Healthcare and SDGs Governance in Light of the Sustainability Helix Model: Evidence from the African Continent

Abstract
:1. Introduction
2. Materials and Methods
Methodology
3. Results
3.1. Overview of the Literature on Development (Objective 1)
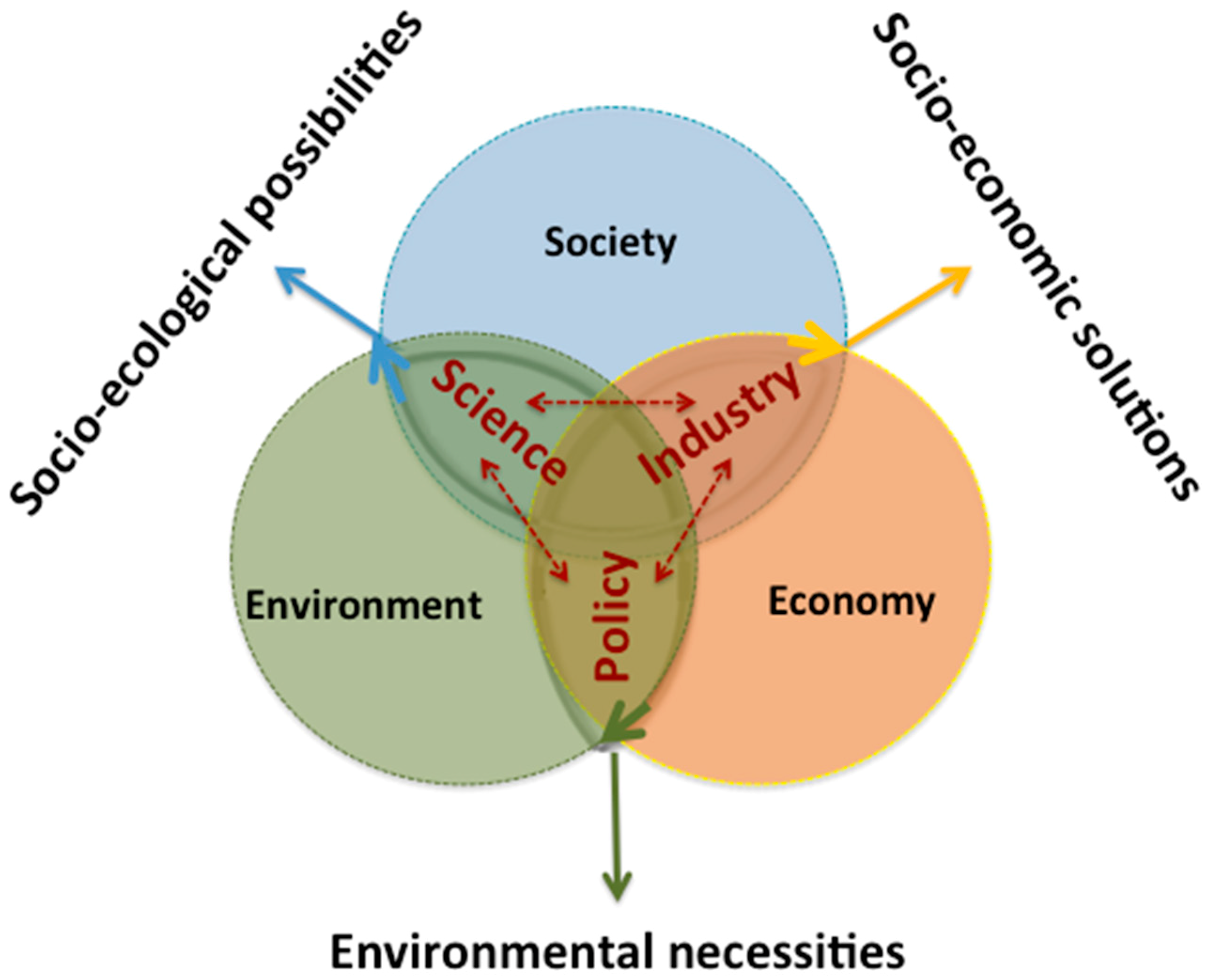
3.2. Novel Interpretative Models: The Viable Systems Approach (vSa) Sustainability Helix Model (Objective 2)
- Policy interprets the environmental necessities, that are the constraints to comply with when using the environmental resources;
- Science defines the socio-ecological possibilities, that is what can be done thanks to the progress of knowledge complying with the environmental necessities;
- Industry develops the socio-economic solutions, that are the feasible possibilities selected among the possible ones.
3.3. Health Programs in Less-Favored Areas: South Africa, Ethiopia and Benin (Objective 3)
3.3.1. Health Strategy of South Africa
3.3.2. Health Strategy of Ethiopia
3.3.3. Health Strategy of Benin
4. Discussion
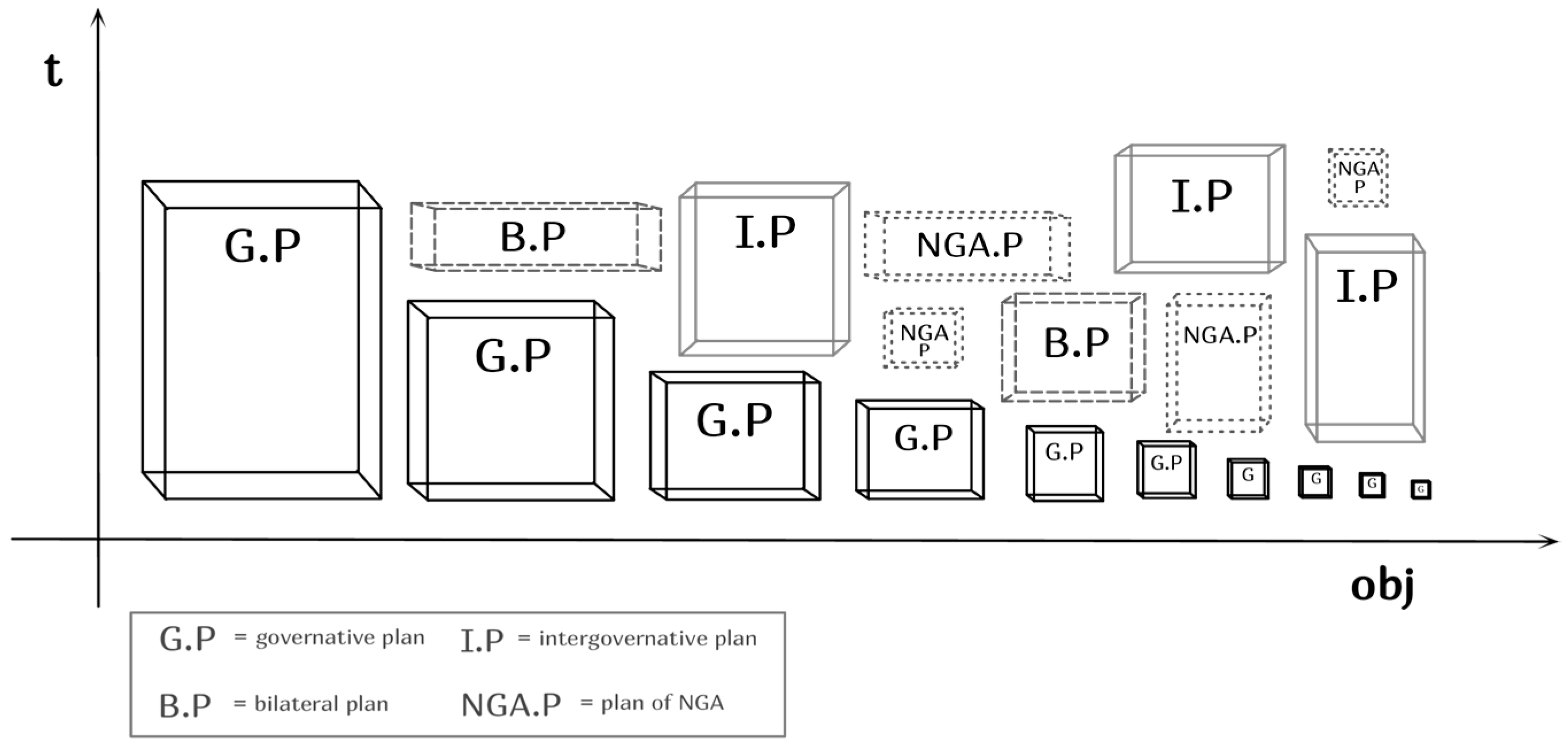
4.1. The Development Chinese Box
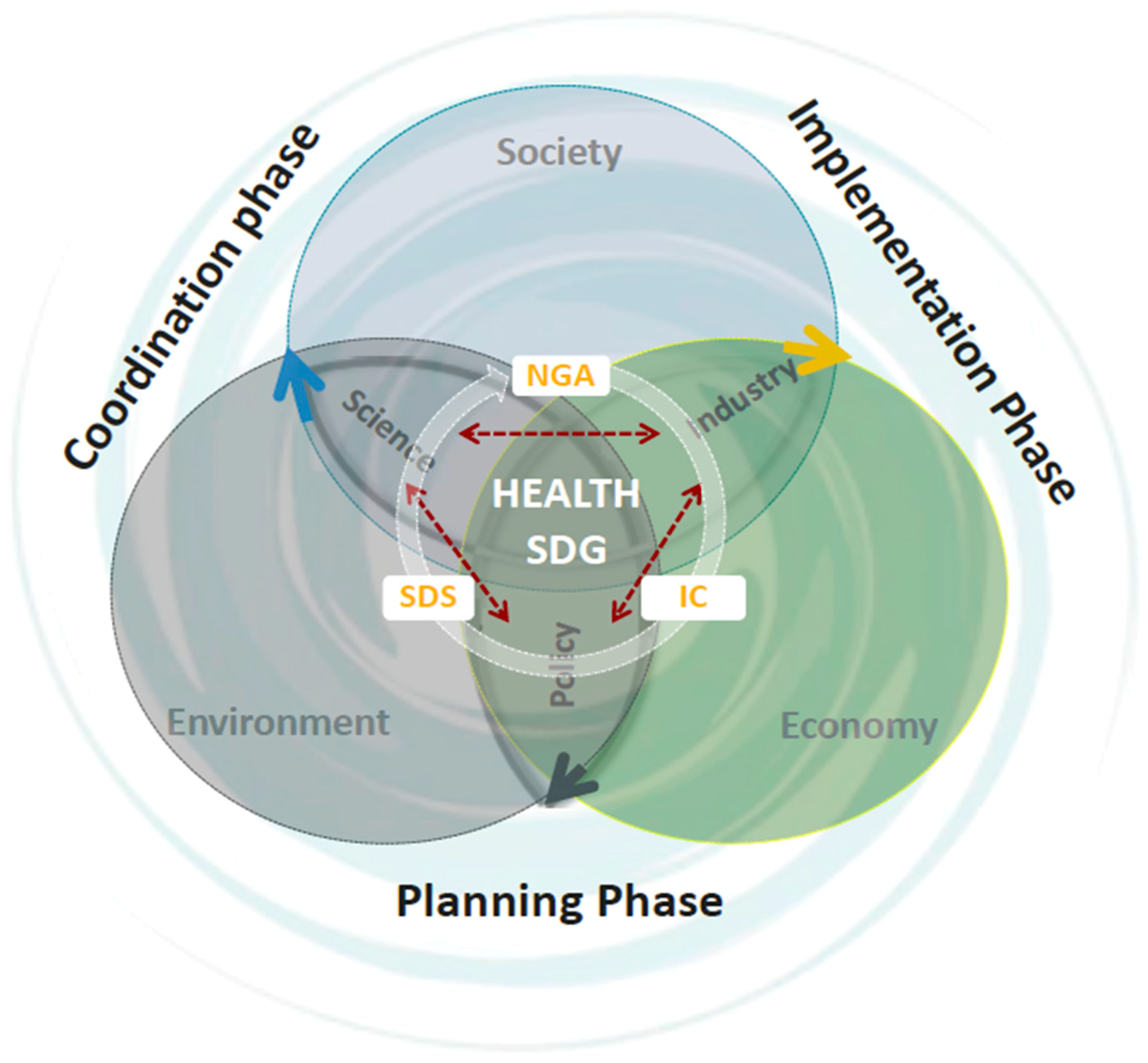
4.2. A Helix Systems Model for Sustainable Development of Health
- Sustainable development state (SDS);
- International community (IC);
- Non-governmental actors (NGA).
- The SDS and the NGA have the task of analyzing the causes of failure in achieving the target index, connoting it within their local context;
- The international community can be added to the first two actors to give indications on feasible solutions, always considering the local characteristics that emerged during the analysis phase;
- The NGAs become the cornerstone of the definition of operational plans together with the SDS, becoming an important strategic and implementation tool;
- The SDS and the NGAs, supported by funding and skills given by the international community (IC), must then devote themselves synergistically to the implementation of the plan and to achieving the objective of reducing maternal and child mortality by enhancing and safeguarding local resources.
- First, because it emphasizes that, to achieve the expected results (e.g., reduction of deaths from AIDS, etc.), there are roles that must be interpreted by any actor, even if they are not institutionalized as such; for example, NGOs can be called to play a para-governmental role.
- Secondly, because it promotes an exchange of roles that is particularly useful for considering the different perspectives; fundamental to making the local community understand local peculiarities (for example, concerning the alternative medicine of healers).
- Third, because it introduces the definition of possible “interface” roles that may be fundamental to effectively interconnecting the three key actors, especially when they are institutionally incapable or ineffective at playing a specific role that is important for producing the helix dynamics.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sustainable Development. Available online: https://sustainabledevelopment.un.org/sdgs (accessed on 30 December 2018).
- UN Sustainable Development Goals. Available online: https://www.un.org/sustainabledevelopment/health/ (accessed on 30 December 2018).
- Barile, S. Management Sistemico Vitale. Decidere in Contesti Complessi; Giappichelli: Torino, Italy, 2009. [Google Scholar]
- Barile, S. Contributions to Theoretical and Practical Advances in Management. A Viable Systems Approach (vSa); Aracne: Roma, Italy, 2013. [Google Scholar]
- Golinelli, G.M.; Barile, S.; Saviano, M.; Farioli, F.; Masaru, Y. Towards a common framework for knowledge co-creation: Opportunities of collaboration between Service Science and Sustainability Science. In Service Dominant Logic, Network and Systems Theory and Service Science: Integrating Three Perspectives for a New Service Agenda; Gummesson, E., Mele, C., Polese, F., Eds.; Giannini: Napoli, Italy, 2015. [Google Scholar]
- Barile, S.; Pels, J.; Polese, F.; Saviano, M. An introduction to the viable systems approach and its contribution to marketing. J. Bus. Mark. Manag. 2012, 5, 54–78. [Google Scholar]
- Barile, S.; Saviano, M. Foundations of systems thinking: The structure-system paradigm. In Contributions to Theoretical and Practical Advances in Management. A Viable Systems Approach (VSA); Various Authors; International Printing: Avellino, Italy, 2011; pp. 1–24. [Google Scholar]
- Sciarelli, F.; Rinaldi, A. Il Macro-Management per le Aree Deboli del Mondo; Franco Angeli: Milano, Italy, 2018. [Google Scholar]
- Sciarelli, F.; Rinaldi, A. Development Management of Transforming Economies. Theories, Approaches and Models for Overall Development; Palgrave Macmillan: London, UK, 2017; pp. 139–158. [Google Scholar]
- Etzkowitz, H. The triple helix as a model for innovation studies. Sci. Publ. Pol. 1998, 25, 195–203. [Google Scholar]
- Elkington, J. Cannibals with Forks. The Triple Bottom Line of 21st Century; New Society Publishers: London, UK, 1997. [Google Scholar]
- Rostow, W.W. The Stages of Economic Growth: A Non-Communist Manifesto; Cambridge University Press: Cambridge, UK, 1960; pp. 4–16. [Google Scholar]
- Lewis, W.A. Economic Development with Unlimited Supplies of Labour. Manch. Sch. 1954, 22, 139–191. [Google Scholar] [CrossRef]
- De la Croix, D.; Docquier, F. Do brain drain and poverty result from coordination failures? J. Econ. Growth 2012, 17, 1–26. [Google Scholar] [CrossRef]
- Deaton, A. Understanding the Mechanisms of Economic Development. J. Econ. Perspect. 2010, 24, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Rinaldi, A.; Sciarelli, F. Overall Development Management Model: A New Approach for Emerging Countries. Comparative Analysis of Six Countries on Two Continents. J. Syst. Cybern. Inform. 2017, 15, 7. [Google Scholar]
- Rinaldi, A.; Sciarelli, F. Economic and Social Causes for a Late Development: India vs. Ethiopia. Int. J. Econ. Policy Emerg. Econ. 2018, 11, 83–99. [Google Scholar]
- Dixon, D.F. Macromarketing: A social systems perspective. J. Macromarket. 1984, 4, 4–17. [Google Scholar] [CrossRef]
- Gummesson, E. Practical Value of Adequate Marketing Management Theory. Eur. J. Market. 2002, 36, 325–349. [Google Scholar] [CrossRef]
- Ritter, T.; Wilkinson, I.F.; Johnston, W.J. Managing in complex business networks. Ind. Market. Manag. 2014, 33, 175–183. [Google Scholar] [CrossRef]
- Mushkin, S.J. Health as an Investment. J. Polit. Econ. 1962, 70, 129–157. [Google Scholar] [CrossRef]
- Thomas, D.; Frankenberg, E. Health, Nutrition and Prosperity: A Microeconomic Perspective. Bull. World Health Organ. 2002, 80, 106–113. [Google Scholar] [PubMed]
- Deaton, A. Health, Inequality and Economic Development. J. Econ. Lit. 2003, 41, 113–158. [Google Scholar] [CrossRef]
- Hansmann, R.; Mieg, H.A.; Frischknecht, P. Principal sustainability components: Empirical analysis of synergies between the three pillars of sustainability. Int. J. Sustain. Dev. World Econ. 2012, 19, 451–459. [Google Scholar] [CrossRef]
- Barile, S.; Saviano, M.; Iandolo, F.; Calabrese, M. The Viable Systems Approach and its Contribution to the Analysis of Sustainable Business Behaviors. Syst. Res. Behav. Sci. 2014, 31, 683–695. [Google Scholar] [CrossRef]
- Barile, S.; Saviano, M.; Iandolo, F.; Caputo, F. La dinamica della sostenibilità tra vortici e correnti: Un modello a Tripla Elica. In Sviluppo, Sostenibilità e Competitività delle Aziende. Il Contributo degli Economisti Aziendali; Borgonovi, E., Aiello, G., Fellegara, A.M., Eds.; Il Mulino: Bologna, Italy, 2017; pp. 61–82. [Google Scholar]
- Etzkowitz, E.; Leydesdorff, L.A. Universities and the Global Knowledge Economy: A Triple Helix of University-industry-government Relations; Cassell: London, UK, 1997. [Google Scholar]
- Dzisah, J.; Etzkowitz, H. Triple helix circulation: The heart of innovation and development. Int. J. Technol. Man. Sustain. Dev. 2008, 7, 101–115. [Google Scholar] [CrossRef]
- Barile, S.; Saviano, M. Complexity and Sustainability in Management: Insights from A Systems Perspective. In Social Dynamics in a Systems Perspective; Barile, S., Pellicano, M., Polese, F., Eds.; Springer International Publishing: New York, NY, USA, 2018; pp. 39–63. [Google Scholar]
- Farioli, F.; Barile, S.; Saviano, M.; Iandolo, F. Re-reading sustainability through the Triple Helix model in the frame of a systems perspective. In The Sage Handbook of Nature; Marsden, T., Ed.; SAGE: London, UK, 2018; pp. 10–37. [Google Scholar]
- Scalia, M.; Barile, S.; Saviano, M.; Farioli, F. Governance for Sustainability: A Triple Helix Model. Sustain. Sci. 2018, 13, 1235–1244. [Google Scholar] [CrossRef]
- Saviano, M.; Barile, S.; Farioli, F.; Orecchini, F. Strengthening the science-policy-industry interface for progressing toward sustainability: A Systems thinking view. Sustain. Sci. 2019. forthcoming.. [Google Scholar]
- Carayannis, E.G.; Barth, T.D.; Campbell, D.F. The Quintuple Helix innovation model: Global warming as a challenge and driver for innovation. J. Innov. Entrep. 2012, 1, 2. [Google Scholar] [CrossRef]
- Pender, J.; Hazel, P. Promoting Sustainable Development in Less-Favored Areas; International Food Policy Research Institute: Washington, DC, USA, 2000. [Google Scholar]
- Todaro, M.P. A Model of Labor Migration and Urban Unemployment in Less Developed Countries. Am. Econ. Rev. 1969, 59, 138–148. [Google Scholar]
- Stark, O.; Bloom, D. The New Economics of Labor Migration. Am. Econ. Rev. 1985, 75, 173–178. [Google Scholar]
- Taylor, J.; Arango, J.; Hugo, G.; Kouaouci, A.; Massey, D.; Pellegrino, A. International Migration and Community Development. Int. Migr. Community Dev. 1996, 62, 397–418. [Google Scholar] [CrossRef]
- Nyberg-Sorensen, N.; Van Hear, N.; Engberg-Pedersen, P. The Migration-Development Nexus: Evidence and Policy Options. Int. Migr. 2002, 40, 49–73. [Google Scholar] [CrossRef]
- National Development Plan. Available online: www.gov.za/issues/national-development-plan-2030 (accessed on 30 December 2018).
- National Health Insurance. Available online: www.gov.za/documents/national-health-act-national-health-insurance-policy-towards-universal-health-coverage-30 (accessed on 30 December 2018).
- Medium Term Strategic Framework. Available online: www.gov.za/documents/medium-term-strategic-framework-2014-2019 (accessed on 30 December 2018).
- Budget Review 2015. Available online: www.treasury.gov.za/documents/national%20budget/2015/review/chapter%205.pdf (accessed on 30 December 2018).
- Health Financing System. Available online: https://openknowledge.worldbank.org/bitstream/handle/10986/24119/9781464808159.pdf;sequence=2 (accessed on 30 December 2018).
- Health Sector Development Program IV. Available online: https://phe-ethiopia.org/admin/uploads/attachment-721-HSDP%20IV%20Final%20Draft%2011Octoberr%202010.pdf (accessed on 30 December 2018).
- Growth and Transformation Plan II (GTP II). Available online: https://www.cmpethiopia.org/media/gtp_ii_policy_matrix_english_final_august_2016_2 (accessed on 30 December 2018).
- National Health Development Plan. Available online: http://www.nationalplanningcycles.org/sites/default/files/country_docs/Benin/benin_pnds_definitif_mis_en_forme_revue_le_21_juillet_2010_-_en.pdf (accessed on 30 December 2018).
- Available online: data.worldbank.org (accessed on 25 February 2019).
- ISTAT Sanità e Salute. Available online: https://www4.istat.it/it/files/2017/12/C04.pdf (accessed on 30 December 2018).
- Alesani, D. Result based management. In Management of International Institutions and NGOs; Missoni, E., Alesani, D., Eds.; Routledge: London, UK, 2014; p. 78 et seq. [Google Scholar]
- Cleland, D.I. Project Management: Strategic Design and Implementation; McGraw-Hill: New York, NY, USA, 2007. [Google Scholar]
- Bussi, F. Progettare in Partenariato; Franco Angeli: Milano, Italy, 2001. [Google Scholar]
- Rossi, M. I progetti di Sviluppo; Franco Angeli: Milano, Italy, 2004. [Google Scholar]
- Stroppiana, A. Progettare in Contesti Difficili; Franco Angeli: Milano, Italy, 2009. [Google Scholar]
- Managing for Development Results. Available online: http://www.oecd.org/dac/effectiveness/41178251.pdf (accessed on 30 December 2018).
- Cooke, P. Regional asymmetric knowledge capabilities & open innovation. Exploring ‘globalisation 2’: A new model of industry organisation. Res. Pol. 2005, 34, 1128–1149. [Google Scholar]
- Brännback, M.; Carsrud, A.; Krueger, N.; Elfving, J. Challenging the triple helix model of regional innovation systems: A venture-centric model. Int. J. Technoentrepreneurship 2008, 1, 257–277. [Google Scholar] [CrossRef]
- Viale, R.; Pozzali, A. Complex adaptive systems and the evolutionary triple helix. Crit. Soc. 2010, 36, 575–594. [Google Scholar] [CrossRef]
- Amir, S.; Nugroho, Y. Beyond the Triple Helix: Framing STS in the Developmental Context. Bull. Sci. Technol. Soc. 2013, 33, 115–126. [Google Scholar] [CrossRef]
- Aquino, R.P.; Barile, S.; Grasso, A.; Saviano, M. Envisioning smart and sustainable healthcare: 3D Printing technologies for personalized medication. Futures 2018, 103, 35–50. [Google Scholar] [CrossRef]
- Scalia, M.; Angelini, A.; Farioli, F.; Mattioli, G.F.; Saviano, M. The chariots of Pharaoh at the red sea: The crises of capitalism and environment. A modest proposal towards sustainability. Cult. Della Sosten. 2016, 1, 3–63. [Google Scholar]
- Saviano, M.; Barile, S.; Spohrer, J.C.; Caputo, F. A service research contribution to the global challenge of sustainability. J. Serv. Theory Pract. 2017, 27, 951–976. [Google Scholar] [CrossRef]
- Saviano, M.; Di Nauta, P.; Montella, M.M.; & Sciarelli, F. The Cultural Value of Protected Areas as Models of Sustainable Development. Sustainability 2018, 10, 1567. [Google Scholar] [CrossRef]
- Aquino, R.; Barile, S.; Grasso, A.; Saviano, M. Managing variety in healthcare through personalized medication: The contribution of 3D-printing technologies. In Cybernetics and Systems. Social and Business Decisions; Barile, S., Espejo, R., Perko, I., Saviano, M., Eds.; Systems Management Book Series; Giappichelli-Routledge: Abingdon, UK, 2019; pp. 345–350. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Life Expectancy at Birth, Total (Years) | |||||
|---|---|---|---|---|---|
| Country | 2010 | 2013 | 2014 | 2015 | 2016 |
| South Africa | 54 | 57 | 61 | 62 | 63 |
| Ethiopia | 61 | 64 | 64.5 | 65 | 65 |
| Bénin | 59 | 59 | 60.4 | 60.6 | 61 |
| Health Indicators 2015/2016 | |||
| Country | Health Exp. PP ($)—2015 | Health Exp. (% GDP)—2015 | Life Expect. at birth—2016 |
| South Africa | 470.80 | 8.2 | 63 |
| Ethiopia | 24.28 | 4.05 | 65 |
| Bénin | 31.29 | 3.99 | 61 |
| Organisation for Economic Co-operation and Development (OECD) Countries | |||
| Italia | 2700.43 | 9.00 | 83 |
| Japan | 3732.56 | 10.90 | 84 |
| USA | 9535.95 | 16.84 | 79 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saviano, M.; Sciarelli, F.; Rinaldi, A.; Alowanou, G.G. Healthcare and SDGs Governance in Light of the Sustainability Helix Model: Evidence from the African Continent. Sustainability 2019, 11, 1203. https://doi.org/10.3390/su11041203
Saviano M, Sciarelli F, Rinaldi A, Alowanou GG. Healthcare and SDGs Governance in Light of the Sustainability Helix Model: Evidence from the African Continent. Sustainability. 2019; 11(4):1203. https://doi.org/10.3390/su11041203
Chicago/Turabian StyleSaviano, Marialuisa, Fabiana Sciarelli, Azzurra Rinaldi, and Georcelin G. Alowanou. 2019. "Healthcare and SDGs Governance in Light of the Sustainability Helix Model: Evidence from the African Continent" Sustainability 11, no. 4: 1203. https://doi.org/10.3390/su11041203
APA StyleSaviano, M., Sciarelli, F., Rinaldi, A., & Alowanou, G. G. (2019). Healthcare and SDGs Governance in Light of the Sustainability Helix Model: Evidence from the African Continent. Sustainability, 11(4), 1203. https://doi.org/10.3390/su11041203