1. Introduction
Radon is the second biggest cause of lung cancer globally, after tobacco smoking, and accounts for about 3% to 14% of all lung cancers [
1,
2]. Each year, radon exposure-related lung cancer fatalities are estimated to be around 18,000 in Europe [
3] and 21,000 in the USA [
4]. Smokers are particularly vulnerable as they are estimated to be 25 times more at risk of developing lung cancer from radon exposure than non-smokers [
2]. Exposure to radon gas has also been associated with other types of cancer such as skin cancer, stomach cancer, brain cancer, and chronic lymphocytic leukaemia, but the evidence is not yet deemed conclusive by the World Health Organisation (WHO) [
1] (p. 14). In Ireland, radon is estimated to cause approximately 300 lung cancer cases every year, representing 12% of all annual lung cancer cases [
5].
Indoor radon concentration levels are measured in becquerels per cubic meter (Bq.m
3) and tested by placing detectors inside dwellings. If home levels are found to be above the national reference level (the maximum accepted radon concentration in a dwelling) of 200 Bq.m
3 (300 Bq.m
3 for workplaces), the procedure is that the test provider recommends remediation work, which usually involves the installation and maintenance of fans known as radon sumps [
6]. Preventative measures include the installation of plastic sheets in the foundation of a house during construction, to avert radon seeping inside over time [
1].
Although a significant percentage of radon-related lung cancer is diagnosed each year in Ireland and mitigation measures are arguably simple, both Irish communities and the Irish legislature have been slow to take radon seriously as a public health issue. Consequently, there is a lack of policies to identify, monitor, and mitigate indoor radon pollution to reduce exposure risk. Given that the evidence connecting radon exposure to heightened lung cancer risks is so compelling, the critical question is: why does Ireland still lack well defined and universally applicable indoor radon pollution-related public health policies that support remediation of radon pollution and improve human health and wellbeing? In this paper, we examine the Irish radon policy case study to answer this question. We critically evaluate why, even when evidence exists that radon exposure is harmful to human health, evidence-based policies can still be under-effective in promoting better human health policies. In doing so, we also point towards some of the inherent challenges of pollution-related public policymaking that are similar to non-radon pollution and applicable in non-Irish contexts in other parts of the world.
We have arranged the remainder of this paper in six sections. The next section introduces evidence-based policy, how it works, and its lacunae as identified in the public policy literature.
Section 3 deals with radon and its significant impacts on human health as an indoor air pollutant.
Section 4 briefly addresses the methods used in conducting the research presented in this paper.
Section 5 presents the findings,
Section 6 discusses the findings, and
Section 7 contains recommendations to policymakers for implementing sustainable radon policies and conclusions.
2. Evidence-Based Policymaking
Politicians in the UK repeatedly claim to be “following the science” when implementing policy decisions during crises, the COVID-19 pandemic being a recent illustration of this pattern [
7]. This claim has been criticised by scientists because it suggests that science offers a single answer that is both simple and easily translated into policy, while ignoring the complexities of the scientific practice and the diversity of scientific views that exists within and across disciplines [
7,
8].
Of course, scientific evidence can be, and often is, used to inform policy decisions around public health. In other words, the use of rigorous and well-tested evidence can identify what works to reduce any unintended harm caused by policies implemented to improve human wellbeing. Baron [
9] (p. 40) defines evidence-based policy as the “application of rigorous research methods, particularly randomised controlled trials (RCTs), to build credible evidence about “what works” to improve the human condition; and the use of such evidence to focus public and private resources on programs, practices, and treatments (“interventions”) shown to be effective.” In essence, the notion of evidence-based policymaking implies that policy decisions should be based on, or informed by, the best available evidence [
9,
10,
11]. However, the default presupposition of this way of thinking is that policies backed by evidence are a good thing and can be amply trustworthy.
Evidence-based policymaking has gained popularity in recent times; in many countries, politicians are judged on how they emphasise and prioritise using evidence when formulating and implementing policies, rather than depending on traditions, public perceptions, or popular sentiments [
12,
13].
However, while the concept of evidence-based policy may appear simple on first consideration, it is actually very complex to put into practice. This is because it requires different kinds of evidence from different disciplines to be understood and engaged with by different stakeholders—including researchers, policymakers, and sections of the public—and integrated into law. Critics have argued that public policymaking is different from technical decision-making, given that multiple incongruent, yet coincidental, public policy problems requiring different trade-offs often contradicting each other can exist [
14,
15]. Public policy issues are often too complex to be supported by evidence of an ideal solution, such as climate change or poverty eradication which Rittel and Webber [
16] famously termed “wicked problems” (p. 155). Therefore, policymaking is different and arguably far more complicated than decision science, given that, at any point in time, multiple ideas, values, and norms that are continuously struggling to attain significance over others may coexist in a policy landscape [
15,
17].
These complexities are evident when integrating knowledge and practices into health policies, such as those around air pollution, exposure to radon and asbestos, drinking water contamination, and the spread of new viruses such as COVID-19.
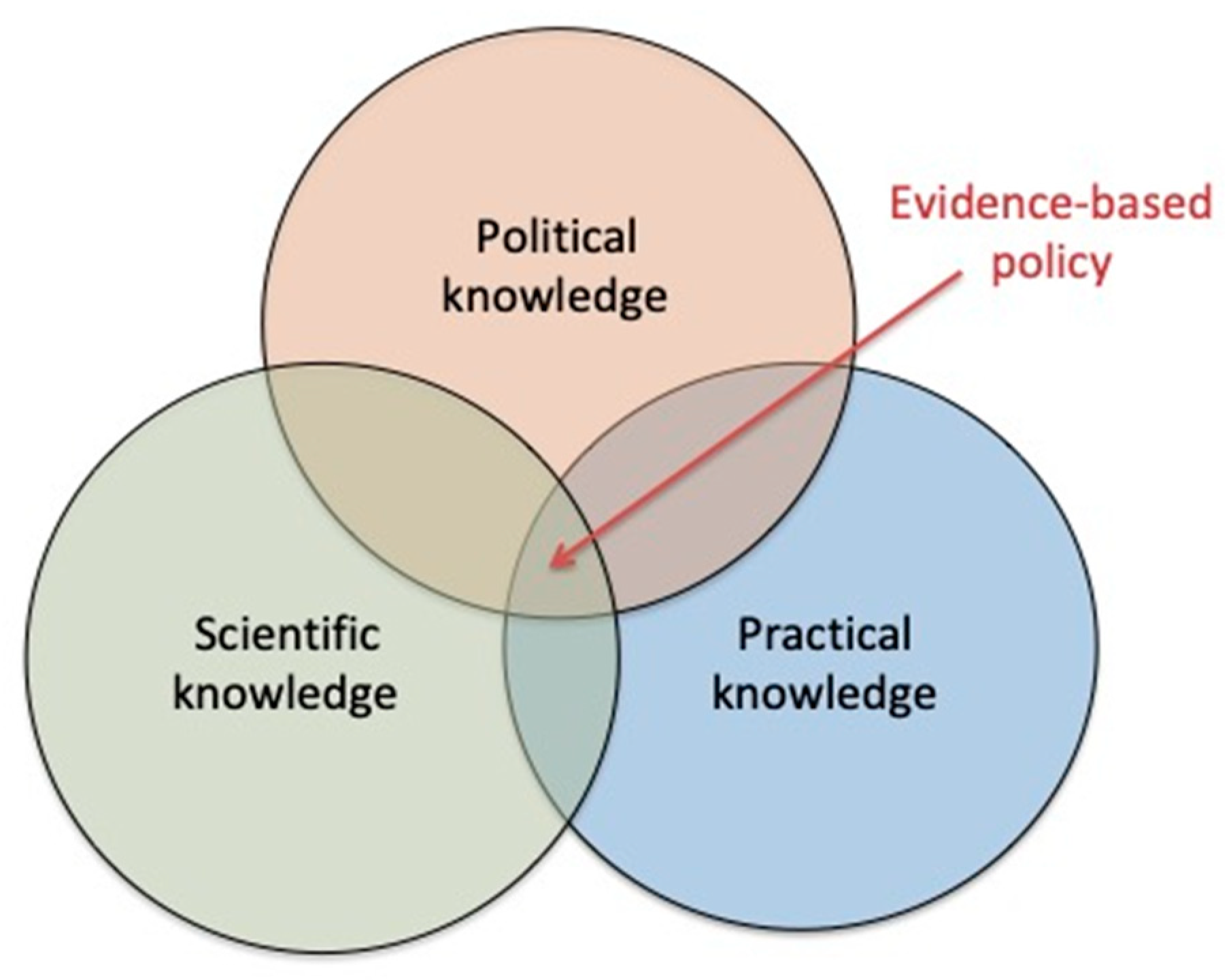
Navigating through these criticisms of evidence-based policymaking in order to find a solution, Head [
18] argues that there are three pillars of knowledge that have to be integrated in order to develop and build evidence-based policies. These are: political knowledge, scientific knowledge, and practical knowledge. Within this framework, policymakers, scientists, and practitioners need to pool and combine their respective forms of knowledge in order to develop evidence-based policies effectively. Figuratively, this would mean that evidence-based policymaking should exist where political knowledge, practical knowledge, and scientific knowledge intersect with each other, as pointed out in
Figure 1.
Ideally, evidence-based policies should be situated at the interface discussed above, but putting this into practice remains challenging. A classic policy cycle consists of five stages: the policy problem identification stage, policy formulation stage, policy decision-making stage, policy implementation stage, and policy monitoring and evaluation stage (see
Figure 2). Alternatively, these stages are also known as agenda-setting, policy formulation, adoption, implementation, and evaluation [
19]. Evidence can play an important role in informing policy at all of these stages, though it is not always invoked by policymakers. In the initial stage, practical and scientific evidence is critical in helping to identify a policy problem. At the policy formulation stage, practical and scientific evidence may be gathered to find relevant information to inform the current state of a social, economic, or environmental problem that needs to be solved through policymaking. Ideally, after gathering adequate information, policymakers propose a range of interventions to address the policy problem. In doing so, policymakers can use different tools such as regulations, standards, guidelines, grants, subsidies, taxation, and awareness-raising initiatives. Based on the evidence, different sets of policies are designed using various combinations of tools. In the next stage of policy decision-making, existing evidence is again brought into the picture to make a policy decision. Evidence should also play an important role in the monitoring and evaluation stage, though this type of evidence is rarely invoked. In the final stages of policymaking, the loop is completed, and new evidence may be gathered to inform future policymaking processes.
It is important to note that such a theoretical model about policy cycles is a simplification of the reality; policy decision-making does not strictly follow these steps and many dynamics and nuances are not captured in such a model. In particular, decisions are not made solely based on evidence, as the individual values, political inputs, and political agendas of policymakers also influence decision-making. However, this cycle can help to understand at which stages knowledge integration could take place and through which avenues this may can be achieved. We aim to explore this in this paper by utilising the case of indoor radon policy in Ireland, since it illustrates very nicely the complexities of evidence-based policymaking in a public health context.
Focusing on indoor radon, we investigate the different types of evidence available to policymakers through the lenses of political, scientific, and practical knowledge (
Figure 1). Using this case study, we highlight the difficulties of balancing and integrating information from multiple disciplines and perspectives, especially when a mix of natural sciences and social sciences is taken into account. We argue that, in order to develop evidence-based health risk policies, input from multiple scientific areas is crucial, and, on the basis of our analysis, suggest that a transdisciplinary perspective, defined as a holistic approach that subordinates disciplines, looking at the dynamics of whole systems [
20], needs to be adopted by policymakers in the context of indoor radon. We end by providing lessons learned and recommendations for evidence-based policymaking when it comes to public health hazards such as radon. In doing so, we also illustrate how sustainable policies can manage problems such as indoor pollution.
3. Indoor Radon Pollution
Radon is a naturally occurring, radioactive gas formed in the ground through the radioactive decay of uranium, which is present in all rocks and soils in varying concentrations [
1,
21]. Uranium concentrations in rocks and soils are usually low (1–3 parts per million, ppm), but can be as high as 100 ppm [
21]. If radon’s decay products are inhaled, they deposit in the airways and lungs, and can lead to lung cancer [
1,
2]. Outdoor radon does not constitute a health problem, but it can be drawn into buildings from the ground [
6]. Radon gas, which has no colour, taste, or smell, can enter buildings through cracks in the floor or gaps in pipes and cables, and accumulate indoors [
6], leading to potentially dangerous high concentrations. Indoor radon concentrations will depend on the geology of an area (e.g., [
4]), the permeability of its soils (for example, radon can move more easily through sand than clay), and the design of a house. Indoor radon can also vary considerably from day to day due to changes in weather conditions and ventilation rates [
6]. In colder months, when buildings are sealed off to prevent heating leakage, indoor concentrations of radon can increase as cold air from the outside is drawn indoors through cracks and fissures, as shown in
Figure 3. Groundwater used in many households, especially in rural areas in countries like Ireland, can also be contaminated with radon if it is present in the surrounding rocks and soil (
Figure 3). When radon-exposed water is used in households, the gas can further escape in the house, increasing the indoor radon concentration. Therefore, people spending more time indoors, which is especially common in countries with abundant rainfall such as Ireland, are at risk of prolonged radon inhalation [
22]. In Ireland, previous studies have identified that around 10% of the total population (approximately 460,000 people) may be exposed to indoor radon concentrations above 200 Bq.m
3 [
23].
Raising awareness of radon pollution, preventive measures (e.g., barriers under the floor, fans, and radon sumps), and ways to remediate (e.g., sealing of cracks and gaps in the floor, increased indoor and under-floor ventilation, and radon sumps) is critical to minimise radon inhalation-induced health impacts. However, as mentioned earlier, even with 10% of the population exposed to indoor radon pollution in Ireland, both the Irish public and its legislature have been slow to take radon seriously as a public health issue. In the subsequent sections of this paper, we seek answers as to why this is the case and provide recommendations for how this can be changed.
4. Materials and Methods
Secondary data gathered from documents were the main source of information required to analyse the case of indoor radon pollution. This type of qualitative method helped in contextualising, interpreting, and understanding the various dimensions relevant to why radon policies are where they are currently in Ireland and in identifying the main obstacles in the policymaking path.
In general, a qualitative case study approach is best suited for investigating current practices as well as addressing “how” and “why” questions (see [
25,
26]). A case study approach was used to systematically explore why radon policies in Ireland are not yet strong and establish how the nexus of political knowledge, scientific knowledge, and practical knowledge plays a critical part in the evolution of evidence-based policies. To begin the empirical work, an inventory was made of relevant national-level policies, reports, and position papers published by different scientific bodies in Ireland. Included also in this inventory were the reports of the National Radon Forum held in Ireland each year since 2002. These forums act as a central platform to report on the progress on radon policies by the national agencies working on radon and highlight the persistent challenges. Content analyses of these documents helped to identify some broad trends in the documents and allowed us to identify themes such as political knowledge, scientific knowledge, and practical knowledge.
After the content of the government agency documents was analysed, purposive document sampling was used to identify and select documents that contained rich information [
27] on radon exposure, radon awareness, radon policies, and other related topics. Qualitative research methods based on purposive document sampling can help explore and obtain an in-depth understanding of why evidence-based practices and policies are either successes or failures [
28]. We began by searching for documents mainly online using search terms like “radon”, “radon policies in Ireland”, “radon risk in Ireland”, “radon awareness in Ireland”, “radon policies in the European Union”, and similar others. Similar terms were also used to search Scopus, Web of Science, JSTOR, and Google Scholar for journal articles on the topic. Through iterative processes of using different search terms, a saturation of information was achieved with no new substantive information that could be acquired, especially with the a priori limits set by the theoretical framework used in the study [
29,
30]. Each document was coded into thematic areas according to how it informed policy with respect to political knowledge, scientific knowledge, and practical knowledge. As we intended to achieve both an in-depth and broad understanding of this issue, following these qualitative methods helped us gather a wide range of information from journal articles, reports, guidance notes, websites, newspaper articles, and other documents on radon in Ireland and other countries.
5. Results: Knowledge Dimensions in Policy Development around Radon
The first step in exploring policy around indoor radon is to understand the three knowledge dimensions that are relevant to this public health hazard (
Figure 1). To this end, we analysed the data gathered from purposive document sampling and divided it into three parts to determine the level of political, scientific, and practical knowledge around radon in Ireland.
While doing so, we identified repetitive themes as the main challenges relevant to each knowledge dimension, which are creating obstacles in the formulation and implementation of radon-related, evidence-based policies in Ireland. Below, we explore each knowledge dimension in turn, discussing the challenges it presents to the policymaking process. As we will see, these knowledge areas do not exist in isolation, but naturally interact and overlap with each other, which is an essential consideration when trying to integrate them into policymaking.
5.1. Political Knowledge
In the realm of public policymaking, at any given time, there are a host of public policy issues that require legislation of one type or another which are vying for the attention of policymakers. However, while some public problems end up being addressed by policies, others are ignored. Which policy problems are addressed by legislation and which are not depends on how different political actors understand, judge, and evaluate events from their perspectives, focusing on how the legislation would harm or benefit the people who keep these political actors in position As a result, political actors employ a host of tactics such as advocating for, pursuing, negotiating, undermining, communicating, and a slew of other methods to make or break a policy as early on as during the problem identification and agenda-setting stage of the policy cycle (see
Figure 2). Therefore, when policy entrepreneurs [
31] promote a specific policy to become legislation using tactics such as lobbying and negotiating, other political actors may try to create obstacles for them. These obstacles may also arise from the fragmentary nature of political knowledge, whereby local politicians are expert in and lobby for particular areas of geography or knowledge, or from the timescales of political discourse which may not coincide with those needed to develop regulations, or from the interests of politicians contrasting with those of other stakeholders. In the remaining part of this section, we point out how different forms of incongruity between political actors and how they envisage radon policies have hindered the formation of stronger radon-related policies in Ireland.
The first set of radon-related policies in Ireland came into effect with the introduction of amended building regulations in 1998, requiring all homes built since July 1998 in high-radon areas (areas where the probability of a dwelling having an indoor radon concentration above the reference level of 200 Bq.m
3 is 10% or higher) to be installed with radon barriers during construction [
32,
33]. These regulations outline the steps to be taken during the design and construction of a building to lessen the risk of radon concentration building up. These include the installation of barriers in the form of fully sealed membranes (plastic-type sheets) with low permeability under the floors of a house [
31]. Parameters, standards, and performance levels of the membranes are outlined in the regulations [
31]. Additionally, the regulations require all new homes to be fitted with a standby radon sump (a pipe under the foundations that connects to the outdoor air) during construction. The sump can be activated by adding a fan if high radon concentrations are subsequently identified [
34]. Specifications of the sump pipes, such as the fitting of caps on the pipework to prevent ingress of water or rodents, are also detailed in the regulations [
31]. These regulations have indeed been effective, given that average indoor radon concentrations in Irish homes are estimated to have decreased from 89 to 77 Bq.m
3 since the introduction of the regulations [
5] (feeding into the monitoring and evaluation phase of the policy cycle). In addition, measurements on local authority homes in a number of high radon areas in Ireland have allowed the impact of these new regulations to be assessed, and a reduction of up to 70% in the mean radon concentration was observed in homes built since 1998 relative to those built before this date [
33]. However, it must be noted that these regulations only concern buildings that are built after 1998, and fail to take into account older buildings.
The exclusion of houses built before 1998 from this radon policy (as part of the formulation phase of the policy cycle) is problematic in the context of solving the radon exposure problem in Ireland, where many houses in cities and rural areas are older than that, yet equally at risk. Borrowing from Ricciuti [
35] the concept of political fragmentation, we argue that these radon policies, which are applicable only to new buildings and inconsequential for older buildings, suffer from a kind of fragmentation, which is a first challenge with respect to evidence-based policymaking. Specifically, we use the term fragmentation to refer to the fragmentary nature of political knowledge, where local politicians are experts in specific areas of knowledge and not others, or may exclude some constituencies knowingly out of the purview of a policy in order to reduce conflicts. This fragmentary knowledge leads to fragmentary regulations, which account for some but not all public health hazards posed by indoor radon. As such, regulations may be valid for one geographical area but not another, or one type of property but not another, resulting in a piecemeal approach to policymaking.
A second challenge stems from the timescale of political discourse: politicians necessarily follow timescales dictated by election cycles, which means regulations which take longer to develop may fall through the cracks. In Ireland, national radon regulations in the early stages of development (policy formulation phase) have recently fallen prey to shifting governments and have failed to be enacted. In January 2020, a bill which sought to require rented properties to be tested for radon gas lapsed with the dissolution of the Irish Parliament. The “Healthy Homes Bill”, which was introduced into the Irish Parliament in February 2019, would have made radon testing of rented accommodation mandatory for landlords [
36]. Specifically, it stated that “the Minister shall make regulations to require testing for radon and to the adoption of remedial measures where tenants may be exposed to dangerous concentrations of radon” [
36] (p. 4). However, due to elections that were held in February 2020, this bill was shelved. With a new government in power, it remains to be seen whether this bill will be reintroduced and whether it will be expanded to account for properties other than rented, given that it only applied to rented homes, omitting other types of properties, illustrating once again the fragmentary nature of these policies.
When discussing the challenges inherent in building up adequate political knowledge for evidence-based policies to come into effect, a third consideration, specifically in the Irish case, comes to the fore. As Ireland is a member of the European Union, the impetus for specific legislation can come from EU directives or recommendations. This is especially useful when policies lack a significant amount of political appeal or the presence of policy entrepreneurs who will lobby and negotiate for them to materialise. As a supra-national entity, the European Union can exert pressure on member countries to institute policies that help build political knowledge, and we see instances of this in the case of radon policy in Ireland. In 2010, the Health Service Executive, Ireland’s public health service, and the Radiological Protection Institute of Ireland (RPII), an independent public body which has now merged with Ireland’s Environmental Protection Agency (EPA), issued a joint position statement recommending the development of a National Radon Control Strategy (NRCS) as a coordinated response which would align with EU directives [
37]. The NRCS was set up four years later by the government as an interagency group to “develop recommendations on a broad range of measures to reduce risk from radon to people living in Ireland” [
38] (p. 2). These measures were articulated in a four-year action plan and included setting up a website (
www.radon.ie), public information campaigns, an advice hotline, public perception studies, and cost-effectiveness analyses. In 2019, a European directive [
39] requiring EU member states to address the risk of radon and other radiation was transposed into Irish law [
40], just two days after the introduction of the “Healthy Homes Bill”. This resulted in the lowering of the reference level of indoor radon in the workplace in Ireland from 400 to 300 Bq.m
3.
In summary, much remains to be done by Irish politicians to address the public health issue of radon exposure with its severe human health impacts. In examining political knowledge and integrating it with other knowledge areas, it must be considered that politicians make decisions on a timescale that is determined and bound by the election cycle, and seek to serve the interests of the electorate, while also following the directives of wider governing bodies.
5.2. Scientific Knowledge
The second type of knowledge that Head [
18] identifies as critical to evidence-based policymaking is rigorous scientific knowledge. However, scientific knowledge can come from different scientific disciplines and integrating these different disciplinary feedbacks is critical at all phases of the policy cycle. Multiple disciplines provide evidence relevant to indoor radon policymaking. Specifically, there are three key scientific areas that provide important evidence on radon risks that can be used by to develop an evidence-based radon policy: epidemiology, health psychology, and economics. Whilst these are the three main scientific areas [
1] relevant to policymaking around radon, other scientific disciplines, such as geoscience and behavioural science, also provide important information in the context of radon and should be drawn from by policymakers as necessary.
The combination and integration of these multiple scientific perspectives is crucial to develop an effective evidence-based radon policy, but this is a complex process, fraught with challenges. Below, we discuss the evidence from each of these research fields and the challenges they present when it comes to integrating scientific knowledge with political and practical knowledge.
5.2.1. Epidemiology
Epidemiology is “the study of how often diseases occur in different groups of people and why” [
41]. In the context of indoor radon, international epidemiological studies have focussed primarily on the relationship between radon exposure and lung cancer [
2,
42], indicating that indoor radon is responsible for a substantial numbers of lung cancers in the general population [
1]. Epidemiological evidence on radon was originally derived from studies of miners who were exposed to radon in underground uranium mines [
43,
44], and, more recently, from case–control studies (where individuals who have not developed lung cancer are treated as a control) investigating the association between lung cancer and indoor radon measurements [
44,
45,
46]. One of these studies [
45], which pooled data from two case–control studies conducted in China, encompassing 1050 lung cancer cases and 1996 controls, found an excess risk of lung cancer with increased residential radon concentration, consistent with other studies in North America [
46] and Europe [
2]. A North American study analysed 3662 cases and 4966 controls from seven studies in the USA and Canada, and found that the risk of lung cancer increased by 11% for every 100 Bq.m
3 increase in indoor radon. Another review paper, which gathered and reanalysed data from 13 European studies estimates that for every 100 Bq.m
3 increase in indoor radon, there is a 16% increase in the risk of developing lung cancer [
2]. The review found evidence for an increase in risk of developing lung cancer even when radon levels were below 200 Bq.m
3, the level commonly taken as that, above which, action is recommended, and it also estimated that radon in homes is responsible for about 2% of all cancer deaths in Europe [
2]. Thus, epidemiological evidence shows that there is no such thing as a safe level of indoor radon, which is an important message that should be communicated amongst stakeholders such as homeowners. As the WHO writes in its Handbook on Indoor Radon [
1] (p. 12), these three pooling studies present “a very similar picture of the risk of lung cancer from residential exposure to radon. There is overwhelming evidence that radon is acting as a cause of lung cancer in the general population at concentrations found in ordinary homes”. In conclusion, there is, to a large extent, consensus among epidemiologists that evidence provides clear indications that indoor radon is a significant public health hazard. Despite the evidence providing a clear answer as to the significance of the hazard, there is a continued push by scientists to come up with better measurements, better estimates of exposure to radon, priority areas, and risk maps. This push comes from a need to reduce the error level inherent in all types of measurements and epidemiological data.
5.2.2. Economics
As a range of radon remediation measures has been identified, a critical question arises on the costs and benefits of each of these measures, which typically falls under the study of economics. Cost-effectiveness studies should follow frameworks considered appropriate for the economic evaluations of health interventions [
47,
48]. In the case of health policies, looking at cost-effectiveness of preventive measures or of remediation is crucial because it helps assess the costs and benefits of different preventative and remedial actions [
1]. In the context of radon, cost-effectiveness studies examine the cost and benefits of preventive measures or of remediation in an effort to evaluate current policies and find new, more cost-effective ways of reducing radon risk (e.g., [
49]). When it comes to air pollution from indoor radon, the cost of testing, prevention, and remediation must be balanced against the cost of lung cancer treatment.
In Ireland, radon tests are relatively inexpensive (costing about EUR 50), and preventative measures cost a few hundred euro [
50]. Remediation works can be more costly (about EUR 1000), possibly contributing to low levels of uptake in the population (see
Section 5.2.3). Government grants are available, but only in high-risk areas [
6], leaving homeowners to cover the costs in low-risk areas.
In general, prevention and remediation are relatively simple and cost-effective solutions for householders [
50]. However, a recent study [
3] found that policies tasked with identifying and remediating existing homes with high radon levels in the UK are neither cost-effective nor able to reduce lung cancer mortality. The study authors argued that policies requiring basic preventive measures against radon in all new homes throughout the UK would be cost-effective. Similarly, the WHO [
1] argues that in many cases, it would be cost-effective to install radon prevention measures such as a radon barrier in all new buildings. These recommendations are relevant for Ireland, where current building regulations require the installation of a standby radon sump in new buildings, but do not require the installation of preventative barriers except in new buildings built in high-radon areas. The RPII also notes that standby sumps offer very poor cost-effectiveness because a very small proportion are converted into active sumps, thereby recommending that installing a passive sump instead of a standby sump upon construction would be more cost-effective [
50].
In general, cost-effectiveness of preventive measures improves as the average radon concentration in an area increases [
1]. However, when it comes to cost-effectiveness analysis, different measures of effectiveness can lead to results that are not comparable across studies [
1]. This lack of comparable evidence represents a huge challenge to policymakers [
49], and there is a need to develop consistent methods of cost-effectiveness analyses across countries and across studies. Only then will results be comparable across countries and contexts, and therefore, more useful to the policymaking process. It is also worth noting that, overall, economic evidence must be balanced against the degree of threat presented by the public health risk and considered in conjunction with all other forms of available evidence. Taking into account the cost of mitigation alone is not enough: it must be integrated with public health and quality of life costs, giving an overall, broad picture of the costs associated with this public health risk. Publicity and awareness campaigns also represent a cost and depend on the availability of funding [
50] and should be part of the equation.
5.2.3. Health Psychology
Health psychology “studies psychological factors related to how people stay healthy, why they become ill, and how they respond when they do become ill” [
51]. A known feature of health risks is that, when people do not experience the immediate negative consequences of potential health risks (e.g., smoking, eating unhealthy food, and alcohol consumption), they are often reluctant to take action. This effect is particularly strong when people underestimate or are largely unaware of health risks [
52], such as risks derived from radon exposure [
53]. Conversely, people who perceive risks are more likely to take health protective behaviours, but only if they actually feel in control of their actions and able to reduce the risks [
54].
Indoor radon, testing, prevention, and remediation are relatively simple and cost-effective solutions [
50], yet testing, prevention, and remediation rates are generally low [
55,
56]. In Ireland, a survey conducted in 2005 with people who had been advised by the RPII to consider remediation found that only 22% of the householders (from a total of 1058 respondents) took action [
35]. Similarly, a later survey-based study [
50] estimated that when radon levels are above the reference level, remediation takes place in less than 25% of cases.
This low level of uptake and action may relate to ineffective communication tactics. Research suggests that simply informing people that they are exposed to high indoor radon levels is often not enough for them to take action (cf., [
52]). In fact, typically, information provision (through publicity campaigns, media, or public talks) tends to assume that there exists a knowledge deficit or gap in the audience that needs to be filled (cf., [
57]). However, the underlying reason for a lack of action is usually much more complex.
Radon, being colourless, odourless, and tasteless, does not provide sensory cues that may motivate people to act. Hevey [
55,
56] argues that risk has both cognitive and emotional aspects, and that the social context in which radon threat occurs (including community, cultural, and social values) is an important consideration. He points out [
56] that a number of cognitive heuristics (“mental shortcuts”) impact people’s risk perception of radon. Moreover, he writes, “the threat from radon can easily be downplayed to justify inaction” (p. 4), since it can easily be perceived as distant, uncertain, and easily discounted [
55,
56]. In addition, information about the serious health risks posed by radon may trigger fear responses and result in defensive coping mechanisms (“defensive systematic programming”) which inhibit behaviours such as testing and remediating [
55,
56].
Following a survey administered to 106 people living in a high-radon area in Ireland, Clifford and colleagues [
53] report that overall radon knowledge was quite high, and “no relationship was found between radon knowledge and testing one’s home for radon” [
53] (p. 146). The survey suggested that the main reason people do not test their home for radon is that they believe their home does not have a problem. Clifford and colleagues ascribe this belief to “optimistic bias”, defined as the tendency of people to think that their risk is less than that of their peers. Participants’ beliefs about what other people think about the behaviour and whether they perform the behaviour were also deemed to be an important contribution in the variation in intentions to measure one’s home for radon. In addition, some homeowners are reluctant to test for radon in case their property becomes devalued as a result [
53]. Alternatively, people may be under the “illusion of control”, suggesting that they feel they can reduce or eliminate risks, which is a factor in other health risks areas [
58]. Such unrealistic feelings of being in control can suppress perceptions of health risks and, subsequently, lead people to ignore information about these risks [
54].
Finally, people have a tendency to attribute positive characteristics to natural products, especially when they are not interfered with by people [
59,
60]. Typically, people associate positive feelings to “natural” products [
54], sometimes even when referring to harmful trace elements such as uranium [
52]. Radon is a naturally occurring gas, and it may well be that people have positive associations with this natural pollutant.
In summary, there is a significant behavioural component when it comes to health risks related to radon gas. However, as yet, there has been relatively little research into people’s motivations in testing, preventing, and remediating when it comes to radon gas-related health risks. Hence, there is a need for research on health psychology and mitigation behaviour around radon-related health risks. In addition, current intervention strategies seem largely ineffective in changing these behaviours, and there is a dire need to develop more effective intervention strategies.
5.2.4. Integrating Scientific Knowledge in Evidence-Based Policy
The process of integrating scientific knowledge in evidence-based policy is fraught with challenges. The first challenge relates to integrating different types of scientific evidence. Relevant evidence from epidemiology, economics, health psychology, and other disciplines such as geoscience, social science, and behavioural science must all be taken into account and integrated into policy at each stage of the policy cycle. Specifically, it is critical for multidisciplinary scientific knowledge to feed into policy formulation, decision-making, and adoption, but also in the later phases of monitoring and evaluation. In discussing radon risk, Hevey [
56] argues that radon risk communication strategies need to adopt a multidisciplinary perspective including expertise from the field of psychology. Ultimately, Hevey argues, a psychological perspective that takes normative complexity into account is well placed to inform risk communication, given that how an individual perceives the risk of radon, as opposed to relying on knowledge of radon, will determine his or her decision-making regarding testing and remediation [
56].
Further, the nature of scientific evidence presents another challenge. Scientific evidence is rarely definite, nor is there usually a consensus about the results. This means that there is always a level of uncertainty around the scientific knowledge used in policy decisions. In discussing the role of scientists in public policy, Oreskes [
61] (p. 370) points out that within a scientific community, “different individuals may weigh evidence differently and adhere to different standards of demonstration, and these differences are likely to be amplified when the results of inquiry have political, religious, or economic ramifications”. The limitations that are inherent in any kind of scientific evidence need to be considered by policymakers in order for them to properly assess uncertainty and risk, and ultimately, make informed policy decisions. This will necessarily involve policymakers talking to scientists (who often take on the role of scientific advisors) about scientific uncertainty, statistical robustness of results, and margins of error right from the early phases of the policy cycle. In addition, there is a need for further applied research to reduce uncertainty around radon measurements and concentrations.
Another challenge is related to competing timescales of the involved actors. The pace of scientific research is often dictated by data gathering, data processing, and publication timelines, as well as funding mechanisms. Given that funding for scientific research, from the government or from industry partners, can wax and wane [
62], the accrual of scientific knowledge may suffer periods of stasis. Publications, one of the chief outputs of scientific knowledge, may take years to be prepared and are often hidden behind paywalls or otherwise inaccessible to non-scientists who may not know where to look for them or have an interest in them. This may be linked to the poor levels of uptake and awareness associated with radon health risks. The timescales of science must contend with political timescales, which are dictated by election cycles and short-term political goals. These competing timescales will be particularly challenging during the policy adoption and implementation phases of the policy cycle, when politicians may require access to data and results.
This leads on to an additional challenge, namely that posed by scientific terminology. Scientific knowledge is shrouded in highly specialised jargon that will be poorly understood by stakeholders outside of academia or specific disciplinary fields. This makes scientific knowledge inaccessible and, therefore, often not considered by non-scientists. Systematically integrating scientific knowledge into policies is a real challenge at all phases of the policy cycle, and may be overcome by policymakers being advised by scientists and science communicators, who can translate scientific jargon into understandable language that is useful to policymaking. However, it is worth noting that repeated interactions with the same scientists or communicators may lead to biases, given that any scientist or science communicator will bring their own particular views and experiences to the table when considering a given public health issue.
At the same time, scientists must be willing to communicate the findings of their research with politicians in a way that is accessible and easy to understand, such as through media and during formal and informal meetings with policymakers. This is a challenge in itself, given that, in academia, there are usually few reward mechanisms (e.g., promotion or tenure criteria) in place to encourage scientists to engage with policymakers. In addition, the monitoring and evaluation of policies should rely on scientific research methods, which is typically the expertise of social scientists [
63].
5.3. Practical Knowledge
Head [
18] (p. 6) defines practical knowledge as the practical wisdom of professionals in their communities of practice and “the organizational knowledge associated with managing program implementation”. As such, it encompasses the public sector, the private sector, and non-governmental organisations. In the context of indoor air pollution from radon, environmental measurements of indoor radon have been undertaken by public bodies in Ireland to gather radon data that are useful to scientists and policymakers at the problem identification, policy formulation, and monitoring and evaluation stages. Contractors and suppliers of radon test kits, as well as those who carry out remediation work, also hold practical knowledge, as well as benefiting from the business of radon testing and remediation.
In the 1990s, the RPII carried out a national survey in homes “to determine, in detail, the geographical distribution of radon levels in dwellings throughout Ireland” [
64] (p. 2). It reported an Irish average indoor radon concentration of 91 Bq.m
3, which is higher than the European average of 59 Bq.m
3 [
65]. The survey results were used to construct a “risk map” of Ireland predicting the percentage of homes with radon above reference levels in 10 × 10 km grid squares visualised on the map. It is worth noting that there is considerable uncertainty in the risk levels in the map, given that it was based on a minimum of only five sampled dwellings per grid [
64]. Error levels and uncertainty are therefore examples of challenges that come with this kind of practical knowledge. Much like in the case of scientific knowledge, there is thus a need to reduce error in measurements and uncertainty levels when it comes to radon concentration. This can be achieved through further measurement campaigns and applied research linking back to the scientific knowledge dimension.
Following completion of the national survey, the RPII set up a commercial radon measurement service [
34]. In July 2003, a radon measurement in a house in Castleisland, in a high radon area in Ireland, found an annual average radon concentration of 49,000 Bq.m
3, almost 250 times higher than the reference level of 200 Bq.m
3. A subsequent survey in the four national grid squares adjacent to the town of Castleisland found 52 homes (14% of those sampled) with radon levels above the reference level (i.e., above 200 Bq.m
3). The EPA, on its website, recommends that a radon test is carried out “within the first year of a new home being occupied” [
66]. While the reference level for homes is 200 Bq.m
3, that for workplaces is 300 Bq.m
3 [
66]. Hence, if the measured radon concentration in a home is above 200 Bq.m
3 and in a workplace, including schools, is greater than 300 Bq.m3, remedial action should be taken to reduce those levels [
6,
66]. In the context of remediation, the EPA recommends that homes whose result is above 800 Bq.m
3 be prioritised for early remediation [
6]. In its advice to local authorities, the EPA surmises that “the higher the radon concentration, the sooner radon remediation should be carried out” [
6].
Further radon measurements by the EPA and by academic scientists continue to be accrued and published each year (feeding into the monitoring and evaluation, and policy decision-making and agenda-setting phases). These scientific studies highlight the connection between practical and scientific knowledge. For example, indoor radon measurements have been used by scientists to estimate residential radon exposure [
5] and combined with other data, such as geological information [
23] and airborne radiometric data [
67], to develop radon risk maps. Significantly, in 2017, a high-resolution radon risk map of Ireland was developed based on 31,910 indoor radon measurements combined with geological information [
23]. This map, which shows the probability of indoor radon concentrations exceeding the reference level, improves the resolution of the older EPA indoor radon map of Ireland, which was developed based solely on indoor measurements [
23]. Of course, while surveys of radon concentrations help to identify the homes with the highest concentrations, they also represent a cost for the government [
34] and need to be considered alongside evidence from economic knowledge.
It is crucial that practical knowledge accrued and held by public bodies is discussed and communicated openly with communities impacted by the findings and with policymakers from relevant regions and county councils in Ireland. In turn, public bodies should also be aware and open to practical knowledge held by communities.
5.4. Integrating Practical Knowledge in Evidence-Based Policy
In the case of indoor radon in Ireland, practical knowledge on indoor air pollution is often held by public bodies. The main challenge that comes with integrating this kind of knowledge into evidence-based policy is that of effective communication between stakeholders at all phases of the policy cycle, from agenda-setting, through formulation, adoption, implementation, and evaluation. Radon data held by public bodies may be complex and will always be associated with levels of uncertainty and error. Public bodies need to communicate the findings of their radon surveys and measurements, as well as the reference levels above which remediation action is needed, in a clear and understandable manner to other stakeholders, including community members and policymakers. This may involve sending letters to households with information on remediation. The content of the letters will vary according to the level of radon detected in the dwelling (e.g., [
6]). In this context, local authorities (county councils in Ireland) should be aware of radon risks relevant to their area and have strategies in place for communicating these risks. This involves, as in the case of scientific knowledge, public bodies being open about the levels of uncertainty and error when communicating with other stakeholders. For instance, in its guidance to local authorities [
6] (p. 3), the EPA points out that “the reference level is not a rigid boundary between safety and danger but a guideline as to when one should consider taking action to reduce the radon concentration”. An efficient way of ensuring communication is effective could be to employ and tap into the expertise of science communicators who will know how to translate complex findings into understandable messages and will have an understanding of risk communication. Communication campaigns should be ongoing, rather than limited to one off meetings or interventions that are connected to specific data gathering phases. In addition, different audiences and publics will require targeted messages and communication strategies, depending on their needs, concerns, and knowledge [
55]. There is thus a need for targeted interventions, tailored to the needs and concerns of stakeholders such as local communities. Only through sustained engagement with communities will members of the public trust representatives of public bodies.
Contractors and suppliers of radon test kits who also hold practical knowledge should have clear guidelines and protocols from policymakers on what knowledge they should provide and through which channels they should provide it to stakeholders (mainly homeowners, renters, and business owners interested in testing dwellings for radon). As mentioned earlier, policymakers may employ the services of professional communicators in developing these guidelines and they can be made available on websites of public bodies and tailored to different audiences.
5.5. Summary
Purposive literature sampling allowed us to identify sources of evidence on indoor radon with respect to political, scientific, and practical knowledge. Our sample comprises documents dealing with indoor radon in Ireland and/or internationally, as well as practical and theoretical papers relevant to the case study of indoor radon in Ireland. Sources of scientific knowledge were further subdivided into epidemiological evidence, economic evidence, and health psychology-related evidence, and challenges related to integrating the scientific and practical knowledge dimensions into evidence-based policy were identified and discussed.
Some of the documents identified comprise both scientific and practical knowledge, while others comprise both political and practical knowledge. It is worth noting that political knowledge was the main focus of only four of the documents examined [
32,
36,
39,
40], with only two documents [
34,
37] encompassing both political and practical knowledge. This may be related to the nature of our sampling method, which was limited to written sources, while political knowledge may also be transmitted orally in formal or informal settings. Interestingly, none of the documents encompassed both scientific and political knowledge, and only one comprised all three types of evidence, namely the Irish EPA website dedicated to radon [
66]. Thus, there is a need for transdisciplinary studies looking at both scientific and political knowledge, and for studies encompassing all three types of knowledge, which is what the present study aims to achieve.
6. Discussion: Developing Evidence-Based Policy for Indoor Radon
We have illustrated how political, scientific, and practical knowledge are dimensions relevant to policymaking in the context of indoor air pollution from radon (
Figure 1). In order for evidence-based policymaking to take place, these different types of evidence need to be understood, balanced, and integrated into policy by policymakers in all phases of the policy cycle. However, given the complexities and challenges inherent in each knowledge dimension presented above, this is no easy task. Using the framework proposed by Head [
18], who argued that evidence-based policies could be successfully implemented when the three forms of knowledge mentioned above are well integrated, we argue that such integration is yet to be achieved in Ireland. Hence, radon-related policies are still not well-developed. Below, we suggest how this integration can be achieved.
The first step is to recognise these different knowledge dimensions and to acknowledge their validity. While, in the past, policy research has assumed that knowledge and practice are different entities and focused on bridging a knowledge gap in practice, recent research in policy has increasingly recognised that all types of knowledge are valid and useful [
10]. This is a key starting point in developing evidence-based policy.
Next, it is necessary to gain an understanding of the different knowledge dimensions. This includes understanding the limitations and uncertainties inherent in each one, as well as the timescales of operations, values, and interests of the different stakeholders involved.
An essential next step in evidence-based policymaking is then that of balancing and integrating these different types of knowledge. Integrating evidence from different disciplines to solve complex social problems requires a transdisciplinary approach [
20,
68,
69]. Satterfield and colleagues [
69], in describing trends in evidence-based practice, note that public health draws on practitioners from many disciplines, and describe a transdisciplinary model of evidence-based practice. In their model, decision-making is defined as the cognitive action that turns evidence into contextualised evidence-based practices. They argue that decision-making combines evidence from the population, resources, and context, and exists at the intersection of best available research evidence, a given population’s characteristics, state, needs, values, and preferences, and resources, including practitioners’ expertise. Therefore, Satterfield and colleagues [
69] suggest policy interventions ought to be considered at the interpersonal, organisational, community, and public policy levels.
In the context of radon, a transdisciplinary model would incorporate into decision-making scientific, practical, and political knowledge, taking into account the values and needs of the communities and stakeholders involved, as well as the expertise of politicians, public bodies, and scientists.
In the context of health care, Légaré and colleagues [
70] argue that interprofessional decision-making necessitates a shared goal of health care decisions based on patients’ values, a sense of trust among professionals, and leadership and organisational structures that facilitate shared decision-making in clinical care [
70]. The same need holds valid in the case of indoor radon, where stakeholders must establish a shared goal at the start. This may involve establishing a joint definition of success [
62]. Ultimately, successful interdisciplinary collaboration requires building trust between parties [
62]. Two-way, open communication is a necessary requirement of collaborations and essential to building mutual trust [
62]. This may involve identification of key communicators among key stakeholders to summarise the evidence available, and the needs and interests of each party. For instance, scientific advisors may act as a bridge between government and science, and certain scientists may take on the role of communicating with different communities or other stakeholders on public health messages, having taken into account all relevant scientific evidence, including from health psychology. In turn, communities may be represented by key spokespeople. Repeated meetings and sustained interactions are crucial in this respect [
62].
In integrating and balancing scientific evidence that comes from multiple disciplines, the establishment of a scientific advisory committee or task force for indoor radon would be well placed to develop recommendations for politicians and practitioners (e.g., [
71]). In Ireland, the NRCS was established as an interagency group to make recommendations on measures dealing with indoor radon [
38] (see
Section 5.1), but a transdisciplinary approach is yet to be achieved.
Crucially, an advisory committee on indoor radon would comprise representatives from all relevant scientific disciplines, and as such, would be able to evaluate the latest and best available scientific evidence and provide policy guidance to politicians. However, it would be naïve to suggest that scientific committees will always reach a clear consensus or can provide proof in matters of public health policy. As Oreskes writes [
61] (p. 380), the “scientific consensus is a complex process—involving a matrix of social, political, economic, historical considerations along with the epistemic—and history shows that its achievement typically requires a long time: years, decades, even centuries. But even when a stable consensus is achieved, scientific uncertainty is not eliminated.” Thus, when providing recommendations to policymakers, scientists need not concern themselves with providing “proof”, but rather point out the consequences of different political decisions, where possible. The committee should also include or hear from representatives who hold practical knowledge, including homeowners and test providers, and representatives of communities impacted by high levels of radon. Similarly, policymakers should genuinely be interested in understanding and applying the input from such scientific committees, and not install them as a check-box exercise.
In summary, in Ireland, ever since indoor radon has been recognised as a health hazard, the policy dial has remained firmly set on risk assessment and risk management, but this has been associated with low levels of public awareness and uptake, as acknowledged by NRCS public perception studies [
50]. In the context of indoor radon in Ireland, the evidence presented above suggests that a cost-effective approach, which may involve radon preventative measures to be put in place in all new homes, goes hand in hand with the introduction of legislation to ensure preventative measures are put in place in all households and places of work in Ireland. In parallel, effective communication strategies around radon are essential. As argued by Hevey [
56], radon awareness programs should consider segmenting their message to take into account different target audiences, such as individuals motivated and non-motivated to test for radon. It remains to the policymakers to integrate and balance the best available evidence in order to make informed decisions and, as we have argued above, this is best achieved through a transdisciplinary approach.
The case study of indoor radon in Ireland can inform other non-radon air pollution contexts, since the inherent challenges of radon pollution-related public policymaking we have illustrated above are similar to those of non-radon, household air pollution (e.g., asbestos, [
72]).
7. Recommendations
We have illustrated that evidence-based policymaking is complex because many different types of evidence, often pointing to conflicting courses of action, must be understood. The following recommendations aimed at policymakers, which stem from this analysis, can help to develop effective policymaking in the context of indoor air pollution from radon, and, more generally, in the context of public health policymaking:
Decide who is the ultimate decision maker when it comes to the policy in question and on the overall goal or definition of success. This decision should be documented by the policymakers and returned to as a guiding principle throughout the policymaking process.
Take information and evidence from all relevant disciplines into account, paying particular attention to the limitations and uncertainty that are inherent in each. This may involve the establishment of a committee or task force, including scientists with expertise in epidemiology, economics, health psychology, and other relevant disciplines (such as geoscience and behavioural science), and practitioners such as homeowners and test providers. Such a committee is well placed to provide recommendations to policymakers on the consequences of different indoor radon policies.
Balance this evidence in the development of policies, including regulations, financial incentives, and communication strategies, using a transdisciplinary approach. At this point, it is up to the policymakers to weigh up and balance recommendations from all relevant stakeholders and develop robust policies.
Communicate a clear message from policymakers to different publics, cognisant that communication should be in the form of a two-way dialogue, rather than a top-down flow of information. This involves targeting messages to ensure they are tailored to suit the needs and concerns of specific audiences (e.g., homeowners in high radon areas or low radon areas) and may be achieved by working with professional science communicators.
Build trust between stakeholders through openness and dialogue, and repeated interactions. Policymakers must ensure repeated meetings take place and communication is sustained to ensure a transparent decision-making process.
Collaborate throughout the policymaking process, being clear about the interests, particular requirements, terminology, and timescales of operation of all stakeholders.
Continue supporting and conducting scientific research within and across disciplines to understand the public health context of the policy and reduce current uncertainties.
These recommendations, stemming from the case of indoor radon in Ireland, are valid for pollution health hazards more generally. Through the case of indoor pollution from radon in Ireland, we have highlighted just how simplistic the notion of “following the science” is in the context of public health hazards. We argue that a better understanding of the complexities and knowledge areas involved in the case of indoor radon policy will aid stakeholders, from politicians and policymakers, to scientists and community members, helping to resolve this important public health issue.


{kind=link}
{kind=link}
{kind=link}