Factors Associated with Nursing Interventions for Smoking Cessation: A Narrative Review



Abstract
:1. Introduction
2. Materials and Methods
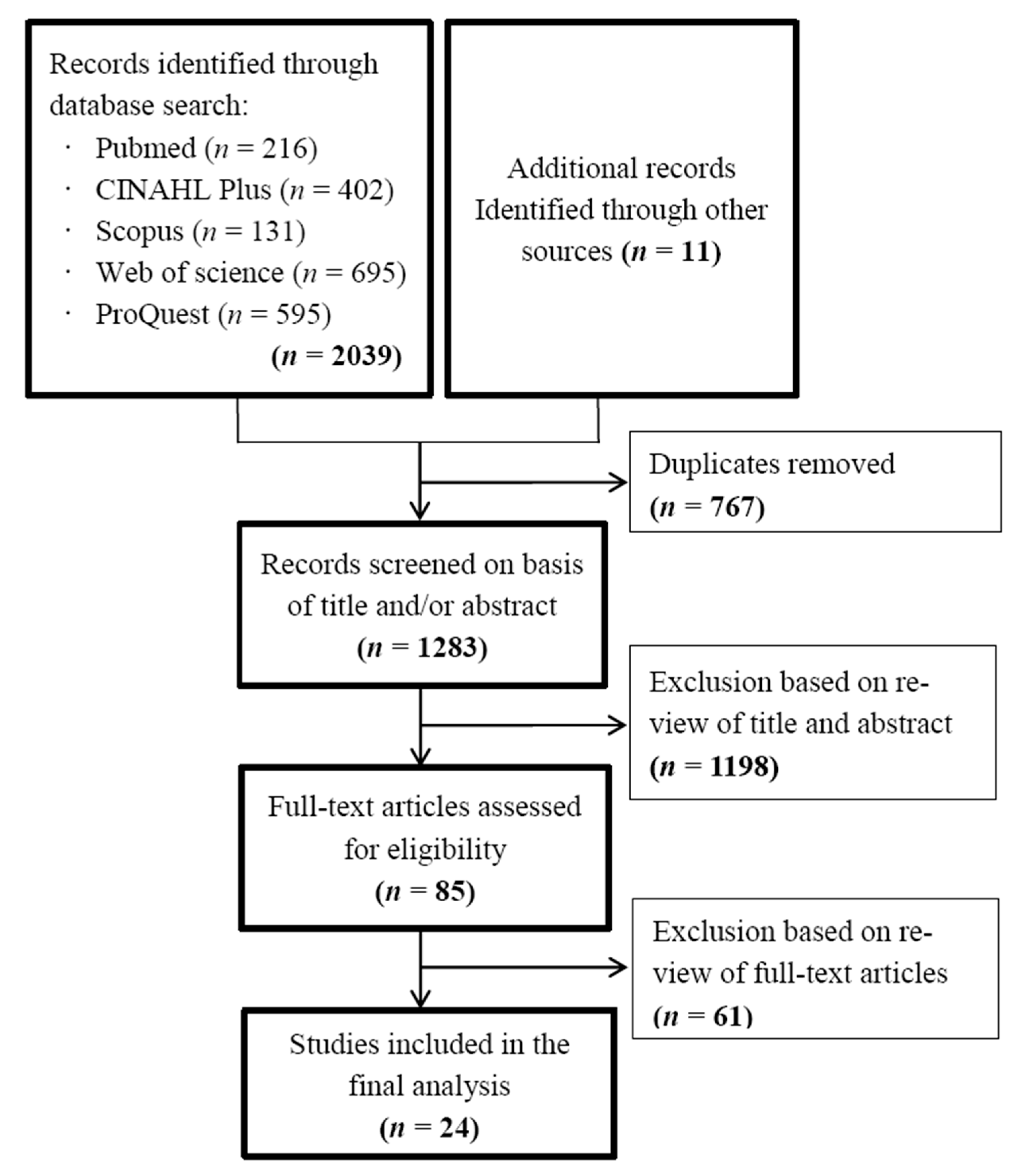
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Extraction
3. Results
3.1. Characteristics of the Included Studies
3.2. Factors Associated with Nursing Interventions for Smoking Cessation
3.2.1. Sociodemographic Factors
3.2.2. Smoking-Related Factors
3.2.3. Motivational Factors
Attitudes or Perceptions on Smoking and Quitting
Social Influence
Self-Efficacy
3.2.4. Enabling Factors and Barriers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Tobacco: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/tobacco (accessed on 24 August 2020).
- The International Council of Nurses (ICN). Tobacco Use and Health. Available online: https://www.icn.ch/sites/default/files/inline-files/A18_Tobacco_Use_Health.pdf (accessed on 27 August 2020).
- Youdan, B.; Queally, B. Nurses’ role in promoting and supporting smoking cessation. Nurs. Times 2005, 101, 26. [Google Scholar] [PubMed]
- Sarna, L.; Bialous, S.A.; Chan, S.S.; Hollen, P.; O’Connell, K.A. Making a difference: Nursing scholarship and leadership in tobacco control. Nurs Outlook. 2013, 61, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Kazemzadeh, Z.; Manzari, Z.S.; Pouresmail, Z. Nursing interventions for smoking cessation in hospitalized patients: A systematic review. Int. Nurs. Rev. 2017, 64, 263–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiore, M.C.; Jaen, C.R.; Baker, T.B.; Bailey, W.C.; Benowitz, N.L.; Curry, S.J.; Dorfman, S.F.; Froelicher, E.S.; Goldstein, M.G.; Healton, C.G.; et al. Treating Tobacco Use and Dependence: 2008 Update; US Dept of Health and Human Services: Rockville, MD, USA, 2008.
- Rice, V.H.; Hartmann-Boyce, J.; Stead, L.F. Nursing interventions for smoking cessation. Cochrane Database Syst. Rev. 2013, 12, CD001188. [Google Scholar] [CrossRef]
- Rice, V.H.; Heath, L.; Livingstone-Banks, J.; Hartmann-Boyce, J. Nursing interventions for smoking cessation. Cochrane Database Syst. Rev. 2017, 12, CD001188. [Google Scholar] [CrossRef]
- Taniguchi, C.; Tanaka, H.; Saka, H.; Oze, I.; Tachibana, K.; Nozaki, Y.; Suzuki, Y.; Sakakibara, H. Changes in self-efficacy associated with success in quitting smoking in participants in Japanese smoking cessation therapy. Int. J. Nurs. Pract. 2018, 24, e12647. [Google Scholar] [CrossRef]
- Sarna, L. Smoking Cessation in Nursing. Available online: https://mdquit.org/providers/nurses (accessed on 17 January 2021).
- De Vries, H.; Mesters, I.; van de Steeg, H.; Honing, C. The general public’s information needs and perceptions regarding hereditary cancer: An application of the Integrated Change Model. Patient Educ. Couns. 2005, 56, 154–165. [Google Scholar] [CrossRef]
- Berndt, N.C.; Bolman, C.; de Vries, H.; Segaar, D.; van Boven, I.; Lechner, L. Smoking cessation treatment practices: Recommendations for improved adoption on cardiology wards. J. Cardiovasc Nurs. 2013, 28, 35–47. [Google Scholar] [CrossRef]
- Smit, E.S.; de Vries, H.; Hoving, C. Determinants of practice nurses’ intention to implement a new smoking cessation intervention: The importance of attitude and innovation characteristics. J. Adv Nurs. 2013, 69, 2665–2674. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.H.; Kim, Y.H. Factors Affecting Korean Registered Nurses’ Intention to Implement Smoking Cessation Intervention. Osong Public Health Res. Perspect. 2016, 7, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Abatemarco, D.J.; Steinberg, M.B.; Delnevo, C.D. Midwives’ knowledge, perceptions, beliefs, and practice supports regarding tobacco dependence treatment. J. Midwifery Womens Health 2007, 52, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, B.; Hecht, J.P.; Papandonatos, G.D.; Emmons, K.M.; Tatewosian, L.R.; Abrams, D.B. Smoking-cessation counseling in the home. Attitudes, beliefs, and behaviors of home healthcare nurses. Am. J. Prev Med. 2001, 21, 272–277. [Google Scholar] [CrossRef]
- Chan, S.S.; Sarna, L.; Wong, D.C.; Lam, T.H. Nurses’ tobacco-related knowledge, attitudes, and practice in four major cities in China. J. Nurs. Sch. 2007, 39, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Chatdokmaiprai, K.; Kalampakorn, S.; McCullagh, M.; Lagampan, S.; Keeratiwiriyaporn, S. Factors Predicting the Provision of Smoking Cessation Services among Occupational Health Nurses in Thailand. Workplace Health Saf. 2017, 65, 253–261. [Google Scholar] [CrossRef]
- Cooke, M.; Mattick, R.P.; Barclay, L. Predictors of brief smoking intervention in a midwifery setting. Addiction 1996, 91, 1715–1725. [Google Scholar] [CrossRef]
- de Ruijter, D.; Smit, E.S.; de Vries, H.; Hoving, C. Dutch practice nurses’ adherence to evidence-based smoking cessation treatment guidelines. Fam. Pract. 2017, 34, 685–691. [Google Scholar] [CrossRef] [Green Version]
- Eiser, J.R.; Main, N.; Lee, A.; Hajek, P. Midwife Attitudes and Advice to Pregnant Smokers. Addict. Res. Theory 1999, 7, 355–368. [Google Scholar] [CrossRef]
- Johnston, J.M.; Chan, S.S.; Chan, S.K.; Lam, T.H.; Chi, I.; Leung, G.M. Training nurses and social workers in smoking cessation counseling: A population needs assessment in Hong Kong. Prev. Med. 2005, 40, 389–406. [Google Scholar] [CrossRef]
- Leung, D.Y.P.; Chan, S.S.; Jiang, C.Q.; Lam, T.H. Providing Smoking Cessation Services and its Relationship with Knowledge and Attitudes: A Comparison of the Guangzhou and Hong Kong Nurses. J. Comp. Asian Dev. 2009, 8, 179–205. [Google Scholar] [CrossRef]
- Mak, Y.W.; Loke, A.Y.; Wong, F.K.Y. Nursing Intervention Practices for Smoking Cessation: A Large Survey in Hong Kong. Int. J. Env. Res. Public Health 2018, 15, 1046. [Google Scholar] [CrossRef] [Green Version]
- McCarty, M.C.; Hennrikus, D.J.; Lando, H.A.; Vessey, J.T. Nurses’ attitudes concerning the delivery of brief cessation advice to hospitalized smokers. Prev. Med. 2001, 33, 674–681. [Google Scholar] [CrossRef] [PubMed]
- McEwen, A.; West, R. Smoking cessation activities by general practitioners and practice nurses. Tob. Control 2001, 10, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Price, J.H.; Jordan, T.R.; Dake, J.A. Perceptions and use of smoking cessation in nurse-midwives’ practice. J. Midwifery Womens Health 2006, 51, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Sarna, L.P.; Brown, J.K.; Lillington, L.; Rose, M.; Wewers, M.E.; Brecht, M.L. Tobacco interventions by oncology nurses in clinical practice: Report from a national survey. Cancer 2000, 89, 881–889. [Google Scholar] [CrossRef]
- Sarna, L.; Bialous, S.A.; Wells, M.; Kotlerman, J.; Wewers, M.E.; Froelicher, E.S. Frequency of nurses’ smoking cessation interventions: Report from a national survey. J. Clin. Nurs. 2009, 18, 2066–2077. [Google Scholar] [CrossRef]
- Sarna, L.; Bialous, S.; Ong, M.; Wells, M.; Kotlerman, J. Nurses’ treatment of tobacco dependence in hospitalized smokers in three states. Res. Nurs. Health 2012, 35, 250–264. [Google Scholar] [CrossRef]
- Sarna, L.P.; Bialous, S.A.; Králíková, E.; Kmetova, A.; Felbrová, V.; Kulovaná, S.; Malá, K.; Roubíčková, E.; Wells, M.J.; Brook, J.K. Tobacco Cessation Practices and Attitudes among Nurses in the Czech Republic. Cancer Nurs. 2015, 38, E22–E29. [Google Scholar] [CrossRef]
- Sarna, L.; Bialous, S.A.; Zou, X.N.; Wang, W.; Hong, J.; Chan, S.; Wells, M.J.; Brook, J. Helping smokers quit: Behaviours and attitudes of Chinese Registered Nurses. J. Adv. Nurs. 2016, 72, 107–117. [Google Scholar] [CrossRef]
- Studts, J.L.; Flynn, S.M.Q.; Dill, T.C.; Ridner, S.L.; Worth, C.T.; Walsh, S.E.; Sorrell, C.L. Nurse Practitioners’ Knowledge, Attitudes, and Clinical Practices Regarding Treatment of Tobacco Use and Dependence. J. Nurse Pract. 2010, 6, 212–219. [Google Scholar] [CrossRef]
- Svavarsdóttir, M.H.; Hallgrímsdóttir, G. Participation of Icelandic nurses in smoking cessation counselling. J. Clin. Nurs. 2008, 17, 1335–1341. [Google Scholar]
- Taniguchi, C.; Hibino, F.; Kawaguchi, E.; Maruguchi, M.; Tokunaga, N.; Saka, H.; Oze, I.; Ito, H.; Hiraki, A.; Nakamura, S.; et al. Perceptions and practices of Japanese nurses regarding tobacco intervention for cancer patients. J. Epidemiol. 2011, 21, 391–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, M.; Cournoyer, D.; O’Loughlin, J. Do the correlates of smoking cessation counseling differ across health professional groups? Nicotine Tob. Res. 2009, 11, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Wetta-Hall, R.; Ablah, E.; Frazier, L.M.; Molgaard, C.A.; Berry, M.; Good, M.J. Factors Influencing Nurses’ Smoking Cessation Assessment and Counseling Practices. J. Addict. Nurs. 2005, 16, 131–135. [Google Scholar] [CrossRef]
- Yankie, V.M.; Price, H.M.; Nanfito, E.R.; Jasinski, D.M.; Crowell, N.A.; Heath, J. Providing smoking cessation counseling: A national survey among nurse anesthetists. Crit. Care Nurs. Clin. North. Am. 2006, 18, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Slater, P.; McElwee, G.; Fleming, P.; McKenna, H. Nurses’ smoking behaviour related to cessation practice. Nurs. Times 2006, 102, 32–37. [Google Scholar] [PubMed]
- Reeve, K.; Adams, J.; Kouzekanani, K. The nurse as exemplar: Smoking status as a predictor of attitude toward smoking and smoking cessation. Cancer Pract. 1996, 4, 31–33. [Google Scholar]
- Duaso, M.J.; Bakhshi, S.; Mujika, A.; Purssell, E.; While, A.E. Nurses’ smoking habits and their professional smoking cessation practices. A systematic review and meta-analysis. Int. J. Nurs. Stud. 2017, 67, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Králíková, E.; Felbrová, V.; Kulovaná, S.; Malá, K.; Nohavová, I.; Roubíčková, E.; Pánková, A.; Bialous, S.A.; Wells, M.J.; Brook, J.; et al. Nurses’ Attitudes toward Intervening with Smokers: Their Knowledge, Opinion and E-Learning Impact. Cent. Eur. J. Public Health 2016, 24, 272–275. [Google Scholar]
- Sarna, L.; Bialous, S.A.; Zou, X.N.; Wang, W.; Hong, J.; Wells, M.; Brook, J. Evaluation of a web-based educational programme on changes in frequency of nurses’ interventions to help smokers quit and reduce second-hand smoke exposure in China. J. Adv. Nurs. 2016, 72, 118–126. [Google Scholar] [CrossRef]
- Sarna, L.; Bialous, S.A.; Wells, M.; Brook, J. Impact of a webcast on nurses’ delivery of tobacco dependence treatment. J. Clin. Nurs. 2018, 27, e91–e99. [Google Scholar] [CrossRef] [Green Version]
- Carson, K.V.; Verbiest, M.E.; Crone, M.R.; Brinn, M.P.; Esterman, A.J.; Assendelft, W.J.; Smith, B.J. Training health professionals in smoking cessation. Cochrane Database Syst. Rev. 2012, 5, CD000214. [Google Scholar] [CrossRef] [PubMed]
- Rezk-Hanna, M.; Sarna, L.; Petersen, A.B.; Wells, M.; Nohavova, I.; Bialous, S. Attitudes, barriers and facilitators to smoking cessation among Central and Eastern European nurses: A focus group study. Eur. J. Oncol. Nurs. 2018, 35, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Thornberry, A.; Garcia, T.J.; Peck, J.; Sefcik, E. Occupational Health Nurses’ Self-Efficacy in Smoking Cessation Interventions: An Integrative Review of the Literature. Workplace Health Saf. 2020, 68, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Banu, M.R. Nurses Attitude and Self-Efficacy in Smoking Cessation Care to Hospitalized Patients. Int. Arch. Subst. Abuse Rehabil. 2018, 1, 1. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Okamoto, R.; Tada, A.; Kiya, M. Factors Associated with Prenatal Smoking Cessation Interventions among Public Health Nurses in Japan. Int. J. Environ. Res. Public Health 2020, 17, 6135. [Google Scholar] [CrossRef]
- Nilsson Kajermo, K.; Alinaghizadeh, H.; Falk, U.; Wändell, P.; Törnkvist, L. Psychometric evaluation of a questionnaire and primary healthcare nurses’ attitudes towards research and use of research fifindings. Scand. J. Caring Sci. 2014, 28, 173–185. [Google Scholar] [CrossRef]


{kind=link}
| Categories | Factors Significantly Associated with Nursing Interventions | Author Year (Reference Number) |
|---|---|---|
| Sociodemographic factors | Gender | Johnston et al. (2005) [22], Leung et al. (2009) [23], Mak et al. (2018) [24], Yankie et al. (2006) [38]. |
| Age | Wetta-Hall et al. (2005) [37], Price et al. (2006) [27], Mak et al. (2018) [24], Leung et al. (2009) [23], Taniguchi et al. (2011) [35], Borrelli et al. (2001) [16] | |
| Work experience | Wetta-Hall et al. (2005) [37], Sarna et al. (2012) [30] | |
| Educational background | Sarna et al. (2000) [28], Sarna et al. (2009) [29], Sarna et al. (2016) [32] | |
| Primary position | Sarna et al. (2000) [28], Sarna et al. (2009) [29], Sarna et al. (2012) [30], Wetta-Hall et al. (2005) [37] | |
| Primary work setting | Sarna et al. (2000) [28], Sarna et al. (2009) [29], Taniguchi et al. (2011) [35], Wetta-Hall et al. (2005) [37] | |
| Work unit | Sarna et al. (2000) [28], McCarty et al. (2001) [25], Sarna et al. (2009) [29], Taniguchi et al. (2011) [35], Mak et al. (2018) [24] | |
| Academic certification | Taniguchi et al. (2011) [35], Sarna et al. (2000) [28] | |
| Level of nursing education | Taniguchi et al. (2011) [35] | |
| Workplace type | Taniguchi et al. (2011) [35] | |
| Region | Eiser et al. (1999) [21], Leung et al. (2009) [23] | |
| State of residence | Sarna et al. (2009) [29] | |
| Smoking-related factors | Smoking status | Sarna et al. (2009) [29], Sarna et al. (2012) [30], Sarna et al. (2015) [31], Svavarsdóttir & Hallgrímsdóttir (2007) [35], Leung et al. (2009) [23], Sarna et al. (2000) [28], Borrelli et al. (2001) [16] |
| Smoking cessation training | Chan et al. (2007) [17], Chatdokmaiprai et al. (2017) [18], Mak et al. (2018) [24], McEwen et al. (2001) [26], Wetta-Hall et al. (2005) [37] | |
| Knowledge on smoking and quitting | Leung et al. (2009) [23], Mak et al. (2018) [24], Yankie et al. (2006) [38] | |
| Exposed to second-hand smoke | Mak et al. (2018) [24] | |
| Family/friend suffering from smoking-related diseases | Mak et al. (2018) [24], Sarna et al. (2000) [28] | |
| Familiar with Tobacco Free Nurses | Sarna et al. )2009) [29] | |
| Clinical practice guideline awareness | Studts et al. (2010) [33], Yankie et al. (2006) [38] | |
| Implementing the 5As including “ask” “advise”, “assess”, “assist” and “arrange” | Sarna et al. (2012) [30] | |
| Perceived severity of tobacco health consequences | Studts et al. (2010) [33] | |
| Pharmacotherapy for smoking cessation | Studts et al. (2010) [33] | |
| Motivational factors | Nurses’ attitude and perceptions on smoking and quitting | Borrelli et al. (2001) [16], de Ruijter et al. (2017) [20], Eiser et al. (1999) [21], Johnston et al. (2005) [22], Leung et al. 2009 [23], Mak et al. (2018) [24], McCarty et al. (2001) [25] |
| Organizational support | Abatemarco et al. (2007) [15], Chatdokmaiprai et al. (2017) [18], Cooke et al. (1996) [19]. | |
| Self-efficacy | Borrelli et al. (2001) [16], Chatdokmaiprai et al. (2017) [18], de Ruijter et al. (2017) [20], Studts et al. (2010) [33], Tremblay et al. 2009 [36]. | |
| Outcome expectations | Borrelli et al. (2001) [16], Price et al. (2006) [27] | |
| Professional norm | Leung et al. (2009) [23], Tremblay et al. (2009) [36], Yankie et al. (2006) [38], Svavarsdóttir & Hallgrímsdóttir 2007 [34]. | |
| Perceived motivation for smokers | Borrelli et al. (2001) [16], Mak et al. (2018) [24] | |
| Perceived efficacy expectations | Price et al. (2006) [27] | |
| Response efficacy–cessation | Studts et al. (2010) [33] | |
| Response efficacy–brief | Studts et al. (2010) [33] | |
| Perceived effectiveness | Borrelli et al. (2001) [16] | |
| Counseling is worthwhile | Yankie et al. (2006) [38] | |
| Interaction between the man and not a duty | Yankie et al. (2006) [38] | |
| Nurses who wanted to receive training | Mak et al. (2018) [24] | |
| Enabling factors and barriers | Ability | Cooke et al. (1996) [19], Johnston et al. (2005) [22], McCarty et al. (2001) [25] |
| Lack of training, time and knowledge | Abatemarco et al. (2007) [15], Svavarsdóttir & Hallgrímsdóttir (2007) [34], de Ruijter et al. (2017) [20], Mak et al. (2018) [24] | |
| Competing priorities in the visit | Abatemarco et al. (2007) [15] | |
| Perceived patient adherence | Borrelli et al. (2001) [16] | |
| Cohesion, work pressure and clarity | Cooke et al. (1996) [19] | |
| Comfort discussing cessation | Studts et al. (2010) [33] | |
| Comfort developing plan | Studts et al. (2010) [33] | |
| Comfort recommending appropriate pharmacological treatments | Studts et al. (2010) [33] | |
| Perceived barriers | Studts et al. (2010) [33] | |
| Only advise if patient asks for information | McCarty et al. (2001) [25] | |
| Possessing skills | Wetta-Hall et al. (2005) [37] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Koide, K.; Tanaka, M.; Kiya, M.; Okamoto, R. Factors Associated with Nursing Interventions for Smoking Cessation: A Narrative Review. Nurs. Rep. 2021, 11, 64-74. https://doi.org/10.3390/nursrep11010007
Li M, Koide K, Tanaka M, Kiya M, Okamoto R. Factors Associated with Nursing Interventions for Smoking Cessation: A Narrative Review. Nursing Reports. 2021; 11(1):64-74. https://doi.org/10.3390/nursrep11010007
Chicago/Turabian StyleLi, Meng, Keiko Koide, Miho Tanaka, Misaki Kiya, and Reiko Okamoto. 2021. "Factors Associated with Nursing Interventions for Smoking Cessation: A Narrative Review" Nursing Reports 11, no. 1: 64-74. https://doi.org/10.3390/nursrep11010007
APA StyleLi, M., Koide, K., Tanaka, M., Kiya, M., & Okamoto, R. (2021). Factors Associated with Nursing Interventions for Smoking Cessation: A Narrative Review. Nursing Reports, 11(1), 64-74. https://doi.org/10.3390/nursrep11010007