
Men in Mental Health: A Scoping Review of Challenges, Contributions, and Future Possibilities of Recruiting into Nursing

 , , , , and
, , , , and 
Abstract
:1. Introduction
1.1. Background
1.2. Problem Statement
1.3. Aim
1.4. Objectives
- To identify the characteristics, qualities, and attributes of men working as nurses within the mental health setting.
- To identify the factors that encourage and/or discourage the attraction and retention of men working as nurses within the mental health setting.
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
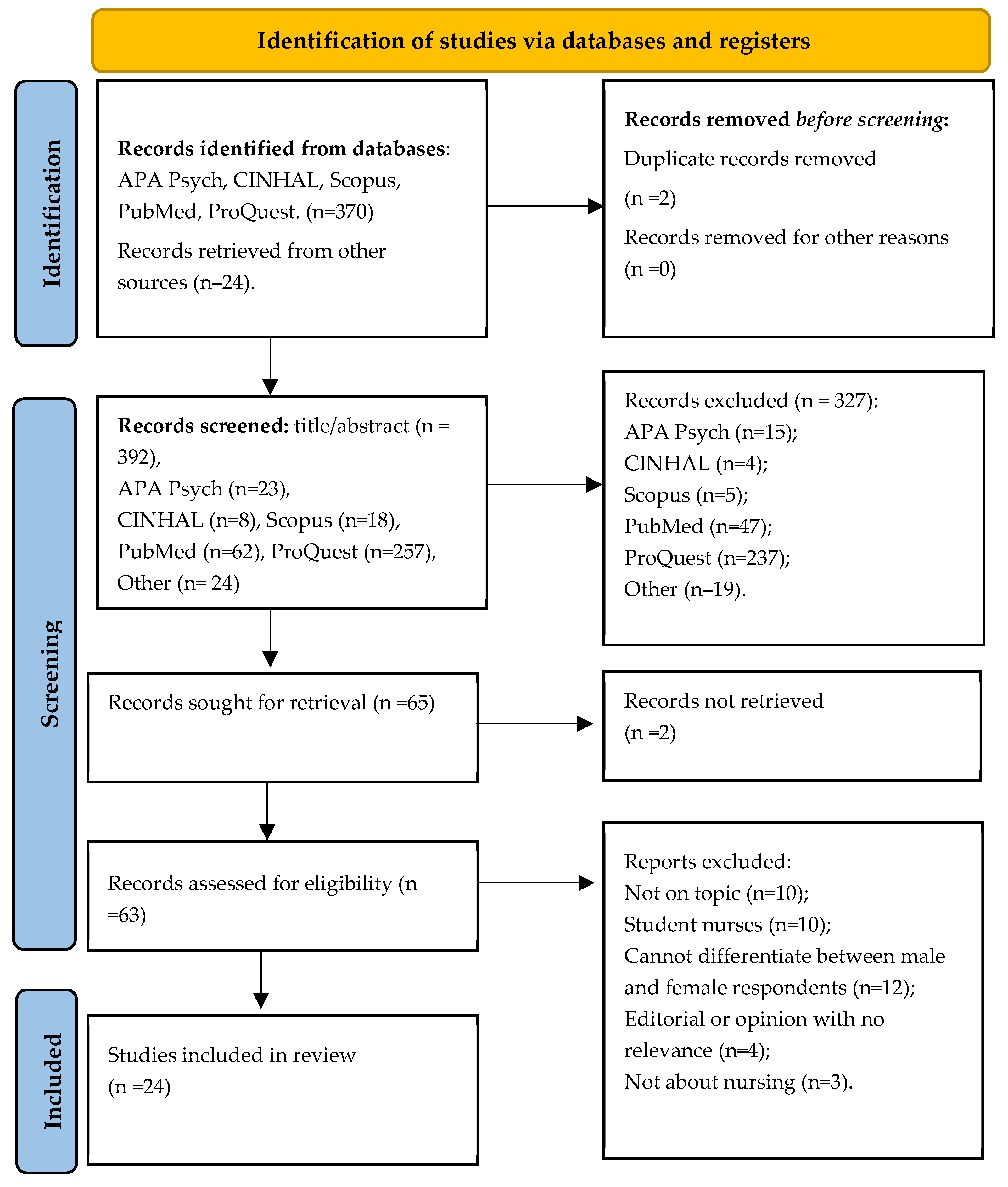
2.3. Study Screening
2.4. Data Extraction and Analysis
3. Results
3.1. Characteristics, Qualities, and Attributes of Male Mental Health Nurses
3.2. Why Men Are Attracted and Stay in Mental Health Nursing
3.3. Why Men Leave Mental Health Nursing
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
Appendix A
Appendix A.1. APA Psych Info (EBSCOHOST) Search
- Conducted on 31 August 2024
- Date limit: 1970 upward
- Other limits: peer reviewed, English language, full text

{kind=link}
| No | Query | Results |
|---|---|---|
| #1 | male AND (nurs* OR nursing) | 12,213 |
| #2 | #1 AND mental health | 205 |
| #3 | #1 AND (mental health OR “psychiatric unit”) | 1648 |
| #4 | #1 AND (mental health OR “psychiatric unit” OR mental asylum) | 1906 |
| #5 | #4 AND career | 1651 |
| #6 | #5 AND retention | 1648 |
| #7 | male AND nurs* AND (mental health OR “psychiatric unit”) AND career AND retention OR attrition. Today’s number for this search = 30. | 7443 |
| #8 | #5 AND (retention OR attrition) AND experience | 2496 |
| #9 | #1 AND (“mental health” OR “psychiatric unit” OR mental asylum) AND career AND (retention OR attrition) AND experience | 2481 |
| #10 | #1 AND (“mental health” OR “psychiatric unit” OR mental asylum) AND career AND retention AND experience | 1633 |
| #11 | #1 AND (“mental health” OR “psychiatric unit” OR mental asylum) | 1891 |
| #13 | “male nurs* AND (mental health nurs* OR psychiatric nurs*) AND (“mental health hospital” OR “psychiatric hospital”) | 23 |
Appendix A.2. CINAHL Search
- CINAHL search conducted on 25 August 2024
- Date limit: 1970 upward
- Other limits: English language, full PDF
| No | Query | Results |
|---|---|---|
| #1 | Male AND (nursing OR nurs*) | 60,293 |
| #2 | #1 AND mental health | 3687 |
| #3 | #2 AND career | 96 |
| #4 | #3 AND retention | 11 |
| #5 | #4 AND attrition | 11 |
| #6 | #5 AND experience | 10 |
Appendix A.3. PubMed Search
- PubMed search conducted on 25 August 2024
- Date limit: 1970–2023
- Other limits: full PDF, English language
| No | Query | Results |
|---|---|---|
| #1 | Male AND (nurs* OR nursing) AND mental health | 17,704 |
| #2 | Male AND (nurs* OR nursing) AND (mental health OR “psychiatric unit”) | 19,670 |
| #3 | Male AND (nurs* OR nursing) AND (mental health OR “psychiatric unit” OR mental asylum) | 52,085 |
| #4 | 3 AND career | 62 |
| #5 | 4 AND retention | 7 |
| #6 | 3 AND (career OR retention) | 7968 |
| #7 | 6 AND experience | 830 |
Appendix A.4. SCOPUS Search
- SCOPUS search conducted on 25 August 2024
- Date limit: 1970 upward
- Other limits: English language, full PDF
| No | Query | Results |
|---|---|---|
| #1 | male AND (nursing OR nurs*) | 151,646 |
| #2 | #1 and mental health | 13,865 |
| #3 | #2 AND career | 239 |
| #4 | #3 AND retention | 24 |
| #5 | #3 AND (retention OR attrition) | 27 |
| #6 | #5 AND experience | 18 |
Appendix A.5. PROQUEST Search
- PROQUEST search conducted on 23 January 2025
- Date limit: 1970 upward
- Other limits: Journals and theses/dissertations, English language
| No | Query | Results |
|---|---|---|
| #1 | male nurse | 703,902 |
| #2 | “male nurse” | 5503 |
| #3 | male NEAR/5 nurse | 26,609 |
| #4 | (male OR men OR man) NEAR/5 nurs* | 187,685 |
| #5 | #4 TI OR AB | 3345 |
| #6 | “psychiatric hospital” | 59,013 |
| #7 | Psychiatric unit | 453,878 |
| #8 | “Mental hospital” | 30,674 |
| #9 | “Mental institution” | 9433 |
| #10 | AND (hospital OR institution OR unit OR asylum) | 2,702,157 |
| #11 | (psychiatric OR mental OR insane) in TI OR AB | 576,242 |
| #12 | #10 TI OR AB | 117,452 |
| #13 | #5 AND #12 | 1062 |
| #14 | abstract((male OR men OR man) NEAR/5 nurs* NOT student) OR title((male OR men OR man) NEAR/5 nurs* NOT student) | 2784 |
| #15 | #13 AND #14 | 117 |
| #16 | #15 AND (career OR retention OR attrition) | 35 |
| #17 | #11 AND #14 | 259 |
References
- World Health Organization. Mental Health. 2024. Available online: https://www.who.int/health-topics/mental-health#tab=tab_1 (accessed on 20 December 2024).
- International Council of Nurses. The Global Mental Health Nursing Workforce: Time to Prioritise and Invest in Mental Health and Wellbeing. 2022. Available online: https://www.icn.ch/sites/default/files/2023-04/ICN_Mental_Health_Workforce_report_EN_web.pdf (accessed on 20 December 2024).
- Turale, S.; Nantsupawat, A. Clinician mental health, nursing shortages and the COVID-19 pandemic. Int. Nurs. Rev. 2021, 68, 12–14. [Google Scholar] [CrossRef] [PubMed]
- Evans, J. Men nurses: A historical and feminist perspective. J. Adv. Nurs. 2004, 47, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, C. A historical study of men in nursing. J. Adv. Nurs. 1997, 26, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Nolan, P. A History of Mental Health Nursing; Nelson Thornes: Oxford, UK, 1998. [Google Scholar]
- Evans, K.; Nizette, D.; O’Brien, A. Psychiatric and Mental Health Nursing, 4th ed.; Elsevier: Chatswood, NSW, Australia, 2017. [Google Scholar]
- Boling, A. The Professionalization of Psychiatric Nursing: From Doctors’ Handmaidens to Empowered Professionals. J. Psychosoc. Nurs. Ment. Health Serv. 2003, 41, 26–40. [Google Scholar] [CrossRef]
- Chatterton, C. Mental health nursing—An overview of its development. Br. J. Healthc. Assist. 2012, 6, 612–617. [Google Scholar] [CrossRef]
- Boschma, G. The Rise of Mental Health Nursing: A History of Psychiatric Care in Dutch Asylums 1890–1920; Amsterdam University Press: Amsterdam, The Netherlands, 2003. [Google Scholar] [CrossRef]
- Peplau, H. Some Reflections on Earlier Days in Psychiatric Nursing. J. Psychosoc. Nurs. Ment. Health Serv. 1982, 20, 17–24. [Google Scholar] [CrossRef]
- Clarke, L. Ideological themes in mental health nursing. In Ethical Issues in Mental Health; Barker, P., Baldwin, S., Eds.; Springer Science + Business Media: Dordrecht, The Netherlands, 1991; pp. 27–44. Available online: https://link.springer.com/chapter/10.1007/978-1-4899-3270-9_3 (accessed on 16 February 2025).
- Nolan, P. Mental health Nursing in the 1950s and 1960s revisited. J. Psychiatr. Ment. Health Nurs. 2020, 4, 333–338. [Google Scholar] [CrossRef]
- Martyr, P. A lesson in Vigilance? Mental Health Nursing Training in Western Australia. Issues Ment. Health Nurs. 2010, 31, 1903–1958. [Google Scholar] [CrossRef]
- Crowther, J.; Ragusa, T. Realities of Mental health Nursing Practice in Rural Australia. Issues Ment. Health Nurs. 2011, 32, 512–518. [Google Scholar] [CrossRef]
- Brimblecombe, N. Analysis of changes in the national mental health nursing workforce in England, 2011–2021. J. Psychiatr. Ment. Health Nurs. 2023, 30, 994–1004. [Google Scholar] [CrossRef]
- Amara, P. Unsupported and burnt out: Why mental health nursing is in crisis: Mental health nurses face huge caseloads, high staff turnover and shortages, and burnout. How can the specialty turn itself around? Ment. Health Pract. 2024, 27, 8–10. [Google Scholar] [CrossRef]
- Popay, J.; Roberts, H.; Sowden, A.; Pettigrew, M.; Arai, L.; Rodgers, M.; Britton, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme; Lancaster University: Lancaster, UK, 2006. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Levac, D.; Moher, D.; Micah, D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS peer review of electronic search strategies: 2015 guideline statement. J. Clin. Epidemiol. 2016, 1, 40–46. [Google Scholar] [CrossRef]
- Colaizzi, P. Psychological Research as the Phenomenologist Views It. In Existential Phenomenological Alternatives for Psychology; Valle, R.S., King, M., Eds.; Oxford University Press: New York, NY, USA, 1978; pp. 48–71. [Google Scholar]
- Harrison, C.; Hauck, Y.; Ashby, R. Breaking down the stigma of mental health nursing: A qualitative study reflecting opinions from Western Australian nurses. J. Psychiatr. Ment. Health Nurses 2017, 24, 513–522. [Google Scholar] [CrossRef] [PubMed]
- McCrae, N.; Askey-Jones, S.; Larker, C. Merely a stepping stone? Professional identity and career prospects following postgraduate mental health nurse training. J. Psychiatr. Ment. Health Nurs. 2014, 21, 767–773. [Google Scholar] [CrossRef]
- Alexander, R.; Diefenbeck, C.; Brown, C. Career Choice and longevity in U.S. Psychiatric-Mental health Nurses. Issues Ment. Health Nurs. 2015, 36, 447–454. [Google Scholar] [CrossRef]
- Hazelton, M.; Rossiter, R.; Sinclair, E.; Morrall, P. Encounters with the ‘dark side’: New graduate nurses’ experiences in a mental health service. Health Sociol. Rev. 2011, 20, 172–186. [Google Scholar] [CrossRef]
- Humble, F.; Cross, W. Being different: A phenomenological exploration of a group of veteran psychiatric nurses. Int. J. Ment. Health Nurs. 2010, 19, 128–136. [Google Scholar] [CrossRef]
- Hung, B.; Huang, X.; Cheng, J.; Wei, S.; Lin, M. The working experiences of novice psychiatric nurses in Taiwanese culture: A Phenomenological study. J. Psychiatr. Ment. Health Nurs. 2014, 21, 536–543. [Google Scholar] [CrossRef]
- Joseph, B.; Olasoji, M.; Moss, C.; Cross, W. Transition Experiences of Indian Nurses into Australian Mental health system. J. Transcult. Nurs. 2022, 33, 41–48. [Google Scholar] [CrossRef]
- Thwala, N.; Mokoena-de Beer, A. Psychological Impact of Violence on Male Nurses in Forensic Units in Gauteng, South Africa. Health SA 2023, 29, 2313. [Google Scholar] [CrossRef]
- Harrison, C.A.; Hauck, Y.; Hoffman, R. Choosing and remaining in mental health. Int. J. Ment. Health Nurs. 2014, 23, 561–569. [Google Scholar] [CrossRef]
- Humpel, N.; Caputi, P. Exploring the relationship between work stress, years of experience and emotional competency using a sample of Australian mental health nurses. J. Psychiatr. Ment. Health Nurs. 2001, 8, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Humpel, N.; Caputi, P.; Martin, C. The relationship between emotions and stress among mental health nurses. Aust. N. Zldn. J. Ment. Health Nurs. 2001, 10, 55–60. [Google Scholar] [CrossRef] [PubMed]
- McAlister, M.; Happell, B.; Bradshaw, J. Making us what we are: Noteworthy people and achievements in Queensland mental health nursing. Int. J. Ment. Health Nurs. 2010, 19, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Shmilovitz, R.; Itzhaki, M.; Koton, S. Associations between gender, sex types and caring behaviours among nurses in mental health. J. Psychiatr. Ment. Health Nurs. 2021, 28, 422–429. [Google Scholar] [CrossRef]
- Yada, H.; Abe, H.; Omori, H.; Matsuo, H.; Otsubo, M.; Ishida, Y.; Katoh, T. Differences in job stress experienced by female and male Japanese psychiatric nurses. Int. J. Ment. Health Nurs. 2014, 23, 468–476. [Google Scholar] [CrossRef]
- Yang, B.; Stone, T.; Petrini, M.; Morris, D. Incidence, type, related factors, and effect of workplace violence on mental health nurses: A cross-sectional survey. Arch. Psychiatr. Nurs. 2018, 32, 31–38. [Google Scholar] [CrossRef]
- Holyoake, D. Male identity in mental health nursing. Nurs. Stand. 2002, 16, 33–37. [Google Scholar] [CrossRef]
- Holyoake, D. Similarly different: Exploring how male nurses in CAMHS experience difference in their gender performance. Compr. Child Adolesc. Nurs. 2020, 43, 389–409. [Google Scholar] [CrossRef]
- Fluttert, F.; van Meijel, B.; Nijman, H.; Bjørkly, S.; Grypdonck, M. Detached concern of forensic mental health nurses in therapeutic relationships with patients: The application of the early recognition method related to detached concern. Arch. Psychiatr. Nurs. 2010, 24, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Torkelson, D.J.; Seed, M.S. Gender differences in the roles and functions of inpatient psychiatric nurses. J. Psychosoc. Nurs. Ment. Health Serv. 2011, 49, 34–41. [Google Scholar] [CrossRef]
- Joseph, B.; Jacob, S.; Lam, L.; Rahman, M. Factors influencing the transition and retention of mental health nurses during the initial years of practice: Scoping review. J. Nurs. Manag. 2022, 30, 4274–4284. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Murrells, T.; Smith, E. Retaining the mental health nursing workforce: Early indicators of retention and attrition. Int. J. Ment. Health Nurs. 2005, 14, 230–242. [Google Scholar] [CrossRef]
- Lockhart, R. Men in Psychiatric Nursing (Publication Number MQ89958) [M.A., Royal Roads University (Canada)]. ProQuest One Academic. Canada—British Columbia, CA. 2024. Available online: https://www.proquest.com/dissertations-theses/men-psychiatric-nursing/docview/305055332/se-2?accountid=14647 (accessed on 1 October 2024).
- Roche, M.; Duffield, C. Issues and challenges in the mental health workforce development. Contemp. Nurse 2007, 25, 94–103. [Google Scholar] [CrossRef]
- Hartley, S.; Raphael, J.; Lovell, K.; Berry, K. Effective nurse–patient relationships in mental health care: A systematic review of interventions to improve the therapeutic alliance. Int. J. Nurs. Stud. 2020, 102, 103490. [Google Scholar] [CrossRef] [PubMed]
- Dickens, G.L.; Ion, R.; Waters, C.; Atlantis, E.; Everett, B. Mental health nurses’ attitudes, experience, and knowledge regarding routine physical healthcare: Systematic, integrative review of studies involving 7,549 nurses working in mental health settings. BMC Nurs. 2019, 18, 16. [Google Scholar] [CrossRef]
- Terry, D.; Peck, B.; Carden, C.; Perkins, A.J.; Smith, A. Traversing the Funambulist’s fine line between nursing and male identity: A systematic review of the factors that influence men as they seek to navigate the nursing profession. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 691–703. [Google Scholar] [CrossRef]
- Dempsey, J. Introduction to Nursing, Midwifery and Person-centred Care. Fundamentals of Nursing and Midwifery: A Person-Centred Approach to Care; Dempsey, J., Hillege, S., Hill, R., Eds.; Wolters Kluwer/Lippincott Williams & Wilkins: Sydney, Australia, 2014; pp. 4–16. [Google Scholar]
- Kitson, A.; Marshall, A.; Bassett, K.; Zeitz, K. What are the core elements of patient-centred care? A narrative review and synthesis of the literature from health policy, medicine, and nursing. J. Adv. Nurs. 2012, 69, 4–15. [Google Scholar] [CrossRef]
- Reedy, N.E. Becoming and Being a Nurse: A Research Informed Theory to Guide Contemporary University and Industry Approaches to Preparing and Supporting Graduate Nurses. Ph.D. Thesis, University of Southern Queensland, Toowoomba, Australia, 2019. [Google Scholar] [CrossRef]
- Australian Health Ministers’ Advisory Council. A National Framework for Recovery-Oriented Mental Health Services: Guide for Practitioners and Providers. 2023. Available online: https://www.health.gov.au/sites/default/files/documents/2021/04/a-national-framework-for-recovery-oriented-mental-health-services-guide-for-practitioners-and-providers.pdf (accessed on 20 December 2024).
- Martínez-Morato, S.; Feijoo-Cid, M.; Galbany-Estragués, P.; Fernández-Cano, M.I.; Arreciado Marañón, A. Emotion management and stereotypes about emotions among male nurses: A qualitative study. BMC Nurs. 2021, 20, 114. [Google Scholar] [CrossRef]
- Alenezi, A. The Impact of Resilience on Workplace Violence Experienced by Mental Health Nurses: A Cross-Sectional Survey. J. Nurs. Manag. 2024, 2024, 4449445. [Google Scholar] [CrossRef]
- Montayre, J.; Alananzeh, I.; Bail, K.; Barnewall, K.; Beament, T.; Campbell, S.; Carmody, C.; Chan, A.; Donnelly, F.; Duff, J.; et al. Development and psychometric testing of the gender misconceptions of men in nursing (GEMINI) scale among students. Contemp. Nurse 2022, 58, 253–263. Available online: https://www.tandfonline.com/doi/full/10.1080/10376178.2022.2107041 (accessed on 1 October 2024). [CrossRef] [PubMed]
- Johnston, I.; Price, O.; McPherson, P.; Armitage, C.J.; Brooks, H.; Bee, P.; Lovell, K.; Brooks, C.P. De-escalation of conflict in forensic mental health inpatient settings: A Theoretical Domains Framework-informed qualitative investigation of staff and patient perspectives. BMC Psychol. 2022, 10, 30. [Google Scholar] [CrossRef] [PubMed]
| Author (Year) | Country | Study Design | Study Aim | Sample Size | Findings | Themes |
|---|---|---|---|---|---|---|
| Alexander (2015) [24] | USA | Descriptive phenomenology | Exploring how nurses who are male in CAMHS experience differences in their gender performance | 8 (4 men, 4 women) | Interest developed in nursing school, personal relevance, and validation of potential were key for career choice. Retention was influenced by overcoming stereotypes, positive team dynamics, and remaining hopeful. | 1, 2 |
| Crowther and Ragusa (2011) [15] | Australia | Focus group | Exploring the relationship between work stress, years of experience, and emotional competency | 32 mental health nurses | Mental health nursing in rural Australia is in decline, affecting consumer outcomes and workplace experiences. | 3 |
| Fluttert et al. (2010) [39] | Netherlands | Cohort study (pre-test–post-test design) | The relationship between emotions and stress among mental health nurses | 116 (men and women not specified) | Detached concern is meaningful in forensic nursing. Levels of concern did not change significantly after applying the early recognition method. | 2, 3 |
| Harrison et al. (2014) [30] | Australia | Cross-sectional design | To explore how mental health nursing could be promoted as a sustainable career option | 192 mental health nurses (41.1%) | Staying in mental health nursing was affected by the following factors: facing reality, passion for mental health nursing, patient-centred caring, and workplace conditions. | 1, 2, 3 |
| Harrison et al. (2017) [22] | Australia | Qualitative study | Transition experiences of Indian nurses into the Australian mental health system | 192 (men and women not specified) | Reducing stigma and improving visibility and recognition of mental health nursing can enhance recruitment and retention. | 2, 3 |
| Hazelton et al. (2011) [25] | Australia | Qualitative study | Factors influencing the transition and retention of mental health nurses during the initial years of practice | Mental health nurses (n = 18); clinical nurse consultants (n = 5) | New graduates face challenges and require support to navigate the complexities of mental health services. | 3 |
| Holyoake (2002) [37] | UK | Ethnographic study | Retaining the mental health nursing workforce: early indicators of retention and attrition | Not specified | Explores the construction and impact of male identity in nursing. | 1, 2 |
| Holyoake (2020) [38] | UK | Ethnographic study | Issues and challenges in mental health workforce development | Not specified | Nurses who are male navigate a balance between similarity and difference in gender performance compared to female colleagues. | 1, 3 |
| Humble and Cross (2010) [26] | Australia | Qualitative study | The lived experiences of veteran psychiatric nurses with more than 10 years’ experience in the psychiatric field to identify the factors that have influenced these nurses to continue to work in this area | Mental health nurses (n = 7) | Participants felt and saw themselves as different in many ways from other nurses. There was a high level of satisfaction achieved from their roles as they strived to achieve harmony. | 1, 2 |
| Humpel and Caputi (2001a) [31] | Australia | Cross-sectional | Associations between gender, sex, and caring behaviours among nurses in mental health | 43 (men and women not specified) | Positive correlation between emotional competency and years of experience. Work stress impacts emotional stability. | 1, 2 |
| Humpel et al. (2001b) [32] | Australia | Cross-sectional | Incidence, type, related factors, and effect of workplace violence on mental health nurses | 43 (men and women not specified) | Emotional competency and trait affectivity are related to stress and experienced emotions. | 1, 2 |
| Hung et al., 2014 [27] | Taiwan | Qualitative study | To understand the working experiences of novice psychiatric nurses during their first year in a clinical setting | Mental health nurses (n = 13 women, n = 2 men) | Nurses are often inadequately prepared for mental health nursing and have little understanding of mental illness, are unable to communicate appropriately with clients, and struggle to cope with the conditions. | 3 |
| Joseph, et al. (2022a) [41] | Australia | Scoping review | Exploring the relationship between work stress, years of experience, and emotional competency | n/a | Identifies factors affecting transition and retention, including support systems and workplace environment. | 1, 2, 3 |
| Joseph et al. (2022b) [28] | Australia | Qualitative study | Exploring how nurses who are male in CAMHS experience differences in their gender performance | Nurses trained in India (n = 16) | Indian nurses face cultural and professional challenges during transition into the Australian mental health system. | 3 |
| Lockhart (2004) [43] | Canada | Action research | Men in psychiatric nursing | 6 (RNs = 3, students = 3) | Previous health work experience, knowing someone who works in psychiatric health, and commitment to and compassion for clients are qualities shared by the participants (all men). | 1, 2 |
| McAllister et al., 2010 [33] | Australia | Cross-sectional | To understanding the heritage of Queensland mental health nursing | Mental health nurses (n = 20) | Qualities included inspirational role model, and passion, dedication and/or commitment. | 1 |
| McCrae et al. (2014) [23] | UK | Qualitative study | To explore facilitators and barriers to professional identification in newly qualified nurses of accelerated post-graduate training | Mental health nurses (n = 9 women, n = 1 man) | Practise was defined in terms of values rather than skills and difficulty found in articulating a distinct role for mental health nursing. Experience in training and as a registered practitioner was considered rewarding; however, concerns were raised that nursing may not fulfil aspirations. Professional identity is likely to be a major factor in satisfaction and retention of nurses. | 1, 2, 3 |
| Robinson et al. (2005) [42] | UK | Longitudinal study | The relationship between emotions and stress among mental health nurses | Mental health nurses (n = 444, 66.8% women, 33.2% men) | Early indicators of retention include job satisfaction and support systems. | 2, 3 |
| Roche and Duffield (2007) [44] | USA | Expert opinion | Transition experiences of Indian nurses into the Australian mental health system | n/a | Workforce development is hindered by recruitment challenges and a lack of training opportunities. | 1, 3 |
| Shmilovitz et al. 2020 [34] | Israel | Cross-sectional | To study the association between sex types and caring behaviours in female and male nurses in the mental health field. | 114 mental health nurses (n = 36 males, n = 78 females) | Androgynous female and male nurses dispalyed higher levels of caring than other sex types. Higher levels of caring were observed in female compared with male nurses overall and in behaviours of respect and attentiveness to patients’ needs and safety. | 1 |
| Thwala & Mokoena-de Beer, 2023 [29] | South Africa | Phenomenology | Psychological impact of violence on male nurses in forensic units in Gauteng, South Africa | 11 | Workplace violence causes physical and psychological injury. Fear of further injury impacts work attendance and ability to complete work tasks. | 2, 3 |
| Torkelson & Seed, 2011 [40] | Correlational design. Convenience sampling. | Gender differences in the roles and functions of inpatient psychiatric nurses | 73 (28 male, 45 female) | Male and female nurses are differently impacted by perceived time spent on patient care, developing therapeutic and collegial relationships, and other nursing tasks. | 1, 2 | |
| Yada et al., 2014, [35] | Japan | Survey: Nurse Job Stressor Scale and the Stress Reaction Scale of the Brief Job Stress Questionnaire | Differences in job stress experienced by female and male Japanese psychiatric nurses | 244 (85 male, 159 female) | Male nurses impacted negatively by their self-perceived limitations regarding their psychiatric nursing abilities. | 1, 3 |
| Yang et al. (2018) [36] | Netherlands | Cross-sectional | Retaining the mental health nursing workforce: early indicators of retention and attrition | Mental health nurses (n = 245, 70% women, 30% men) | Workplace violence is prevalent and impacts mental health nurses’ well-being. | 2, 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reedy, N.; Luyke, T.; McGregor, R.; King, R.; Dawson, R.; Robinson, B.; Terry, D. Men in Mental Health: A Scoping Review of Challenges, Contributions, and Future Possibilities of Recruiting into Nursing. Nurs. Rep. 2025, 15, 97. https://doi.org/10.3390/nursrep15030097
Reedy N, Luyke T, McGregor R, King R, Dawson R, Robinson B, Terry D. Men in Mental Health: A Scoping Review of Challenges, Contributions, and Future Possibilities of Recruiting into Nursing. Nursing Reports. 2025; 15(3):97. https://doi.org/10.3390/nursrep15030097
Chicago/Turabian StyleReedy, Natasha, Trish Luyke, Rowena McGregor, Rachel King, Rhonda Dawson, Brendon Robinson, and Daniel Terry. 2025. "Men in Mental Health: A Scoping Review of Challenges, Contributions, and Future Possibilities of Recruiting into Nursing" Nursing Reports 15, no. 3: 97. https://doi.org/10.3390/nursrep15030097
APA StyleReedy, N., Luyke, T., McGregor, R., King, R., Dawson, R., Robinson, B., & Terry, D. (2025). Men in Mental Health: A Scoping Review of Challenges, Contributions, and Future Possibilities of Recruiting into Nursing. Nursing Reports, 15(3), 97. https://doi.org/10.3390/nursrep15030097