1. Introduction
Sleep and rest are fundamental physiological needs of humans. Indeed, adequate sleep provides the recovery and maintenance of energy, efficiently improves physical and intellectual functions, and promotes well-being and emotional balance [
1]. Nurses, among all healthcare professionals, are particularly exposed to sleep disturbances [
2] and insomnia for the changes in sleep–wake rhythm due to the variation in working hours, covering 24 h shifts (namely morning, afternoon, and night shifts) [
3,
4], heavy workloads, the emotional and psychological impact that some clinical settings can exert [
5], and the occurrence of burnout [
6,
7], as well as the physiological process of decreased sleep hours, not to mention increased sleep fragmentation due to aging [
8].
According to a recent meta-analysis, the prevalence of sleep disturbances in Chinese nurses was 45.1% (CI 95%: 37.2–53.1%) [
9], while Ielapi et al. reported a prevalence of 65.4% [
10]. Sleep disturbances can influence personal well-being and mental health, also causing depression [
11], which has been reported in 60.3% of cases [
12]. Furthermore, observational research has shown that a reduction in the time dedicated to sleep is associated with decreased productivity [
13], quality of care, and patient safety [
14]. These features took on particularly important aspects during the first waves of COVID-19 pandemic. Pooled data from 44 meta-analyses showed that the prevalence of sleep disturbance reported among hospital healthcare workers during the first waves of the COVID-19 pandemic was 40% (CI 95%: 36.9% to 42.0%) [
15]. Moreover, in a meta-analysis published in 2020, nurses accounted for 34.8% of sleep disturbance (CI 95%: 24.8–46.4%) [
16]. The literature also reports the deterioration of healthcare workers’ psychological and emotional status due to anxiety, fear, depression, and fatigue [
17,
18,
19,
20].
In addition to the worsening of sleep quality, other psychological conditions negatively affected nurses operating in COVID-19 hospital areas, namely a pooled prevalence of anxiety at 16–41%, depression at 14–37%, and stress/post-traumatic stress disorder at 18.6–56.5% were reported in a recent meta-review of systematic reviews about the mental health status of healthcare professionals during the COVID-19 pandemic [
21].
Anxiety was reported in percentages varying from 20% to 72% among healthcare professionals working in first-line COVID-19 settings in many countries [
22]. Moreover, anxiety has been shown to affect nurses’ ability to relax and obtain adequate quality of sleep, thus presenting a significant risk factor for insomnia [
23,
24]. During the first wave of COVID-19, high levels of anxiety were registered among all healthcare professionals, especially nurses, due not only to the novelty of the SARS-CoV2 infective threat but also to the lack of personal protective equipment (PPE) and training, fatigue due to the wearing of PPE for many consecutive hours, and the absence of a vaccine that could have protected first-line operators [
25,
26,
27].
However, the way nurses faced this global emergency showed the presence of psychological points of strength, identified in the concept of resilience [
28], which was positively related to the quality of general life and working life [
29,
30] and showed negative correlations with depression and burnout while mitigating the effect of pandemic fatigue on mental health and sleep quality [
31,
32,
33,
34].
When dealing with resilience, we should remember that it has a fundamental antecedent, represented by hardiness, a multifaceted behavioral approach characterized by three components: (i) commitment: the motivation to engage fully in one’s work and personal life, even in the face of adversity; (ii) control: the belief that one can influence outcomes via one’s actions and efforts; and (iii) challenge: the view that change and adversity are opportunities for growth and development [
35,
36,
37,
38]. This represents a very important behavioral trait, as adequate levels of hardiness allow individuals to face challenging and dangerous situations by showing the ability to counterbalance the negative emotional and psychological effects of catastrophic conditions and to be prepared to face life challenges. Previous studies have shown a relationship between hardiness levels and anxiety in nurses employed as first-line healthcare providers during the first wave of the COVID-19 pandemic [
39]. However, to date, scientific literature has not analyzed the influence of hardiness on insomnia levels in nurses. Therefore, we designed a study to identify the relationship between insomnia, anxiety, and hardiness in a cohort of nurses working in hospital and out-of-hospital clinical settings during the first wave of the COVID-19 pandemic. Therefore, the primary aim of this study was to describe the insomnia levels of Italian nurses during the first wave of the COVID-19 pandemic, specifically those involved in the care of COVID-19 patients. The secondary aim was to determine the effect of hardiness and anxiety levels on the occurrence of insomnia as well as the associated risk and promoting factors.
3. Results
A cohort of 1693 healthcare providers, of which 1354 were nurses, were included in the original AIR-COVID-19 study. In the current study, 1167 nurses filled out the questionnaire regarding insomnia, thus maintaining 86.2% (1167/1354 nurses) of respondents (81.2 % women—4948/1167), with a mean age of 42.4 (SD ± 10.7) years (CI 95% 41.7–43.0) and a mean length of service of 17.9 ± 11.6 years (CI 95% 17.2–18.6).
As a consequence of the COVID-19 pandemic, nurses were reallocated to another unit in 27.8% (324/1167) of cases, and 33.6% (109/324) were transferred to a COVID-19 unit. Transferees reported an average positive satisfaction rate of 78.4%. Moreover, 383 out of 1167 (32.8%) nurses reported caring for COVID-19 patients (784/1167 did not). The perception of being adequately provided with personal protective equipment (PPE) was also assessed, and 52.1% (608/1167) reported satisfaction. Results reported in
Table 1 show that nurses who served in COVID-19 wards were significantly younger (40.9 ± 10.3 vs. 43.1 ± 10.8;
p < 0.001) and with lower seniority (16.6 ± 11.3 vs. 18.5 ± 11.7;
p < 0.01) when compared to nurses not involved in caring for COVID-19 patients. As for other characteristics, such as the transfer of department, its evaluation, and the perception of being provided with adequate PPE, no statistically significant differences between the two groups were reported (
Table 1).
As for the state and trait anxiety values, the nurses enrolled in the study reported values of 47.0 ± 12.4 and 42.6 ± 10.1, respectively, meaning that both the state (48.8 ± 12.5 vs. 46.1 ± 12.2;
p < 0.001) and trait (43.5 ± 10.0 vs. 42.2 ± 10.2;
p < 0.05) anxiety levels were significantly higher in the group of nurses caring for COVID-19 patients (
Table 2).
As for insomnia levels, the descriptive results in
Table 3 show that similar percentages reported no clinically significant insomnia in either group (57.5% nurses caring for COVID-19 patients and 58.8% of those who did not) before the beginning of the pandemic, while after the first wave, sub-threshold and clinical insomnia were more represented, showing a shift of respondents from the first group before the beginning of the pandemic to the other three groups after the first wave of the pandemic (
Table 3).
Moreover, pre-score insomnia levels were lower than post-score levels, meaning that insomnia levels worsened after the first COVID-19 pandemic wave in the whole sample and in both groups of nurses. However, our data showed significant differences between the two groups of nurses in post- and delta insomnia scores (
Table 4).
Hardiness levels (measured by DRS total) showed lower values after the first wave of the pandemic than before the beginning of the pandemic for both groups of nurses, as reported in
Table 4. No statistically significant differences in hardiness levels (total, control, challenge, and commitment) assessed before the beginning of the pandemic were reported in the groups of nurses, whereas statistically significant differences between the groups were reported for total hardiness and challenge levels assessed after the first wave of the pandemic (
p < 0.05).
Regarding hardiness delta levels (post–pre), our data showed negative scores for the hardiness total (−1.3 ± 5.1; CI 95% −1.6; −1.0; p < 0.01) and all subscales, indicating that hardiness levels decreased after the first wave of the pandemic, and all the scores showed statistically significant differences between the two groups of nurses (p < 0.05).
Regarding the inferential analysis assessing the correlation between insomnia levels and other variables, no significant differences were found in relation to gender, age, or length of service in the entire sample of nurses after the first wave of the COVID-19 pandemic. However, insomnia levels were directly and significantly correlated with anxiety trait–state levels (
p ≤ 0.05) and inversely and significantly correlated with hardiness levels (total and subscales) (
p ≤ 0.05) (
Table 5).
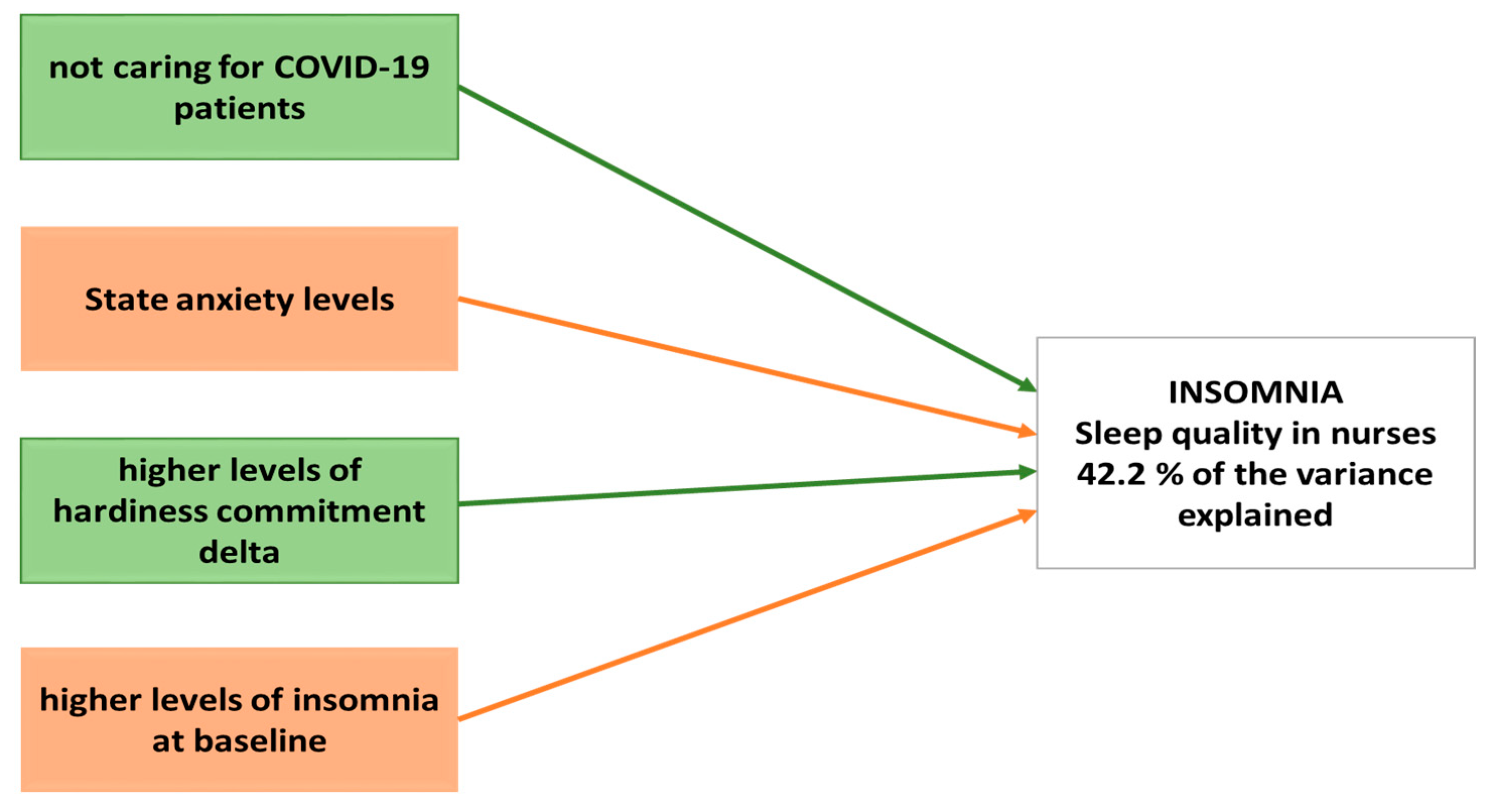
Finally, a generalized linear model was used to calculate the best predictive model for insomnia levels among nurses during the first wave of the COVID-19 pandemic. Our results showed that 42.2% of the variance was explained by four variables: (i) not caring for COVID-19 patients, (ii) higher levels of hardiness commitment delta, (iii) state anxiety, and (iv) higher levels of insomnia at baseline. Indeed, the general linear model takes the original level of insomnia into account, clearly demonstrating that greater initial insomnia results in a lower possibility of symptom progression or deterioration (
Table 6 and
Figure 1).
4. Discussion
Our results show that insomnia levels referred to by the participants before the beginning of the pandemic were above the average of general population; however, insomnia levels increased further after the first wave of the pandemic. Moreover, anxiety levels also increased due to the pandemic and were directly and significantly associated with insomnia levels. In particular, our results show a statistically significant difference, not only before and after the first wave of the pandemic, but also in the two subgroups considered, i.e., those nurses who were caring for COVID-19 patients and those who were not. Finally, dispositional resilience plays a pivotal role in the final score of insomnia levels, depending on low scores (risk factors) or high scores (promoting factor).
In our previous study, we analyzed the promotive and risk factors of hardiness levels in nurses involved in the care of COVID-19 patients, showing that length of service, positive evaluation of department reallocation, and, surprisingly, inadequate PPE when considering a positive assessment of department reallocation constituted promotive factors [
39]. The risk factors for the worsening of hardiness levels were anxiety alone, the association of anxiety with length of service, the negative assessment of department reallocation, and the evaluation of insufficient PPE when associated with a negative assessment of department reallocation [
39]. Thus, in the present study, we focused on the insomnia and sleep quality of nurses, and any differences were revealed between the beginning of the pandemic and after the first wave of the pandemic.
Several studies on mental distress in healthcare workers were conducted during the first wave of the COVID-19 pandemic (from March to May 2020); however, studies carried out during subsequent waves showed similar outcomes, either demonstrating that different regions were hit harder by the pandemic during different periods or highlighting the persistence of the pandemic and the subsequent impact on nurses’ mental health status [
16]. Likewise, in accordance with our previous results on hardiness, a systematic review by García-Vivar et al. highlighted the mental health effects on nurses working in different parts of the world during the COVID-19 pandemic [
50]. Indeed, the authors claim that nurses, among all healthcare workers, reported the highest levels of psychological distress because of their working conditions, which worsened when they were female and lacked access to PPE [
50]. Accordingly, in our study, the group of nurses caring for COVID-19 patients reported significantly higher values for state and trait anxiety levels than those who did not, indicating that the impact of the COVID-19 pandemic played an important role in nurses’ anxiety. In addition, insomnia levels were directly correlated with anxiety trait levels.
Moreover, a study conducted in Italy by Simonetti et al. (2021) reported the worst outcomes compared with similar studies included in the systematic review by García-Vivar et al., with 75.72% of nurses reporting poor sleep quality (data collected from February to April 2020) [
50,
51]. Accordingly, all the included studies examining sleep quality described overall negative outcomes and a high prevalence of sleep disturbances in nurses. In addition, independent of the COVID-19 pandemic, nurses are at a high risk of insomnia, as reported in a systematic review by Booker et al. (2018) [
52]. Indeed, our results on insomnia levels showed similar baseline percentages in both groups (57.5% nurses caring for COVID-19 patients and 58.8% of nurses not caring for COVID-19 patients), with a shift towards sub-threshold and clinical insomnia immediately after the first wave of the pandemic, highlighting the worsening of sleep quality and disturbances (as shown in
Table 3). Liu et al. (2020) [
53] in their cross-sectional study reported that the percentage of medical staff who suffered from insomnia in China was 32.0%, lower than similar previous studies but higher than the 30.5% prevalence of insomnia in non-medical personnel under the COVID-19 epidemic [
54]. Italian nurses participating in the study reported higher ISI scores (more than 55%) for insomnia, which is likely due to the fact that at the start of the COVID-19 outbreak, Italy was the first European country affected, and due to the unpreparedness of the national health system, medical staff lacked PPE and knowledge of the disease, which increased their anxiety, fear, and insomnia.
Furthermore, in our sample, pre-score insomnia levels were lower than post-score levels, indicating that insomnia levels worsened after the first COVID-19 pandemic wave in the whole sample of nurses, with statistically significant differences between the two groups in the post- and delta scores (as shown in
Table 4); that is, nurses caring for COVID-19 patients reported worse levels. Surprisingly, Nashwan et al., in their cross sectional study on 200 nurses in Qatar, reported no statistically significant differences between COVID-19 and non-COVID-19 facilities for insomnia levels; we assume that these results could be influenced and explained either by the nursing management support of nurses or the rapid adaptation to the pandemic condition [
55].
Moreover, despite the number of published papers to date, only one study has dealt with the correlation between psychological hardiness and insomnia in nurses during the COVID-19 pandemic [
56]. However, hardiness [
57] is a critical trait for nurses, who face several challenges and stressors during their work shifts. Nurses who show higher levels of hardiness are better equipped to cope with these challenges while maintaining their well-being.
As for hardiness levels, lower values were reported after the first wave of the COVID-19 pandemic for both groups of nurses, with statistically significant differences between the groups only for total hardiness and challenge. Similarly, hardiness levels decreased after the first wave of the pandemic, and all scores showed statistically significant differences between the two groups of nurses. Insomnia levels were inversely correlated with hardiness levels.
When dealing with sleep quality, we should remind the reader that an important relationship between mental health distress, namely sleep quality, and burnout has previously been demonstrated in nurses [
6]. Indeed, a recent systematic review and meta-analysis suggested that a considerable proportion of healthcare workers experienced mood and sleep disturbances, especially due to the pandemic, stressing the need to establish ways to mitigate mental health risks and deliver appropriate interventions [
56]. In fact, high work pressure and uncertainty about the risks of COVID-19 increased nurses’ anxiety, depression, post-traumatic stress disorder [
58], emotional exhaustion [
59], and burnout [
32] rates.
Considering this, our study confirms that hardiness represents one of the most important factors to consider and implement as a risk factor (when displaying low values) or a promotive factor (when displaying high values) for insomnia and sleep quality [
59].
Thus, a predictive model was developed using a generalized linear model that showed 42.2% of the variance was explained by four variables: not caring for COVID-19 patients, higher levels of hardiness commitment delta, state anxiety, and higher levels of insomnia at baseline. Clearly, the baseline insomnia score is taken into account, providing validity to greater initial insomnia, resulting in the possibility of symptom progression or deterioration; thus, strategies based on sleep hygiene should always be implemented to enhance sleep quality at all times, not only in the case of catastrophic events. However, the high pre-pandemic insomnia level as a protective factor can be counterintuitive and might merit further investigation to confirm this conclusion.
Our study is not without limitations; in fact, we are well aware that the online survey performed after the first wave of the pandemic in Italy questioned our respondents about how they felt before the beginning of the pandemic: this aspect may be affected by a recall bias, as the data are based on respondents’ memory and experience. We cannot exclude the presence of a self-selection bias, which is typical in survey design research.
In conclusion, the assessment of hardiness as a behavioral trait in healthcare professionals, especially nurses, might be useful to identify individuals with low or high scores and optimize the allocation of human resources by nurse managers. The experience of the COVID-19 pandemic has taught us that it is mandatory to prioritize healthcare professionals’ wellbeing during high-stress periods due to hard working conditions and high workload. Thus, it is necessary to design further studies to identify additional risk factors for poor sleep quality and to develop educational courses and strategies aimed at enhancing rest and sleep quality, especially for frontline nurses.


 ,
, 

{kind=link}