Abstract
Bioprosthetic valve thrombosis (BPVT) is considered a relatively rare but life-threatening clinical entity. Thus, there is the need of high clinical suspicion in order to make a timely diagnosis and related appropriate therapeutic interventions. In this regard, the management of BPVT is high risk, whatever the option taken (surgery and/or systemic fibrinolysis). The presence of severe comorbidities—as decompensated cirrhosis—further complicates the clinical decision-making process, calling for a patient-tailored integrated multidisciplinary approach. We report a challenging case of a 45-year-old patient with mitral bioprosthetic valve thrombosis and hepatitis C virus (HCV)-related cirrhosis complicated by active duodenal variceal bleeding.
1. Introduction
Prosthetic valve thrombosis (PVT) represents a life-threatening cardiovascular emergency needing a prompt diagnosis and timely appropriate therapeutic intervention [1,2].
Portal hypertension is a severe complication of decompensated cirrhosis and is responsible for the development of ascites and bleeding from esophagogastric varices [3,4,5]. Approximately one-third of patients with histologically confirmed cirrhosis have varices, and one-third of patients with varices develop bleeding, with a mortality rate of approximately 40% [6,7,8].
We report a very challenging clinically unstable case of a 45-year-old patient with mitral bioprosthetic valve thrombosis (M-BPVT) and hepatitis C virus (HCV)-related cirrhosis complicated by duodenal variceal bleeding.
2. Case Description
A 45-year-old man, smoker, and former drug addict with known HCV-related cirrhosis (Child–Pugh C), was admitted to the emergency department for shortness of breath and melena. His vital signs were as follows: blood pressure 100/60 mmHg, heart rate 98/min, respiratory rate 19/minute, body temperature 37 °C, and peripheral oxygen saturation (SpO2) level 95%. Standard hematologic tests and blood chemistries showed severe anemia (hemoglobin 6.2 mg/dL), hepatic dysfunction (serum albumin 3.1 g/dL, AST 169 UI/L, 155 ALT UI/L, GGT 25 UI/L, bilirubin 1.5 mg/dL) including altered coagulation tests (INR 2.06, PT 39 %, aPTT 44.6 s). Impaired renal function was also observed (serum creatinine 4.93 mg/dL, eGFR 16 mL/min, KDIGO stage IV). Past medical history included recurrent variceal bleeding treated with cyanoacrylate injections, chronic coronary syndrome (occlusion of first and second diagonal branch on coronary angiography) and mitral valve infective endocarditis (Staphylococcus aureus) requiring mitral valve replacement surgery (St Jude Medical bio prosthesis 29). Subsequently, the M-BPV was complicated by major dehiscence and extensive “rocking motions” with related moderate paravalvular leak that was successfully treated with percutaneous intervention.
It should be highlighted that the patient had poor adherence to home therapy consisting of furosemide, spironolactone, low-dose aspirin, and ramipril. After the initial workup with transfusion of two packed red blood cells, the patient underwent esophago-gastro-duodenoscopy, which revealed duodenal variceal bleeding (Figure 1), which was subsequently treated with endoscopic injection sclerotherapy. He was started on medical therapy with combination of antibiotics, propranolol, furosemide, spironolactone, pantoprazole, lactulose, octreotide, and intravenous fluid with albumin.

Figure 1.
Esophago-gastro-duodenoscopy: duodenal variceal bleeding.
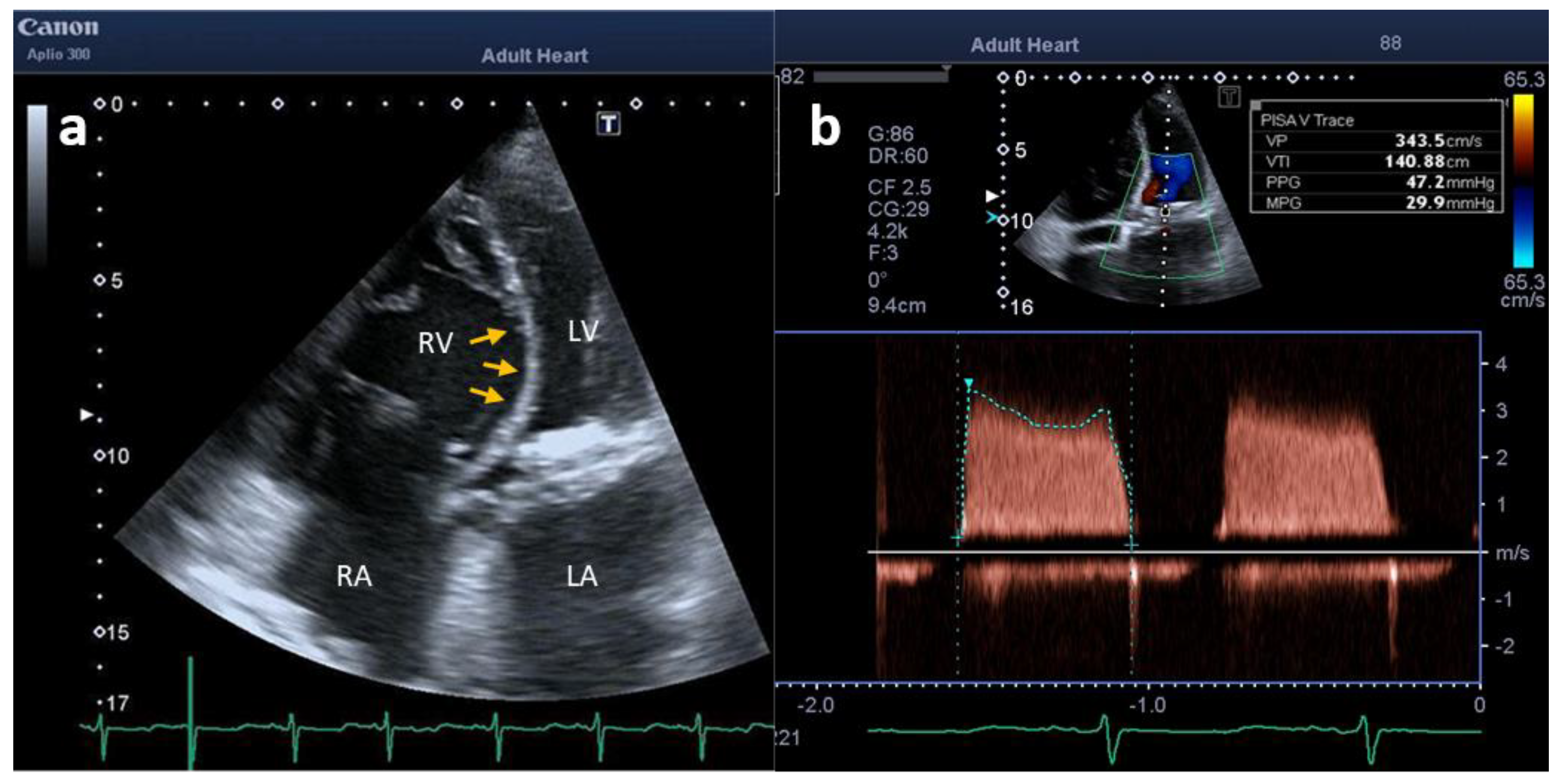
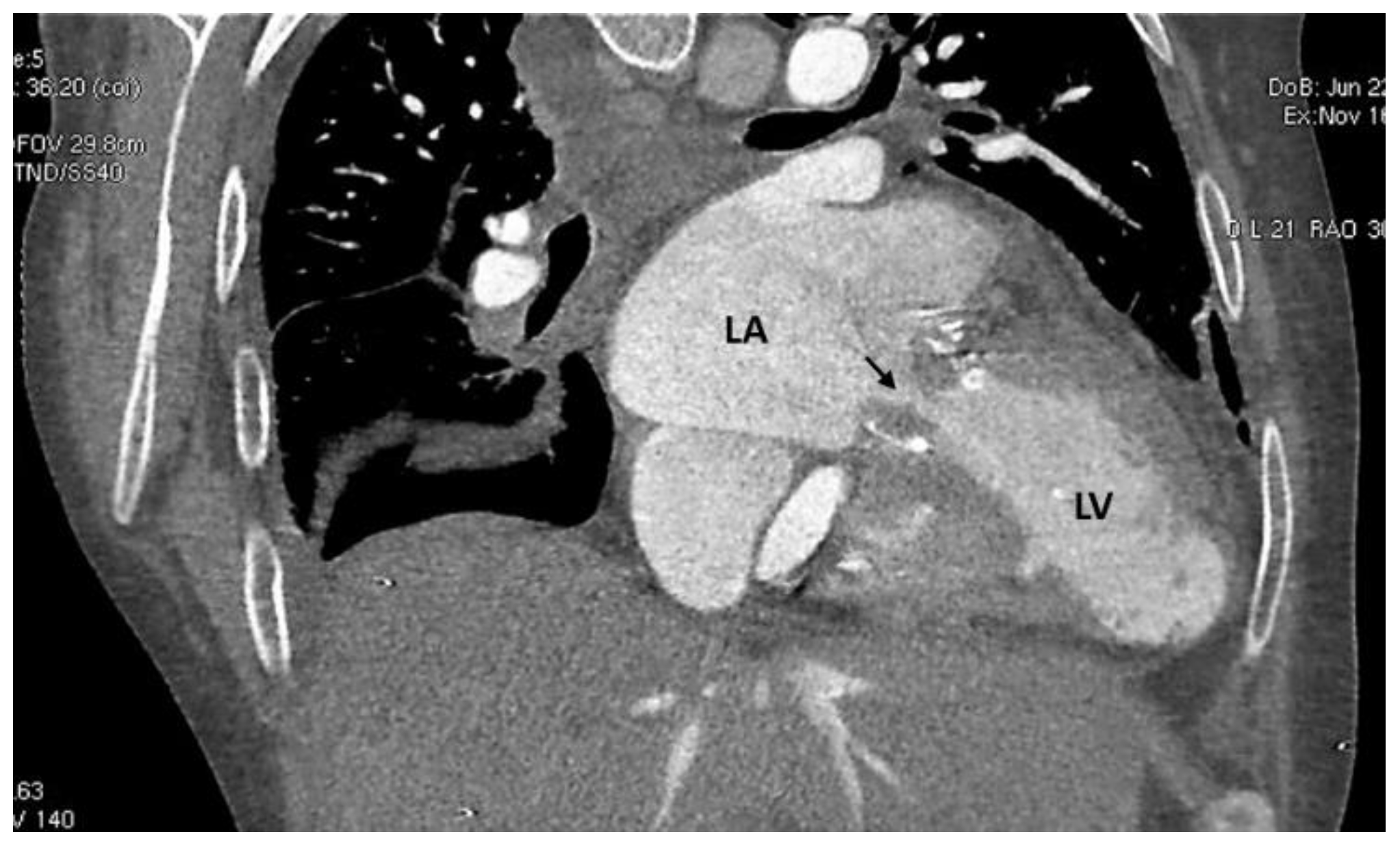
A bidimensional transthoracic Doppler echocardiography (TTE) exam was performed, which showed M-BPVT with severe stenosis (mean pressure gradient: 29.9 mmHg) and right ventricle dilatation/dysfunction along with severe pulmonary hypertension (estimated systolic pulmonary artery pressure: 70 mmHg) (Figure 2). A cardiac computed tomography (CCT) provided unique views of MVP dysfunction and excluded pulmonary embolism (Figure 3).
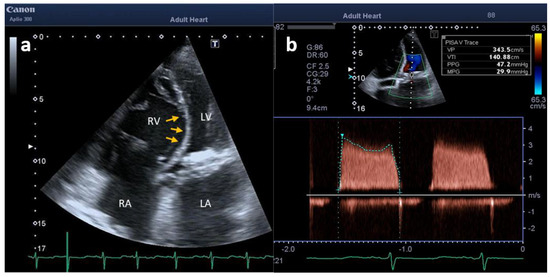
Figure 2.
TTE showing (a) dilatation and overload of right chambers (arrows) in apical four − chamber view and (b) high trans—prosthetic mitral valve velocities and gradients (b). LA: left atrium; LV: left ventricle; RA: right atrium; RV: right ventricle.
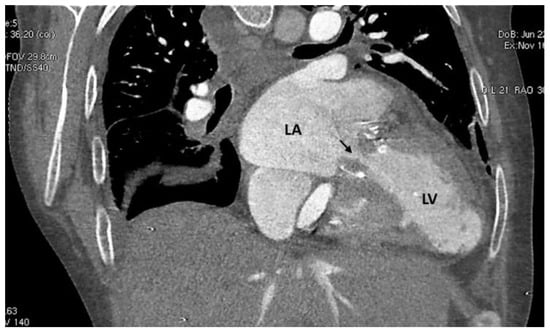
Figure 3.
CCT showing obstruction to the blood flow across the stenotic mitral valve prosthesis (arrow). LA: left atrium; LV: left ventricle.
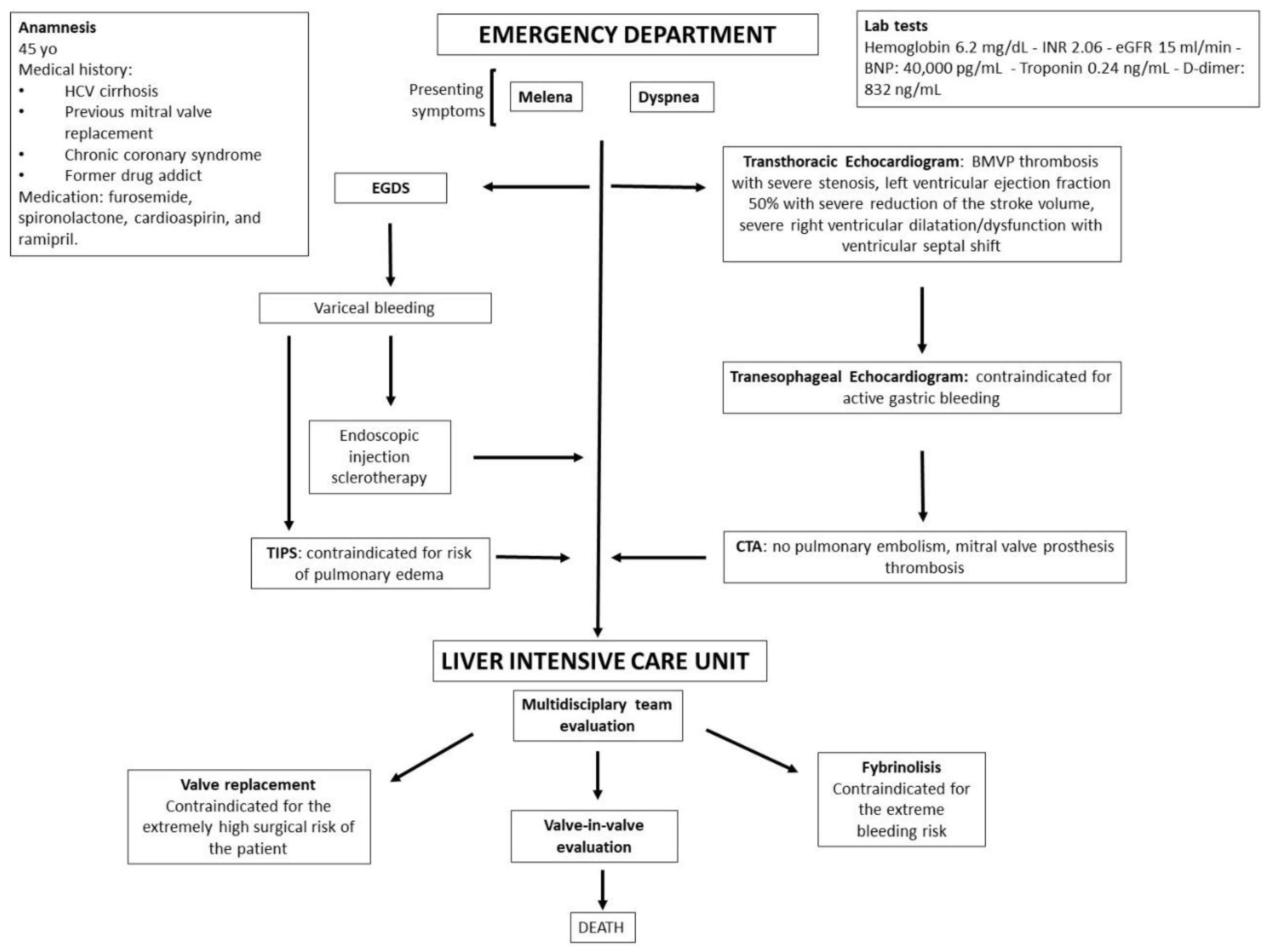
A transjugular intrahepatic portosystemic shunt (TIPS) was then excluded, as it could have precipitated the patient into pulmonary oedema as a direct consequence of volume overload [9]. For the worsening hemodynamic status, the patient was transferred to the liver intensive care where a multidisciplinary team was activated involving a cardiologist, cardiac surgeon, infectious disease specialist, pneumologist, and nephrologist (Figure 4). Different therapeutic interventions were evaluated: fibrinolysis was contraindicated for the extreme bleeding risk of the patient; valve replacement was excluded for the extremely high surgical risk of the procedure and valve-in-valve procedure was pending [10].
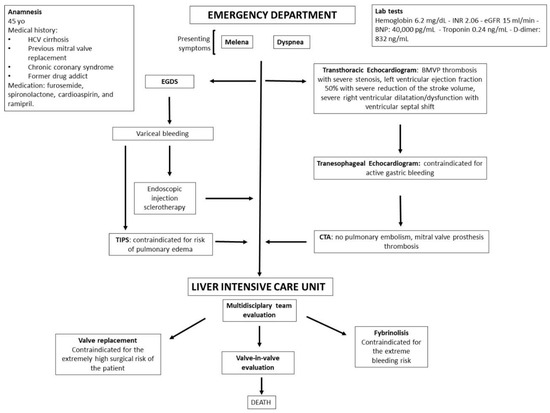
Figure 4.
Timeline of events.
Eventually, the patient developed a septic shock and died of multiorgan failure.
3. Discussion
Obstructive PVT is a cardiovascular emergency with a high mortality rate (approximately 10%) independent of treatment modality [2].
Due to non-specific symptoms and signs, a high index of suspicion is warranted, and it should be suspected in patients with any type of prosthetic valve presenting with symptoms of heart failure, thromboembolism, and/or low cardiac output, new and pathologic heart murmurs, and/or documentation of inadequate anticoagulation [1,2]. The diagnosis should be rapidly confirmed by TTE and transesophageal (TOE) Doppler echocardiography (first-line imaging technique). Cinefluoroscopy, CCT, cardiac magnetic resonance imaging (CMR), and to a lesser extent nuclear imaging represent additional tools in the case of inconclusive echocardiography (TTE + TEE) and/or additional information is needed. (Table 1).

Table 1.
Mechanical vs. bioprosthetic valve thrombosis [2,10,11,12,13,14,15,16]. BPVT: bioprosthetic valve thrombosis; C-CMR: cardiac magnetic resonance imaging; CCT: cardiac computed tomography; OAC: oral anticoagulants; TOE: transesophageal echocardiography; TTE: trans-thoracic echocardiography; UFH: unfractionated heparin; VKA: vitamin k antagonist.
The management of a patient with M-BPVT and HCV-related cirrhosis complicated by duodenal variceal bleeding is high risk, whatever the option taken.
In general, the first therapeutic option to try in case of duodenal varicose veins is the endoscopic treatment. However, if the duodenal varices are large in size and/or located in the submucosal layer, there is a high risk of duodenal perforation, and it is difficult to access with an endoscope, so an intervention such as TIPS should be evaluated [17].
TIPS is known to be an effective and safe treatment for varicose bleeding, including duodenal varices, by lowering portal hypertension [17]. However, in this specific case, TIPS was limited by the high risk of pulmonary oedema as a direct consequence of volume overload [9].
A balloon-assisted retrograde transvenous obliteration (BRTO), or plug-assisted retrograde transvenous obliteration (PARTO), or coil-assisted retrograde transvenous obliteration (CARTO) could be performed (if specific expertise is present) as an alternative to TIPS depending upon the patient’s clinical status [18,19,20,21].
On the other hand, the M-BPVT treatment strategy depends on the patient’s hemodynamic status, the presence or absence of BPV obstruction, and valve location. Conventional treatment options include surgery, fibrinolysis, and anticoagulation [2]. Anticoagulation using a vitamin K antagonist (VKA) and/or UFH (unfractionated heparin) is the first-line treatment in hemodynamically stable M-BPVT [2].
For non-obstructive M-BPVT with large (>5 mm), mobile, and pedunculated thrombi, surgery could be considered if an intravenous heparin fails to resolve these features. For small (<5 mm) thrombi, medical therapy with oral anticoagulants (OAC) is usually the preferred option. In cases of obstructive thrombi, surgery or fibrinolysis could be considered [2].
Fibrinolysis may be considered if surgery is not an option or is very high risk for the treatment of thrombosis but carries a risk of bleeding and thromboembolism [2].
In this complex case, it was not possible to implement anticoagulation/systemic fibrinolysis for the high bleeding risk due to duodenal bleeding varices. Furthermore, it was not possible to undertake surgical mitral valve replacement due to the extremely high surgical risk of the patient [2,10,11,12] (Figure 4).
Finally, the patient had an unfortunate ending while a transcatheter valve-in-valve procedure evaluation was pending. However, the presence of a large thrombus could have led to high risk of periprocedural embolization [2].
In conclusion, in a challenging unstable clinical scenario such as the case presented here, it is of paramount importance to implement an integrated multidisciplinary team approach (involving a cardiologist, cardiac surgeon, internist, infectious disease specialist, hepatologist- gastroenterologist, pneumologist, and nephrologist) in order to evaluate the risk/benefit of every therapeutic intervention.
Author Contributions
R.C., S.C. and E.B. have designed the study and were major contributors in writing the manuscript. R.C., S.C., G.L., L.R., V.C., L.A., R.B., B.R., G.R., C.M. and E.B. have drafted the work and substantively revised it. All authors have read and agreed to the published version of the manuscript.
Funding
Valentina Capone has been supported by a research grant provided by the Cardiopath PhD program.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the patient to publish this paper.
Data Availability Statement
The data that support the findings of this case report are openly available in the References section.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zipes, D.P.; Libby, P.; Bonow, R.; Mann, L.D.; Tomaselli, G.F.; Braunwald, E. Braunwald’s Heart Disease a Textbook of Cardiovascular Medicine, 11th ed.; Elsevier: Philadelphia, PA, USA, 2019; pp. 1455–1463. [Google Scholar]
- Puri, R.; Auffret, V.; Rodés-Cabau, J. Bioprosthetic Valve Thrombosis. J. Am. Coll. Cardiol. 2017, 69, 2193–2211. [Google Scholar] [CrossRef] [PubMed]
- Jameson, J.L.; Fauci, A.S.; Kasper, D.L.; Hauser, S.L.; Longo, D.L.; Loscalzo, J. Harrison’s Principles of Internal Medicine, 20th ed.; McGraw Hill Higher Education: New York, NY, USA, 2018; pp. 2405–2414. [Google Scholar]
- GBD 2017 Cirrhosis Collaborators. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 245–266. [Google Scholar] [CrossRef]
- Tsochatzis, E.A.; Bosch, J.; Burroughs, A.K. Liver cirrhosis. Lancet 2014, 383, 1749–1761. [Google Scholar] [CrossRef]
- Weishaupt, D.; Pfammatter, T.; Hilfiker, P.R.; Wolfensberger, U.; Marincek, B. Detecting bleeding duodenal varices with multislice helical CT. AJR Am. J. Roentgenol. 2002, 178, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Saad, W.E.; Lippert, A.; Saad, N.E.; Caldwell, S. Ectopic varices: Anatomical classification, hemodynamic classification, and hemodynamic-based management. Tech. Vasc. Interv. Radiol. 2013, 16, 158–175. [Google Scholar] [CrossRef] [PubMed]
- Henry, Z.; Uppal, D.; Saad, W.; Caldwell, S. Gastric and ectopic varices. Clin. Liver Dis. 2014, 18, 371–388. [Google Scholar] [CrossRef] [PubMed]
- Lotterer, E.; Wengert, A.; Fleig, W.E. Transjugular intrahepatic portosystemic shunt: Short-term and long-term effects on hepatic and systemic hemodynamics in patients with cirrhosis. Hepatology 1999, 29, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Guyton, R.A.; O’Gara, P.T.; Ruiz, C.E.; Skubas, N.J.; Sorajja, P.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, 2440–2492. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Pibarot, P.; Chambers, J.; Edvardsen, T.; Delgado, V.; Dulgheru, R.; Pepi, M.; Cosyns, B.; Dweck, M.R.; Garbi, M.; et al. Recommendations for the imaging assessment of prosthetic heart valves: A report from the European Association of Cardiovascular Imaging endorsed by the Chinese Society of Echocardiography, the Inter-American Society of Echocardiography, and the Brazilian Department of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 589–590. [Google Scholar]
- Mauro, C.; Vriz, O.; Romano, L.; Citro, R.; Russo, V.; Ranieri, B.; Alamro, B.; Aladmawi, M.; Granata, R.; Galzerano, D.; et al. Imaging Cardiovascular Emergencies: Real World Clinical Cases. Heart Fail. Clin. 2020, 16, 331–346. [Google Scholar] [CrossRef] [PubMed]
- Roudaut, R.; Serri, K.; Lafitte, S. Thrombosis of prosthetic heart valves: Diagnosis and therapeutic considerations. Heart 2007, 93, 137–142. [Google Scholar] [CrossRef]
- Karamitsos, T.D.; Karvounis, H. Magnetic resonance imaging is a safe technique in patients with prosthetic heart valves and coronary stents. Hellenic J. Cardiol. 2019, 60, 38–39. [Google Scholar] [CrossRef] [PubMed]
- Boyer, T.D.; Haskal, Z.J. American Association. The role of transjugular intrahepatic portosystemic shunt in the management of portal hypertension. Hepatology 2005, 41, 386–400. [Google Scholar] [CrossRef] [PubMed]
- Copelan, A.; Chehab, M.; Dixit, P.; Cappell, M.S. Safety and efficacy of angiographic occlusion of duodenal varices as an alternative to TIPS: Review of 32 cases. Ann. Hepatol. 2015, 14, 369–379. [Google Scholar] [CrossRef]
- Lee, E.W.; Saab, S.; Gomes, A.S.; Busuttil, R.; McWilliams, J.; Durazo, F.; Han, S.H.; Goldstein, L.; Tafti, B.A.; Moriarty, J.; et al. Coil-assisted retrograde transvenous obliteration (CARTO) for the treatment of portal hypertensive variceal bleeding: Preliminary results. Clin. Transl. Gastroenterol. 2014, 5, e61. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Jeon, G.S. Coil-assisted retrograde transvenous obliteration for the treatment of duodenal varix. Diagn. Interv. Radiol. 2018, 24, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Darcy, M.D.; Mani, N.B.; Park, A.W.; Akinwande, O.; Ramaswamy, R.S.; Kim, S.K. Modified balloon-occluded retrograde transvenous obliteration (BRTO) techniques for the treatment of gastric varices: Vascular plug-assisted retrograde transvenous obliteration (PARTO)/coil-assisted retrograde transvenous obliteration (CARTO)/balloon-occluded antegrade transvenous obliteration (BATO). Cardiovasc. Interv. Radiol. 2018, 41, 835–847. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).