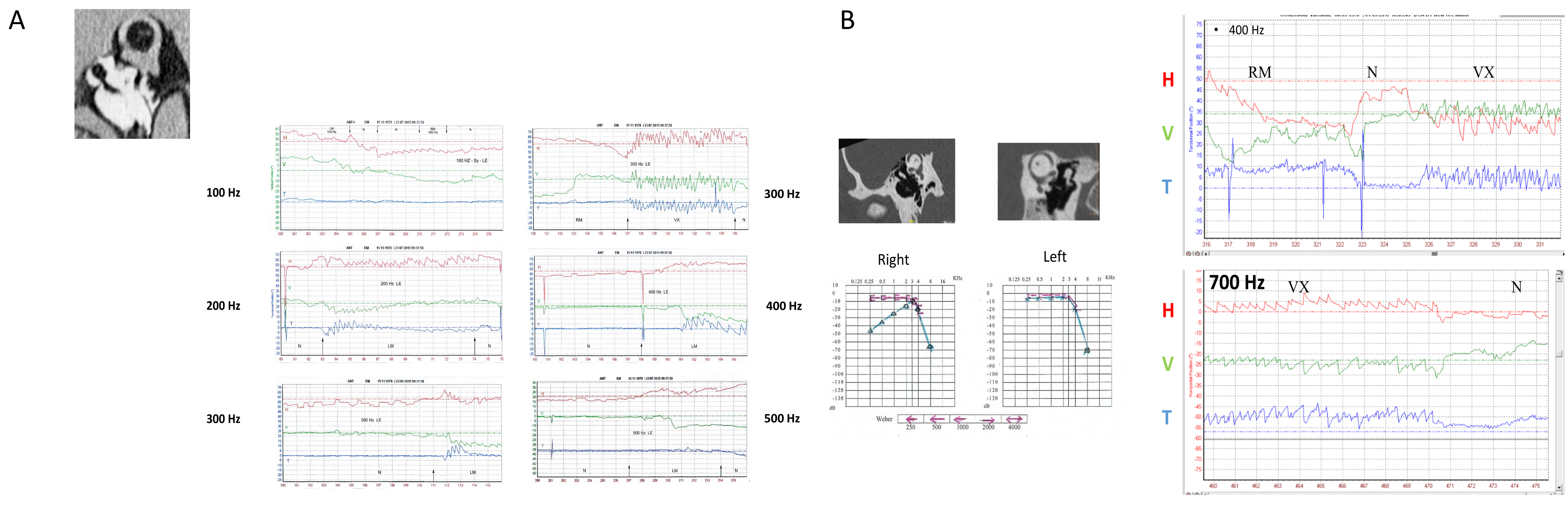
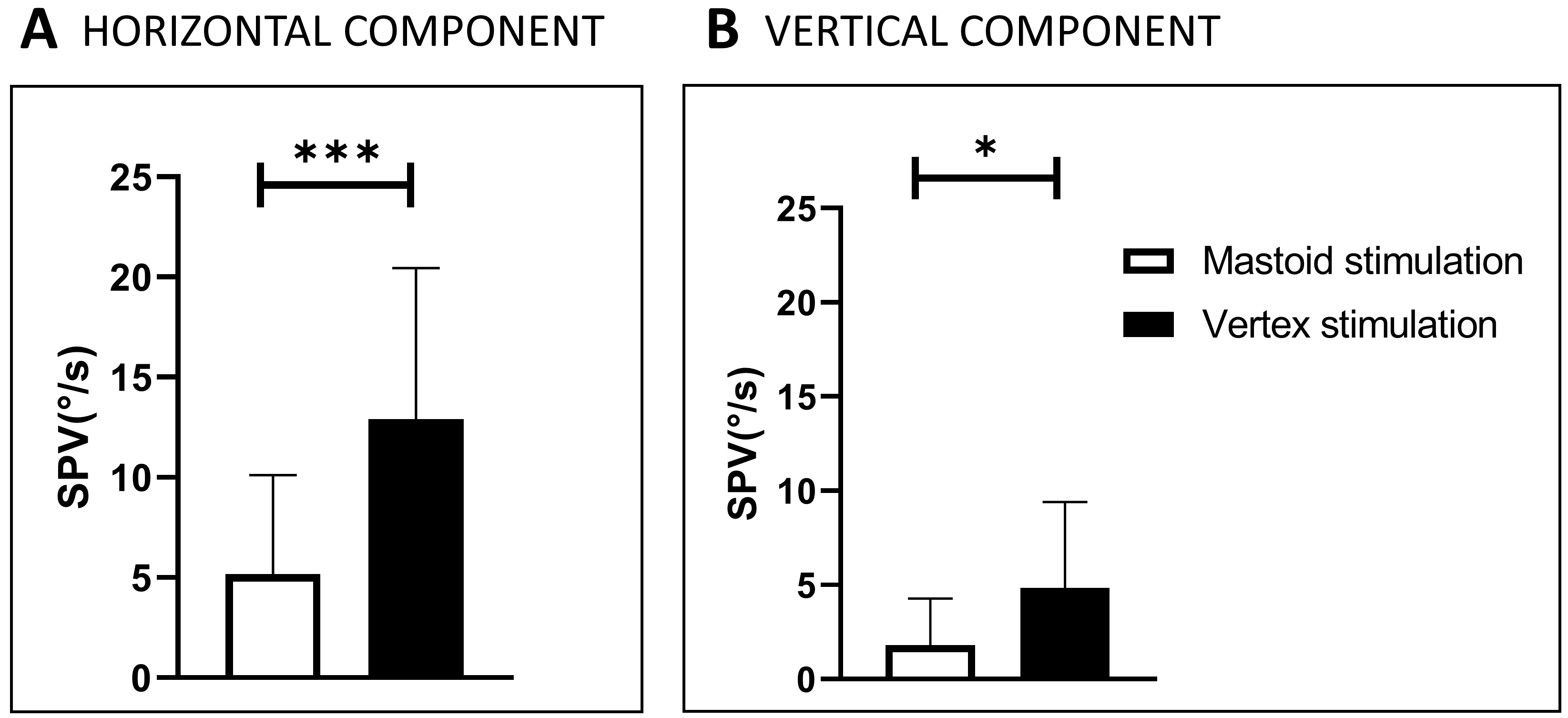
4.1. Optimal Location of Stimulation in SCD
4.1.1. BC Stimulation Locations
4.1.2. Possible Explanations for Variable Results in SCD Patients
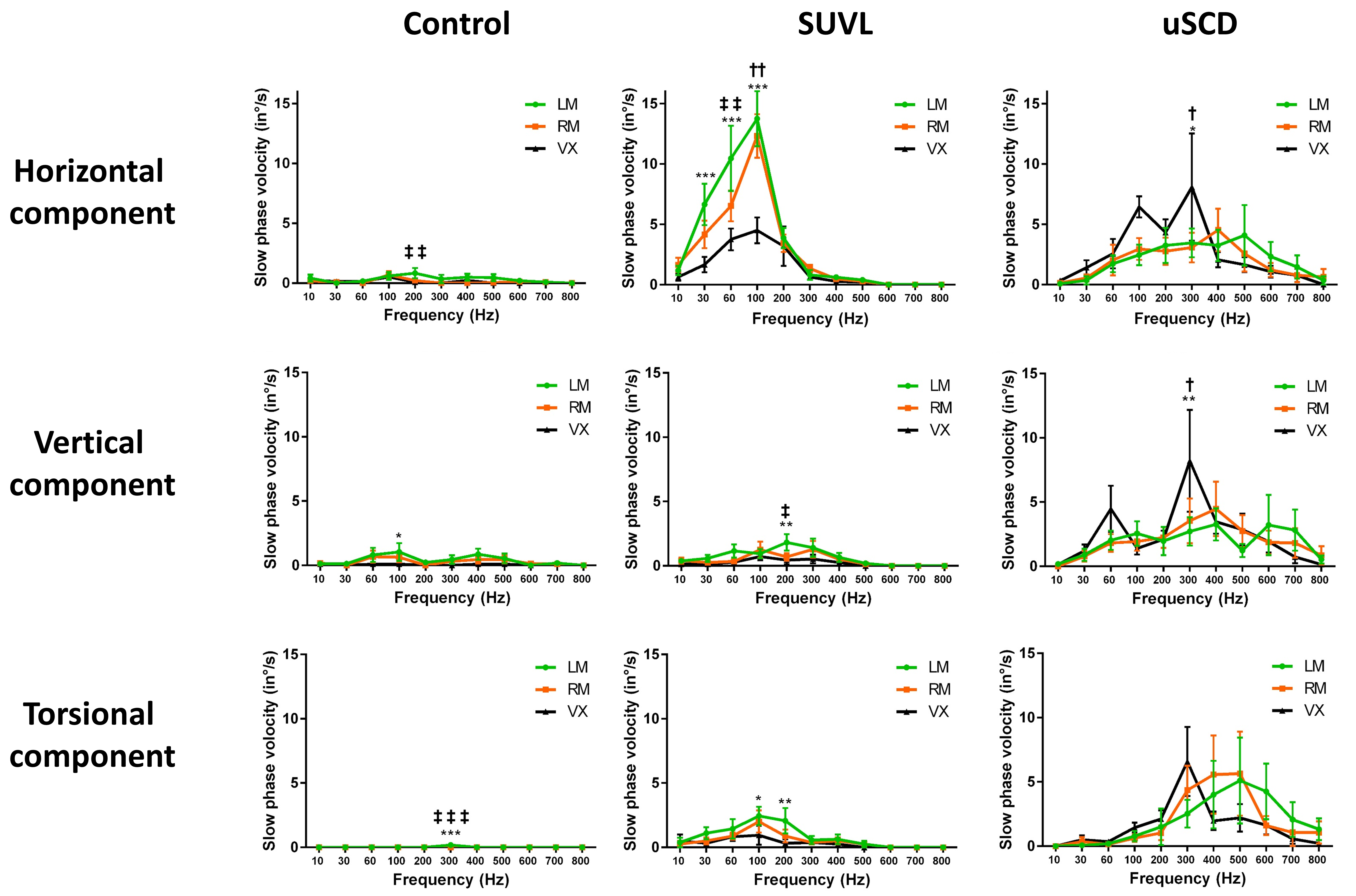
4.2. Stimulus Optimal Frequency—Frequency Spectrum Sensitivity for SVIN in SCD
4.3. Characteristics of the Nystagmus Obtained in SCD (Direction, Components)
4.4. SVIN as a Bone-Conducted Tullio Phenomenon (BCTP)
- (1)
- Cycle-by-cycle phase-locked activation of action potentials in SCC afferents with irregular resting discharge;
- (2)
- Cupula deflection by fluid streaming caused by the traveling waves of fluid displacement initiated by sound or vibration at the point of dehiscence. This fluid flow causes a slow deflection of the cupula, allowing for a slow return at the end of BCV stimulation and thus accounting for after-nystagmus. This cupula deflection stimulates neurons with regular resting discharge that are not directly activated by cycle-by-cycle phase-locked vibration [24,26]. The direction of the fluid current depends on the location of the stimulus, the location and size of the dehiscence, and the frequency of the stimulus [26,27,28]. The direct measures showed that the direction of fluid flow changed with frequency.
- (1)
- Direct stimulation on the affected side of the type I vestibular receptor hair cells (and afferent neurons with irregular neural discharge) at high frequency favored by BC facilitation toward the side of the dehiscence in relation to the third window mechanism [25]. This explains the most commonly observed ipsilateral excitatory nystagmus.
- (2)
4.5. Sensitivity of SVIN to Detect SCD Compared with Other Bedside Explorations or Vestibular Test Explorations
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACTP | air-conducted Tullio phenomenon |
| BCTP | bone-conducted Tullio phenomenon |
| SCD | superior (semi-circular) canal dehiscence |
| uSCD | unilateral SCD |
| bSCD | bilateral SCD |
| uVL | unilateral vestibular loss |
| BC or BCV | bone-conducted vibrations |
| SVIN | skull-vibration-induced nystagmus |
| SVINT | SVIN test |
| SPV | slow-phase velocity |
| ViVOR | vibration-induced vestibulo-ocular reflex |
References
- Minor, L.B. Superior canal dehiscence syndrome. Am. J. Otol. 2000, 21, 9–19. [Google Scholar] [CrossRef]
- Minor, L.B.; Solomon, D.; Zinreich, J.S.; Zee, D.S. Sound- and/or Pressure-Induced Vertigo Due to Bone Dehiscence of the Superior Semicircular Canal. Arch. Otolaryngol. Head Neck Surg. 1998, 124, 249. [Google Scholar] [CrossRef] [PubMed]
- Songer, J.E.; Rosowski, J.J. A mechano-acoustic model of the effect of superior canal dehiscence on hearing in chinchilla. J. Acoust. Soc. Am. 2007, 122, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Ward, B.K.; Carey, J.P.; Minor, L.B. Superior Canal Dehiscence Syndrome: Lessons from the First 20 Years. Front. Neurol. 2017, 8, 177. [Google Scholar] [CrossRef]
- Tullio, P. Das Ohr und die Entstehung der Sprache und Schrift; England Urban & Schwartzenberg: Oxford, UK, 1929; p. 445. [Google Scholar]
- Tullio, P. Sulla Funzione Delle Varie Parti Dell’orecchio Interno; Capelli: New York, NY, USA, 1926. [Google Scholar]
- Parker, D. Effect of Sound on the Vestibular System; Miami University: Oxford, OH, USA, 1976; p. TR-75-89. [Google Scholar]
- Dumas, G.; Perrin, P.; Morel, N.; N’Guyen, D.Q.; Schmerber, S. Skull vibratory test in partial vestibular lesions--influence of the stimulus frequency on the nystagmus direction. Rev. Laryngol. Otol. Rhinol. 2005, 126, 235–242. [Google Scholar]
- Dumas, G.; Tan, H.; Dumas, L.; Perrin, P.; Lion, A.; Schmerber, S. Skull vibration induced nystagmus in patients with superior semicircular canal dehiscence. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, 263–272. [Google Scholar] [CrossRef]
- White, J.A.; Hughes, G.B.; Ruggieri, P.N. Vibration-induced nystagmus as an office procedure for the diagnosis of superior semicircular canal dehiscence. Otol. Neurotol. 2007, 28, 911–916. [Google Scholar]
- Rosengren, S.M.; Colebatch, J.G.; Young, A.S.; Govender, S.; Welgampola, M.S. Vestibular evoked myogenic potentials in practice: Methods, pitfalls and clinical applications. Clin. Neurophysiol. Pract. 2019, 4, 47–68. [Google Scholar] [CrossRef]
- Zhang, A.S.; Govender, S.; Colebatch, J.G. Tuning of the ocular vestibular evoked myogenic potential (oVEMP) to air- and bone-conducted sound stimulation in superior canal dehiscence. Exp. Brain Res. 2012, 223, 51–64. [Google Scholar]
- Manzari, L.; Burgess, A.M.; McGarvie, L.A.; Curthoys, I.S. An indicator of probable semicircular canal dehiscence: Ocular vestibular evoked myogenic potentials to high frequencies. Otolaryngol. Head Neck Surg. 2013, 149, 142–145. [Google Scholar]
- Zuniga, M.G.; Janky, K.L.; Nguyen, K.D.; Welgampola, M.S.; Carey, J.P. Ocular versus cervical VEMPs in the diagnosis of superior semicircular canal dehiscence syndrome. Otol. Neurotol. 2013, 34, 121–126. [Google Scholar] [PubMed]
- Welgampola, M.; Rosengren, S.; Halmagyi, G.; Colebatch, J. Vestibular activation by bone conducted sound. J. Neurol. Neurosurg. Psychiatry 2003, 74, 771–778. [Google Scholar]
- Cremer, P.; Minor, L.; Zee, D. Nystagmus produced by mastoid vibration in patients with Tullio’s phenomenon. In Transactions of the XXth Regular Meeting of the Barany Society; Würzburg; 11–12 September 1998; Claussen, C.F., Haid, C.T., Hofferberth, B., Eds.; Elsevier: Amsterdam, The Netherlands, 1998. [Google Scholar]
- Dumas, G.; Lion, A.; Karkas, A.; Perrin, P.; Perottino, F.; Schmerber, S. Skull vibration-induced nystagmus test in unilateral superior canal dehiscence and otosclerosis: A vestibular Weber test. Acta Oto-Laryngol. 2014, 134, 588–600. [Google Scholar] [CrossRef] [PubMed]
- Aw, S.T.; Aw, G.E.; Todd, M.J.; Bradshaw, A.P.; Halmagyi, G.M. Three-dimensional vibration-induced vestibulo-ocular reflex identifies vertical semicircular canal dehiscence. J. Assoc. Res. Otolaryngol. 2011, 12, 549–558. [Google Scholar] [PubMed]
- Manzari, L.; Modugno, G.C.; Brandolini, C.; Pirodda, A. Bone vibration-induced nystagmus is useful in diagnosing superior semicircular canal dehiscence. Audiol. Neurootol. 2008, 13, 379–387. [Google Scholar]
- Park, J.H.; Kim, H.J.; Kim, J.S.; Koo, J.W. Costimulation of the horizontal semicircular canal during skull vibrations in superior canal Dehiscence syndrome. Audiol. Neurootol. 2014, 19, 175–183. [Google Scholar] [PubMed]
- Batuecas-Caletrío, Á.; Jara, A.; Suarez-Vega, V.M.; Marcos-Alonso, S.; Sánchez-Gómez, H.; Pérez-Fernández, N. Skull Vibration-Induced Nystagmus and High Frequency Ocular Vestibular-Evoked Myogenic Potentials in Superior Canal Dehiscence. Audiol. Res. 2022, 12, 202–211. [Google Scholar] [CrossRef]
- Schmerber, S.; Dumas, G.; Perrin, P. Anterior semicircular canal dehiscence and cranial vibration-induced nystagmus test. Otol. Neurotol. 2008, 29, 573–574; author reply 574. [Google Scholar] [CrossRef]
- Mehta, R.; Klumpp, M.L.; Spear, S.A.; Bowen, M.A.; Arriaga, M.A.; Ying, Y.L.M. Subjective and objective findings in patients with true dehiscence versus thin bone over the superior semicircular canal. Otol. Neurotol. 2015, 36, 289–294. [Google Scholar] [CrossRef]
- Dumas, G.; Curthoys, I.S.; Castellucci, A.; Dumas, L.; Perrin, P.; Schmerber, S. A bone-conducted Tullio phenomenon—A bridge to understand skull vibration induced nystagmus in superior canal dehiscence. Front. Neurol. 2023, 14, 1183040. [Google Scholar] [CrossRef]
- Songer, J.E.; Rosowski, J.J. The effect of superior canal dehiscence on cochlear potential in response to air-conducted stimuli in chinchilla. Hear. Res. 2005, 210, 53–62. [Google Scholar] [PubMed]
- Iversen, M.M.; Zhu, H.; Zhou, W.; Della Santina, C.C.; Carey, J.P.; Rabbitt, R.D. Sound abnormally stimulates the vestibular system in canal dehiscence syndrome by generating pathological fluid-mechanical waves. Sci. Rep. 2018, 8, 10257. [Google Scholar] [CrossRef] [PubMed]
- Rabbitt, R.D. Semicircular canal biomechanics in health and disease. J. Neurophysiol. 2019, 121, 732–755. [Google Scholar] [CrossRef]
- Liebau, G. Uber ein ventiloses pumpprinzip. Naturwissenschaften 1954, 41, 327. [Google Scholar] [CrossRef]
- Merchant, S.N.; Rosowski, J.J. Conductive Hearing Loss Caused by Third-Window Lesions of the Inner Ear. Otol. Neurotol. 2008, 29, 282–289. [Google Scholar] [CrossRef] [PubMed]
- White, J.; Krakovitz, P. Nystagmus in Enlarged Vestibular Aqueduct: A Case Series. Audiol. Res. 2015, 5, 120. [Google Scholar] [PubMed]
- Stenfelt, S. Investigation of Mechanisms in Bone Conduction Hyperacusis With Third Window Pathologies Based on Model Predictions. Front. Neurol. 2020, 11, 966. [Google Scholar]
- Freeman, S.; Sichel, J.Y.; Sohmer, H. Bone conduction experiments in animals—Evidence for a non-osseous mechanism. Hear. Res. 2000, 146, 72–80. [Google Scholar] [CrossRef]
- Dlugaiczyk, J.; Burgess, A.M.; Goonetilleke, S.C.; Sokolic, L.; Curthoys, I.S. Superior Canal Dehiscence Syndrome: Relating Clinical Findings With Vestibular Neural Responses From a Guinea Pig Model. Otol. Neurotol. 2019, 40, e406–e414. [Google Scholar] [CrossRef]
- Koo, J.W.; Hong, S.K.; Kim, D.K.; Kim, J.S. Superior semicircular canal dehiscence syndrome by the superior petrosal sinus. J. Neurol. Neurosurg. Psychiatry 2010, 81, 465–467. [Google Scholar] [CrossRef]
- Cohen, B.; Suzuki, J.I.; Bender, M.B. Eye movements from semicircular canal nerve stimulation in the cat. Ann. Otol. Rhinol. Laryngol. 1964, 73, 153–169. [Google Scholar] [PubMed]
- Suzuki, J.I.; Tokumasu, K.; Goto, K. Eye movements from single utricular nerve stimulation in the cat. Acta Otolaryngol. 1969, 68, 350–362. [Google Scholar] [CrossRef]
- Lehmkuhl, B.; Andaloro, C. Tullio Phenomenon. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK513229/ (accessed on 28 November 2022).
- Halmagyi, G.M.; Curthoys, I.S.; Colebatch, J.G.; Aw, S.T. Vestibular responses to sound. Ann. N. Y. Acad. Sci. 2005, 1039, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Basura, G.J.; Cronin, S.J.; Heidenreich, K.D. Tullio phenomenon in superior semicircular canal dehiscence syndrome. Neurology 2014, 82, 1010. [Google Scholar] [CrossRef]
- Addams-Williams, J.; Wu, K.; Ray, J. The experiments behind the Tullio phenomenon. J. Laryngol. Otol. 2014, 128, 223–227. [Google Scholar]
- Carey, J.P.; Hirvonen, T.P.; Hullar, T.E.; Minor, L.B. Acoustic Responses of Vestibular Afferents in a Model of Superior Canal Dehiscence. Otol. Neurotol. 2004, 25, 345–352. [Google Scholar]
- Taylor, R.L.; Magnussen, J.S.; Kwok, B.; Young, A.S.; Ihtijarevic, B.; Argaet, E.C.; Reid, N.; Rivas, C.; Pogson, J.M.; Rosengren, S.M.; et al. Bone-Conducted oVEMP Latency Delays Assist in the Differential Diagnosis of Large Air-Conducted oVEMP Amplitudes. Front. Neurol. 2020, 11, 580184. [Google Scholar] [CrossRef] [PubMed]
- Erlich, M.A.; Lawson, W. The incidence and significance of the Tullio phenomenon in man. Otolaryngol. Head Neck Surg. 1979, 88, 630–635. [Google Scholar] [CrossRef]
- Ionescu, E.C.; Reynard, P.; Damien, M.; Ltaief-Boudrigua, A.; Hermann, R.; Gianoli, G.J.; Thai-Van, H. Why should multiple dehiscences of the otic capsule be considered before surgically treating patients with superior semicircular canal dehiscence? A radiological monocentric review and a case series. Front. Neurol. 2023, 14, 1209567. [Google Scholar] [CrossRef]
- Carey, J.P.; Minor, L.B.; Nager, G.T. Dehiscence or thinning of bone overlying the superior semicircular canal in a temporal bone survey. Arch. Otolaryngol. Head Neck Surg. 2000, 126, 137–147. [Google Scholar] [CrossRef]
- Ward, B.K.; van de Berg, R.; van Rompaey, V.; Bisdorff, A.; Hullar, T.E.; Welgampola, M.S.; Carey, J.P. Superior semicircular canal dehiscence syndrome: Diagnostic criteria consensus document of the committee for the classification of vestibular disorders of the Bárány Society. J. Vestib. Res. 2021, 31, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Masaki, Y. The prevalence of superior canal dehiscence syndrome as assessed by temporal bone computed tomography imaging. Acta Otolaryngol. 2011, 131, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Reynard, P.; Idriss, S.; Ltaief-Boudrigua, A.; Bertholon, P.; Pirvan, A.; Truy, E.; Thai-Van, H.; Ionescu, E.C. Proposal for a Unitary Anatomo-Clinical and Radiological Classification of Third Mobile Window Abnormalities. Front. Neurol. 2022, 12, 792545. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Se (%) | Cohort Size | Patient Count uSCD/ bSCD | Stimulus Locations Optimal Location | Stimulus Frequency (Hz) | SHC Num (%) | SVC Num (%) | STC Num (%) | SVIN DCF Location Num - (%) | SVIN DCF Frequency Num - (%) | After-nyst Num | AC Tullio Num - (%) Hennebert Num - (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| White et al., 2007 [10] | 100 | 8 | 6 | RM, LM, Vx, SO | 100 | ND | Down 2 Up 1 | Contr3 Ipsi 2 | 1/8 (12) | ND | 1/8 combined with positional nyst. | ND 2/8 (25) |
| 2 | Opt. SO | ND | Down 1 Up 0 | 2 | ||||||||
| Schmerber et al., 2008 [22] | - | 6 | 4 | RM, LM Vx | 100 | Ipsi 3 (50) | Down 2 Up 2 | ND | ND | ND | ND | rarely |
| 2 | Opt Vx | - | 0 | 0 | ND | |||||||
| Manzari et al., 2008 [19] | 100 | 16 | 9 7 | RM, LM - | 100 - | Poor Poor | Down 7 Up 2 Down 4 Up 1 | Ipsi 4 Contr 0 | HC: 7/9 VC: 7/9 TC: 6/7 | ND | ND | 9/16 (56) ND |
| Aw et al., 2011 [18] (ViVOR) | 100 | 17 | 12 | RM, LM | 500 | Small (negligible) | ViVOR up | ViVOR contr | 0 TC: RM/LM | ND | 9/12 (80) ND 5/5 (100) ND | |
| 5 | - | - | Small | ViVORup++ | ||||||||
| Dumas et al., 2014 [17] | 82 | 17 | 17 | RM, LM Vx Opt Vx | 100 | Ipsi (70) | Up (47) | ipsi (62) | HC 2/17 VC 1/17 TC 2/17 | ND | 4/17 | 4/17 (24) ND ND |
| 0 | 0 | 0 | 0 | 0 | ||||||||
| Park et al., 2014 [20] (ViVOR) | 90 | 10 | 9 | RM, LM | 100 | ViVOR Ipsi (18) Contr (70) | Down (21) Up (75) | 1 | ND | ND | ND | 8/10 (80) ND |
| 1 | - | - | - | - | - | |||||||
| Mehta et al., 2015 [23] | 55 | 38 CD (50 CD+T) | ND | RM, LM | ND | ND | ND | ND | ND | ND | ND | 10/38 (26) 8/38 (21) |
| Dumas et al., 2019 [9] | 86 54 | 40 | 27 | RM, LM, Vx | 100–800 | Ipsi (85) Contr (2) | Down (40) Up (60) | Ipsi (57) Contr (2) | 2/10 (20) | 2/8 (25) | 1 | 5/20 (25) ND ND ND |
| 13 | Opt Vx | Down (25) Up (75) | ||||||||||
| Batuecas et al., 2022 [21] | 66 | 30 | 25 | RM, LM Vx | 100 | 6/30 | Up 14/30 | ND | ND | ND | ND | ND ND ND ND |
| 5 | Opt: ND | 4/9 | Up 4/9 | ND | ||||||||
| Dumas et al., 2023 [24] | 91 | 52 | 39 | RM, LM Vx | 30–800 | Ipsi 29/36 (81) Contr 5/36 (19) | Down13/25 (52) Up 12/25 (48) | 21/37 (56) | 2/8 (25) | 10/28 (25) | 12/34 (35) 10/35 (30) | |
| 13 | Opt Vx = M |
| Series | Nb | Age (Mean +/− SD) | Gender M/F | Size Mean +/− SD | SVIN Se VX + M Nb, (%) | Optimal Location Nb, (%) | SVIN Direction On VX Stim. Nb, (%) | SVIN CDFL Vx/M LM/RM | SVIN CDFF 60–800 Hz | After-nyst. | oVEMP | cVEMP | VHIT Ipsi Hypo Nb, (%) Gain Mean+/− SD | ACTP (Tullio) | Hennebert | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vx | Vx = M | M | H Comp | V Comp | ||||||||||||||
| GD | 12 | 62.2 10.32 | M = 5 F = 7 | 4.55 1.80 | 11 (91) | 9 (82) | 2 (18) | 0 (0) | Ip:10/11 (91) Ctl:1/11 (9) | Up: 2/8 Down: 6/8 | 6/11 (54) | 2/8 (25) | 3/12 (25) | 8/9 (88) | 9/10 (90) | 2/12 Gain ND | 4/10 (40) | 2/10 (20) |
| AC | 27 | 64.03 9.80 | M = 15 F = 12 | 3.20 1.29 | 25 (93) | 2 (8) | 9 (35) | 15 (57) | Ip:19/25 (75) Ctl:4/25 (15) | Up: 10/17 Down: 7/17 | 15/26 (57) | ND | 7/26 (26) | 23/27 (85) | 24/27 (96) | 21/27 Gain 0.56 0.17 | 8/24 (33) | 8/23 (35) |
| Total | 39 | 63.4 9.86 | M = 20 F = 19 | 3.58 1.55 | 36 (92) | 11 (30) | 11 (30) | 15 (40) | Ip:29/36 (81) Ctl:5/36 (19) | Up: 12/25 Down: 13/25 | 21/37 (56) | (25) | 10/28 (25) | 31/36 (86) | 33/37 (89) | 23/39 (58) | 12/34 (35) | 10/35 (30) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dumas, G.; Curthoys, I.; Castellucci, A.; Dumas, L.; Peultier-Celli, L.; Armato, E.; Malara, P.; Perrin, P.; Schmerber, S. Skull Vibration-Induced Nystagmus in Superior Semicircular Canal Dehiscence: A New Insight into Vestibular Exploration—A Review. Audiol. Res. 2024, 14, 96-115. https://doi.org/10.3390/audiolres14010009
Dumas G, Curthoys I, Castellucci A, Dumas L, Peultier-Celli L, Armato E, Malara P, Perrin P, Schmerber S. Skull Vibration-Induced Nystagmus in Superior Semicircular Canal Dehiscence: A New Insight into Vestibular Exploration—A Review. Audiology Research. 2024; 14(1):96-115. https://doi.org/10.3390/audiolres14010009
Chicago/Turabian StyleDumas, Georges, Ian Curthoys, Andrea Castellucci, Laurent Dumas, Laetitia Peultier-Celli, Enrico Armato, Pasquale Malara, Philippe Perrin, and Sébastien Schmerber. 2024. "Skull Vibration-Induced Nystagmus in Superior Semicircular Canal Dehiscence: A New Insight into Vestibular Exploration—A Review" Audiology Research 14, no. 1: 96-115. https://doi.org/10.3390/audiolres14010009
APA StyleDumas, G., Curthoys, I., Castellucci, A., Dumas, L., Peultier-Celli, L., Armato, E., Malara, P., Perrin, P., & Schmerber, S. (2024). Skull Vibration-Induced Nystagmus in Superior Semicircular Canal Dehiscence: A New Insight into Vestibular Exploration—A Review. Audiology Research, 14(1), 96-115. https://doi.org/10.3390/audiolres14010009