
Improving Physical Assessment and Clinical Judgment Skills without Increasing Content in a Prelicensure Nursing Health Assessment Course


Abstract
:1. Introduction
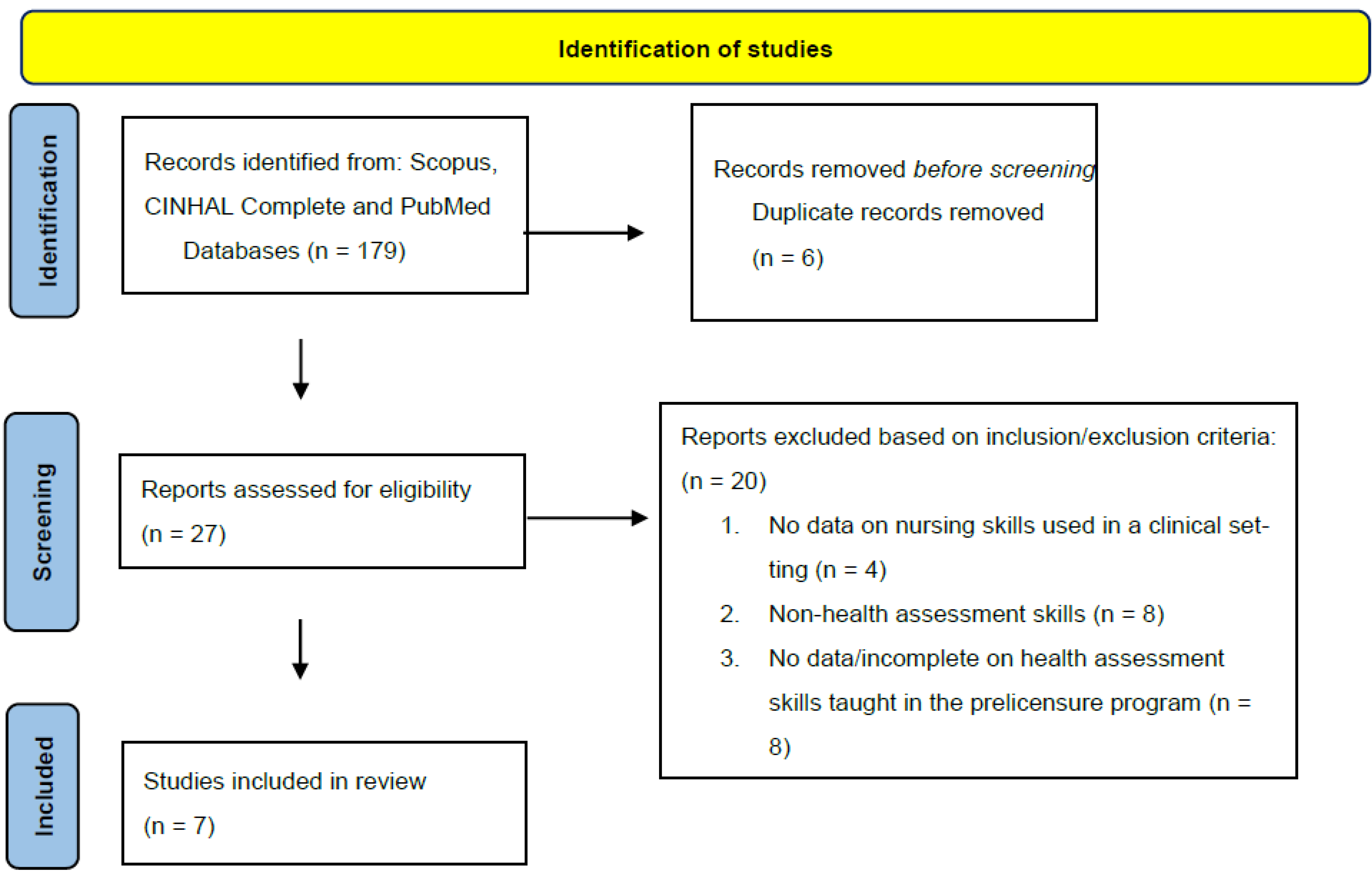
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fusner, S.M.; Moots, H.; O’Brien, T.; Sinnott, L.T. Faculty perceptions of the importance of physical assessment skills taught in pre licensure nursing education. Nurse Educ. 2020, 45, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Tanner, C.A. Thinking like a nurse: A research-based model of clinical judgment in nursing. J. Nurs. Educ. 2006, 45, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Reibel, M.D.; Cason, M.; Screws, S. Creating simulation experience to promote clinical judgment. Teach. Learn. Nurs. 2019, 14, 298–302. [Google Scholar] [CrossRef]
- Dickison, P.; Haerling, K.A.; Lasater, K. Integrating the National Council of State Boards of Nursing Clinical Judgement Model into nursing educational frameworks. J. Nurs. Educ. 2019, 58, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, J.M.; Szweda, C. A crisis in competency: The strategic and ethical imperative to assessing new graduate nurses’ clinical reasoning. Nurs. Educ. Perspect. 2017, 38, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Spectorm, N.; Ulrich, B.T.; Barnsteiner, J. New graduate transition into practice: Improving quality and safety. In Quality and Safety in Nursing: A Competency Approach to Improving Outcomes, 1st ed.; Sherwood, G., Barnsteiner, J., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2012; pp. 267–274. [Google Scholar]
- Murray, M.; Sundin, D.; Cope, V. A mixed-methods study on patient safety insights of new graduate registered nurses. J. Nurs. Care Qual. 2020, 35, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Douglas, C.; Windsor, C.; Lewis, P. Too much knowledge for a nurse? Use of physical assessment by final semester nursing students. Nurs. Health Sci. 2015, 17, 492–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meulenburg, A.N. Shifting the perceptions of error reporting among newly licensed nurses. J. Nurses Prof. Dev. 2020, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Giddens, J.F.; Eddy, L. A survey of physical examination skills taught in undergraduate nursing programs: Are we teaching too much? J. Nurs. Educ. 2009, 48, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.; Nix, E.; Norman, B.; McPike, H.D. An evidence based approach to undergraduate physical assessment practicum course development. Nurse Educ. Pract. 2014, 14, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Kohtz, C.; Brown, S.C.; Williams, R.; O’Connor, P.A. Physical assessment techniques in nursing education: A replicated study. J. Nurs. Educ. 2017, 56, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Morrell, S.; Ralph, J.; Giannotti, N.; Dayus, D.; Dennison, S.; Bornais, J. Physical assessment skills in nursing curricula: A scoping review protocol. Joanna Briggs Inst. 2019, 17, 1086–1091. [Google Scholar] [CrossRef]
- Secrest, J.A.; Norwood BRDuMont, P.M. Physical assessment skills: A descriptive study of what is taught and what is practiced. J. Prof. Nurs. 2005, 21, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Egisdottir, H.O.; Byermoen, K.R.; Moen, A.; Eide, H.E. Revitalizing physical assessment in undergraduate nursing education dash what skills are important to learn, and how are these skills applied during clinical rotation? A cohort study. BMC Nurs. 2019, 18, 41. [Google Scholar] [CrossRef] [Green Version]
- Giddens, J.F. A survey of physical assessment techniques performed by RNs: Lessons for nursing education. J. Nurs. Educ. 2007, 46, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Douglas, C.; Booker, C.; Fox, R.; Windsor, C.; Osborne, S.; Gardner, G. Nursing physical assessment for patient safety in general wards: Reaching consensus on core skills. J. Clin. Nurs. 2016, 25, 1890–1900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birks, M.; Jones, A.; Chung, C.; Davis, J.; Cant, R. The teaching of physical assessment skills in pre-registration nursing programmes in Australia: Issues for nursing educations. Collegian 2014, 21, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.A.; Crookes, P.A.; Iverson, D. An audit of skills taught in registered nursing preparation programmes in Australia. BMC Nurs. 2015, 14, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poje, K. Are We over Teaching Health Assessment at the RN Level? Am. Nurse 2020. Available online: https://www.myamericannurse.com/are-we-over-teaching-health-assessment-at-the-rn-level/ (accessed on 19 February 2020).


{kind=link}
| Essential Skills | Anderson et al. (2014) [11] | Kohtz, et al. (2017) [12] | Giddons, (2007) [16] | Douglas, et al. (2016) [17] | Egilsdottir, et al. (2019) [15] | Birks, et al. (2014) [18] | Secrest et al. (2005) [14] |
|---|---|---|---|---|---|---|---|
| Vital Signs | |||||||
| Assess pain | X | ||||||
| BP | X | X | |||||
| RR | X | X | |||||
| HR | X | X | X | ||||
| Sa02 | X | X | |||||
| Body temp | X | ||||||
| Weight | X | ||||||
| Height | X | ||||||
| Integumentary | |||||||
| Inspect skin color | X | X | X | X | X | X | |
| Skin lesions | X | X | X | X | X | X | |
| Skin wounds | X | X | X | X | X | X | |
| Estimate skin fold | X | ||||||
| Head: | |||||||
| Inspect facial structures | X | X | X | X | |||
| Oral cavity | X | X | X | X | X | ||
| Ears: | |||||||
| Assess hearing based on conversation | X | X | X | X | X | ||
| Eyes: | |||||||
| Inspect external eyes | X | X | X | X | X | X | |
| Visual acuity | X | X | X | X | |||
| PERRLA | X | X | X | X | X | X | |
| Thorax: | |||||||
| Inspect chest shape | X | X | X | X | X | X | |
| Breathing effort | X | X | X | X | X | ||
| Palpate chest wall expansion | X | X | X | ||||
| Auscultate breath sounds | X | X | X | X | X | X | X |
| Ability to cough | |||||||
| Percuss lungs | X | X | X | ||||
| Abdomen: | |||||||
| Inspect abdomen | X | X | X | X | X | X | X |
| Auscultate bowel sounds | X | X | X | X | X | X | X |
| Palpate for tenderness/distention | X | X | X | X | X | X | X |
| Assess stool | X | X | X | X | |||
| Percuss abdomen | |||||||
| Cardiovascular: | |||||||
| Inspect cap refill | X | X | X | X | X | X | X |
| Palpate distal pulses | X | X | X | X | X | X | X |
| Inspect/palpate edema | X | X | X | X | X | X | X |
| Palpate extremities temp | X | X | X | X | X | X | |
| Inspect extremities for color and hair growth | X | X | X | X | X | X | X |
| Auscultate carotid artery | X | X | |||||
| Inspect jugular pulsation | X | X | X | X | X | X | X |
| Auscultate heart sounds | X | ||||||
| Musculoskeletal: | |||||||
| Inspect back/Spine | X | X | X | ||||
| Inspect muscles/extremities size/symmetry | X | X | X | X | |||
| Palpate extremities/joints/calve for tenderness | X | X | X | X | X | ||
| Observe ROM | X | X | X | X | X | X | |
| Assess muscle strength | X | X | X | X | X | X | X |
| Neurological: | |||||||
| Assess mental/LOC | X | X | X | X | X | ||
| Glascow Coma Scale | X | X | X | ||||
| Evaluate speech | X | X | X | X | X | ||
| Facial movement/sensation | X | X | X | X | X | ||
| Assess gait | |||||||
| CN I-XII | X | X | X | X | X | X | |
| Patella/Planter reflex | X | ||||||
| Gag reflex | X | X | |||||
| Total Skills | 34 | 28 | 30 | 32 | 30 | 36 | 19 |
| Skills | HEENT | Cardiovascular | Thorax | Neurological | Abdomen | Musculoskeletal |
|---|---|---|---|---|---|---|
| Decreased by | 74% | 39% | 30% | 58% | 73% | 74% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinyon, K.; D’Alton, S.; Poston, K.; Navarrete, S. Improving Physical Assessment and Clinical Judgment Skills without Increasing Content in a Prelicensure Nursing Health Assessment Course. Nurs. Rep. 2021, 11, 600-607. https://doi.org/10.3390/nursrep11030057
Kinyon K, D’Alton S, Poston K, Navarrete S. Improving Physical Assessment and Clinical Judgment Skills without Increasing Content in a Prelicensure Nursing Health Assessment Course. Nursing Reports. 2021; 11(3):600-607. https://doi.org/10.3390/nursrep11030057
Chicago/Turabian StyleKinyon, Kathryn, Shannon D’Alton, Kristen Poston, and Sarah Navarrete. 2021. "Improving Physical Assessment and Clinical Judgment Skills without Increasing Content in a Prelicensure Nursing Health Assessment Course" Nursing Reports 11, no. 3: 600-607. https://doi.org/10.3390/nursrep11030057
APA StyleKinyon, K., D’Alton, S., Poston, K., & Navarrete, S. (2021). Improving Physical Assessment and Clinical Judgment Skills without Increasing Content in a Prelicensure Nursing Health Assessment Course. Nursing Reports, 11(3), 600-607. https://doi.org/10.3390/nursrep11030057