
Nurses’ Knowledge and Anxiety Levels toward COVID-19 in Saudi Arabia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample and Setting
2.3. Measures
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
3.1. Participants
3.2. Knowledge Level of Participants
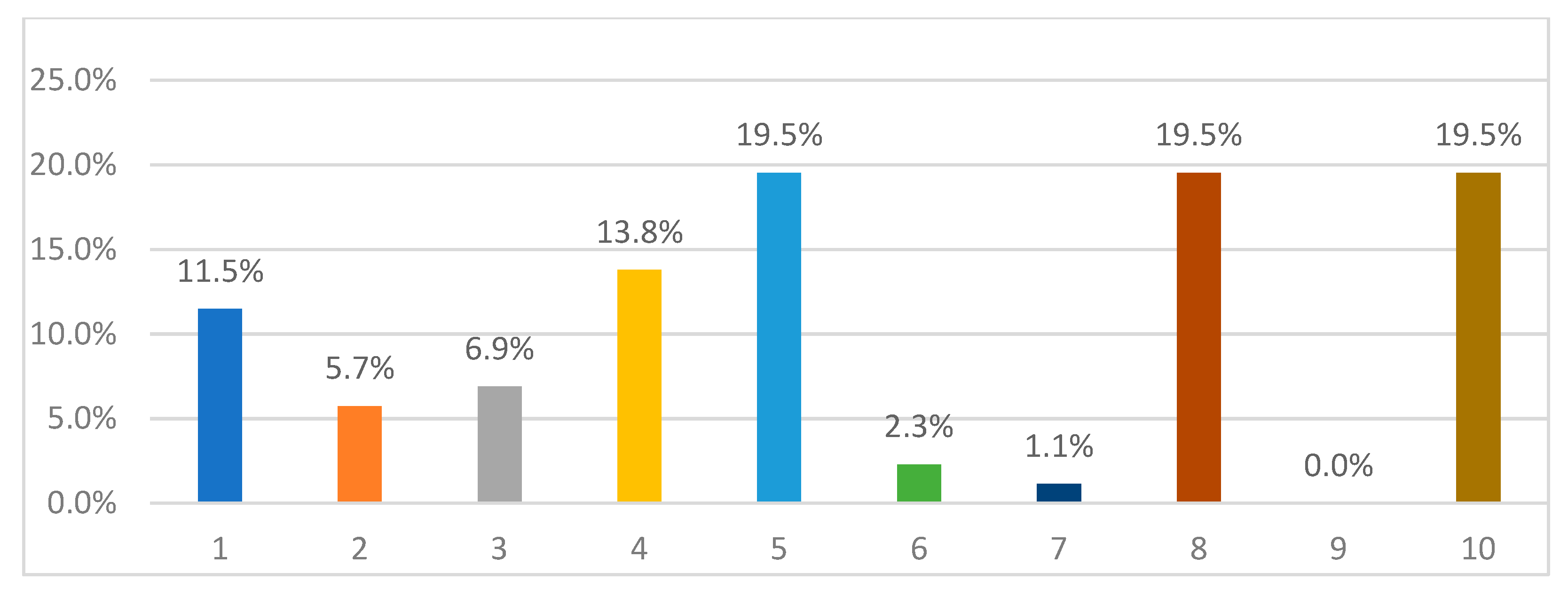
3.3. Level of Anxiety of Participants
3.4. Level of Knowledge and Anxiety of Participants
4. Discussion
5. Limitations
6. Study Implications
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saudi Arabia Announces First Case of Coronavirus REUTERS. Available online: https://www.reuters.com/article/us-health-coronavirus-saudi/saudi-arabia-announces-first-case-of-coronavirus-idUSKBN20P2FK (accessed on 2 January 2021).
- Kang, L.; Li, Y.; Hu, S.; Chen, M.; Yang, C.; Yang, B.X.; Wang, Y.; Hu, J.; Lai, J.; Ma, X.; et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry 2020, 7, e14. [Google Scholar] [CrossRef] [Green Version]
- AlAteeq, D.A.; Aljhani, S.; Althiyabi, I.; Majzoub, S. Mental health among healthcare providers during coronavirus disease (COVID-19) outbreak in Saudi Arabia. J. Infect.Public Health 2020, 13, 1432–1437. [Google Scholar] [CrossRef] [PubMed]
- Arafa, A.; Mohamed, A.; Saleh, L.; Senosy, S. Psychological Impacts of the COVID-19 Pandemic on the Public in Egypt. Community Ment. Health J. 2021, 57, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.Z.; Han, M.F.; Luo, T.D.; Ren, A.K.; Zhou, X.P. Mental health survey of medical staff in a tertiary infectious disease hospital for COVID-19. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2020, 38, 192–195. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health Considerations during the COVID 19 Outbreak; World Health Organization: Geneva, Switzerland, 2020; Available online: https://yotambien.mx/consideraciones-de-la-oms-de-salud-mental-durante-el-brote-de-covid-19/n.d (accessed on 23 March 2020).
- Nemati, M.; Ebrahimi, B.; Nemati, F. Assessment of Iranian nurses’ knowledge and anxiety toward COVID-19 during the current outbreak in Iran. Arch. Clin. Infect. Dis. 2020, 15, e102848. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China: A web-based cross-sectional survey. medRxiv 2020, 288, 112954. [Google Scholar] [CrossRef] [Green Version]
- Alrubaiee, G.G.; Al-Qalah TA, H.; Al-Aawar, M.S.A. Knowledge, attitudes, anxiety, and preventive behaviours towards COVID-19 among health care providers in Yemen: An online cross-sectional survey. BMC Public Health 2020, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, M.U.; Shah, S.; Ahmad, A.; Fatokun, O. Knowledge and attitude of healthcare workers about Middle East Respiratory Syndrome in multispecialty hospitals of Qassim, Saudi Arabia. BMC Public Health 2014, 14, 1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tork, H.M.; Mersal, F.A. Middle East Respiratory Syndrome-Corona virus: Knowledge and attitude of Qassim University students, KSA. Glob. Adv. Res. J. Med. Med. Sci. 2018, 7, 90–97. [Google Scholar]
- Al-Mohaissen, M. Awareness among a Saudi Arabian university community of Middle East respiratory syndrome coronavirus fol-lowing an outbreak. East. Mediterr. Health J. 2017, 23, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Grosso, P.; Loret de Mola, C.; Vega-Dienstmaier, J.M.; Arevalo, J.M.; Chavez, K.; Vilela, A.; Huapaya, J. Validation of the Spanish Center for Epidemiological Studies Depression and Zung Self-Rating Depression Scales: A comparative validation study. PLoS ONE 2012, 7, e45413. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Factor | n | % | |
|---|---|---|---|
| Gender | Male | 5 | 5.7 |
| Female | 82 | 94.3 | |
| Age | 20–25 | 1 | 1.1 |
| 26–30 | 3 | 3.4 | |
| 31–40 | 53 | 60.9 | |
| 41–50 | 23 | 26.4 | |
| 51 and above | 7 | 8.0 | |
| Education level | Nursing diploma | 48 | 55.2 |
| Bachelor’s degree in nursing | 38 | 43.7 | |
| Master’s degree‘ or above | 1 | 1.1 | |
| Work experience | 1–5 years | 6 | 6.9 |
| 5–15 years | 41 | 47.1 | |
| 15–25 years | 31 | 35.6 | |
| More than 25 years | 9 | 10.3 | |
| Yes, n (%) | No, n (%) | |
|---|---|---|
| Been infected with COVID-19 | 3 (3.4%) | 84 (96.6%) |
| Received a COVID-19 diagnostic test | 39 (44.8%) | 48 (55.2%) |
| Descriptive Statistics | |||||
|---|---|---|---|---|---|
| n | Min | Max | Mean | Overall Score | |
| What Is the Rate of Your Anxiety Level about Infection? (1–10) | 87 | 1 | 10 | 5.7011 | 6% |
| Knowledge | 87 | 1 | 18 | 12.9425 | 71.90% |
| Rate Weight | From | To |
|---|---|---|
| 1 | 1 | 1.9 |
| 2 | 1.9 | 2.8 |
| 3 | 2.8 | 3.7 |
| 4 | 3.7 | 4.6 |
| 4 | 4.6 | 5.5 |
| 6 | 5.5 | 6.4 |
| 7 | 6.4 | 7.3 |
| 8 | 7.3 | 8.2 |
| 9 | 8.2 | 9.1 |
| 10 | 9.1 | 10 |
| n | Mean | Std. Deviation | Std. Error | F | Sig. | |
|---|---|---|---|---|---|---|
| Nursing diploma | 48 | 11.7917 | 2.19243 | 0.31645 | 16.523 | <0.01 |
| Bachelor’s degree | 38 | 14.5000 | 2.37953 | 0.38601 | ||
| Master’s degree or above | 1 | 9.0000 | ||||
| Total | 87 | 12.9425 | 2.65609 | 0.28476 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsharif, F. Nurses’ Knowledge and Anxiety Levels toward COVID-19 in Saudi Arabia. Nurs. Rep. 2021, 11, 356-363. https://doi.org/10.3390/nursrep11020034
Alsharif F. Nurses’ Knowledge and Anxiety Levels toward COVID-19 in Saudi Arabia. Nursing Reports. 2021; 11(2):356-363. https://doi.org/10.3390/nursrep11020034
Chicago/Turabian StyleAlsharif, Fatmah. 2021. "Nurses’ Knowledge and Anxiety Levels toward COVID-19 in Saudi Arabia" Nursing Reports 11, no. 2: 356-363. https://doi.org/10.3390/nursrep11020034
APA StyleAlsharif, F. (2021). Nurses’ Knowledge and Anxiety Levels toward COVID-19 in Saudi Arabia. Nursing Reports, 11(2), 356-363. https://doi.org/10.3390/nursrep11020034