Promoting Healthy Lifestyle through Basic Psychological Needs in Inactive Adolescents: A Protocol Study from Self-Determination Approach

 ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
2. Methods
2.1. Design of the Study
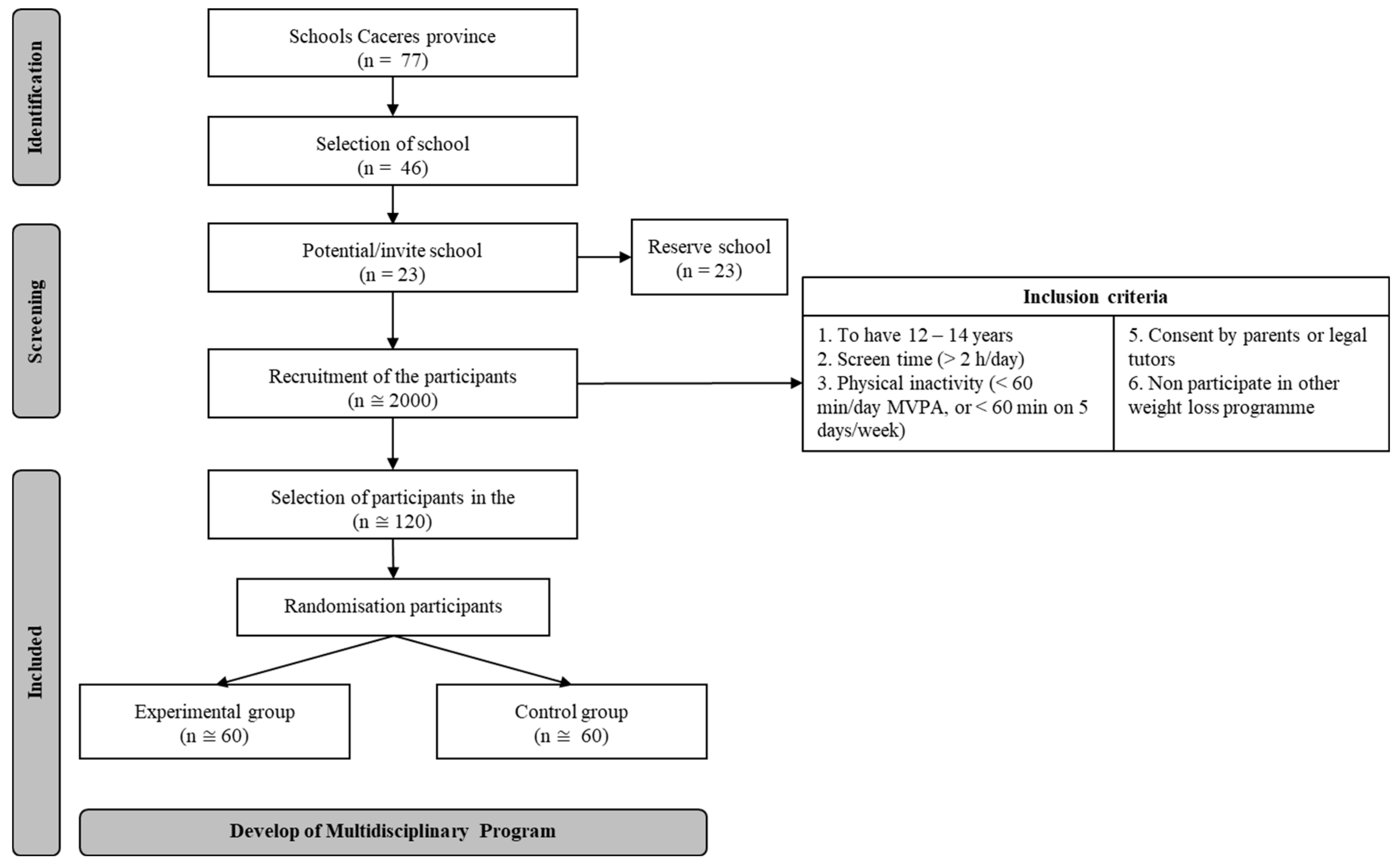
2.2. Participants
2.3. Procedure and Measure
2.3.1. Procedure
2.3.2. Sociodemographic Measures, PA and Screen Time
2.4. Multidisciplinary Program
2.4.1. Justification of Duration, Volume, Frequency, Type PA and Load Training
2.4.2. Initial Meeting
2.4.3. Initial Measure
2.4.4. Development of the Sessions
2.4.5. Final Measure
2.4.6. Follow-up Postintervention
2.5. Statistical Analysis
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organización. Global Recommendations on Physical Activity for Health; World Health Organization, 2010; Available online: https://apps.who.int/iris/bitstream/handle/10665/44399/9789241599979_eng.pdf;jsessionid=F4695575142FAB14D76A83F157002A76?sequence=1 (accessed on 6 July 2020).
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Akhtar-Danesh, N.; Dehghan, M.; Morrison, K.M.; Fonseka, S. Parents’ perceptions and attitudes on childhood obesity: A Q-methodology study. J. Am. Acad. Nurse Pract. 2011, 23, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.R.; Goodman, A.; Page, A.S.; Sherar, L.B.; Esliger, D.W.; van Sluijs, E.M.F.; Andersen, L.B.; Anderssen, S.; Cardon, G.; Davey, R.; et al. Objectively measured physical activity and sedentary time in youth: The International children’s accelerometry database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalman, M.; Inchley, J.; Sigmundova, D.; Iannotti, R.J.; Tynjala, J.A.; Hamrik, Z.; Haug, E.; Bucksch, J. Secular trends in moderate-to-vigorous physical activity in 32 countries from 2002 to 2010: A cross-national perspective. Eur. J. Public Health 2015, 25, 37–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cliff, D.P.; Hesketh, K.D.; Vella, S.A.; Hinkley, T.; Tsiros, M.D.; Ridgers, N.D.; Carver, A.; Veitch, J.; Parrish, A.M.; Hardy, L.L.; et al. Objectively measured sedentary behaviour and health and development in children and adolescents: Systematic review and meta-analysis. Obes. Rev. 2016, 17, 330–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, S.M.P.; Power, C. Change in health and social factors in mid-adulthood and corresponding changes in leisure-time physical inactivity in a prospective cohort. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 89. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Heal. 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Unión Europea. Traducción e impresión Consejo Superior de Deportes. CSD. Directrices Act; Física Ue Madrid: Madried, Spain, 2008. [Google Scholar]
- Sallis, J.F.; Owen, N. Ecological Models of Health Behavior. In Health Behavior and Health Education: Theory, Research and Practice, 3rd ed.; Jossey-Bass: San Francisco, CA, USA, 2002. [Google Scholar]
- Demetriou, Y.; Bachner, J. A school-based intervention based on self-determination theory to promote girls’ physical activity: Study protocol of the CReActivity cluster randomised controlled trial. BMC Public Health 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Report: Tackling Physical Inactivity—A Coordinated Approach | All-Party Commission on Physical Activity on WordPress.com. Available online: https://activitycommission.com/report-tackling-physical-inactivity-a-coordinated-approach (accessed on 6 July 2020).
- Smith, J.J.; Morgan, P.J.; Plotnikoff, R.C.; Dally, K.A.; Salmon, J.; Okely, A.D.; Finn, T.L.; Lubans, D.R. Smart-phone obesity prevention trial for adolescent boys in low-income communities: The ATLAS RCT. Pediatrics 2014, 134, e723–e731. [Google Scholar] [CrossRef] [Green Version]
- Jago, R.; Edwards, M.J.; Sebire, S.J.; Cooper, A.R.; Powell, J.E.; Bird, E.L.; Simon, J.; Blair, P.S. Bristol girls dance project (BGDP): Protocol for a cluster randomised controlled trial of an after-school dance programme to increase physical activity among 11-12 year old girls. BMC Public Health 2013, 13, 1003. [Google Scholar] [CrossRef] [Green Version]
- Alvirde-García, U.; Rodríguez-Guerrero, A.J.; Henao-Morán, S.; Gómez-Pérez, F.J.; Aguilar-Salinas, C.A. Results of a community based life style intervention program for children. Salud Publica Mex. 2013, 55, 406–414. [Google Scholar] [PubMed]
- Jacobs, N.; Hagger, M.S.; Streukens, S.; De Bourdeaudhuij, I.; Claes, N. Testing an integrated model of the theory of planned behaviour and self-determination theory for different energy balance-related behaviours and intervention intensities. Br. J. Health Psychol. 2011, 16, 113–134. [Google Scholar] [CrossRef] [PubMed]
- Pardo, B.M.; Bengoechea, E.G.; Julián Clemente, J.A.; Lanaspa, E.G. Empowering adolescents to be physically active: Three-year results of the Sigue la Huella intervention. Prev. Med. (Baltim) 2014, 66, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Sevil, J.; García-González, L.; Abós, Á.; Generelo, E.; Aibar, A. Can High Schools Be an Effective Setting to Promote Healthy Lifestyles? Effects of a Multiple Behavior Change Intervention in Adolescents. J. Adolesc. Heal. 2019, 64, 478–486. [Google Scholar] [CrossRef]
- Michie, S.F.; West, R.; Campbell, R.; Brown, J.; Gainforth, H. ABC of Behaviour Change Theories; Silverback publishing: London, UK, 2014. [Google Scholar]
- Brown, H.E.; Whittle, F.; Jong, S.T.; Croxson, C.; Sharp, S.J.; Wilkinson, P.; Wilson, E.C.; Van Sluijs, E.M.; Vignoles, A.; Corder, K. A cluster randomised controlled trial to evaluate the effectiveness and cost-effectiveness of the GoActive intervention to increase physical activity among adolescents aged 13–14 years. BMJ Open 2017, 7, e014419. [Google Scholar] [CrossRef]
- Koorts, H.; Eakin, E.; Estabrooks, P.; Timperio, A.; Salmon, J.; Bauman, A. Implementation and scale up of population physical activity interventions for clinical and community settings: The PRACTIS guide. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 51. [Google Scholar] [CrossRef]
- Baranowski, T.; Jago, R. Understanding the Mechanisms of Change in Children’s Physica...: Exercise and Sport Sciences Reviews. Exerc. Sport Sci. Rev. 2005, 33, 163–168. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Intrinsic and Extrinsic Motivations: Classic Definitions and New Directions. Contemp. Educ. Psychol. 2000, 25, 54–67. [Google Scholar] [CrossRef]
- Deci, E.L.; Tyan, R.M. The general causality orientations scale: Self-Determination in Personality. J. Res. Pers. 1985, 19, 109–134. [Google Scholar] [CrossRef]
- Vaquero-Solís, M.; Gallego, D.I.; Tapia-Serrano, M.Á.; Pulido, J.J.; Sánchez-Miguel, P.A. School-based physical activity interventions in children and adolescents: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 999. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, Physical Activity, and Self-Determination Theory: A Systematic Review; BioMed Central: London, UK, 2012; Volume 9, p. 78. [Google Scholar]
- González-Cutre, D.; Sierra, A.C.; Beltrán-Carrillo, V.J.; Peláez-Pérez, M.; Cervelló, E. A school-based motivational intervention to promote physical activity from a self-determination theory perspective. J. Educ. Res. 2016, 111, 320–330. [Google Scholar] [CrossRef]
- Sánchez-Oliva, D.; Pulido-González, J.J.; Leo, F.M.; González-Ponce, I.; García-Calvo, T. Effects of an intervention with teachers in the physical education context: A Self-Determination Theory approach. PLoS ONE 2017, 12, e0189986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory. Basic Psychological Needs in Motivation, Development and Wellness; Consortium Erudit; Guilford Press: New York, NY, USA, 2017; Volume 38. [Google Scholar]
- Reeve, J.; Jang, H. What teachers say and do to support students’ autonomy during a learning activity. J. Educ. Psychol. 2016, 98, 209–218. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Intrinsic and extrinsic motivation from a self-determination theory perspective: Definitions, theory, practices, and future directions. Contemp. Educ. Psychol. 2020, 101860. [Google Scholar] [CrossRef]
- Deci, E.; Ryan, R. “Facilitating optimal motivation and psychological well-being across life’s domains”: Correction to Deci and Ryan. Can. Psychol. Can. 2008, 49, 262. [Google Scholar] [CrossRef]
- Corder, K.; Atkin, A.J.; Ekelund, U.; Van Sluijs, E.M. What do adolescents want in order to become more active? BMC Public Health 2013, 13, 718. [Google Scholar] [CrossRef] [Green Version]
- Kriemler, S.; Meyer, U.; Martin, E.; Van Sluijs, E.M.F.; Andersen, L.B.; Martin, B.W. Effect of school-based interventions on physical activity and fitness in children and adolescents: A review of reviews and systematic update. Br. J. Sports Med. 2011, 45, 923–930. [Google Scholar] [CrossRef] [Green Version]
- Dobbins, M.; Husson, H.; Decorby, K.; Larocca, R.L. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2013, 2013. [Google Scholar] [CrossRef]
- Lonsdale, C.; Rosenkranz, R.R.; Peralta, L.R.; Bennie, A.; Fahey, P.; Lubans, D.R. A systematic review and meta-analysis of interventions designed to increase moderate-to-vigorous physical activity in school physical education lessons. Prev. Med. 2013, 56, 152–161. [Google Scholar] [CrossRef]
- Owen, K.B.; Smith, J.; Lubans, D.R.; Ng, J.Y.Y.; Lonsdale, C. Self-determined motivation and physical activity in children and adolescents: A systematic review and meta-analysis. Prev. Med. (Baltim) 2014, 67, 270–279. [Google Scholar] [CrossRef]
- Castro-Piñero, J.; Carbonell-Baeza, A.; Martinez-Gomez, D.; Gómez-Martínez, S.; Cabanas-Sánchez, V.; Santiago, C.; Veses, A.M.; Bandrés, F.; Gonzalez-Galo, A.; Gomez-Gallego, F.; et al. Follow-up in healthy schoolchildren and in adolescents with DOWN syndrome: Psycho-environmental and genetic determinants of physical activity and its impact on fitness, cardiovascular diseases, inflammatory biomarkers and mental health; the UP& study. BMC Public Health 2014, 14, 400. [Google Scholar]
- Lonsdale, C.; Rosenkranz, R.R.; Sanders, T.; Peralta, L.R.; Bennie, A.; Jackson, B.; Taylor, I.M.; Lubans, D.R. A cluster randomized controlled trial of strategies to increase adolescents’ physical activity and motivation in physical education: Results of the Motivating Active Learning in Physical Education (MALP) trial. Prev. Med. (Baltim) 2013, 57, 696–702. [Google Scholar] [CrossRef] [Green Version]
- Robbins, L.; Wen, F.; Research, J.L. Mediators of Physical Activity Behavior Change in the “Girls on the Move” Intervention. Nurs. Res. 2019, 68, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Carson, V.; Chaput, J.-P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, I. Effects of increased physical activity on motor skills and marks in physical education: An intervention study in school years 1 through 9 in Sweden. Phys. Educ. Sport Pedagog. 2011, 16, 313–329. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Gipson-Jones, T.L.; Myer, G.D. Exercise Deficit Disorder in Youth. J. Sch. Nurs. 2012, 28, 252–255. [Google Scholar] [CrossRef]
- Ardoy, D.N.; Fernández-Rodríguez, J.M.; Ruiz, J.R.; Chillón, P.; España-Romero, V.; Castillo, M.J.; Ortega, F.B. Improving Physical Fitness in Adolescents Through a School-Based Intervention: The EDUFIT Study. Rev. Española Cardiol. 2011, 64, 484–491. [Google Scholar] [CrossRef]
- González-Gross, M.; Ruiz, J.R.; Moreno, L.A.; de Rufino-Rivas, P.; Garaulet, M.; Mesana, M.I.; Gutiérrez, A.; AVENAGroup*, T. Body composition and physical performance of Spanish adolescents: The AVENA pilot study. Acta Diabetol. 2003, 40, s299–s301. [Google Scholar] [CrossRef]
- Naylor, P.-J.P.J.; Macdonald, H.M.; Zebedee, J.A.; Reed, K.E.; McKay, H.A. Lessons learned from Action Schools! BC—An ‘active school’model to promote physical activity in elementary schools. J. Sci. Med. Sport 2006, 9, 413–423. [Google Scholar] [CrossRef]
- Quaresma, A.M.; Palmeira, A.L.; Martins, S.S.; Minderico, C.S.; Sardinha, L.B. Effect of a school-based intervention on physical activity and quality of life through serial mediation of social support and exercise motivation: The PESSOA program. Health Educ. Res. 2014, 29, 906–917. [Google Scholar] [CrossRef]
- Kowalski, K.C.; Crocker, P.R.E.; Donen, R.M. The Physical Activity Questionnaire for Older Children (PAQ-C) and Adolescents (PAQ-A) Manual; College of Kinesiology, University of Saskatchewan, 2013; Available online: https://www.researchgate.net/profile/Peter_Crocker/publication/228441462_The_Physical_Activity_Questionnaire_for_Older_Children_PAQ-C_and_Adolescents_PAQ-A_Manual/links/00b7d51a37fe869464000000.pdf (accessed on 7 July 2020).
- Martínez-Gómez, D.; Martínez-de-Haro, V.; Pozo, T.; Welk, G.J.; Villagra, A.; Calle, M.E.; Marcos, A.; Veiga, O.L. Fiabilidad y validez del cuestionario de actividad física PAQ-A en adolescentes españoles. Rev. Esp. Salud Publica 2009, 83, 427–439. [Google Scholar] [CrossRef] [PubMed]
- Telama, R.; Yang, X. Decline of physical activity from youth to young adulthood in Finland. Med. Sci. Sport. Exerc. 2000, 32, 1617–1622. [Google Scholar] [CrossRef]
- Cabanas-Sánchez, V.; Martínez-Gómez, D.; Esteban-Cornejo, I.; Castro-Piñero, J.; Conde-Caveda, J.; Veiga, Ó.L. Reliability and validity of the Youth Leisure-time Sedentary Behavior Questionnaire (YLSBQ). J. Sci. Med. Sport 2018, 21, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Amoura, C.; Berjot, S.; Gillet, N.; Caruana, S.; Cohen, J.; Finez, L. Autonomy-Supportive and Controlling Styles of Teaching. Swiss J. Psychol. 2015, 74, 141–158. [Google Scholar] [CrossRef]
- Jang, H.; Reeve, J.; Ryan, R.M.; Kim, A. Can Self-Determination Theory Explain What Underlies the Productive, Satisfying Learning Experiences of Collectivistically Oriented Korean Students? J. Educ. Psychol. 2009, 101, 644–661. [Google Scholar] [CrossRef]
- Haerens, L.; Aelterman, N.; Vansteenkiste, M.; Soenens, B.; Van Petegem, S. Do perceived autonomy-supportive and controlling teaching relate to physical education students’ motivational experiences through unique pathways? Distinguishing between the bright and dark side of motivation. Psychol. Sport Exerc. 2015, 16, 26–36. [Google Scholar] [CrossRef]
- Taylor, I.M.; Ntoumanis, N.; Standage, M.; Spray, C.M. Motivational predictors of physical education students’ effort, exercise intentions, and leisure-time physical activity: A multilevel linear growth analysis. J. Sport Exerc. Psychol. 2010, 32, 99–120. [Google Scholar] [CrossRef] [Green Version]
- Vasconcellos, D.; Parker, P.D.; Hilland, T.; Cinelli, R.; Owen, K.B.; Kapsal, N.; Lee, J.; Antczak, D.; Ntoumanis, N.; Ryan, R.M.; et al. Self-Determination Theory Applied to Physical Education: A Systematic Review and Meta-Analysis. J. Educ. Psychol. 2019. [Google Scholar] [CrossRef]
- Sánchez-Oliva, D.; Sánchez-Miguel, P.A.; Kinnafick, F.-E.; Leo, F.M.; García-Calvo, T. Physical education lessons and physical activity intentions within Spanish Secondary Schools: A Self-Determination perspective. J. Teach. Phys. Educ. 2014, 33, 232–249. [Google Scholar] [CrossRef]
- Reeve, J. Why teachers adopt a controlling motivating style toward students and how they can become more autonomy supportive. Educ. Psychol. 2009, 44, 159–175. [Google Scholar] [CrossRef]
- Cox, A.; Williams, L. The roles of perceived teacher support, motivational climate, and psychological need satisfaction in students’ physical education motivation. J. Sport Exerc. Psychol. 2008, 30, 222–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardoy, D.N.; Fernández-Rodríguez, J.M.; Chillón, P.; Artero, E.G.; España-Romero, V.; Jiménez-Pavón, D.; Ruiz, J.R.; Guirado-Escámez, C.; Castillo, M.J.; Ortega, F.B. Educando para mejorar el estado de forma física, estudio EDUFIT: Antecedentes, diseño, metodología y análisis del abandono/adhesión al estudio. Rev. Esp. Salud Publica 2010, 84, 151–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheon, S.H.; Reeve, J.; Ntoumanis, N. A needs-supportive intervention to help PE teachers enhance students’ prosocial behavior and diminish antisocial behavior. Psychol. Sport Exerc. 2018, 35, 74–88. [Google Scholar] [CrossRef] [Green Version]
- Lonsdale, C.; Lester, A.; Owen, K.B.; White, R.L.; Peralta, L.; Kirwan, M.; Diallo, T.M.O.; Maeder, A.J.; Bennie, A.; Macmillan, F.; et al. An internet-supported school physical activity intervention in low socioeconomic status communities: Results from the Activity and Motivation in Physical Education (AMPED) cluster randomised controlled trial. Br. J. Sports Med. 2017, 53, 341–347. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Control: WHO Report 2010; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P.; American College of Sports Medicine American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “What” and “Why” of Goal Pursuits: Human Needs and the Self-Determination of Behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Currie, C.; Molcho, M.; Boyce, W.; Holstein, B.; Torsheim, T.; Richter, M. Researching health inequalities in adolescents: The development of the Health Behaviour in School-Aged Children (HBSC) Family Affluence Scale. Soc. Sci. Med. 2008, 66, 1429–1436. [Google Scholar] [CrossRef]
- Robusto, K.M.; Trost, S.G. Comparison of three generations of ActiGraphTM activity monitors in children and adolescents. J. Sports Sci. 2012, 30, 1429–1435. [Google Scholar] [CrossRef]
- Vanhelst, J.; Mikulovic, J.; Bui-Xuan, G.; Dieu, O.; Blondeau, T.; Fardy, P.; Béghin, L. Comparison of two ActiGraph accelerometer generations in the assessment of physical activity in free living conditions. BMC Res. Notes 2012, 5, 187. [Google Scholar] [CrossRef] [Green Version]
- Rothney, M.P.; Apker, G.A.; Song, Y.; Chen, K.Y. Comparing the performance of three generations of ActiGraph accelerometers. J. Appl. Physiol. 2008, 105, 1091–1097. [Google Scholar] [CrossRef] [Green Version]
- Ward, D.S.; Evenson, K.R.; Vaughn, A.; Rodgers, A.B.; Troiano, R.P. Accelerometer use in physical activity: Best practices and research recommendations. Med. Sci. Sports Exerc. 2005, 37, S582–S588. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Konstabel, K.; Pasquali, E.; Ruiz, J.R.; Hurtig-Wennlöf, A.; Mäestu, J.; Löf, M.; Harro, J.; Bellocco, R.; Labayen, I.; et al. Objectively Measured Physical Activity and Sedentary Time during Childhood, Adolescence and Young Adulthood: A Cohort Study. PLoS ONE 2013, 8, e60871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segura-García, C.; Papaianni, M.C.; Rizza, P.; Flora, S.; Fazio, P. De The development and validation of the Body Image Dimensional Assessment (BIDA). Eat. Weight Disord. Stud. Anorexia Bulim. Obes. 2012, 17, e219–e225. [Google Scholar]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Vázquez, A.J.; Rosa, M.; García-Bóveda, J. Escala de autoestima de Rosenberg: Fiabilidad y validez en población clínica española. Apunt. Psicol. 2004, 22, 247–255. [Google Scholar]
- Markland, D.; Tobin, V. A modification to the behavioural regulation in exercise questionnaire to include an assessment of amotivation. J. Sport. Exerc. 2004, 26, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.M.; Sabiston, C.M.; Mack, D.E.; Blanchard, C.M. On the nature and function of scoring protocols used in exercise motivation research: An empirical study of the behavioral regulation in exercise questionnaire. Psychol. Sport Exerc. 2012, 13, 614–622. [Google Scholar] [CrossRef]
- Diener, E.; Eunkook, M.S.; Richard, E.L.; Heidi, L.S. Subjective Well-Being: Three Decades of Progress. Psychol. Bull. 1984, 95, 542–575. [Google Scholar] [CrossRef]
- Atienza, F.; Balaguer, I.; García-Merita, M. Propiedades Psicométricas de la Escala de Satisfacción con la Vida en Adolescentes. Psicothema 2000, 12, 314–319. [Google Scholar]
- Watson, D.; Clark, L.A.L.A.; Tellegen, A. Development and Validation of Brief Measures of Positive and Negative Affect. PANAS Scales 1988, 54, 1063–1070. [Google Scholar]
- Ruíz, J.R.; España Romero, V.; Castro Piñero, J.; Artero, E.G.; Ortega, F.B.; Cuenca García, M.; Jiménez Pavón, D.; Chillón, P.; Girela Rejón, M.J.; Mora, J.; et al. Batería ALPHA-Fitness: Test de campo para la evaluación de la condición física relacionada con la salud en niños y adolescentes. SciELO Esp. 2011, 26, 1210–1214. [Google Scholar]
- Ruiz, J.R.; Castro-Piñero, J.; España-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.A.M.; Enez-Pavón, D.J.; Chillón, P.; Girela-Rejón, M.J.; Mora, J.; et al. Field-based fitness assessment in young people: The ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.; Roche, A.F.; Matorell, R. Anthropometric Standardization Reference Manual; Human Kinetics: Champaign, IL, USA, 1991. [Google Scholar]
- Slaughter, M.; Lohman, T.; Boileau, R.; Horswill, C.; Stillman, R.; Loan, V.; Bemben, D. Skinfold Equations for Estimation of Body Fatness in Children. Biology (Basel) 1988, 60, 709–723. [Google Scholar]
- Nagy, E.; Vicente-Rodriguez, G.; Manios, Y.; Béghin, L.; Iliescu, C.; Censi, L.; Dietrich, S.; Ortega, F.B.; De Vriendt, T.; Plada, M.; et al. Harmonization process and reliability assessment of anthropometric measurements in a multicenter study in adolescents. Int. J. Obes. 2008, 32, S58–S65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- España-Romero, V.; Ortega, F.B.; Vicente-Rodríguez, G.; Artero, E.G.; Rey, J.P.; Ruiz, J.R. Elbow Position Affects Handgrip Strength in Adolescents: Validity and Reliability of Jamar, DynEx, and TKK Dynamometers. J. Strength Cond. Res. 2010, 24, 272–277. [Google Scholar] [CrossRef] [PubMed]
- España-Romero, V.; Artero, E.G.; Santaliestra-Pasias, A.M.; Gutierrez, A.; Castillo, M.J.; Ruiz, J.R. Hand Span Influences Optimal Grip Span in Boys and Girls Aged 6 to 12 Years. J. Hand Surg. Am. 2008, 33, 378–384. [Google Scholar] [CrossRef]
- Ruiz, J.R.; España-Romero, V.; Ortega, F.B.; Sjöström, M.; Castillo, M.J.; Gutierrez, A. Hand Span Influences Optimal Grip Span in Male and Female Teenagers. J. Hand Surg. Am. 2006, 31, 1367–1372. [Google Scholar] [CrossRef]
- García-Calvo, T.; Sánchez-Oliva, D.; Leo, F.M.; Amado, D.; Pulido, J.J. Effects of an intervention programme with teachers on the development of positive behaviours in Spanish physical education classes. Phys. Educ. Sport Pedagog. 2016, 21, 572–588. [Google Scholar] [CrossRef]


{kind=link}
| Initial Meeting | Initial Measure | Development of the Sessions | Final Measure | Follow-Up Post Intervention | |
|---|---|---|---|---|---|
| Control Group | X | X | X | ||
| Experimental Group | X | X | X | X | X |
| Assessment in Both Groups | |||||
| Lifestyle variables | |||||
| Physical activity (self-reported and Actigraph) | X | X | X | ||
| Sedentary behaviour | X | X | X | ||
| Body dissatisfaction | X | X | X | ||
| Adherence to the Mediterrean diet | X | X | X | ||
| Regulation of behaviour in physical exercise | X | X | X | ||
| Satisfaction with life | X | X | X | ||
| Positive and negative affect | X | X | X | ||
| Anthropometric measure | |||||
| Weight and height | X | X | X | ||
| Skinfold | X | X | X | ||
| Waist circumference | X | X | X | ||
| Neck circumference | X | X | X | ||
| Physical fitness | |||||
| Cardiorespiratory fitness | X | X | X | ||
| Handgrip strength | X | X | X | ||
| Lower limb strength | X | X | X | ||
| Shuttle run test | X | X | X | ||
| Phases | Weeks | Aerobic Training | Strength Training | Socialization | Speed |
|---|---|---|---|---|---|
| Familiarization | 1 | INITIAL MEASURE | |||
| 2 | XX | X | XXX | X | |
| 3 | X | X | XXX | X | |
| 4 | XX | X | XX | X | |
| Month 1 | 5 | XX | X | XX | XX |
| 6 | XX | XX | XX | X | |
| 7 | XX | XX | XX | XX | |
| 8 | X | XX | XX | X | |
| Month 2 | 9 | X | XX | XXX | XX |
| 10 | XX | XX | XX | X | |
| 11 | XX | X | XX | XX | |
| 12 | XX | X | XX | X | |
| Month 3 | 13 | X | X | XX | XX |
| 14 | X | XX | XX | X | |
| 15 | XX | XX | XX | XX | |
| 16 | XX | X | XX | X | |
| 17 | X | XX | XX | X | |
| Month 4 | 18 | X | X | XXX | XX |
| 19 | X | XX | XX | X | |
| 20 | XX | X | XX | X | |
| 21 | XX | X | XX | X | |
| 22 | X | X | XXX | X | |
| 23 | FINAL MEASURE | ||||
| 3 months later | FOLLOW-UP POST INTERVENTION | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Miguel, P.A.; Vaquero-Solís, M.; Sánchez-Oliva, D.; Pulido, J.J.; López-Gajardo, M.A.; Tapia-Serrano, M.A. Promoting Healthy Lifestyle through Basic Psychological Needs in Inactive Adolescents: A Protocol Study from Self-Determination Approach. Sustainability 2020, 12, 5893. https://doi.org/10.3390/su12155893
Sánchez-Miguel PA, Vaquero-Solís M, Sánchez-Oliva D, Pulido JJ, López-Gajardo MA, Tapia-Serrano MA. Promoting Healthy Lifestyle through Basic Psychological Needs in Inactive Adolescents: A Protocol Study from Self-Determination Approach. Sustainability. 2020; 12(15):5893. https://doi.org/10.3390/su12155893
Chicago/Turabian StyleSánchez-Miguel, Pedro Antonio, Mikel Vaquero-Solís, David Sánchez-Oliva, Juan J. Pulido, Miguel A. López-Gajardo, and Miguel Angel Tapia-Serrano. 2020. "Promoting Healthy Lifestyle through Basic Psychological Needs in Inactive Adolescents: A Protocol Study from Self-Determination Approach" Sustainability 12, no. 15: 5893. https://doi.org/10.3390/su12155893
APA StyleSánchez-Miguel, P. A., Vaquero-Solís, M., Sánchez-Oliva, D., Pulido, J. J., López-Gajardo, M. A., & Tapia-Serrano, M. A. (2020). Promoting Healthy Lifestyle through Basic Psychological Needs in Inactive Adolescents: A Protocol Study from Self-Determination Approach. Sustainability, 12(15), 5893. https://doi.org/10.3390/su12155893